in vivo optical coherence tomography of the human larynx ... · lial thickness of laryngeal...
TRANSCRIPT

The LaryngoscopeLippincott Williams & Wilkins, Inc.© 2005 The American Laryngological,Rhinological and Otological Society, Inc.
In Vivo Optical Coherence Tomography ofthe Human Larynx: Normative and BenignPathology in 82 Patients
Brian J. F. Wong, MD, PhD; Ryan P. Jackson, MS; Shuguang Guo, PhD; James M. Ridgway, MD;Usama Mahmood; Jianping Su; Terry Y. Shibuya, MD; Roger L. Crumley, MD; Mai Gu, MD, PhD;William B. Armstrong, MD; Zhongping Chen, PhD
Objectives: Optical coherence tomography (OCT)is an emerging imaging modality that combines low-coherence light with interferometry to produce cross-sectional images of tissue with resolution about 10�m. Patients undergoing surgical head and neck en-doscopy were examined using a fiberoptic OCT imag-ing probe to study and characterize microstructuralanatomy and features of the larynx and benign laryn-geal pathology in vivo. Study Design: Prospective clin-ical trial. Materials and Methods: OCT imaging of thelarynx was performed in 82 of 115 patients who un-derwent surgical endoscopy for various head andneck pathologies. The OCT device employs a 1.3 �mbroadband light source (FWHM, 80 nm). The framerate is 1 Hz. Imaging was performed using a handheldprobe placed in near contact with the target site. Themaximum axial and lateral dimensions for the regionof interest imaged were 2.5 mm � 6 mm, with resolu-tions of 10 �m. Simultaneously, conventional endo-
scopic images were obtained to provide anatomic cor-relation with OCT images and histology. Opticalmicrometry was performed to measure the epitheliumthickness. Results: Systematic OCT imaging of laryn-geal structures and subsites provided information onthe thickness of the epithelium, integrity of the base-ment membrane, and structure of the lamina propria.Microstructural features identified included glands,ducts, blood vessels, fluid collection/edema, and thetransitions between pseudostratified columnar andstratified squamous epithelium. The mean epithe-lial thickness of laryngeal subsites was calculated:true vocal cord (129 �m), false vocal cords (124 �m),aryepiglottic fold (177 �m), subglottis (98 �m), andepiglottis (185 �m). True vocal cord pathology im-aged included Reinke’s edema, papillomatosis, pol-yps, mucous cysts, and granulation tissue. Subglotticimaging identified boundaries between epithelium,lamina propria, and cartilage. The OCT images com-pared favorably with conventional histopathology.Conclusion: OCT has the unique ability to imagelaryngeal tissue microstructure and can detail mi-croanatomic changes in benign, premalignant, andmalignant laryngeal pathologies. OCT holds the po-tential to guide surgical biopsies, direct therapy,and monitor disease, particularly when office-basedsystems are developed. This is a promising imagingmodality to study the larynx. Key Words: Opticalcoherence tomography, larynx, vocal cord, vocalcord polyps, laryngeal cancer, Reinke’s edema, en-doscopy, optical biopsy, respiratory papillomas, hy-perkeratosis, laryngology.
Laryngoscope, 115:1904–1911, 2005
INTRODUCTIONOptical coherence tomography (OCT) is an emerging
imaging modality that uses advanced photonics to producehigh-resolution images in living tissues.1 OCT works in amanner analogous to ultrasound but relies on light ratherthan sound to discern intrinsic differences in tissue struc-ture and uses coherence gating instead of time-of-flight
This work will be presented at the 108th Annual Meeting of theTriological Society on May 16 in Boca Raton, Florida, U.S.A.
Ryan P. Jackson is now at the Stanford University School of Medi-cine.
From the Department of Otolaryngology– Head and Neck Surgery(B.J.F.W., R.P.J., J.M.R., U.M., T.Y.S., R.L.C., W.B.A.), University of CaliforniaIrvine, Orange, California, U.S.A., the Beckman Laser Institute, Univer-sity of California Irvine (B.J.F.W., R.P.J., S.G., J.M.R., U.M., J.S, Z.C.), EastIrvine, California, U.S.A., the Department of Biomedical Engineering(B.J.F.W., R.P.J., S.G., J.S., Z.C.), Rockwell Engineering Center, University ofCalifornia Irvine, Irvine, California, U.S.A., and the Department of Pathol-ogy (M.G.), University of California Irvine, Orange, California, U.S.A.
This work was supported by the National Institutes of Health (DC006026, CA 91717, EB 00293, RR 01192, RR00827), Flight AttendantMedical Research Institute (32456), State of California Tobacco RelatedDisease Research Program (12RT-0113), Air Force Office of Scientific Re-search (F49620_00_1_0371), and the Arnold and Mabel Beckman Founda-tion.
