imaging in multiple ring enhancing brain lesions
TRANSCRIPT

MULTIPLE RING ENHANCING BRAIN LESIONS
PRESENTED BYDR SUMIYA ARSHAD

CASE PRESENTATION
Patient Perveen 29 years of age presented with complains of: Headache Imbalance gait
She was a suspected case of tuberculous meningitis and tuberculomas
Known case of pulmonary TB. On ATT for past 01 year MRI brain with contrast was performed

MRI BRAIN WITH CONTRAST
Multiple variable size supra tentorial brain parenchymal lesions larger one in right sided temporal lobe is seen extending inferiorly and involving right aspect of mid brain causing minimal pressure effect. It is shows heterogeneous hypointesnisty on T2WI within it.
Another lesion in deep temporal lobe anteriorly Similar intensity variable lesions seen in left sided temporal lobe. These lesions show post contrast ring enhancement. Right sided leptomeningeal thickening is noted along side the sylvian
fissure.




CONCLUSION
Multiple supratentorial parenchymal lesions with the larger one in right temporal lobe extending inferiorly to involve the mid brain with post contrast ring enhancement --- suggestive of multiple tuberculomas keeping in view the history of tuberculosis.
INTRODUCTION
Multiple ring enhancing lesions are a commonly encountered neuroimaging abnormality.
Can be caused by a variety of infectious, neoplastic and inflammatory diseases.
Distinguishing between neoplastic and non neoplastic etiology is extremely important because a misdiagnosis can lead to unwarranted neurosurgery and exposure to toxic chemotherapy or potentially harmful brain irradiation.
CLINICAL FINDINGS
Clinically, they manifest as: recurrent seizures
visual impairment
focal neurological deficit
Signs of raised intracranial pressure (severe headache, vomiting and papilledema).
If cerebral edema is severe, patients may develop loss of sensorium and posturing of limbs because of transtentorial brain herniation.

DIFFERENTIAL DIAGNOSISINFECTIVE Tuberculomas Pyogenic abscess Neurocysticercosis Echinococcus infection Amebic brain abscess
NEOPLASTIC Metastases Glioblastoma Primary CNS lymphoma
INFLAMMATORY & DEMYELINATING Tumefactive multiple sclerosis ADEM Radiation necrosis

In developing and poor countries, the spectrum of etiologies of multiple ring-enhancing lesions of the brain is likely to be different from developed countries; as infective pathologies are more frequently encountered.
TUBERCULOMAS Central nervous system (CNS) tuberculosis (TB) is a serious form of
TB, due to haematogenous spread of Mycobacterium tuberculosis (MT).
Represent a common neurological disorder in developing countries, accounting for 10% to 30% of all intracranial masses
Intracranial tuberculomas are the least common presentation of CNS TB and can occur with or without tuberculous meningitis.
Numerous small tuberculomas are common in patients with miliary pulmonary tuberculosis.
The diameter of these lesions usually ranges from 1 mm to 5 cm.
CLINICAL FEATURES
Tuberculomas often present with symptoms and seizures, signs of raised intracranial pressure and focal neurological deficit without evidence of systemic disease.

RADIOGRAPHIC FEATURESCT SCAN
Hypo to iso dense lesions are seen with edema and necrosis appearing as a low attenuating area on CT scan.
Once the granuloma has begun to organize, there may be high attenuation, contrast enhancement and calcification, as well as ring enhancement and a variable degree of surrounding edema.
The enhancement may be homogenous or there may be a central radiolucent area corresponding to the central zone of necrosis.

