imaging children with acute abdominal pain -- -- role ...€¦ · imaging children with acute...
TRANSCRIPT

Imaging Children with Acute Imaging Children with Acute Abdominal Pain Abdominal Pain ---- Role/Protocols of US, CT, MRRole/Protocols of US, CT, MR
Kimberly E. Applegate, MD, MS Kimberly E. Applegate, MD, MS Emory UniversityEmory University
March 2010
Financial disclosures: AIM (American Imaging Management) radiation protection advisory board;Springer book contract: Evidence-based Pediatric Imaging

EvidenceEvidence--based imaging based imaging approachesapproaches
((MalrotationMalrotation & & MidgutMidgut volvulusvolvulus))Pyloric Pyloric stenosisstenosisIntussusceptionIntussusceptionAppendicitisAppendicitis
Key surgical conditions:Key surgical conditions:

MalrotationMalrotationRare: 3.9 per 10,000 live births Rare: 3.9 per 10,000 live births birthsbirths90% age <1yr (75% neonatal)90% age <1yr (75% neonatal)Mortality 3Mortality 3--5%5%Associated syndromes, anomaliesAssociated syndromes, anomaliesDifficult diagnosis in older childrenDifficult diagnosis in older children

The UGI seriesThe UGI series Diagnostic PerformanceDiagnostic Performance
Imaging gold standardImaging gold standard15% FP 315% FP 3--6% FN6% FNVolvulusVolvulus: sensitivity 54%: sensitivity 54%

Question 1Question 1
3. How often is the 3. How often is the cecumcecum abnormally abnormally positioned in children with positioned in children with malrotationmalrotation??A. 20%A. 20%B. 50%B. 50%C. 80%C. 80%D. 100%D. 100%

Answer 1Answer 1
C. C. CecumCecum abnormally abnormally positioned in 80positioned in 80-- 85% of 85% of malrotationmalrotation casescases
•• LigamentousLigamentous laxity in children laxity in children •• False Positives:False Positives:
Liver transplantLiver transplantSpenomegalySpenomegalyDilated adjacent bowelDilated adjacent bowelEnteralEnteral tubestubes

Helpful tipsHelpful tips…… UGI techniqueUGI technique
Document first pass of barium through Document first pass of barium through duodenum duodenum Document DJJ on frontal Document DJJ on frontal andand laterallateralDo not overfill stomachDo not overfill stomachUse manual palpationUse manual palpationReview other imaging studiesReview other imaging studiesIf doubt, SBFT or enema If doubt, SBFT or enema cecumcecumIf clinical doubt, repeat UGIIf clinical doubt, repeat UGI

VolvulusVolvulusBowel gas pattern Bowel gas pattern in neonatesin neonates--““sad sausagessad sausages”” vsvs““happy polygonshappy polygons””
VolvulusVolvulus: a surgical emergency: a surgical emergency

Clinical presentation Clinical presentation in older childrenin older children
Tricky!Tricky!Rarely bilious emesisRarely bilious emesisLess specific symptomsLess specific symptomsLong average delays in diagnosis of Long average delays in diagnosis of 1.7 years to 5 years (3 published series) 1.7 years to 5 years (3 published series)

Special situationsSpecial situations
VolvulusVolvulus limited to the colonlimited to the colon
Neonates: distal transverse colonNeonates: distal transverse colon
Older children: Older children: cecalcecalHeterotaxyHeterotaxy syndromesyndromeParaduodenalParaduodenal herniasherniasAcquired Acquired volvulusvolvulus