Editor’s Note: This manuscript was accepted for publication July 21,2005.
Send Correspondence to Dr. Wong, The Beckman Laser Institute,University of California Irvine, 1002 Health Sciences Road, East Irvine,CA 92612, U.S.A. E-mail: [email protected]
DOI: 10.1097/01.MLG.0000181465.17744.BE
Laryngoscope 115: November 2005 Wong et al.: Optical Coherence Tomography of the Human Larynx
1904

measurements to localize the origin of the reflected opticalsignal. However, because most biological tissues are tur-bid, OCT has a relatively limited depth of penetration (2–3mm with current technology).
Clinical applications of OCT have generated the mostinterest in the diagnostic evaluation of structures wheretissue microstructural information is of paramount impor-tance, but where biopsy carries significant morbidity. Thegreatest clinical utility to date of OCT has been in retinalimaging where OCT can diagnose subtle pathologicchanges within the retina.2 Likewise, there is tremendousinterest in developing OCT as a diagnostic tool for man-agement of cardiovascular disease.3 In contrast, OCT ap-plications in otolaryngology have been limited.4–7
Biopsy of the true vocal cords (TVC) in the larynxmay produce significant morbidity, albeit less than retinalor intraarterial procedures. Voice quality may change dra-matically and permanently after vocal fold surgery re-gardless of whether the pathology is benign or malignant.The negative impact of TVC surgery on voice quality hasbeen well documented, and there are a number of cases ofTVC surgery precipitating a retreat from public service orthe end of a career in the entertainment industries. Like-wise, distinguishing between microinvasive cancer, pre-malignant lesions, and benign disorders that clinicallymimic cancer remains a challenge. Currently, no imagingtechnology is available to aid the guidance and targetingof biopsies or for that matter in the monitoring of diseaseprogression.
Analogous to real-time CT, ultrasound, and magneticresonance imaging (MRI) guided therapy, OCT has a po-tential role in the management of superficial diseasewhere the pathologic and key structural information is atthe histologic level. Even though ex vivo OCT imaging wasfirst reported in 1991, the first clinical imaging of thelarynx was not reported until 1997.8 This first clinicalstudy was limited in case numbers and used a slow, low-resolution, first generation system to accomplish imaging.The present study is a comprehensive evaluation of 82patients who underwent laryngeal OCT imaging duringsurgical endoscopy. The current series demonstrates thein vivo microstructural features of the larynx while pro-viding quantitative epithelial information. We present thelargest series of OCT head and neck pathology reported todate.
MATERIALS AND METHODS
Patient Population and EndoscopyOCT imaging was performed in 115 patients undergoing
laryngeal, esophageal, or tracheobronchial endoscopy under gen-eral anesthesia at the University of California, Irvine (UCI) Med-ical Center in accordance with guidelines of the Human SubjectsInstitutional Review Board at UCI. Eighty-two of these patientshad at least one subsite of the larynx evaluated using OCT,whereas other regions of the head and neck were imaged in theremaining patients. OCT imaging of the larynx was performedwith or without the use of laryngeal suspension depending on theclinical need. When possible, correlative digital images of thelarynx were recorded using either a rigid telescope or operatingmicroscope. When clinically indicated (e.g., for tumor diagnosis,polyp removal), biopsy or excision of suspicious mucosal lesions
was performed. Information obtained from OCT imaging waspurposely not used to alter clinical decision making in any wayduring this study. Imaging generally required approximately 5minutes of additional operating room time.
OCT InstrumentationThe core OCT device has been described previously.9,10 The
system used in this study used a low coherence light source(central wavelength � � 1310 nm, FWHM �� � 80 nm, AFC BT1310, JDS Uniphase, San Jose, CA).11 Raster scanned imageswere generated by controlled motion of the imaging fiber using aprecision piezoelectric translation stage (Model 663.4pr, PhysikInstrumente, Tustin, CA). The delicate fiber and optical elementsare enclosed by a transparent plastic tube, which was, in turn,surrounded by a second metal tube (diameter 2 mm) for mechan-ical support.
The axial resolution of the system is 9 �m and is determinedby the coherence length of the light source. The lateral resolutionis diffraction limited (20 �m). Signals were obtained up to a depthof 2.6 mm, whereas the lateral extent of each image was deter-mined by the length over which the fiber was translated by thestage, typically 6 mm.