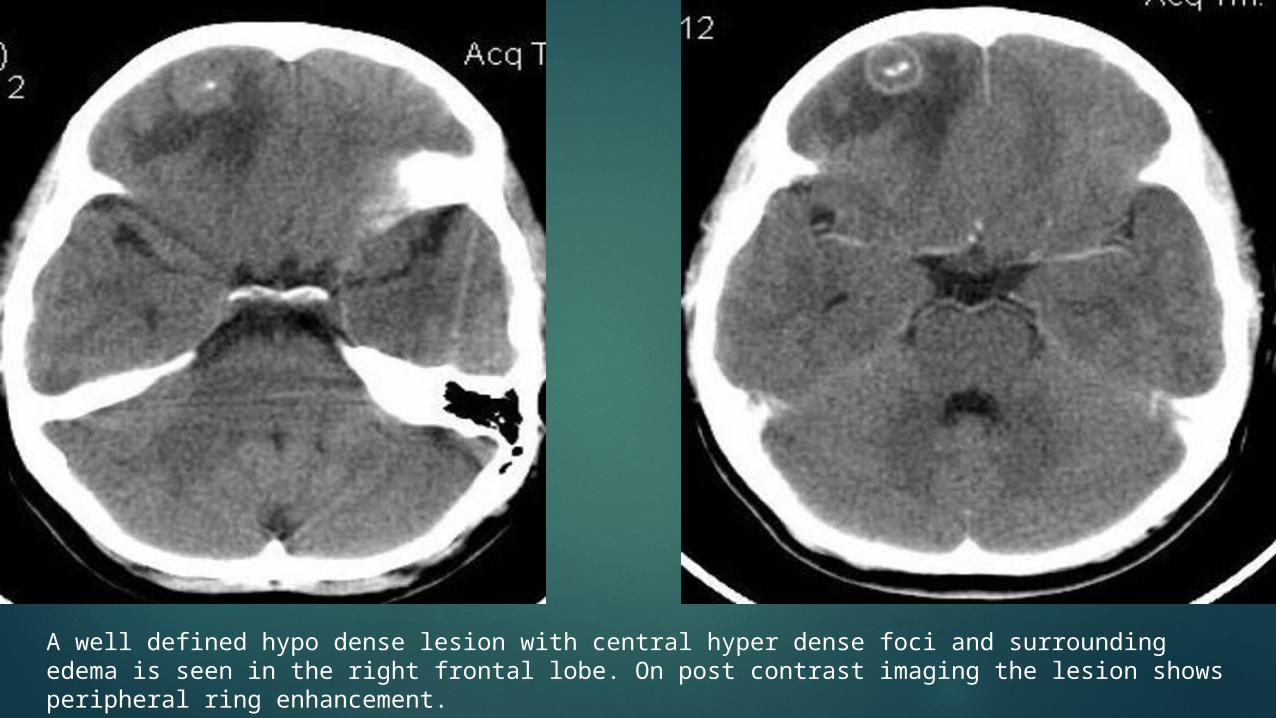
A well defined hypo dense lesion with central hyper dense foci and surrounding edema is seen in the right frontal lobe. On post contrast imaging the lesion shows peripheral ring enhancement.
MRI T1WI
Iso intense to grey-matter may have central region of hyper intensity representing caseation
T2WI Iso intense to grey-matter may have central region of hypo intensity representing gliosis and
abundant monocyte infiltration lesions are surrounded by vasogenic edema
T1 C+ (Gd) usually appears as ring-enhancement may appear as a conglomerate enhancing mass

ENHANCEMENT PATTERNS
Tuberculomas on contrast administration appear as nodular or ring-like enhancing lesions.
Tuberculomas frequently show varied types of enhancement, including irregular shapes, ring-like shapes, open rings and lobular patterns. Target-like lesions are common.