HeterotaxyHeterotaxy syndromesyndrome malrotationmalrotation and annular pancreasand annular pancreas
Malrotation, ascites
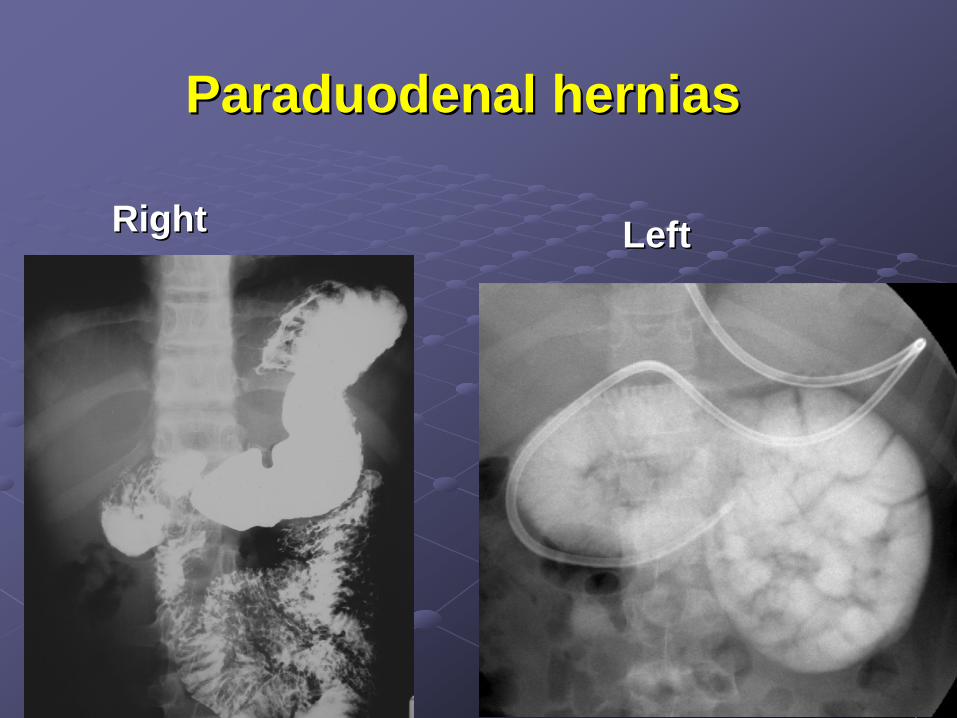
ParaduodenalParaduodenal herniashernias
RightRight LeftLeft

CecalCecal VolvulusVolvulus around MACEaround MACE MMalonealone aantegradentegrade ccatheterizableatheterizable eenemanema

Question 2Question 2
4. What is the most common cause of GI 4. What is the most common cause of GI obstruction in children?obstruction in children?A. Pyloric A. Pyloric StenosisStenosisB. B. IntussusceptionIntussusceptionC. AppendicitisC. Appendicitis

Answer 2Answer 2
A. Pyloric A. Pyloric StenosisStenosisIncidence: 2Incidence: 2--5 per 1,000 births5 per 1,000 birthsPeak age 4 wks (2Peak age 4 wks (2--12 wks)12 wks)
IntussusceptionIntussusception is 2is 2ndnd most commonmost commonAppendicitis most common Appendicitis most common abdabd surgerysurgery
SBO rareSBO rare---- perforated appendicitis (1perforated appendicitis (1--2%)2%)

Pyloric Pyloric StenosisStenosisEarlier diagnosisEarlier diagnosisIncreased reliance on imagingIncreased reliance on imaging
ClinClin exam: exam: 72% 72% senssens, 97% spec, 97% spec
US exam: US exam: 97% 97% senssens, 100% spec, 100% spec

Question 3Question 3
5. Which of the following is NOT 5. Which of the following is NOT associated with pyloric associated with pyloric stenosisstenosis??A. Family historyA. Family historyB. Male genderB. Male genderC. PrematurityC. PrematurityD. Erythromycin D. Erythromycin

Answer 3Answer 3
C. PrematurityC. Prematurity
Male: female 4:1Male: female 4:1Mild increased incidence if family Mild increased incidence if family historyhistoryLate gestation or neonatal use of Late gestation or neonatal use of systemic erythromycin associated systemic erythromycin associated with PSwith PS