OCT ImagingImages were acquired during surgical endoscopy by insert-
ing the probe through the laryngoscope and placing the tip eitherin near contact or gentle contact with the region of interest. OCTimages were acquired with the left and right side of each image,respectively, representing proximal and distal tissues. The imageplane is defined by the direction of light propagation, which isorthogonal to the long axis of the probe. OCT imaging was typi-cally performed in tandem with a rigid endoscope, allowing si-multaneous viewing of the video and the OCT image on adjacentmonitors. OCT images were digitally captured and then cata-logued in a database.
Image AnalysisDigital micrometry (Photoshop, Adobe, San Jose, CA) was
performed to obtain normative measurements of epithelial thick-ness in each laryngeal subsite. In each image, measurements ofepithelial thickness were obtained at five evenly spaced pointsseparated by 1 mm. These data were averaged to obtain theepithelial thickness per subject. In turn, measurements for eachpatient were analyzed to obtain an overall average of our studygroup. Measurements were not taken from those images in whichthe demarcation between the epithelium and underlying laminapropria (LP) could not be clearly identified. Whereas 82 patientsunderwent laryngeal imaging, the TVCs were imaged only in 68.In the case of TVC imaging, many patients had abnormal vocalcords features (i.e., nodules, papillomas [P], tumors) and were notincluded in the normative analysis. Imaging of other laryngealsubsites was limited by the constraints of operative time and alsothe need to reposition the laryngoscope in those patients under-going laryngeal suspension.
HistopathologySixty of the 82 patients underwent laryngeal biopsy, and
vocal cord biopsies were obtained in 23. Specimens were fixed in10% neutral buffered formalin, sectioned in 5-micron thickness,and then stained with hematoxylin-eosin followed byhistologicexamination under microscopy.
RESULTSOCT imaging of at least one laryngeal subsite was
performed in 82 patients during surgical endoscopy. The
Laryngoscope 115: November 2005 Wong et al.: Optical Coherence Tomography of the Human Larynx
1905
majority of the subjects demonstrated normal vocal cords(n � 43); however, the larynx was imaged during opera-tive endoscopy for pathology in other regions of the headand neck. The laryngeal diseases and lesions studied arelisted in Table I by subsite. Some patients underwentendoscopy for injection TVC medialization to improve dys-phonia associated with vocal cord paralysis. Some of thesubjects evaluated in this study were diagnosed with la-ryngeal cancer and are excluded from the present analysisand will be reported in greater detail in the future. Thepresent results primarily focuses on normative laryngealstructure, benign pathology, and limited examples of in-vasive laryngeal cancer.
The following images are representative illustrationsof the features, disorders, and pathology that were imagedand selected to emphasize the potential of OCT as a tool inlaryngology. It must be emphasized that OCT imaging,similar to ultrasound, results in the acquisition of time-series imaging in registry and can be viewed as a “video,”albeit at slower frame rates. The difference between indi-vidual static images and an OCT “video” examination issignificant, and representative video clips are archived onthe internet-based companion to this journal.
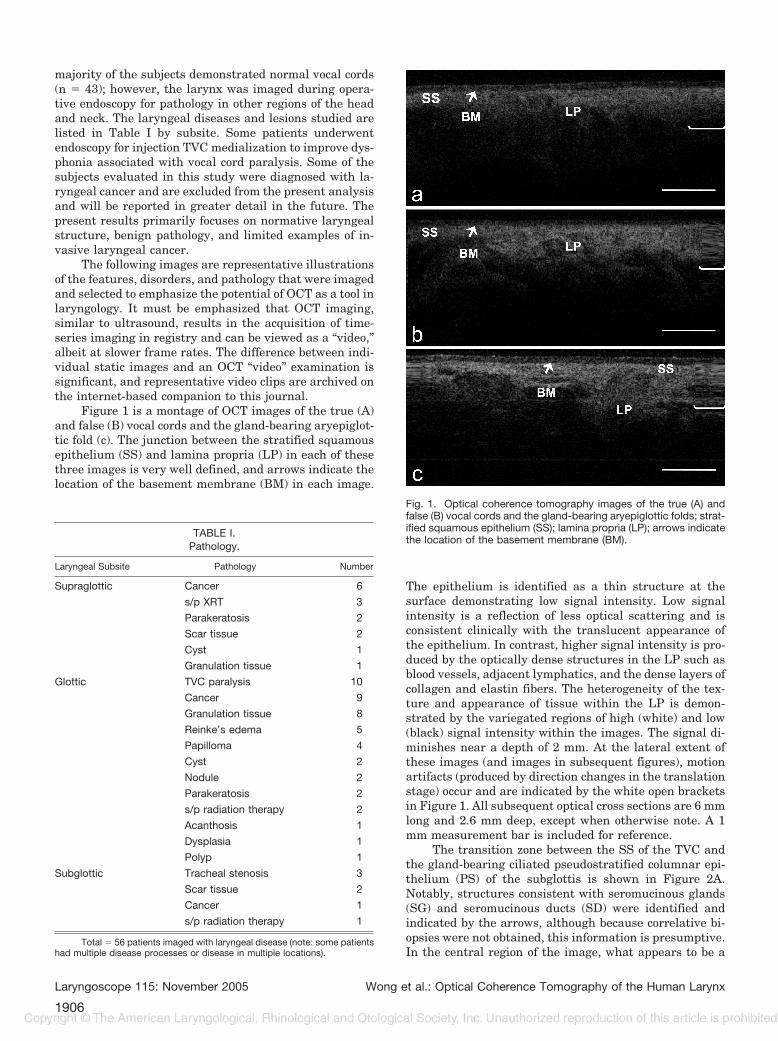
Figure 1 is a montage of OCT images of the true (A)and false (B) vocal cords and the gland-bearing aryepiglot-tic fold (c). The junction between the stratified squamousepithelium (SS) and lamina propria (LP) in each of thesethree images is very well defined, and arrows indicate thelocation of the basement membrane (BM) in each image.