PYOGENIC BRAIN ABSCESS Potentially life threatening condition requiring prompt diagnosis
and treatment. Results from pathogens growing within the brain initially as
cerebritis, then later demarcating into cerebral abscess. Haematogenous spread is recognized as the most common source.
Risk factors include: congenital heart diseases, endocarditis, IV drug abusers, lung abscess, empyema thoracis, Sino nasal infections, dental abscess and systemic sepsis.
RADIOGRAPHIC FEATURESCT SCAN
Pre and post contrast scans should be obtained. Typical appearance includes: Ring of iso or hyper dense tissue of uniform thickness
representing capsule of the abscess which show ring enhancement on post contrast scans.
Some mass effect, usually not as marked in relation to the extent of edema.
Ventriculitis --- bad prognostic sign; enhancement of ependymal. Obstructive hydrocephalus due to ventricular spread may occur.
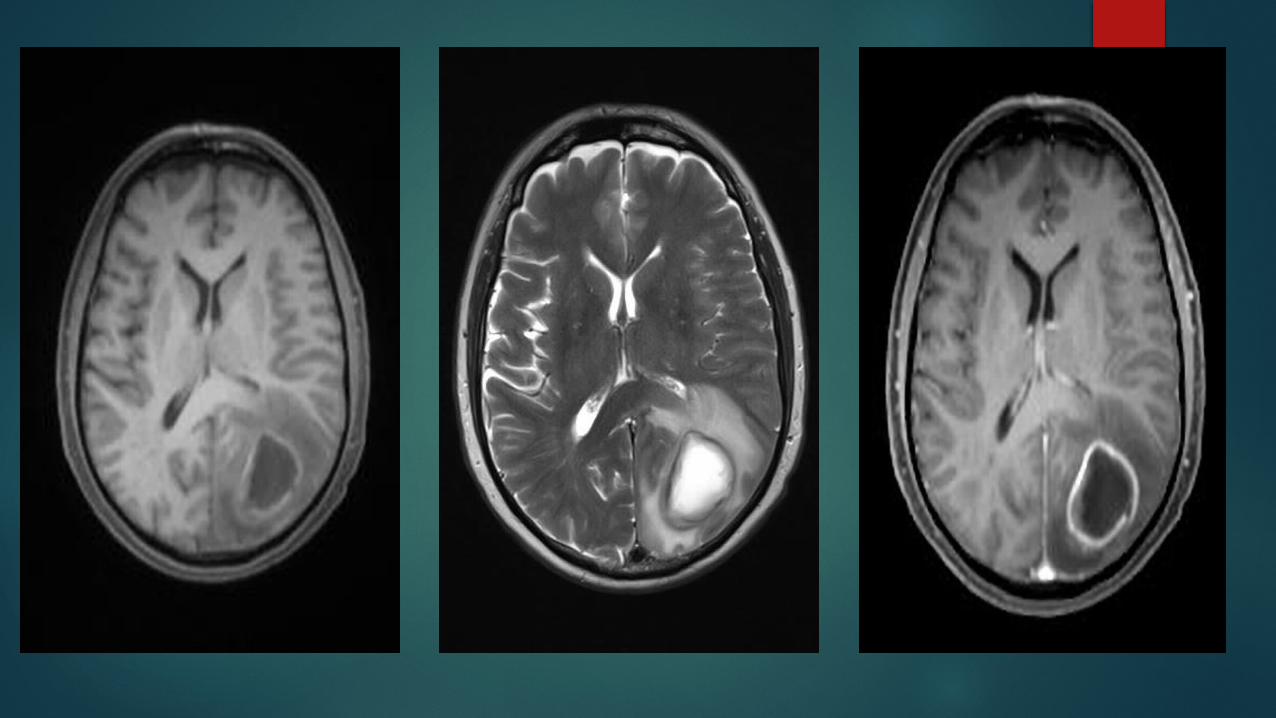
MRIT1WI The central zone of liquefying necrosis in a mature abscess is
slightly hyper intense to CSF. Peripheral low intensity --- vasogenic edema. Capsule is commonly iso to slightly hyper intense to brain
parenchyma. Significant post contrast ring enhancement.T2WI Iso to hypo intense to CSF, does not attenuate on FLAIR. Peripheral high intensity --- vasogenic edema. Capsule --- intermediate to low signal thin rim.

