imaging of pulmonary embolism - afiim.com · imaging of pulmonary embolism state of the art salah...
TRANSCRIPT

Imaging ofPulmonary embolism
State of The art
Salah D. Qanadli, MD, PhD
Cardiothoracic and Vascular UnitQuantitative Imaging Lab
Department of Radiology, CHUV, Lausanne, SwitzerlandAFIIM Annual Meeting, Paris, March 2010
14 March 2010

Clinical profile of VTED
•Incidence– US: 500 000 /yr– Fr: 100 000 /yr
•Prevalence– Clinically suspected PE
• Mean prevalence: 20 %• Prevalence range : 8-67% !*/**
•Mortality- M3 (untreated): 15-30%***- Y1 (treated): 1.5 %**** *Kearon C, CMAJ, 2003
**Perrier A et al., Arch Intern Med, 2000***Carson JL, NEJM, 1992Siddique RM et al., Arch Intern Med, 1996****Douketis JD et al., JAMA, 1998
Learning objectives
• Diagnosis of PE/VTED• Prognosis of PE/VTED• Alternative diagnoses• Associated diagnoses
• Triage of Acute Chest Pain

Learning objectives
• Diagnosis of PE/VTED• Prognosis of PE/VTED• Alternative diagnoses• Associated diagnoses
• Triage of Acute Chest Pain

• Sensitivity- > 90%
• Specificity- >90%
Performances du CTA
Subramanian RM et al., Aust Radiology, 2006Schoepf U et al., Radiology, 2004


Clinical probability of VTED
• Wells score• Geneva and modified (revised) Geneva Scores
2 6Intermediate HighLowStein P et al. N Engl J Med 2006

VTED markers
• D-dimers– Current strategy (2008) in Emergency Department (Out-patients)
• Low and Intermediate probability*– Negative tests exclude VTED (NPV 100%)
• High probability**– Limited adding value of D-dimers in diagnostic strategy
» other investigations recommended
*Di Nisio M et al., J Thromb Haemost 2007Kearon C et al., Ann Intern Med 2006**Kruip MJ et al., J Intern Med 2006Righini M et al., J Thromb Haemost 2004

Inconclusive CTA

Inconclusive CTA

Inconclusive CTA
• Isolated sub-segmental PE– Clinical significance
• Outcome of Negative CTA– Metaanalysis
• NPV 99% !• Comparable to negative transcatheter pulmonary angiography
Prologo et al., AJR 2005Eyer BA et al., AJR 2005Quiroz R et al., JAMA, 2005Moores LK et al., Ann Int Med, 2004

CT phlebography
•Diagnostic– CTP vs US - Combined CTA/CP: 15 à 35%
•Limits- Radiation exposure
- x500 à 2000 !!
- NON recommended for young patient (<40 years)
Loud PA et al., AJR 2000Subramaniam RM et al, Aust Radiology, 2006


Clinical value of CTA/CTP
• Current diagnosis strategies of PE/VTED !– Level 1: Clinical probability– Level 2: CTA/D-dimers– Level 3: CTP/US

Clinical value of CTA/CTP
• Diagnosis of PE/VTED• Prognosis of PE/VTED• Alternative diagnoses• Associated diagnoses
• Triage of Acute Chest Pain

PE Severity assessment
• Clinical assessment– PESI
• Laboratory testing
• Imaging