IntussusceptionIntussusceptionLack of seasonality but Lack of seasonality but
associated with multiple associated with multiple virusesvirusesPeak age: 5Peak age: 5--9 months (range 9 months (range
3mo3mo--4 yrs)4 yrs)10% spontaneous reduction10% spontaneous reduction10% recur (50% at 48hrs)10% recur (50% at 48hrs)5% lead points5% lead points
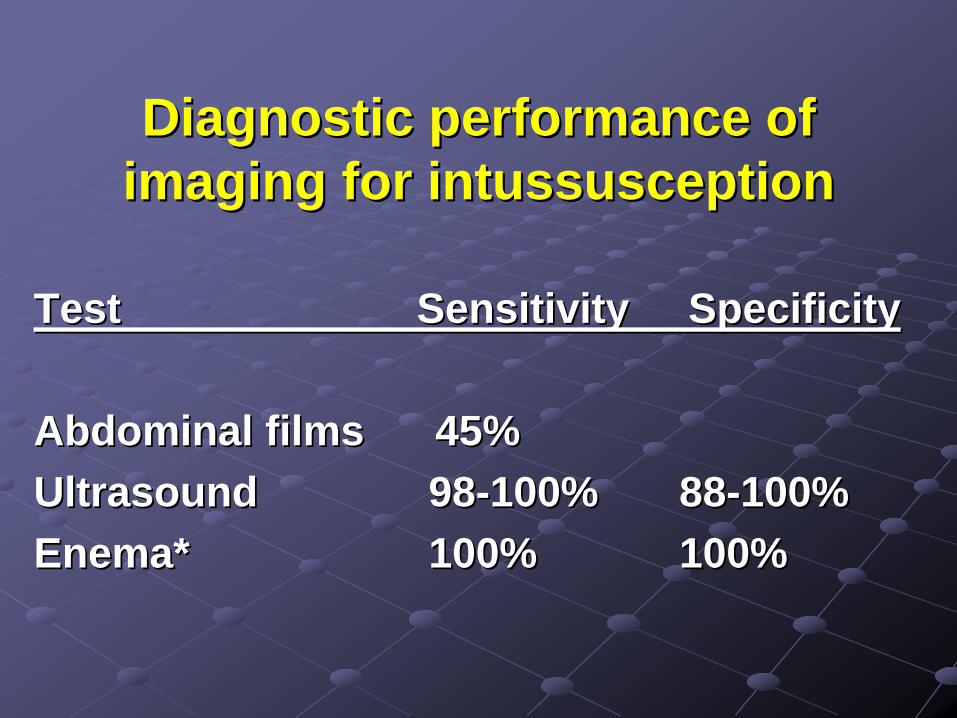
Diagnostic performance of Diagnostic performance of imaging for imaging for intussusceptionintussusception
TestTest Sensitivity SpecificitySensitivity Specificity
Abdominal films 45% Abdominal films 45% UltrasoundUltrasound 9898--100%100% 8888--100%100%Enema*Enema* 100%100% 100%100%

ReducibilityReducibility
#1: duration of #1: duration of symptomssymptoms
>48 hours>48 hoursAge <3 months, Age <3 months,
dehydration, SBOdehydration, SBOSonographySonography
Trapped fluidTrapped fluid
Lack of color Lack of color dopplerdoppler

BurkittBurkitt lymphoma withlymphoma withSmall bowel wall tumor seedingSmall bowel wall tumor seedingAnd And intussusceptionintussusception

