hypothalamic hormoneshypothalamic hormones pituitary hormonespituitary hormones parathyroid...
TRANSCRIPT
•Hypothalamic hormonesHypothalamic hormones•Pituitary hormonesPituitary hormones•Parathyroid hormoneParathyroid hormone
Assoc. Prof. Iv. LambevE-mail: [email protected]
HormonesHormones (from Greek hormaein – to set in motion)are chemical substances of intense biological activity. They are secreted by specific endocrine glands and are transported in the bloodstream to act on theirdistant target organs. Hormones regulate body functions and maintain homeostasis in the face ofmarkedly variable external and internal environment.The natural hormones and their synthetic analogues(which in many cases may be more effective), are used as drugs for substitution therapy as well as for pharmacotherapy.In addition, hormone antagonists and hormone syn-thesis release inhibitors have significant therapeuticimportance too.

1. Hypothalamic hormones Thyrotrophin releasing hormone (TRH) – peptide
Corticotrophin releasing hormone (CRH) – peptideGonadotrophin releasing hormone
(GnRH – Gonadorelin): LH-RH/FSH-RH – peptideGrowth hormone releasing hormone: (GHRH) – peptideProlactin releasing hormone (PRH): UnknownProlactin release inhibitory hormone (PRIH):
Dopamine (DA)Growth hormone release inhibitory hormone:
(GHRIH): Somatostatin – peptide
Classification of hormones

2. Pituitary hormones
a) Anterior Pituitary hormones Growth hormone (GH) Prolactin Adrenocorticotropic hormone (ACTH, Corticotrophin) Thyroid stimulating hormones (TSH, Thyrotrophin) Gonadotrophins
- Follicle stimulating hormone (FSH)- Luteinizing hormone (LH)
b) Posterior Pituitary hormones Oxytocin Antidiuretic hormone (ADH, Vasopressin)
2. Thyroid hormonesThyroxine (T4), Triiodothyronine (T3)Calcitonin
3. Parathyroid hormone: Parathormone (PTH)4. Hormones of endocrine pancreas: Insulin, Amylin, Glucagon5. Adrenal hormones a) Hormones of Adrenal cortex (Steroids) - Glucocorticoids (GCS): Hydrocortisone, Cortisone
- Mineralocorticoids: Aldosterone- Sex steroids: Dehydroepiandrosterone (Testost.)
b) Hormone of Adrenal medulla: Adrenaline6. Hormone of Gonads
a) Androgens: Testosteroneb) Estrogens: Estradiolc) Progestins: Progesterone
8. Placental hormones Estrogens, Progesterone, Chorionic gonadotrophin9. Hormne of Adipocytes: Leptin – acts on receptors in the hypothalamus of the brain where it inhibits appetite. 10. Ghrelin is a peptide hormonethat is produced mainly bythe fundus of the stomach andepsilon cells of the pancreas. It stimulates hunger. Ghrelin levels increasebefore meals and decrease after meals.