NEUROCYSTICERCOSIS
Caused by CNS infection with pork tape worm Taenia Solium.
There is a variable time interval between the point of infection and the onset of symptoms ranging from 1-30 years.
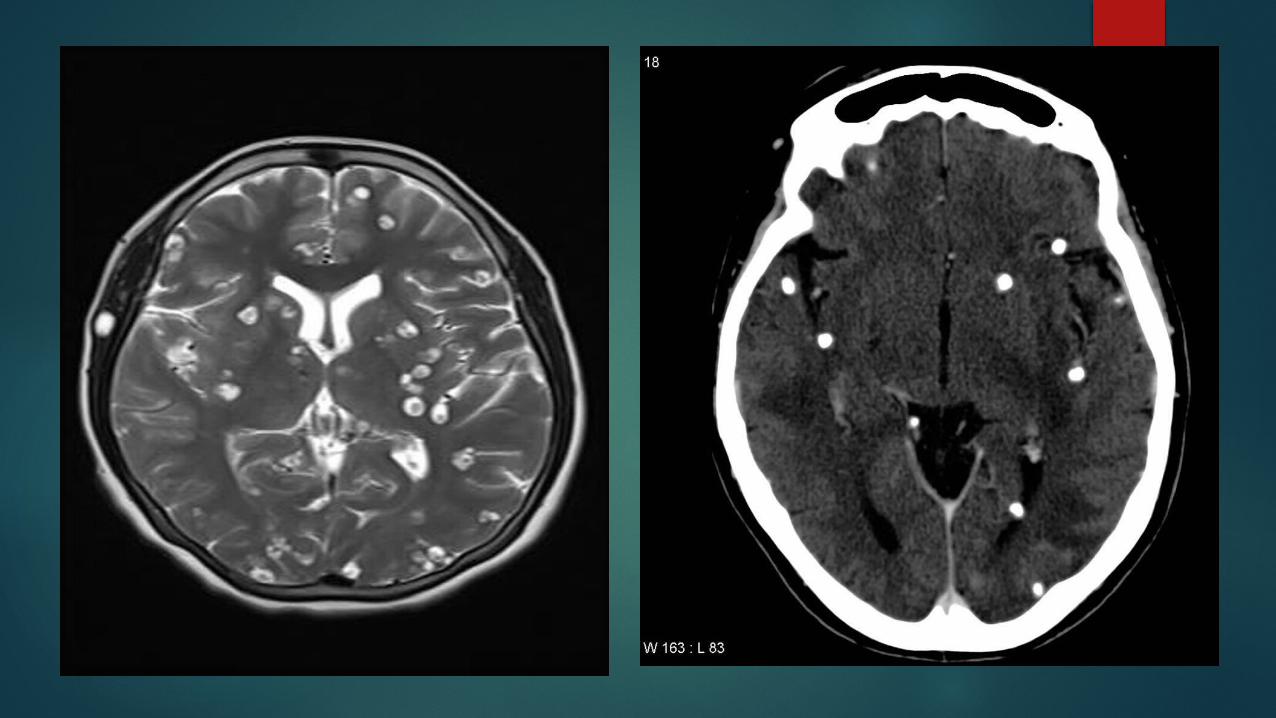
Can be both intra or extra axial. Commonest locations are: subarachnoid space over the cerebral hemispheres, parenchyma, basal cisterns, ventricles.
Usually, the lesions are <20 mm in diameter. The lesions are often multiple and most often do not have extensive oedema.
RADIOGRAPHIC FETURES Extra-intestinal infection undergoes specific imaging changes as
it progresses through four stages of infection. Imaging findings depend upon location and stage of infection.
VESICULAR STAGE: Cyst with dot sign
CSF intensity
Hyper intense scolex on T1 can be seen sometimes
No enhancement is typical, however faint enhancement of the wall and the scolex can be seen.