The epithelium is identified as a thin structure at thesurface demonstrating low signal intensity. Low signalintensity is a reflection of less optical scattering and isconsistent clinically with the translucent appearance ofthe epithelium. In contrast, higher signal intensity is pro-duced by the optically dense structures in the LP such asblood vessels, adjacent lymphatics, and the dense layers ofcollagen and elastin fibers. The heterogeneity of the tex-ture and appearance of tissue within the LP is demon-strated by the variegated regions of high (white) and low(black) signal intensity within the images. The signal di-minishes near a depth of 2 mm. At the lateral extent ofthese images (and images in subsequent figures), motionartifacts (produced by direction changes in the translationstage) occur and are indicated by the white open bracketsin Figure 1. All subsequent optical cross sections are 6 mmlong and 2.6 mm deep, except when otherwise note. A 1mm measurement bar is included for reference.
The transition zone between the SS of the TVC andthe gland-bearing ciliated pseudostratified columnar epi-thelium (PS) of the subglottis is shown in Figure 2A.Notably, structures consistent with seromucinous glands(SG) and seromucinous ducts (SD) were identified andindicated by the arrows, although because correlative bi-opsies were not obtained, this information is presumptive.In the central region of the image, what appears to be a
TABLE I.Pathology.
Laryngeal Subsite Pathology Number
Supraglottic Cancer 6
s/p XRT 3
Parakeratosis 2
Scar tissue 2
Cyst 1
Granulation tissue 1
Glottic TVC paralysis 10
Cancer 9
Granulation tissue 8
Reinke’s edema 5
Papilloma 4
Cyst 2
Nodule 2
Parakeratosis 2
s/p radiation therapy 2
Acanthosis 1
Dysplasia 1
Polyp 1
Subglottic Tracheal stenosis 3
Scar tissue 2
Cancer 1
s/p radiation therapy 1
Total � 56 patients imaged with laryngeal disease (note: some patientshad multiple disease processes or disease in multiple locations).
Fig. 1. Optical coherence tomography images of the true (A) andfalse (B) vocal cords and the gland-bearing aryepiglottic folds; strat-ified squamous epithelium (SS); lamina propria (LP); arrows indicatethe location of the basement membrane (BM).
Laryngoscope 115: November 2005 Wong et al.: Optical Coherence Tomography of the Human Larynx
1906

duct-like structure terminates on the surface of the cord.The epiglottis (Fig. 2B) is also known to be highly glan-dular, and similar glandular features were identified. Asharp demarcation exists between the LP and what islikely the smooth surface of the epiglottic cartilage (EC).
Gland-like structures and soft tissue-cartilage bor-ders are also seen in the subglottis (Fig. 3). In the proxi-mal subglottis (Fig. 3A), low signal intensity structuresextending longitudinally from proximal to distal wereidentified and may be consistent with glandular tissues.At the left side, the high signal intensity at the epithelialsurface is caused by specular reflection and is an artifact.At the far right, the arc shaped border between the LP andthe cricoid cartilage (CC) is seen. Distally, the CC is seenas well (Fig. 3B). The high signal intensity line at the topof the image is caused by serosanguinous debris collectingon the plastic surface of the OCT probe.