Mechanisms of hormone action
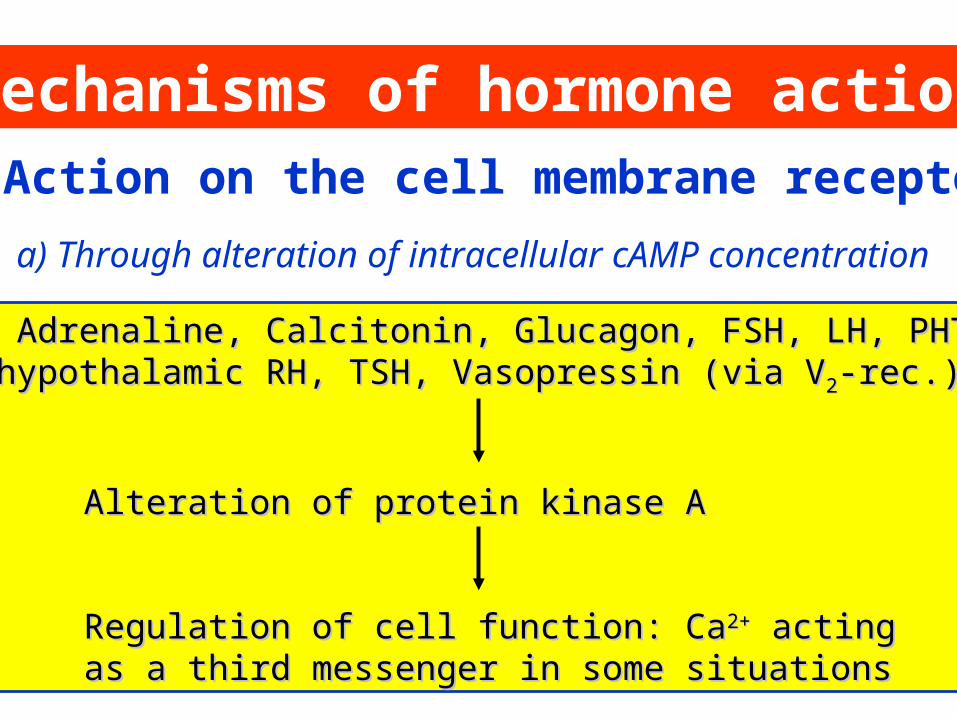
ACTH, Adrenaline, Calcitonin, Glucagon, FSH, LH, PHT,ACTH, Adrenaline, Calcitonin, Glucagon, FSH, LH, PHT,some hypothalamic RH, TSH, Vasopressin (via Vsome hypothalamic RH, TSH, Vasopressin (via V22-rec.)-rec.)
Alteration of protein kinase AAlteration of protein kinase A
Regulation of cell function: CaRegulation of cell function: Ca2+2+ acting acting as a third messenger in some situationsas a third messenger in some situations
1. Action on the cell membrane receptors
a) Through alteration of intracellular cAMP concentration
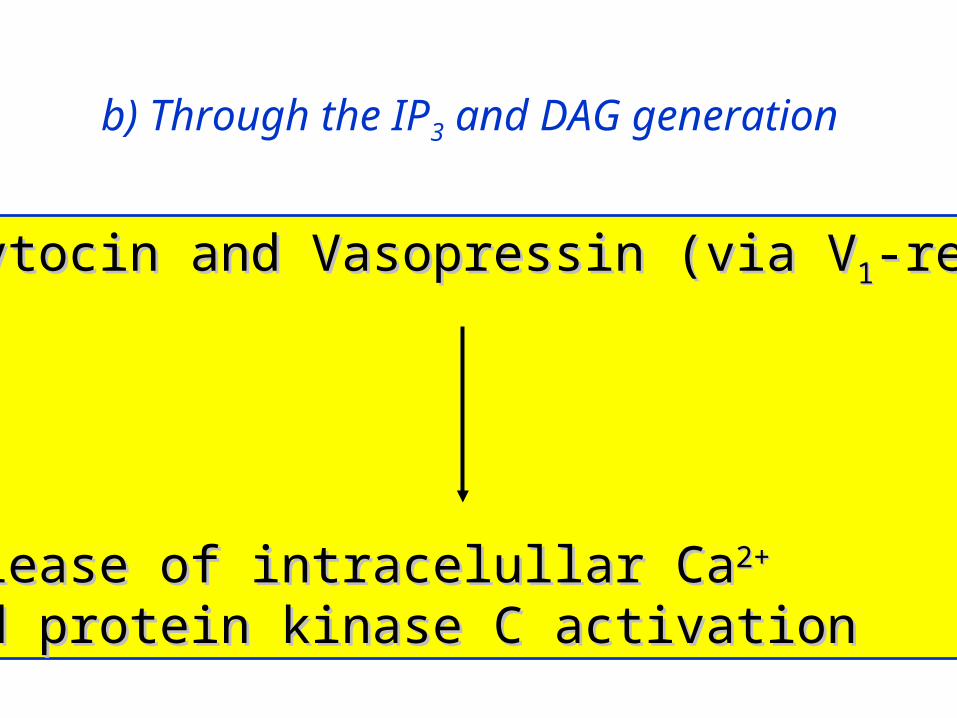
Oxytocin and Vasopressin (via VOxytocin and Vasopressin (via V11-rec.)-rec.)