Question 4Question 4 IntussusceptionIntussusception
6. 6. Which of the following enema Which of the following enema techniques has the highest reduction techniques has the highest reduction rate?rate?A. BariumA. BariumB. Iodinated contrastB. Iodinated contrastC. AirC. AirD. USD. US--guided Salineguided Saline
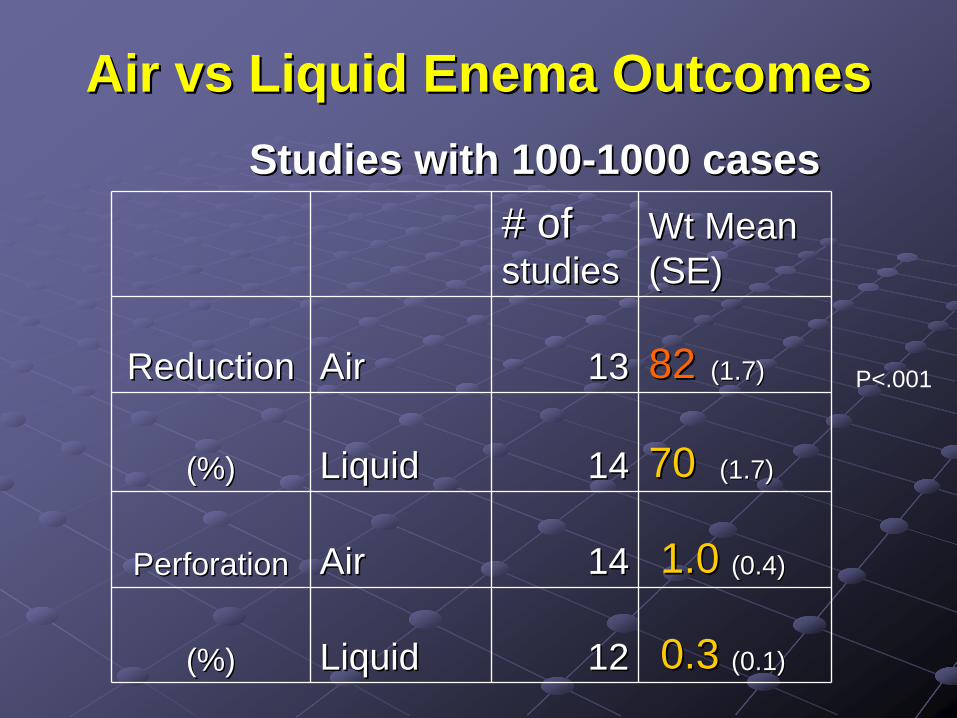
Air Air vsvs Liquid Enema OutcomesLiquid Enema Outcomes
# of # of studiesstudies
Wt Mean Wt Mean (SE)(SE)
ReductionReduction AirAir 1313 8282 (1.7)(1.7)
(%)(%) LiquidLiquid 1414 70 70 (1.7)(1.7)
PerforationPerforation AirAir 1414 1.0 1.0 (0.4)(0.4)
(%)(%) LiquidLiquid 1212 0.30.3 (0.1)(0.1)
Studies with 100Studies with 100--1000 cases1000 cases
P<.001

Are we getting better at enema Are we getting better at enema reduction? YES!reduction? YES!
MethodMethod 1980's1980's 1990's1990's 2000's2000'sReductioReductio
n Rate n Rate (%) (%) LiquidLiquid 6666 (5.6)(5.6) 72 (2.5)72 (2.5) 7979 (3.9)(3.9)
AirAir 7979 (2.9)(2.9) 83 (1.8)83 (1.8) 8686 (2.5)(2.5)PerforatiPerforati
on on Rate Rate (%) (%)
LiquidLiquid 0.4 (0.2)0.4 (0.2) 0.5 (0.3)0.5 (0.3) 0.4 (0.3)0.4 (0.3)
AirAir 00 1.3 (0.3)1.3 (0.3) 0.6 (0.4)0.6 (0.4)

Air Enema Air Enema IntussIntuss ReductionReduction
IntussusceptionIntussusception SummarySummary
SonographySonography for diagnosisfor diagnosisAir enema superior to liquidAir enema superior to liquidNo bariumNo bariumUSUS--guided saline enema avoids radiationguided saline enema avoids radiationDelayed repeat enema?Delayed repeat enema?

AppendicitisAppendicitisLifetime risk 7%Lifetime risk 7%>260,000 cases (70,000 children)/yr USA>260,000 cases (70,000 children)/yr USAPeak age 10Peak age 10--19 yrs (rare under 3 yrs)19 yrs (rare under 3 yrs)Clinical presentation overlaps benign Clinical presentation overlaps benign conditions (conditions (egeg, gastroenteritis) , gastroenteritis) Children poorly localize painChildren poorly localize pain