Pathologic conditions were imaged as well usingOCT. The microstructure of the vocal cord in Reinke’sedema has been primarily studied during limited postmor-tem examinations. Little is known about the true in vivochanges in TVC structure accompanying this disorder.Five patients with a clinical diagnosis of Reinke’s edemawere examined. The image in Figure 4A shows numerouswell-demarcated fusiform low-signal intensity regionswithin the LP, which we believe are the regions whereclear fluid has collected (E). Homogenous regions with lowsignal intensity are produced by a low optical scattering inclear rather than turbid media. At the upper left of theimage, two arrows point toward circular low-signal inten-sity regions, which may represent capillaries (CP) as ves-sels, were directly visualized during endoscopy in this
general vicinity. The LP in the image has greater signalintensity, likely because of the increased density of matrixproteins such as collagen and elastin. Numerous linearstructures are seen as well, suggesting a layered structureof the TVC LP in Reinke’s edema. Of interesting note is
Fig. 2. (A) Transition zone of between the stratified squamousepithelium of the true vocal cord and the gland-bearing ciliatedpseudostratified columnar epithelium (PS) of the subglottis; sero-mucinous glands (SG); and seromucinous ducts (SD). Epiglottis (B).Note the sharp demarcation is identified between the lamina propriaand what is likely the smooth surface of the epiglottic cartilage.
Fig. 3. Optical coherence tomography (OCT) images of the sub-glottis. In the proximal subglottis (A), low signal intensity structuresextending longitudinally from proximal to distal were identified andmay be consistent with glandular tissues. At the left side, the highsignal intensity at the epithelial surface is caused by specular re-flection. At the far right, the arc shaped border between the laminapropria and the cricoid cartilage (CC) is seen. Distally (B), the CC isseen as well. The high signal intensity line at the top of the image iscaused by serosanguinous debris collecting on the plastic surfaceof the OCT probe.
Fig. 4. Optical coherence tomography images of Reinke’s edema.(A) Numerous well-demarcated fusiform low-signal intensity regionswithin the lamina propria which are consistent with edema (E).Arrows point toward circular low-signal intensity regions, which maybe capillaries (CP). A second example (B). Endoscopic image of thepatient’s (inset). Regions of what is likely fluid collection (arrows).
Laryngoscope 115: November 2005 Wong et al.: Optical Coherence Tomography of the Human Larynx
1907

the accumulation of fluid collections in discrete locationswithin the vocal cord, rather than as a diffuse swellingthroughout the LP. The dimensions of Figure 4A are only1.275 � 3 mm, which was selected to provide a moredetailed image.
A second image of Reinke’s edema (Fig. 4B) is shownalongside an inset endoscopic image of the patient’s lar-ynx. Arrows in the image point to regions of what is likelyfluid collection. Given the location (TVC), it is unlikelythat these structures are glandular. They are not bloodvessels because the erythrocytes absorb light and cast an“optical shadow,” obfuscating structures distal to the di-rection of light propagation.
OCT images of vocal cord polyps (Fig. 5, A to C) werealso obtained, where A is an endoscopic image of an orga-nized polyp, B is the corresponding OCT image, and C isthe corresponding histopathology after excision. There isgood correlation between the in vivo OCT images andhistopathology, although differences result from registra-tion mismatches because of orientation, sectioning, andartifacts produced by fixation. A photograph of a simplesupraglottic respiratory epithelial lined mucous retentioncyst (Fig. 5D) and the corresponding OCT image of thecyst (Fig. 5E) are also illustrated. Correlative histopathol-ogy (not shown) demonstrated the cyst was lined withrespiratory epithelium.
Several examples of histologically confirmed laryn-geal hyperkeratosis (Fig. 6A) and respiratory papilloma-tosis (Fig. 6B) were imaged during the study. In hyper-keratotic lesions of the larynx, the epithelial layer ismarkedly thickened up to 300 �m, whereas the BM wasclearly demonstrated to remain intact. Similarly, withlaryngeal papilloma (P), illustrated in the lower image,the BM was also shown to be intact. The double-headedarrow indicates the extent of projection of the P. NormalSS is seen to the right of the lesion in this image.
BM disruption was seen in several cases in the study.Loss of a BM on OCT was seen in cases of microinvasivesquamous cell carcinoma of the larynx and in vocal pro-cess granulomas. Early microinvasive squamous cell car-cinoma was imaged (Fig. 7A), which clearly demonstratedthe loss of the BM and confluence of structural detailbetween superficial epithelium and the LP. The diagnosis
was confirmed histologically. This demonstrates the po-tential value of OCT as a means to guide or direct biopsiesinto regions of the cord where the diagnostic yield wouldbe greater. Likewise, granulomas (Fig. 7B) also demon-strate loss of BM integrity on OCT just as they do on Fig.7A (the length of the image has been cropped to 4 mm).Although clinically vocal process granulomas have a dis-tinctive history and appearance, there can be clinical con-cern for the possibility of malignancy. OCT was able todemonstrate loss of BM integrity in both processes, butthe resolution is not yet adequate to provide the cellulardetail needed to distinguish benign from malignant cellu-lar processes. In this case, the diagnosis can only be madeusing microscopy as structural detail below the OCT res-olution limit of 10 �m is required.