Release of intracelullar CaRelease of intracelullar Ca2+2+
and protein kinase C activationand protein kinase C activation
b) Through the IP3 and DAG generation
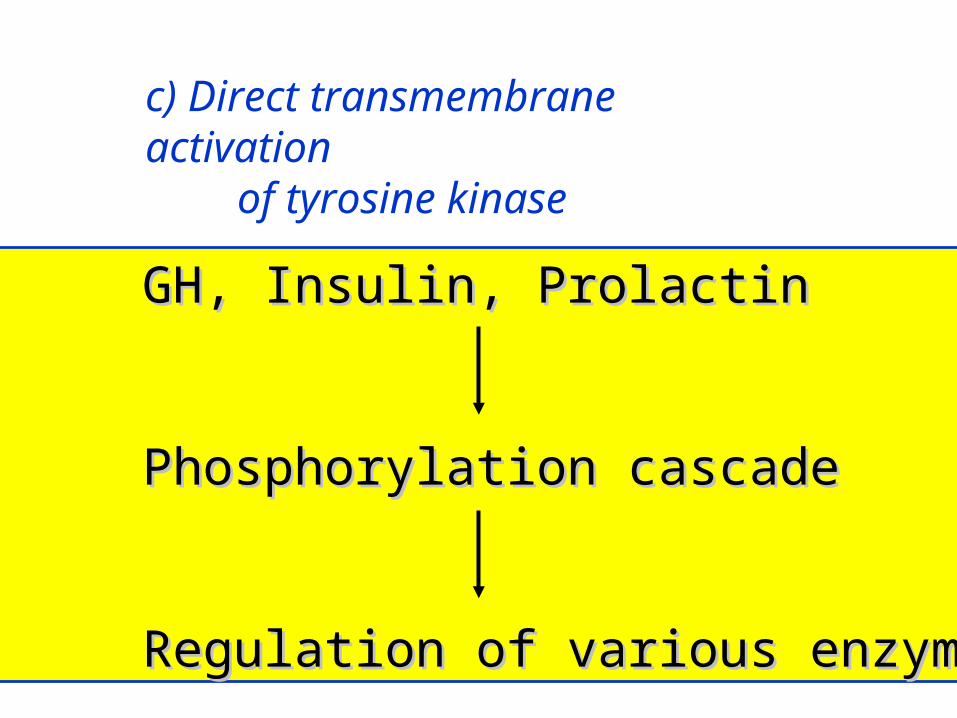
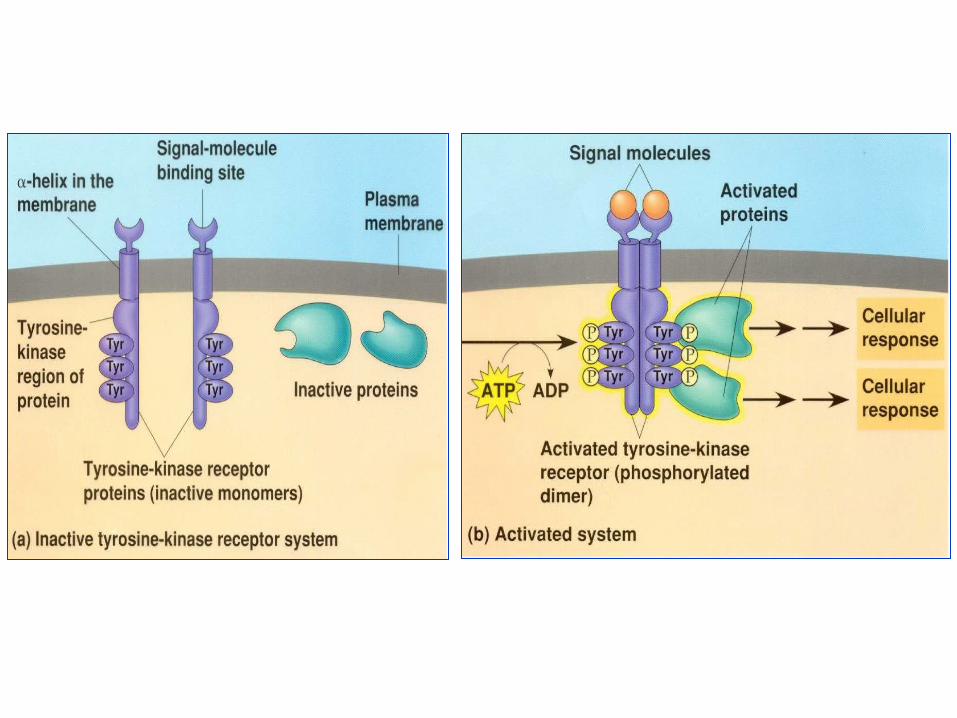
GH, Insulin, ProlactinGH, Insulin, Prolactin
Phosphorylation cascadePhosphorylation cascade
Regulation of various enzymesRegulation of various enzymes
