implementing inpatient precision medicine€¦ · implementing inpatient precision medicine ... •...
TRANSCRIPT

Implementing Inpatient Precision Medicine
Stephen Kingsmore MD DSc
Radygenomics.org

Conflicts of Interest
• None

Learning Objectives
• Understand principles of genomic medicine
• Understand status of clinical whole genome sequencing
• Be able to ascertain inpatients who may benefit from whole genome sequencing
• Comprehend the evidence base for rapid WGS in ill infants
• 2 month old male admitted for jaundice x 1 month and
poor weight gain
• Pregnancy/birth: uneventful
• Negative family history
• Birth weight 2.9kg (14%ile)
Rady Children’s Hospital Baby 6026, Sunday
15% of US newborns admitted to a NICU or PICU

Children with
Severe Chronic
Illness
High Risk
Children
Healthy
Children
% Cost % Children
76%
14%
10%
10%
20%
70%
NICU, PICU, CVICUNeuro-oncologyInpatients
Why start here?
• Weight 3.9kg (0.05%ile).
• Head circumference 3%ile, length 1%ile
• Jaundiced
• High pitched continuous murmur left chest
• III/VI low pitched harsh systolic murmur LUSB
• No hepatosplenomegaly
Physical Examination

Labs: AST 241, ALT 188, GGT 562, total bilirubin 10.6, direct bilirubin 5.1, ammonia 27 (L)
Abdominal ultrasound: normal
Liver Biopsy: giant cell hepatitis
Hepatobiliary HIDA scan: non-excreting
Tests negative for infection, alpha-1 antitrypsin deficiency, thyroid disease
Chest X-Ray, echocardiogram, CT scan heart:
• Patent ductus arteriousus
• Hypoplastic branch pulmonary arteries,
• Patent foramen ovale
• Aberrant right subclavian artery
Tests
Genomics: the study of all of your DNA letters
We are fearfully and wonderfully made. Psalm 139
Each of My 37 Trillion Cells Contains2 Genomes of 3.2 Billion DNA Letters

Molecular Diagnosis: ID the cause of a genetic disease in a patient

Leading cause of NICU and PICU
death
Genetic diseases in infants often look atypical
Conventional molecular testingtoo slow to guideNICU and PICU care
Timely Diagnosis of 8,000 Genetic
Diseases in NICUs and PICUs
Unique Requirements for Diagnosis of Genetic Diseases in Neonatal, Pediatric and Cardiovascular ICU

The conventional model in medicine does not work well in rare diseases or precision therapies
• Clinical diagnosis → Empiric Treatment
• Molecular diagnosis → Precision Therapy
• Situation today:
– Misdiagnosis & mistreatment
– Delayed diagnosis & empiric treatment

Tuesday
• Tachypnea, acidosis: Transferred to PICU
• Clinical diagnosis: biliary atresia
– Incidence 1 in 10,000
• Empiric treatment: Kasai procedure
– Prognosis worsens with time to surgery