Epithelial thickness was measured at several laryn-geal subsites (Table II). The epithelium was thinnest inthe subglottis and thickest along the lingual surface of theepiglottis. TVC and false vocal cord thickness were bothabout 125 �m, which corresponds to approximately 10 celllayers in thickness. Measurements were made only inthose subjects who had normal larynges and were under-going endoscopy for other abnormalities of the head andneck.
DiscussionWe present our experience in imaging normal laryn-
ges as well as benign pathologic conditions in 82 adultsubjects and report the first comprehensive study to sys-tematically examine vocal cord microstructure using OCT.Present image guided therapies relies on the relativelycoarse imaging resolution of CT, MRI, or ultrasound todiagnose or treat disease with tissue resolution at verybest of 1 mm. Contact endoscopy, a form of microscopy,requires extensive training, the use of dyes to stain tissuefor contrast, and can only provide extremely superficial
Fig. 5. Optical coherence tomography (OCT) images of a vocal cordpolyps and a supraglottic retention cyst. (A) Endoscopic image of anorganized polyp; (B) corresponding OCT image; (C) histopathology.(D) endoscopic image of supraglottic mucous retention cyst; (E)OCT image of the cyst.
Fig. 6. Optical coherence tomography images of hyperkeratosis (A)and respiratory papillomatosis (B). Papilloma (P) illustrated in thelower image is notable for the thickened tumor layer, which at thisstage does not violate the basement membrane.
Laryngoscope 115: November 2005 Wong et al.: Optical Coherence Tomography of the Human Larynx
1908

en-face image date. In contrast, OCT is a high-resolution(approximately 10 �m) imaging modality, which is opti-mally suited to evaluate thin-layered structures such asthose that line the surface of the body, airway, and gas-trointestinal tract. Many of the laryngeal pathologies areidentified within the first 1 to 2 mm of the mucosa andmake OCT an ideal diagnostic imaging modality. Currentnoninvasive diagnostic tests rely on either two dimen-sional imaging or global physiologic measures of cord func-tion such as those acquired during videostroboscopy oracoustic analysis. With the exception of contact endoscopy,which is not widely practiced, no other noninvasive imag-ing technique has been applied to provide detailed micro-anatomic information of the larynx.
The principal value of OCT in laryngology is that itstands alone in its ability to provide in vivo images of vocal
cord microstructure to a depth not attainable with otherimaging modalities. The images presented in Figures 1 to7 are static representations of tissue structure and unfor-tunately do not demonstrate the full capabilities of thenear real-time in vivo capability of OCT imaging. Theelectronic supplement to this article on the Internet con-tains several such “video” OCT image clips that corre-spond to the single image figures, which will be describedbelow. In our study, an OCT image was acquired everysecond during endoscopic study. Similar to clinical ultra-sonography, a great deal more information can be gleanedin these near real-time “movies” compared with images.Structures can be gently palpated using the probe to as-sess the degree of compressibility, the angle or imageplane can be reoriented to obtain other views or projec-tions, and larger regions of interest can be scanned in asweeping panorama. As high-speed, high-resolution OCTsystems evolve, the use of this technology will likely bemore similar to dynamic imaging modalities such as ul-trasound rather than static imaging like CT or MRI. Al-though the present system can acquire images at up to 12frames/second, a high-speed endoscopic probe that usesmicro-electromechanical system (MEMS) technology iscurrently under development in our laboratories.
The second objective of this study was to obtain quan-titative measurements of the thickness of the epitheliumin the different subsites of the larynx (Table II) becausethis variable may be important in aiding in the diagnosisof numerous processes such as epithelial hyperkeratosis.A comprehensive analysis of the epithelial thickness of
Fig. 7. Optical coherence tomographyimages of (A) microinvasive squamouscell carcinoma (C), which clearly dem-onstrates the loss of the basementmembrane and confluence of struc-tural detail between superficial epithe-lium and the lamina propria; (B) gran-uloma with endoscopic images of thegranulomas at left.
TABLE II.Laryngeal Epithelium Thickness.