c) Direct transmembrane activation of tyrosine kinase

a) At cytoplasmic receptors:• Steroid hormones, Calcitriol
2. Action on the 2. Action on the intracellularintracellular(steroid or thyroid) receptors(steroid or thyroid) receptors
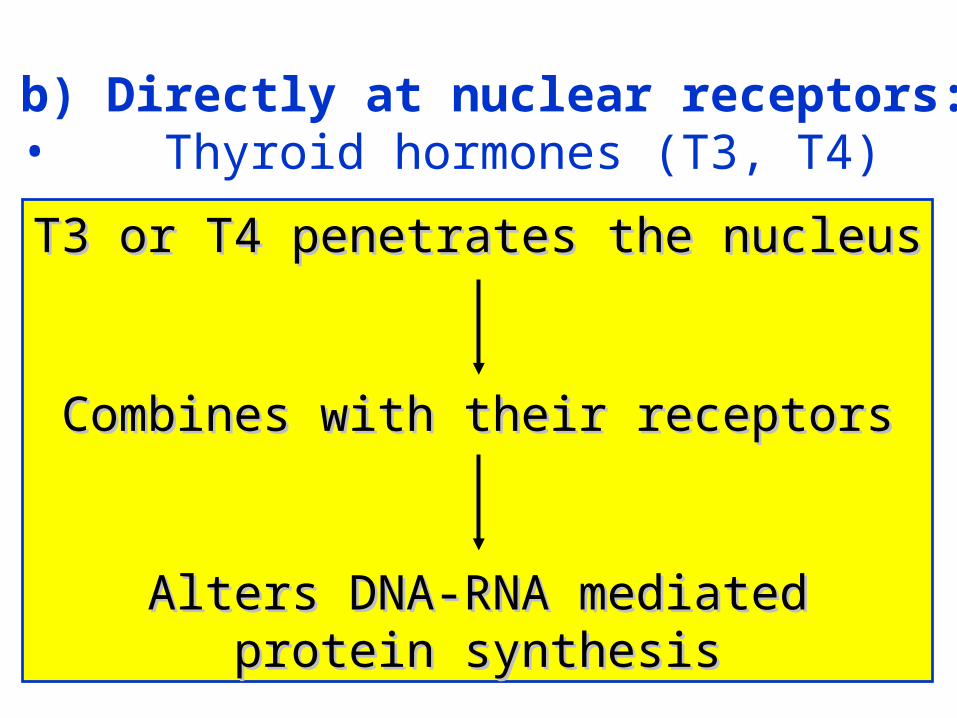
b) Directly at nuclear receptors:• Thyroid hormones (T3, T4)
T3 or T4 penetrates the nucleusT3 or T4 penetrates the nucleus