Question 4Question 4
7. What are the sensitivity and specificity 7. What are the sensitivity and specificity of CT for the diagnosis of acute of CT for the diagnosis of acute appendicitis in children?appendicitis in children?A. 90%, 90%A. 90%, 90%B. 95%, 90%B. 95%, 90%C. 90%, 95%C. 90%, 95%D. 95%, 95%D. 95%, 95%
Answer 4Answer 4D. 95% sensitivity and D. 95% sensitivity and
specificity for CTspecificity for CT
Similar accuracy to Similar accuracy to adults if performed adults if performed with meticulous with meticulous techniquetechnique

Imaging of appendicitis Imaging of appendicitis in childrenin children
CT false positives & negatives: 5%CT false positives & negatives: 5%Less fat, more difficult CT Less fat, more difficult CT dxdxCT > US in kids in USA since 2002!CT > US in kids in USA since 2002!CT appendix size cut point: >7mmCT appendix size cut point: >7mm

Question 5Question 5 What is the role of the What is the role of the vermiform appendix?vermiform appendix?
A.A. There is no known functionThere is no known functionB.B. There is a functionThere is a function

Answer 5Answer 5 ““BiofilmsBiofilms in the large bowel suggest an in the large bowel suggest an
apparent function of the human apparent function of the human vermiform appendixvermiform appendix..””
Parker W and Bollinger R. (Duke) J Parker W and Bollinger R. (Duke) J TheorTheor Biol. 2007;249(4):826Biol. 2007;249(4):826--31.31.““We propose that the human appendix is well We propose that the human appendix is well suited as a "safe house" for suited as a "safe house" for commensalcommensal bacteria, providing support for bacterial bacteria, providing support for bacterial growth and potentially facilitating regrowth and potentially facilitating re-- inoculation of the colon in the event that the inoculation of the colon in the event that the contents of the intestinal tract are purged contents of the intestinal tract are purged following exposure to a pathogen.following exposure to a pathogen.””

MDCT for AppendicitisMDCT for Appendicitis Many ApproachesMany Approaches
kV 120, kV 120, mAsmAs 5050--175175Avoid delayed or repeat imagingAvoid delayed or repeat imagingIV contrastIV contrastTrend of decreased use of Trend of decreased use of enteralenteral
contrastcontrast
Caveat: role of Caveat: role of enteralenteral contrast more important contrast more important in young children with little in young children with little intraperitonealintraperitoneal and and retorperitonealretorperitoneal fatfat
National push from Emergency Physicians to National push from Emergency Physicians to abandon oral contrast use to improve TAT abandon oral contrast use to improve TAT

CreatinineCreatinine in Childrenin Children Suggested cutSuggested cut--off levelsoff levels
Neonates* to 6 months: >0.3Neonates* to 6 months: >0.36 months6 months--1 year: >0.61 year: >0.611--5 yrs: >0.85 yrs: >0.866--12 12 ysys: >1.0: >1.0For children >12 years old: For children >12 years old: creatcreat >1.1>1.1For adults >21 years old: For adults >21 years old: creatcreat >1.5>1.5
based on Schwartz formula (muscle mass)based on Schwartz formula (muscle mass)