COLLOID VESICULAR STAGE : Cyst fluid becomes turbid
CT = hyper attenuating to CSF MRI T1WI = hyper intense to CSF
Surrounding edema Cyst and the wall become thickened and brightly enhances. Scolex can still be seen as a eccentric focus of enhancement.
GRANULAR NODULAR:• Edema decreases• Cyst retracts• Enhancement persists but is less marked.

NODULAR CALCIFIED:• End stage calcified cyst remnant• No edema• No enhancement• Signal drop out on T2WI• Some intrinsic high T1v signal may be present

METASTASES Brain metastases are estimated to account for approximately 25-50% of
intracranial tumors in hospitalized patients. Due to great variation in imaging appearances, these metastases present a
common diagnostic challenge. 80% of brain metastases can be accounted for by five primary tumors :
• lung cancer
• renal cell carcinoma
• melanoma
• breast cancer
• GI tract adenocarcinoma majority being colorectal CA.
80% of metastases localize to the cerebral hemispheres, 15% localize to the cerebellum and 3% localize to the basal ganglia.
Macroscopically metastases are relatively well demarcated from the surrounding parenchyma and usually there is a zone of peritumoural edema out of proportion with the tumor size.

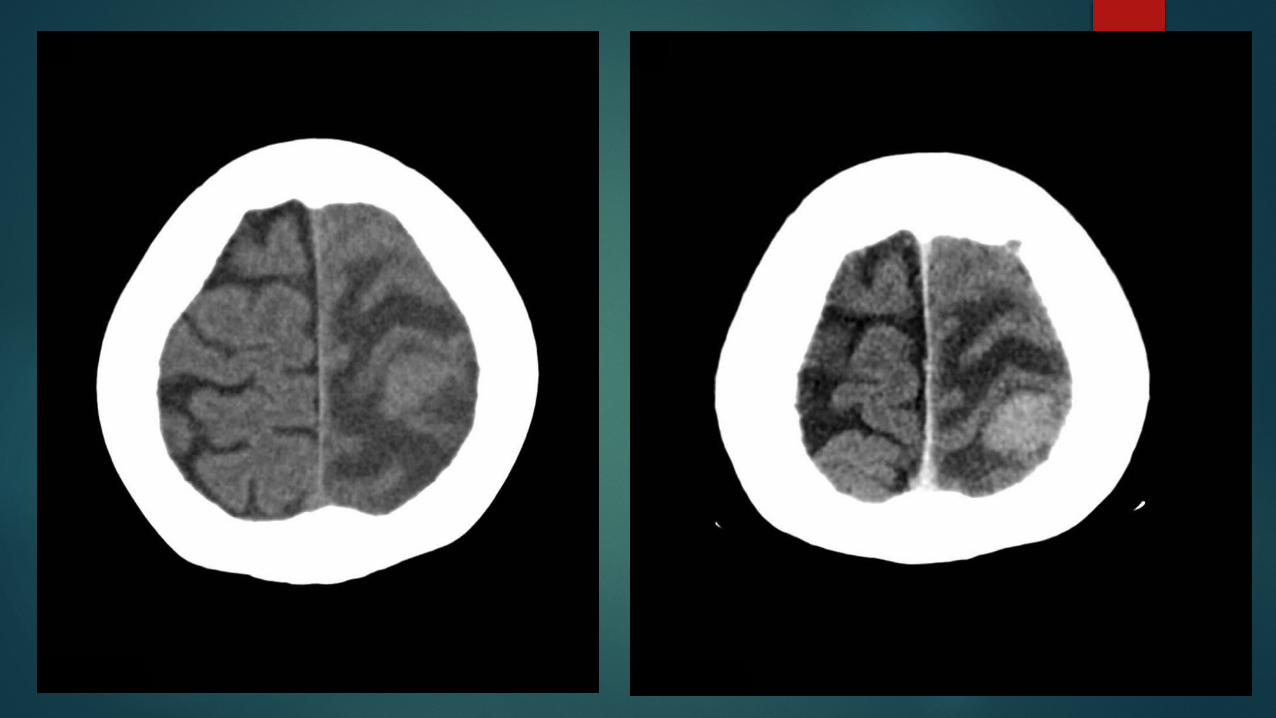
RADIOGRAPHIC FEATURESCT SCAN
PRECONTRAST IMAGING:
the mass may be iso dense, hypo dense or hyper dense (classically melanoma) compared to normal brain parenchyma with variable amounts of surrounding vasogenic edema.
POST CONTRAST:
enhancement is also variable and can be intense, punctate, nodular or ring-enhancing if the tumor has out grown it's blood supply.
MRI T1
• typically iso to hypo intense• if hemorrhagic may have intrinsic high signal• non-hemorrhagic melanoma metastases can also have intrinsic high
signal due to the paramagnetic properties of melanin T2
• typically hyper intense• hemorrhage may alter this
FLAIR• typically hyper intense• Hyper intense peritumoural edema of variable amounts
T1C+• enhancement pattern can be uniform, punctate, or ring-enhancing,
but it is usually intense• delayed sequences may show additional lesions, therefore contrast-
enhanced MR is the current standard for small metastases detection