Combines with their receptorsCombines with their receptors
Alters DNA-RNA mediatedAlters DNA-RNA mediatedprotein synthesisprotein synthesis
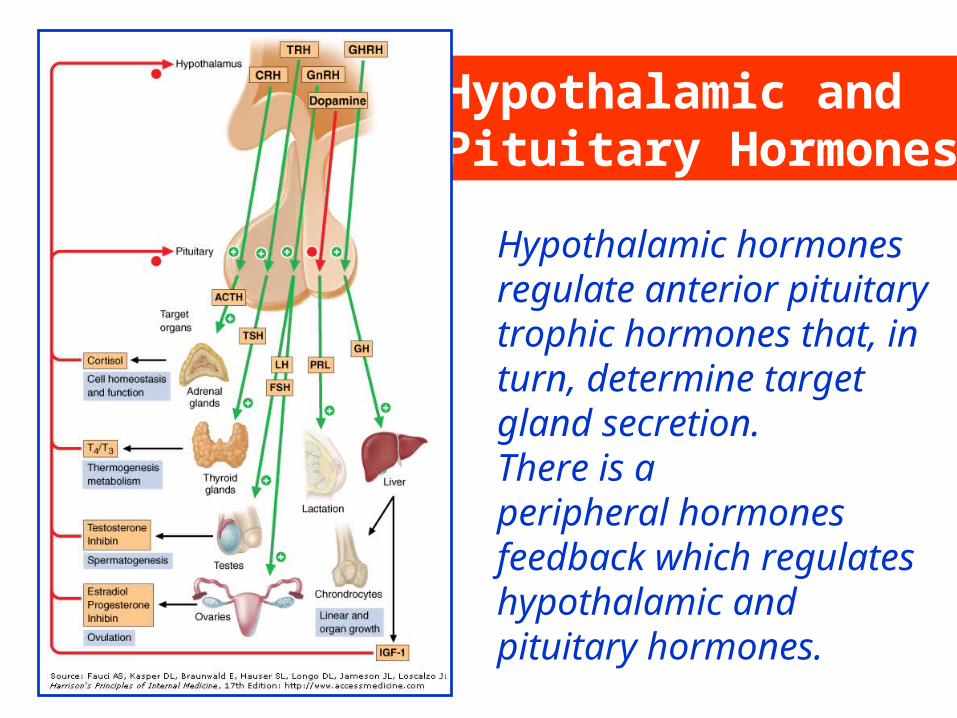
Hypothalamic hormonesregulate anterior pituitarytrophic hormones that, inturn, determine target gland secretion. There is aperipheral hormones feedback which regulates hypothalamic and pituitary hormones.