2:30PM Consent, blood sample from mum, dad & baby

Implementing Inpatient Precision Medicine

Computer readable digest of infant’s medical record

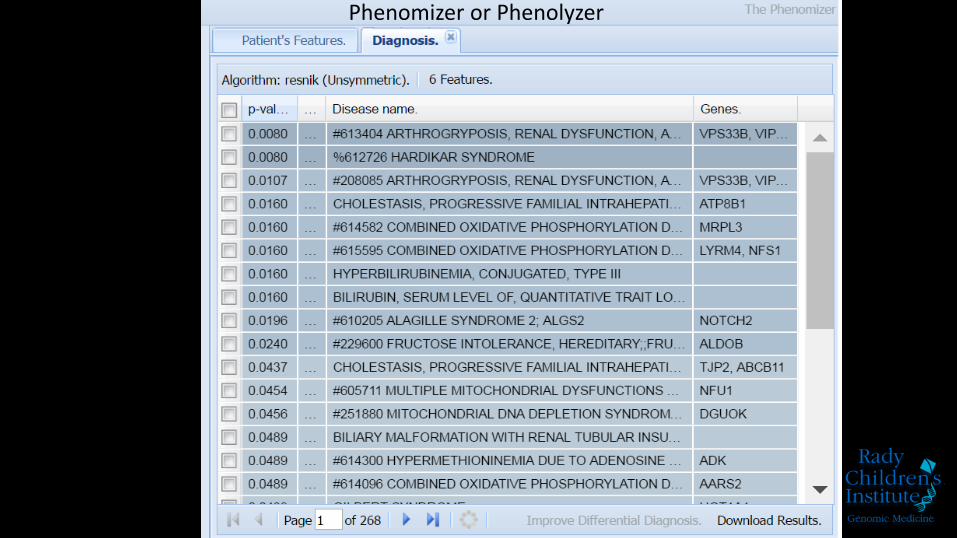
Phenomizer or Phenolyzer

Isolate DNA and prepare it for sequencing
Rapid genome sequencing


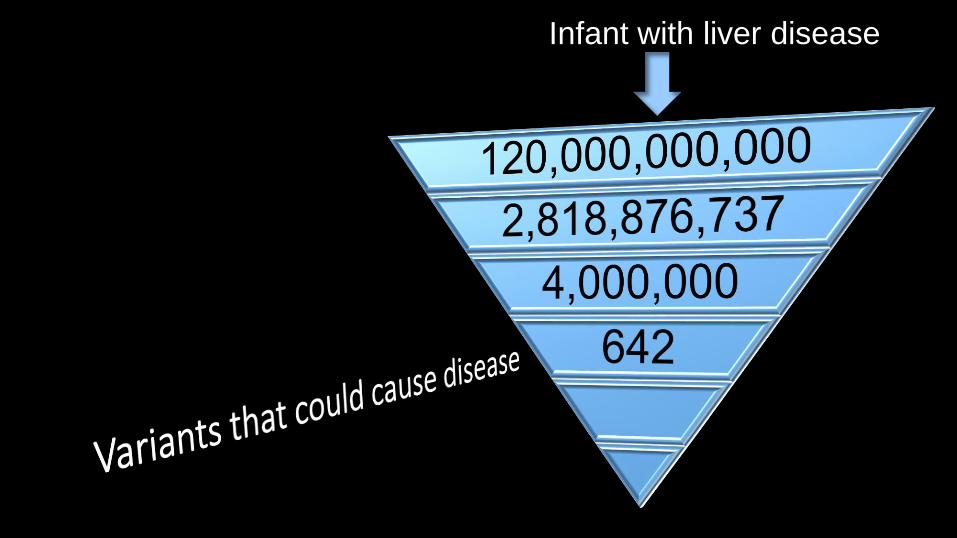
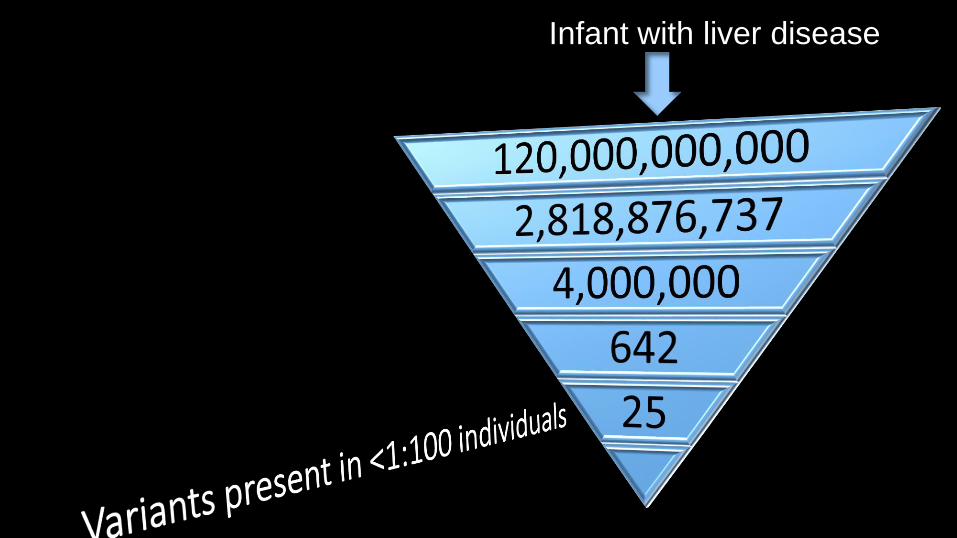
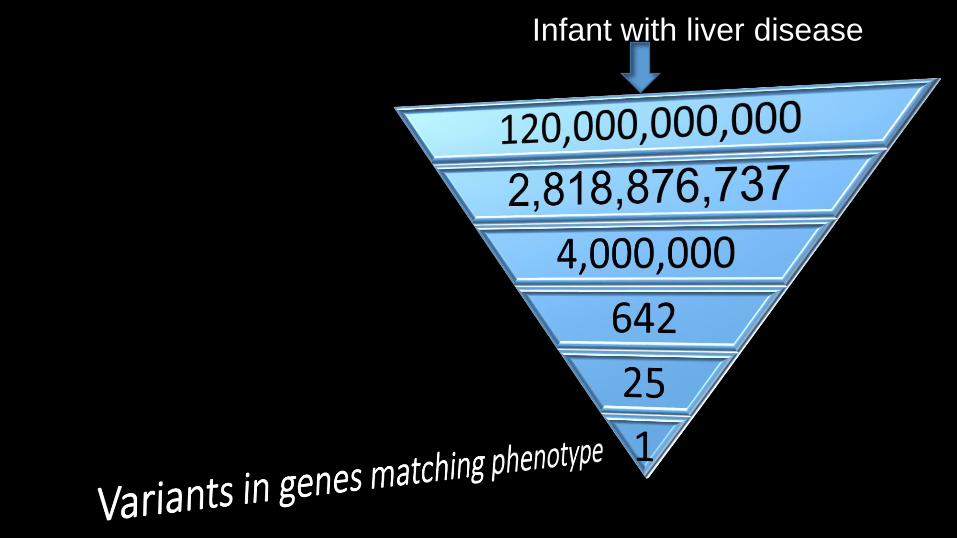
Genome Analysis and Interpretation