GLIOBLASTOMA
Glioblastoma (GBM) is the most common adult primary intracranial neoplasm.
Carries the worst prognosis (WHO grade IV). These tumors are multifocal in 20% of patients and are rarely
multi centric. Usually occur after the age of 40 years with a peak incidence
between 65 and 75 years of age. There is a slight male preponderance with a 3:2 M:F ratio. Caucasians are affected somewhat more frequently than other
ethnicities.

Glioblastomas are typically poorly marginated, diffusely infiltrating necrotic masses localized to the cerebral hemispheres. The supratentorial white matter is the most common location.
Infiltration beyond the visible tumor margin is always present.

RADIOGRAPHIC FEATURESCT SCAN
Irregular thick margins: iso to slightly hyper attenuating (high cellularity).
Irregular hypo dense center representing necrosis Marked mass effect Surrounding vasogenic edema Hemorrhage occasionally seen Calcification is uncommon Intense irregular, heterogeneous enhancement of the margins is
almost always present
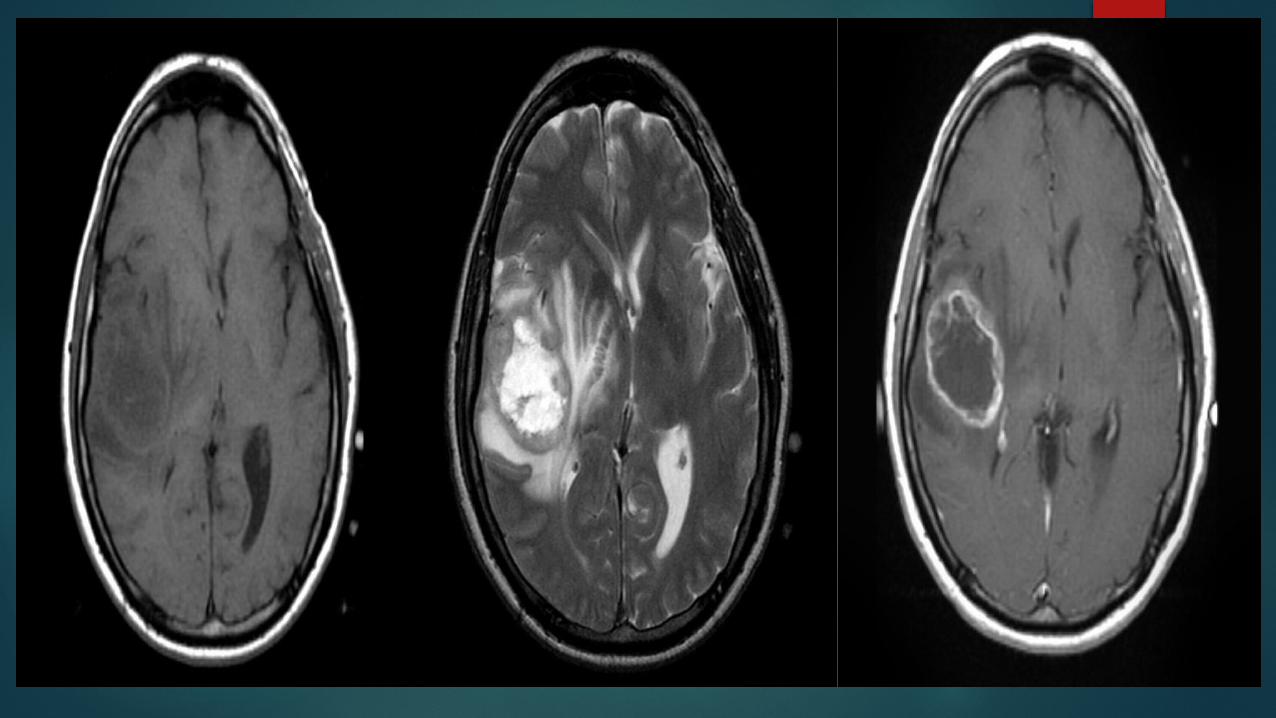
MRI T1
• hypo to iso intense mass within white matter• central heterogeneous signal (necrosis, intra tumoral hemorrhage)
T2/FLAIR• Hyper intense• surrounded by vasogenic edema• flow voids occasionally seen
T1 C+ (Gd)• enhancement is variable but is almost always present• typically peripheral and irregular with nodular components• usually surrounds necrosis