Hypothalamic and Pituitary Hormones
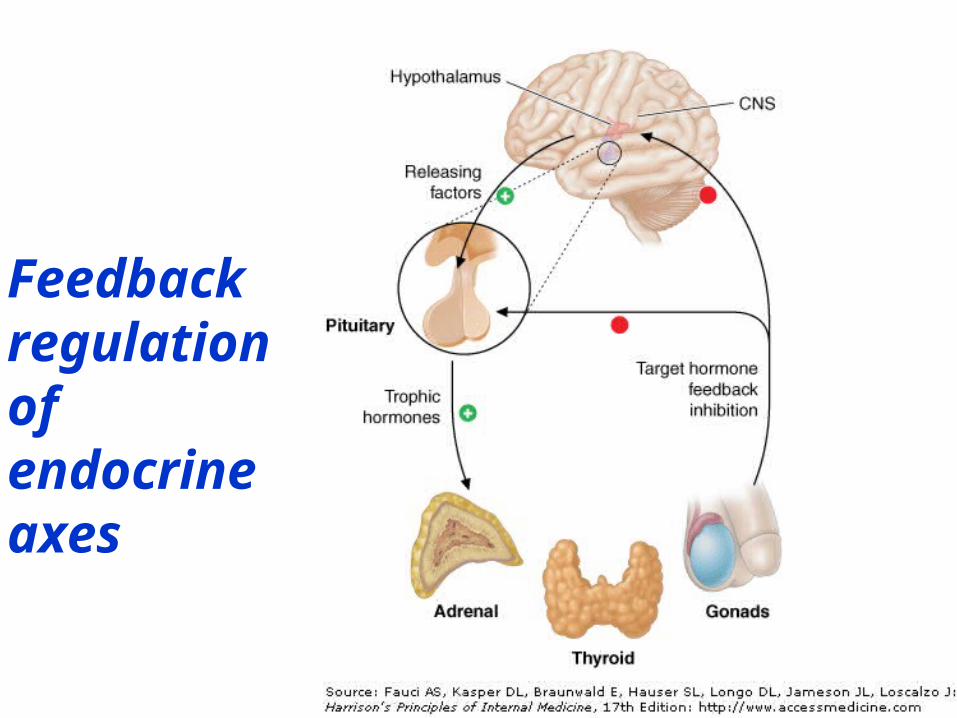
Feedbackregulationof endocrineaxes
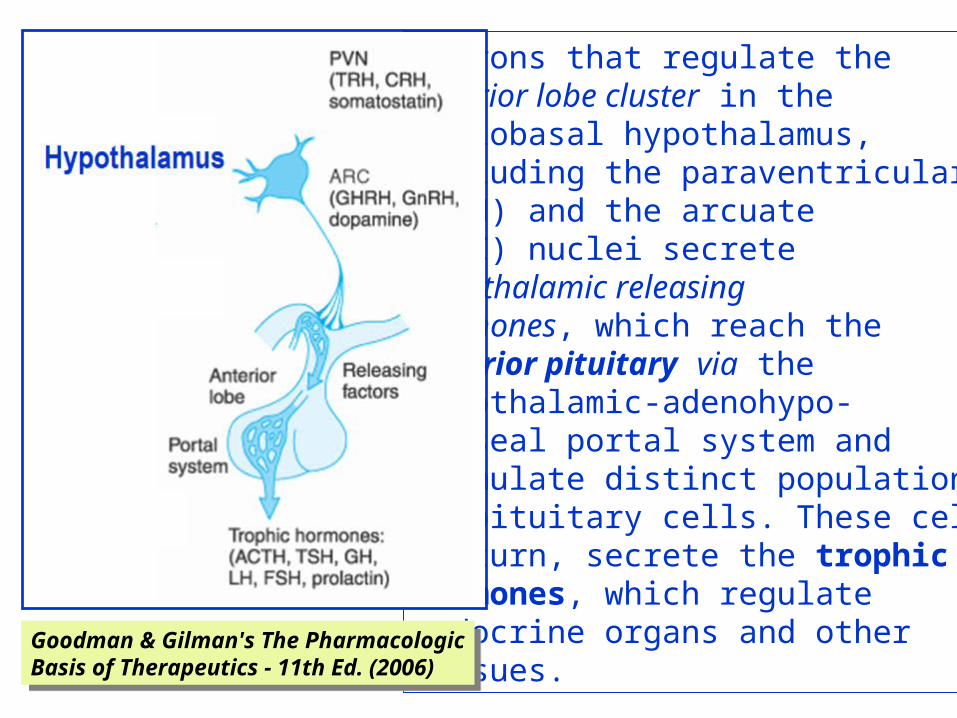
Neurons that regulate the anterior lobe cluster in themediobasal hypothalamus,including the paraventricular(PVN) and the arcuate (ARC) nuclei secretehypothalamic releasing hormones, which reach the anterior pituitary via the hypothalamic-adenohypo-physeal portal system and stimulate distinct populationsof pituitary cells. These cells,in turn, secrete the trophic hormones, which regulateendocrine organs and othertissues.