Infant with liver disease

Infant with liver disease
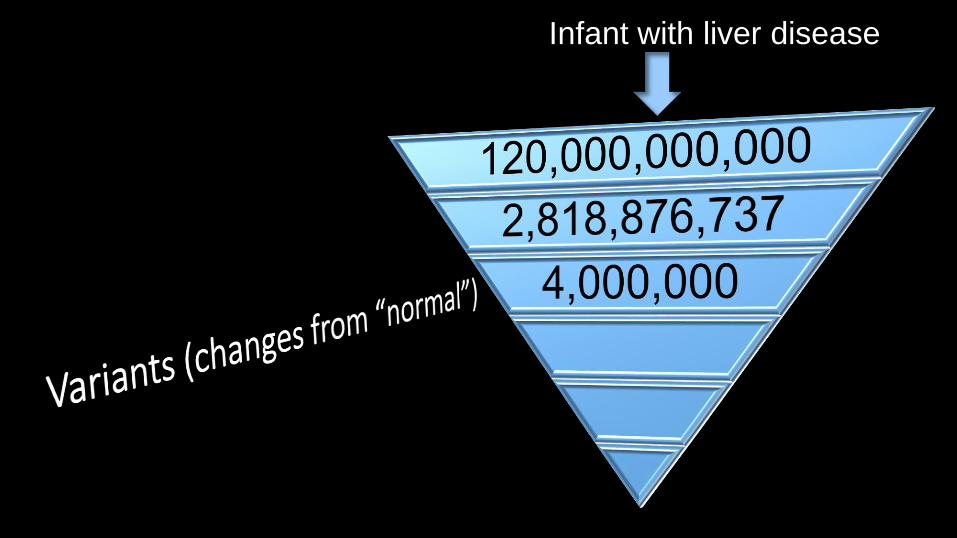
Infant with liver disease
Infant with liver disease
Infant with liver disease
Infant with liver disease