TUMEFACTIVE MULTIPLE SCLEROSIS
Tumefactive multiple sclerosis is a term used to describe patients with established multiple sclerosis who develop large aggressive demyelinating lesions.
Most frequently encountered in women, usually young middle age. It is a separate entity then Tumefactive demyelinating lesions also
sometimes called mono focal acute inflammatory demyelination (MAID), is a locally aggressive form of demyelination, usually manifesting as a solitary lesion; greater than 2 cm that may mimic a neoplasm on imaging.
TMS and TDL have similar radiological appearance with different clinical picture.
RADIOGRAPHIC FEATURESCT SCAN
Tumefactive multiple sclerosis plaques appears as hypo attenuating lesion with ill-defined ring enhancement, central necrosis, perilesional edema and minimal mass effect.

MRI Tumefactive demyelinating lesions tend to be large but with
relatively little mass effect or surrounding edema.
T1 C+ (Gd)• about half of tumefactive demyelinating lesions demonstrate
contrast enhancement.• the enhancement pattern is usually in the form on an open ring and
the incomplete portion of the ring is on the gray matter side of the lesion


CONCLUSION Multiple ring enhancing lesions are a commonly encountered
neuroimaging abnormality. Distinguishing between neoplastic
and non neoplastic etiology is extremely important.
Many features of the lesion as well as clinical presentation and
patient demographics need to be taken together to help narrow
the differential.

Helpful rules of thumb include: Enhancing wall characteristics
• thick and nodular favors neoplasm
• thin and regular favors abscess
• incomplete ring often opened toward the cortex favors demyelination
• intermediate to low T2 signal capsule favors abscess
• restricted diffusion of enhancing wall favors GBM or demyelination
Surrounding edema• extensive edema relative to lesion size favors abscess
• increased perfusion favors neoplasm (metastases or primary cerebral malignancy)

Central fluid content• restricted diffusion favors abscess
• absence of diffusion restriction favor a tumor with a central necrotic component (classically a metastases)
Number of lesions• similar sized rounded lesions at grey white matter junction favors metastases or
abscesses
• irregular mass with adjacent secondary lesions embedded in the same region of 'edema' favors GBM.
• small (<1-2cm) lesions with thin walls especially if other calcific foci are present suggest Neurocysticercosis.

THANK YOU
?