IV flow rates 2IV flow rates 2--5 ml/sec5 ml/sec
PowerPower--InjectableInjectable Venous Catheters:Venous Catheters:Quality of enhancement &Quality of enhancement &
Quality of life issue for patientsQuality of life issue for patients
Children:Children:•• PICCsPICCs (4,5 Fr)(4,5 Fr)•• Central lines Central lines (8(8--10 Fr)10 Fr)
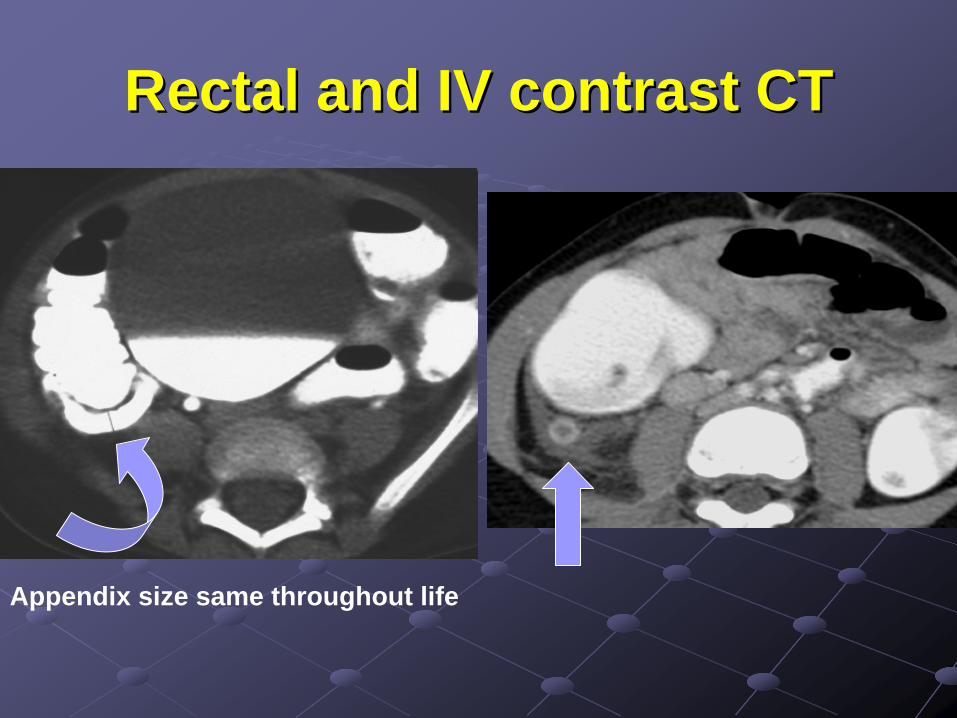
Rectal and IV contrast CTRectal and IV contrast CT
Appendix size same throughout life

Cocktail Party FactoidsCocktail Party FactoidsFrom birth to death, the human vermiform From birth to death, the human vermiform
("worm("worm--like") appendix size stays the samelike") appendix size stays the same---- it is a 5it is a 5--10cm long and 0.510cm long and 0.5--1cm wide pouch1cm wide pouch
The only other mammals known to have The only other mammals known to have appendices are rabbits, opossums and appendices are rabbits, opossums and wombatswombats, and their appendices are markedly , and their appendices are markedly different than the human appendix. different than the human appendix.
[W Parker, Duke][W Parker, Duke]

Alternative Diagnoses at CT, USAlternative Diagnoses at CT, US
Mesenteric Mesenteric lymphadenopathylymphadenopathyOvarian cyst Ovarian cyst PyelonephritisPyelonephritisUreteralUreteral StoneStoneTOATOAOmentalOmental infarctioninfarctionIleoIleo--colitiscolitis
* up to 50% of cases* up to 50% of cases