Laryngeal SubsiteNumber of
PatientsAverage number ofImages per patient
EpithelialThickness
(�m)
True Vocal Cord 46 2.96 129 � 58
False Vocal Cord 25 1.68 124 � 47
Aryepiglottic fold 6 1.67 177 � 70
Subglottis 15 1.87 98 � 44
Laryngeal epiglottis 15 1.93 185 � 82
Lingual epiglottis 4 1.50 271 � 26
Laryngoscope 115: November 2005 Wong et al.: Optical Coherence Tomography of the Human Larynx
1909

each laryngeal subsite in vivo has not been previouslyreported. The benefits of in vivo real-time tissue analysisinclude avoidance of formalin fixation artifacts. The datain Table II provides the first set of data on the normativein vivo microstructural anatomy of the larynx.
Only one very limited study has previously imagedthe human larynx in vivo using OCT and reported find-ings on 15 patients, all with vocal cord pathology (primar-ily cancer).8,12 Although this initial study did demonstratethe potential value of OCT, there were a number of short-comings, which the present study addresses. From a tech-nical standpoint, Sergeev et al.8 used an 830 nm lightsource with a narrower bandwidth, yielding a shallowerdepth of penetration (approximately 1 mm) and lowerresolution (approximately 20 �m) in comparison with the2 to 3 mm depth of penetration and 10 �m resolution inour present study. Their mechanical scanning was nonlin-ear, resulting in image distortion, and required 1.5 sec-onds to image a 2 mm wide region of interest. Our rela-tively rapid acquisition of images in this study requiredonly 1 second to image a 6 mm frame and provided asubstantial increase in image size (510 � 1,200 pixels vs.200 � 200 pixels).
The most important observation in this study is theconsistent identification of the demarcation between thelaryngeal epithelium and the underlying LP in normalpatients and most benign pathologic processes, includingcysts, polyps, hyperkeratotic lesions, and swelling withinthe LP (Fig. 4 to 6). This sharp border likely representsthe junction between the epithelial BM and LP. The BMseparates the translucent epithelium largely devoid ofblood vessels from the vascularized LP, which is also com-posed of relatively dense layers of collagen and elastin.Even in benign disorders, such as that illustrated in Fig-ure 4 (Reinke’s edema) and Figure 5 (cysts), this demar-cation remains distinct. The potential clinical impact ofOCT’s ability to delineate the BM cannot be overempha-sized because it is the disruption of BM integrity, whichdefines invasive cancer. Most likely the single greatestutility of OCT will be its ability to identify subtle disrup-tions in BM integrity. This ability can be used to charac-terize lesions, identify areas for biopsy, and perhaps aidearlier detection of malignant lesions by decreasing thelikelihood of missing a cancer because of sampling errorduring biopsy. Figure 7A illustrates the potential of OCTin early cancer management; the image depicts both thethickening of the epithelium and the loss of a clear andsharp transition between this layer and the LP. Identify-ing the location of these sites could facilitate more accu-rate targeting of biopsies and improve the diagnostic yieldwhile reducing the number of procedures required.
The presumptive identification of glandular struc-tures and ducts in the supraglottic and subglottic larynx isa novel in vivo observation that has not been previouslydemonstrated using any imaging modality. The imagesacquired in the transition zones between the TVC andeither the gland-bearing false vocal cords (Fig. 2) or sub-glottis (Fig. 3) identified glandular structures in a complexductal system terminating at the epithelial surface.
The OCT findings in Reinke’s edema (Fig. 4) arestriking because discrete regions of low signal intensity
(presumably clear serous fluid) were readily identified.Reinke’s edema is essentially a clinical entity, with littleknown about its true cross-sectional histology. Reinke’sedema presumably results from the paucity of lymphaticsin the TVC and build up of gelatinous edema. Whereasremoval of chronic irritation such as reflux or smoking arethe first options, surgical treatment involves microsurgeryand removal of the fluid or gel. Currently, laryngologistsoperate without knowledge of where or how deep this fluidis sequestered. The present OCT images demonstrate thedepth and location of these fluid/gel filled regions, andimaging Reinke’s edema during surgery in the future canaid or guide surgery, particularly if high-resolution robot-assisted microsurgery is adopted by surgeons. In the fu-ture, office-based laryngeal OCT imaging may provideinsight into the pathophysiology as well because laryngealabnormalities can be imaged as they evolve over timewithout the need for anesthesia.
OCT remains a technology in continual evolution andbroader clinical adoption will be driven by reduction incomponent costs, further commercialization, and ad-vances broadband light sources. The technology relatedfactors, in our opinion, are most important as the cost ofthe components for OCT systems continues to drop. TheOCT system used in this study is a relatively advanceddevice with respect to clinical implementation and haslimit of 9 �m resolution. However, it does require thepatient to be relatively immobile to eliminate severe mo-tion artifacts. Our next generation instruments usingbroadband fiber laser sources should be able to obtainimages with resolution approaching 1 �m, which wouldfacilitate the identification of individual cells at fasterscanning rates13,14 but at present remains a researchdevice and cannot be transported to the operating room.