PE Severity pathophysiology

RVD assessment
• Echocardiography– Dilatation
• absolute value (cut off)• Relative ratio (RV/LV)
– Hypokinesia
• CTA (CMR)– Relative ratio (RV/LV)
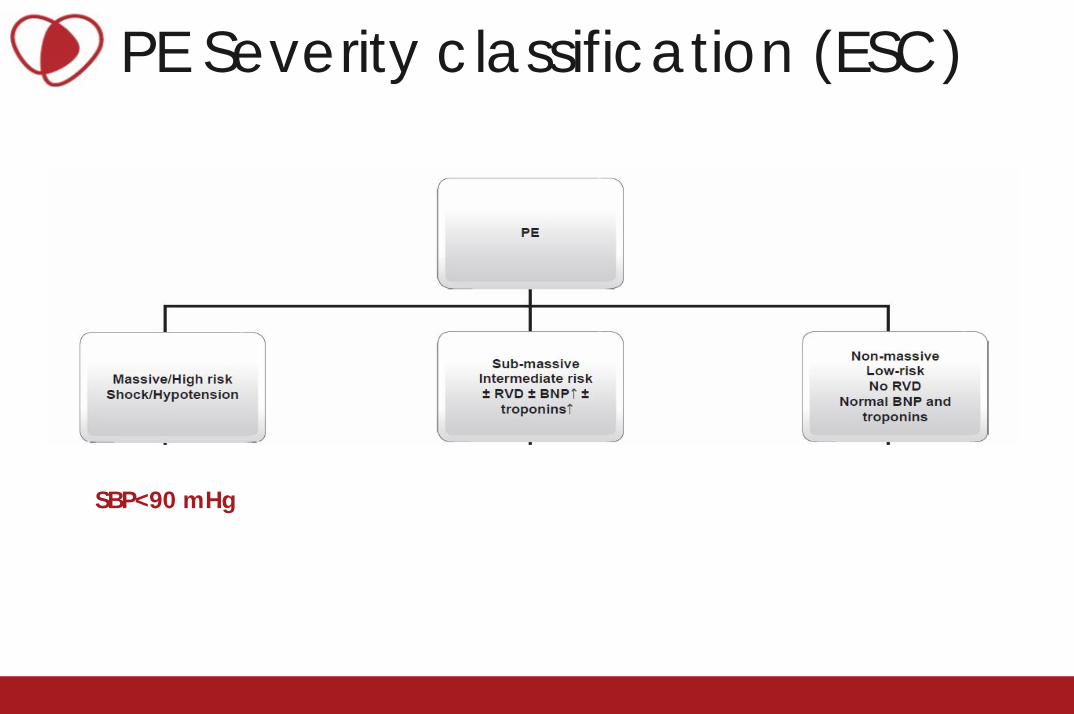
PE Severity classification (ESC)
SBP<90 mHg

Pulmonary Embolism Severity Index (PESI)
Aujesky et al. AJRCCM 2005; 172: 1041-6

PE Severity assessment
• Laboratory testing– Blood gas analysis: PaO2– D-dimers– Troponin I and/or T– Natiuretic Peptides (NP)
• BNP• Pro BNP
– H-FABP
– Myoglobin– Growth differentiation factor-15

Assessment of PE severity
• Non controversial findings– Cardiac CT measurements
– RV/LV» Threshold: 0.9
• Controversial findings- Arterial obstruction quantification (CTOI)
- Bankier et al.- Qanadli et al.- Mastora et al.- Ghanima et al.
- Others


Axial view 4-Chambers viewKamel EM, ,Qanadli SD, JCAT 2007

Prognostic value of right ventricular dysfunction for mortality in patientswith pulmonary embolism without shock
Sanchez O et al. Eur Heart J 2008;29:1569-1577

CT RVD valueTest
Echocardiography Computed tomography BNP Pro-BNP Cardiac
troponin
Sensitivity (%) (95% CI) 70 (46–86) 65 (35–85) 88 (65–96) 93 (14–100) 81 (23–100)
Specificity (%) (95% CI) 57 (47–66) 56 (39–71) 70 (64–75) 58 (14–92) 84 (77–90)
Negative predictive value (%) (95% CI)
60 (55–65) 58 (51–65) 76 (73–79) 81 (65–97) 73 (68–78)
Positive predictive value (%) (95% CI)
58 (53–63) 57 (49–64) 67 (64–70) 63 (50–76) 75 (69–80)

Io=3/40(7,5%)
Io=20 / 40(50 %)
Qanadli SD et al., AJR, 2001
Io = Σ (n.d)

CT obstruction index value
• Wu e al. 2004 (n=59)• Van der Meer et al. 2005 (n=120)
• Araoz et al. 2003 (n=173)• Ghaye et al. 2006
• Qanadli et al. RSNA (intermediate results 2008)
Van der Meer et al. Radiology 2005Wu et al. Radiology 2004Ghaye et al., Radiology, 2006Araoz J Thorac Imaging

CT obstruction index value
• CTOI Qanadli et al.• Linear (good to very good) correlation
• Pa02• RVD• D-dimers• Troponin• CT Perfusion
Ghanima et al. J Intern Med 2007Qanadli et al. AJR 2001Massoti et al. J Intern Med 2007Muller-Bardoff et al. Clin Chem 2002Chae, E. J. et al. Am. J. Roentgenol. 2010