43 Hours Later: Molecular Diagnosis
0
10
20
30
40
50
60
9 10 11 12 13 14Chromosome 20
Gen
om
e se
qu
ence
co
vera
ge
Position 10,471,400
Position 13,459,331
JAG1: Alagille Syndrome Gene
Jaundice, bile duct paucity on liver biopsy; congenital heart disease, primarily involving
pulmonary arteries
Kasai hepatoportoenterostomy for biliary atresia
Friday 11AM

Pediatr Gastroenterol Hepatol Nutr. 2015 18:175-9.
“5% of infants with Alagille syndrome are diagnosed clinically asbiliary atresia and undergo Kasai operation.Among 15 children with Alagille syndrome, mortality was 60%among the Kasai group, and 10% in the non-Kasai group .Liver transplantation was performed in 100% of the Kasai group,and 20% of the non-Kasai group.”
Precision Medicine: 50% Reduction in Likelihood of Death

Rady NICU Infant 6041
• 2 day old female with seizures since 16 hours after delivery
• Normal pregnancy, delivery• Electroencephalogram: tonic & myoclonic
seizures, background burst suppression• Head circumference 5th %ile
• Physical exam normal• Brain MRI normal• Infection, metabolic tests normal• Standard anti-epileptics ineffective:
• Phenobarbital then • Levetiracetam then• Topiramate

Molecular Diagnosis in 68 hours
• Ohtahara syndrome
• de novo KCNQ2 c.875T>C; p.Leu292Pro• Gene Name DNA Change Protein Change
• Precision Medicine: carbamazepine, phenytoin
• Seizures controlled – child discharged (18 days after admission) in time for family Christmas
Previous Ohtahara diagnosis in same NICU one year earlier (pre-WGS)
• 59 day hospital stay; diagnosis after discharge
• “Early recognition of KCNQ2 encephalopathy followed by the most appropriate and effective treatment may be important for reducing the neurodevelopmental impairment associated with this disorder”
• Pisano et al. Epilepsia 2015 56:685-91.

Randomized Controlled Trial

Faster Time to Diagnosis
Case Series
Less than 1 year old
Inpatient July 2016 – February 2017
Presentation that may be caused by a single gene disorder or clinical course not following typical pattern
Without known genetic diagnosis

Enrollment by Location
SourceEnrolled
Families
NICU 24
CVICU 3
PICU 3
Gastro 9
Neurology 2
Hematology 1
42

Less than 1 year of age and inpatient:
42
Diagnosis:18
Non-Diagnostic:24
43%

Diagnostic Utility of Whole Genome and Exome Sequencing
NICU rWGS
NICU rWGS

Less than 1 year of age and inpatient:
42
Diagnosis:18
Non-Diagnostic:24
No change in care: 6 cases