Our future work is focused on evaluating the efficacyin detecting BM integrity in patients with visible lesionssuspicious for early laryngeal cancer. We are focused onthe development of a better portable high-speed and high-resolution OCT system, which will allow imaging of cellsand subcellular level structures. In addition, office-basedOCT system is currently in development as well and iscurrently being evaluated on patients during officevideostroboscopy.
CONCLUSIONS1. We present the largest study of OCT imaging pub-
lished to date examining its utility in evaluating laryngealpathologies.
2. We have found considerable utility for OCT inclinically assessing laryngeal pathology.
3. OCT images the laryngeal tissues to a resolutionand depth of penetration not obtainable with any cur-rently available imaging modalities in a noninvasivefashion.
4. OCT has the potential to be a valuable complemen-tary tool in laryngeal diagnostics, to provide more tar-geted biopsy of suspicious lesions, and to allow more ob-jective, noninvasive monitoring of disease progression andresponse to therapeutic interventions.
Laryngoscope 115: November 2005 Wong et al.: Optical Coherence Tomography of the Human Larynx
1910

5. The importance of the ability of OCT to demon-strate the integrity or disruption of the BM cannot beoveremphasized.
AcknowledgmentsThe authors thank master machinists Rudolph Lim-
burg and Steve Knisley for assistance with construction ofthe instrumentation and Aya Yamamoto, RN, and ClevanM. Barclay for their help and patience in the operatingroom.
BIBLIOGRAPHY1. Huang D, Swanson EA, Lin CP, et al. Optical coherence
tomography. Science 1991;254:1178–1183.2. Voo I, Mavrofrides EC, Puliafito CA. Clinical applications of
optical coherence tomography for the diagnosis and man-agement of macular diseases. Ophthalmol Clin North Am2004;17:21–31.
3. Patwari P, Weissman NJ, Boppart SA, et al. Assessment ofcoronary plaque with optical coherence tomography andhigh frequency ultrasound. Am J Cardiol 2000;85:641–644.
4. Wong BJF, de Boer JF, Park BH, et al. Optical coherencetomography of the rat cochlea. J Biomed Opt 2000;5:367–70.
5. Wong BJF, Zhao Y, Yamaguchi M, et al. Imaging the internalstructure of the rat cochlea using optical coherence tomog-raphy at 0.827 mm and 1.3 mm. Otolaryngol Head NeckSurg 2004;130:334–338.
6. Bibas AG, Podoleanu AG, Cucu RG, et al. 3-D optical coher-
ence tomography of the laryngeal mucosa. Clin Otolaryn-gol 2004;29:713–720.
7. Pitris C, Saunders KT, Fujimoto JG, Brezinski ME. High-resolution imaging of the middle ear with optical coherencetomography: a feasibility study. Arch Otolaryngol HeadNeck Surg 2001;127:637–642.
8. Sergeev AM, Gelikonov VM, Gelikonov GV, et al. In vivoendoscopic OCT imaging of precancer and cancer states ofhuman mucosa. Opt Express 1997;1:432–440.
9. Zhao Y, Chen Z, Saxer C, et al. Phase-resolved opticalcoherence tomography and optical Doppler tomographyfor imaging blood flow in human skin with fast scanningspeed and high velocity sensitivity. Optics Lett2000;25::114 –116.
10. Ren H, Ding Z, Zhao Y, et al. Phase-resolved functional opti-cal coherence tomography: simultaneous imaging of in situtissue structure, blood flow velocity, standard deviation,birefringence, and Stokes vectors in human skin. OpticsLett 2002;27:1702–1704.
11. Hanna N, Saltzman D, Mukai D, et al. Two-dimensional and3-dimensional optical coherence tomographic imaging ofthe airway, lung, and pleura. J Thorac Cardiovasc Surg2005;129:615–622.
12. Shakhov AV, Terentjeva AB, Kamensky VA, et al. Opticalcoherence tomography monitoring for laser surgery of la-ryngeal carcinoma. J Surg Oncol 2001;77:253–258.
13. Wang Y, Zhao Y, Nelson JS, Chen Z. Ultrahigh-resolutionoptical coherence tomography by broadband continuumgeneration from a photonic crystal fiber. Opt Lett 2003;28:182–184.
14. Lim H, Jiang Y, Wang Y, et al. Ultrahigh- resolution opticalcoherence tomography with a fiber laser source at 1 �m.Optics Lett 2005;30:1171–1173.
Laryngoscope 115: November 2005 Wong et al.: Optical Coherence Tomography of the Human Larynx
1911