CT and US for AppendicitisCT and US for Appendicitis MetaMeta--analysisanalysis
A Doria et al. Radiology 2006Children, adults sens, spec15 peds, 29 adult articles CT higher sens for both peds, adults
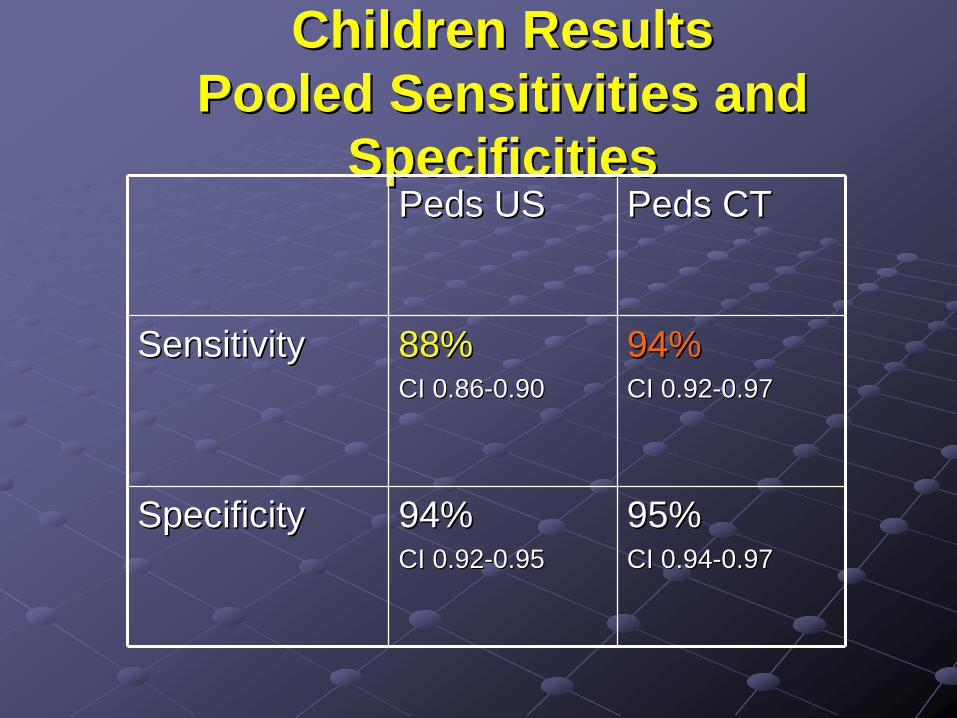
Children ResultsChildren Results Pooled Sensitivities and Pooled Sensitivities and
SpecificitiesSpecificitiesPedsPeds USUS PedsPeds CTCT
SensitivitySensitivity 88%88%CI 0.86CI 0.86--0.900.90
94%94%CI 0.92CI 0.92--0.970.97
SpecificitySpecificity 94%94%CI 0.92CI 0.92--0.950.95
95%95%CI 0.94CI 0.94--0.970.97

What does this mean?What does this mean?
For every 10,000 kids (11 For every 10,000 kids (11 y/oy/o) scanned ) scanned with US instead of CT, 280 cases of with US instead of CT, 280 cases of appendicitis would be missedappendicitis would be missed
13 future cancers may be prevented13 future cancers may be prevented

Imaging Algorithm in Suspected Imaging Algorithm in Suspected AppendicitisAppendicitis
Pain control in EDPain control in EDSonographySonography
If negative, CT scanIf negative, CT scan

Spontaneous Resolution vs. Spontaneous Resolution vs. Perforating AppendicitisPerforating Appendicitis
Likely that most people experience selfLikely that most people experience self-- limited degrees of limited degrees of appendicealappendiceal inflammation at some time in their livesinflammation at some time in their lives
22% infants at autopsy had signs of 22% infants at autopsy had signs of subacutesubacute appendicitisappendicitis
Contributes to false Contributes to false negneg/positive rates/positive rates
Kraemer M, et al. Kraemer M, et al. EurEur J J SurgSurg 19991999

Effectiveness vs. EfficacyEffectiveness vs. EfficacyFlumFlum et al., U Washington, JAMA 2001et al., U Washington, JAMA 2001Measured Measured ‘‘bad outcomebad outcome’’ over 13 year over 13 year trendtrend
Diffusion of CT, US, laparoscopyDiffusion of CT, US, laparoscopy““These data suggest that on a These data suggest that on a population level, diagnosis of population level, diagnosis of appendicitis has not improved with the appendicitis has not improved with the availability of advanced diagnostic availability of advanced diagnostic testingtesting””

13yr trend result: 13yr trend result: No improvement in NA or No improvement in NA or perfperf ratesrates
Possible explanations:Possible explanations:(1) misapplication of imaging exams to (1) misapplication of imaging exams to
wrong patients, or at wrong timewrong patients, or at wrong time(2) misinterpretation/mistrust of exam (2) misinterpretation/mistrust of exam
interpretation by clinicians after hours interpretation by clinicians after hours by less experienced imagers (e.g., by less experienced imagers (e.g., residents)residents)
(3) availability and belief that laparoscopy (3) availability and belief that laparoscopy is less invasive than is less invasive than laparotomylaparotomy

SummarySummaryImaging depends on Imaging depends on clinical clinical ddxddxIn older children, CT is In older children, CT is a useful toola useful toolIn younger children, In younger children, fluorofluoro and US more and US more common toolscommon tools