Presentations of cases with diagnosis but no change in care
Presentation Causative Gene
Cholestasis SERPINA1
Seizure-like/spasm activity. Cluster of infantile spasms SCN1A
Apnea, cyanosis, posturing, abnormal EEGTetrasomy for 15q1.2q13.1
Cardiomegaly, heart block, prolonged QT interval, respiratory failure POLR1C
Myelomeningocele, congenital hydrocephalus CELSR1
Preterm pulmonary atresia with intact ventricular septum with sinusoids, poor weight gain, feeding intolerance, recurrent pneumonia
ACTG2
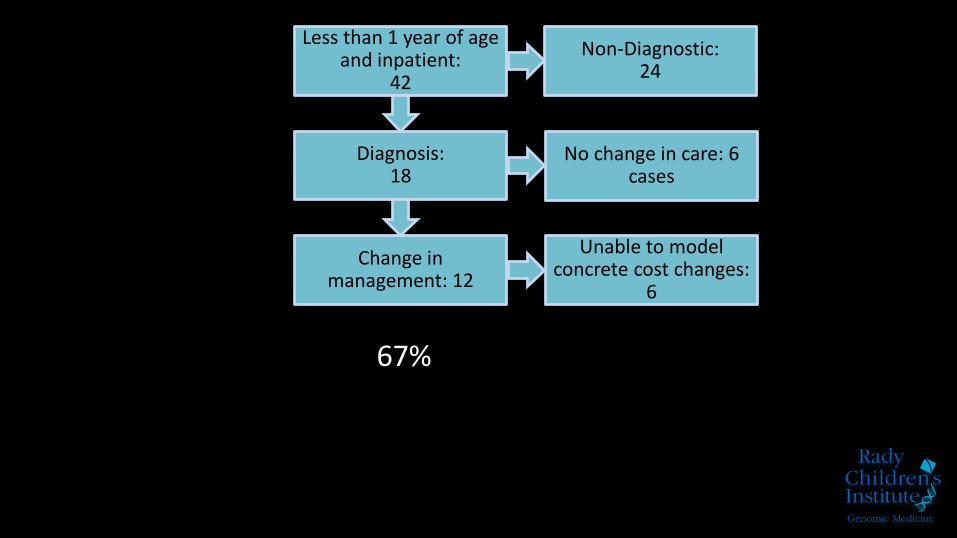
Less than 1 year of age and inpatient:
42
Diagnosis:18
Change in management: 12
Non-Diagnostic:24
No change in care: 6 cases
Unable to model concrete cost changes:
6
67%

Clinical Utility of Whole Genome and Exome Sequencing
NICU rWGS
NICU rWGS

Presentation Etiology Outcome
Infantile Spasms, hypertonia, esotropia, poor weight
gainGABRA1 Appropriate seizure medication
Hydrops fetalis, cardiomyopathy TPM1
LSD and arythmogenic
cardiomyopathy excluded –
proceeded with heart transplant
Complex partial epilepsy PCDH19
Switched to targeted therapy
and referred for research
protocol
IUGR, Compex cardiac disease, vertebral
segmentation defect, GU anomaliesPHEX
Medication started to prevent
rickets
Hirschprung’s disease, congenital ileal stenosis RETComprehensive surgical
approach
Pulmonary atresia, osteopenia, frequent unexplained
fevers. NF1
Pre-emptive management of
extra cardiac disease
Congenital hyperinsulinemia, bilateral ventricular
hypertrophy & left ventricular outflow tract obstructionABCC8 Targeted surgery, preventing DM
Presentations of cases with diagnosis & change in care

Less than 1 year of age and inpatient:
42
Diagnosis:18
Change in management: 12
Change in management possible
to model: 5
Prospective Change in care: 4
Retrospective care model: 2
Non-Diagnostic:24
No change in care: 6 cases
Unable to model concrete cost changes:
6