Dual Energy CT pulmonary perfusion
Chae, E. J. et al. AJR 2010

Dual Energy CT pulmonary perfusion
Chae, E. J. et al. AJR 2010
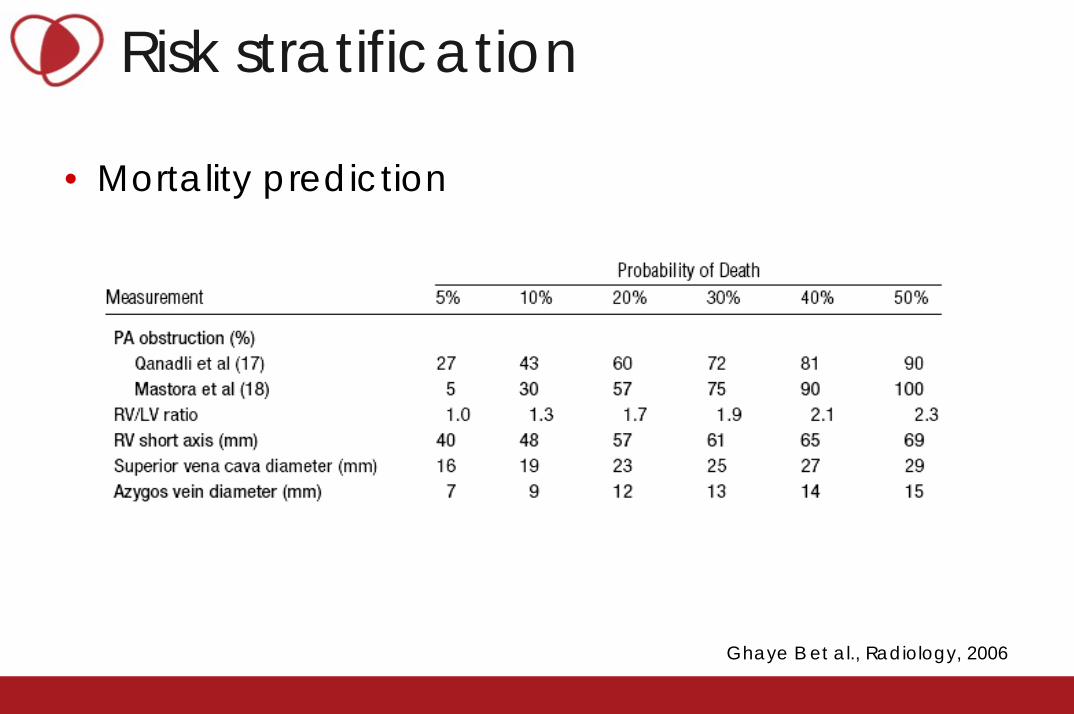
Risk stratification
• Mortality prediction
Ghaye B et al., Radiology, 2006

Over-estimation of RV/LV diameters
Obstruction Index=5%RV/LV=1.1
(pre-existing right ventricular dilatation)

Under-estimation of RV/LV diameters
Obstruction Index=40%RV/LV=0.85
(pre-existing left ventricular dilatation)

PE Severity pathophysiology

Risk stratificationDecision therapeutic making
>15% <3%

Clinical value of CTA/CTP
• Diagnosis of PE/VTED• Prognosis of PE/VTED• Alternative diagnoses• Associated diagnoses
• Triage of Acute Chest Pain

Adding clinical value of CTA
• Alternative diagnosis– Occurrence: > 50 %* (> 35 %)
• Pneumonia• Acute aortic disorders• Heart failure• Pleural effusion• Cancer…
– M3-Follow up• unchanged in 94,6%**
• Associated diagnosis***
*Garg et al, AJR, 1999**van Stirjen MJ et al., J Thromb Haemost, 2005***McKie SJ et al., Clin Radiol, 2005


Clinical value of CTA/CTP
• Diagnosis of PE/VTED• Prognosis of PE/VTED• Alternative diagnoses• Associated diagnoses
• Triage of Acute Chest Pain

Acute Chest Pain
??
?
?
AAS PE
ACS

Acute Chest Pain
2%
9%
6%
AAS PE
ACS
Al Qahtani S, et al., submitted for publication

Take Home Messages• Imaging
– Integrative diagnostic tool of PE in Emergency Departments
• Combined CTA/CTP recommended for patients > 40 years-old
• CTA reporting should include- Assessment of the PE severity
- RV/LV- CTOI
• Integration of CTA in the triple rule out concept needs– More clinical evaluation – More technical improvement (radiation exposure)

Good judgment is based on experienceand
experience is based on bad judgment
Martin J. Lipton