Cost savings from care avoided as a result of WGS
Case Cost avoided Cost saving
NPC1Avoided biopsies and one hospitalization, started
precision medicine$54,000
ARID1B Multiple unnecessary surgeries, ECMO etc. $1,410,000
KCNQ2 Shortened hospital stay, avoided neurologic damage $129,000
ARID1B Avoided prolonged hospitalization for IV antibiotics $269,000
JAG1 Kasai surgery avoided $36,000
NEB Muscle biopsy avoided $10,000
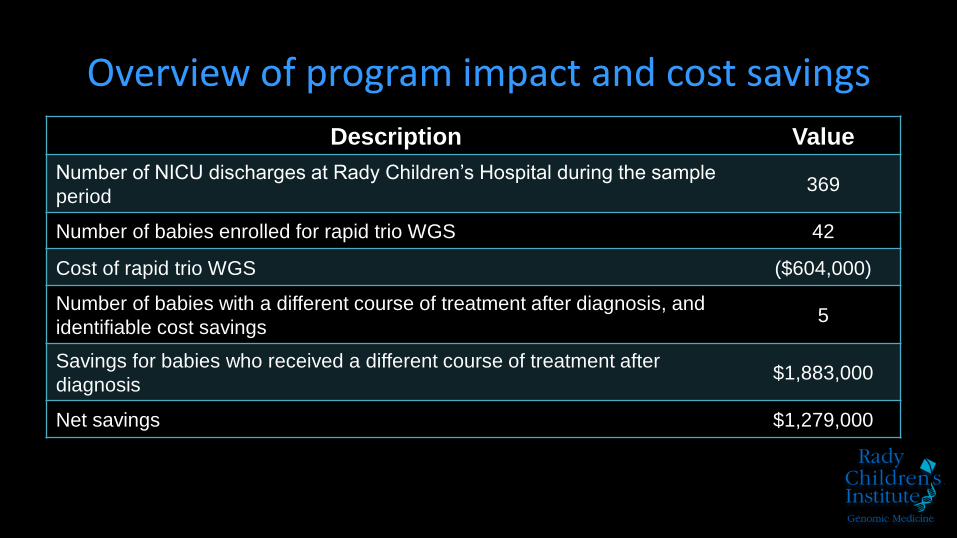
Overview of program impact and cost savings
Description Value
Number of NICU discharges at Rady Children’s Hospital during the sample
period369
Number of babies enrolled for rapid trio WGS 42
Cost of rapid trio WGS ($604,000)
Number of babies with a different course of treatment after diagnosis, and
identifiable cost savings5
Savings for babies who received a different course of treatment after
diagnosis$1,883,000
Net savings $1,279,000

Conclusions
• 49% of 125 NICU/PICU infants received diagnoses by rapid WGS
• Rapid WGS returned results faster than standard tests
• 39% of 93 NICU/PICU infants had a change in care as a result of rapid WGS
• Cost savings $30,450 per family tested

“The most significant breakthrough in healthcare in the past 40 years”
GENOME SEQUENCING
GOINGBIG
FOR
THE
LITTLE
ONES

Improved outcomesEmpowered families
Cost effectiveness
NovaSeq
Mum DadBaby

Newborn Sequencing In GenomicMedicine and Public Health

The LORD is my creativity, Psalm 27
• Josh Petrikin• Laurel Willig
• Carol Saunders• John Lantos
• Neil Miller• Emily Farrow
• Todd Laird• Joe Gleeson, MD, PhD• Julie Cakici• Ray Veeraraghavan,
PhD• Jennifer Azares• Vanessa Wertheim, PhD• Shareef Nahas, PhD
• David Dimmock, MD• Julie Reinke• Yan Ding, MD• Michelle Clark, PhD• Wendy Benson• Matt Bainbrindge, PhD• Sergei Batalov, PhD• Shimul Chowdhury PhD
• Patrick Mulrooney• Olivia Simonides• Daeheon "Danny" Oh• Catherine Yamada• Jennifer Silhavy,• Matthew Bainbridge,
PhD • Lisa Salz
• Lance Prince, MD, PhD• Farhad Imam, MD, PhD• Nicole Coufman, MD,
PhD• Julie Ryu, MD• George Chiang, MD• James Perry, MD
• Jenni Friedman, MD• Tina Chambers, PhD• Jeff Neul, MD, PhD• Lauge Farnaes, MD, PhD• Gail Knight, MD• Nathaly Sweeney, MD• Cynthia Kuelbs, MD
• Lynn Byrd, MD• Amber Hildreth, DO• Jonathan Sebat, PhD• Albert Oriol• Cyndi Kuelbs, MD• Bruce Barshop, MD
• Kevin Hall, PhD• James Richardson• Kyle Farh, MD• Susan Tousi• Ryan Taft, PhD
• Severine Catreux• Mike Ruehle
Support:• Rady Children’s Institute for
Genomic Medicine • NICHD• NHGRI• NIDDK• Illumina

The children are waiting….