Goodman & Gilman's The PharmacologicBasis of Therapeutics - 11th Ed. (2006)
Goodman & Gilman's The PharmacologicBasis of Therapeutics - 11th Ed. (2006)
Corticotrophin releasing hormoneCorticotrophin releasing hormone (CRH) – corticoliberin, is a hypothalamic polypeptide fordiagnostic use. It increases ACTH secretion inCushing's diseas. Natural corticotrophincorticotrophin (ACTH) is a 39-amino-acidpolypeptide secreted by the anterior pituitary gland, obtained from animal pituitaries. The physiologicalactivity resides in the first 24-amino acids (whichare common to many species) and most of the immu-nological activity resides in the remaining 15 aminoacids. The pituitary output of corticotrophin responds rapidly to physiological requirements by the familiar negative-feedback homeostatic mechanism.
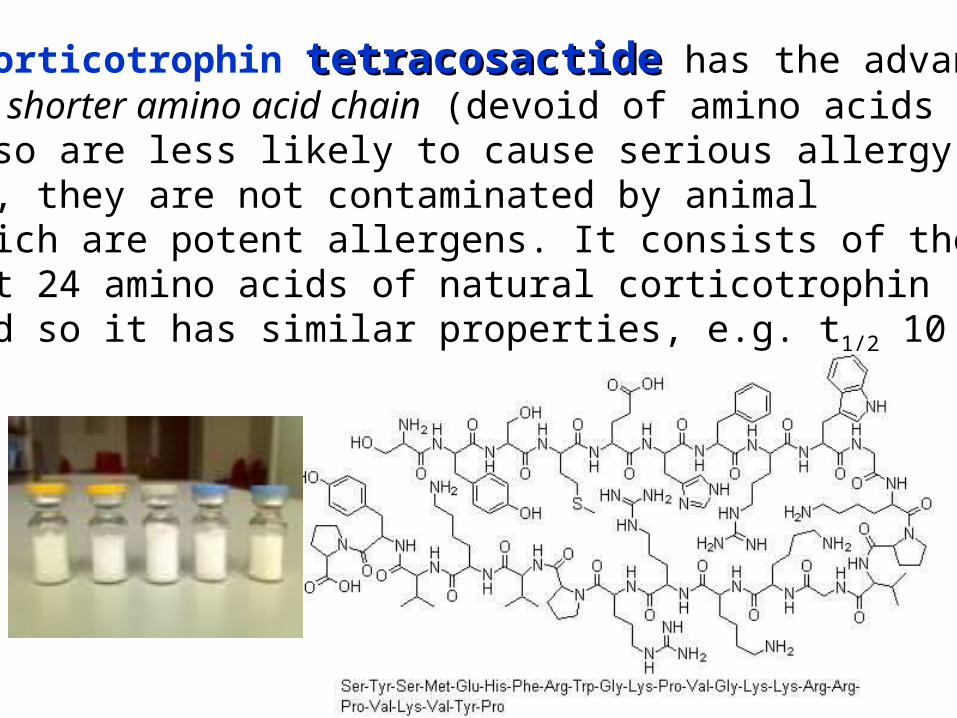
Synthetic corticotrophin tetracosactidetetracosactide has the advantagethat contains shorter amino acid chain (devoid of amino acids25–39) and so are less likely to cause serious allergy.In addition, they are not contaminated by animalproteins which are potent allergens. It consists of the biologicallyactive first 24 amino acids of natural corticotrophin (from man oranimals) and so it has similar properties, e.g. t1/2 10 min.
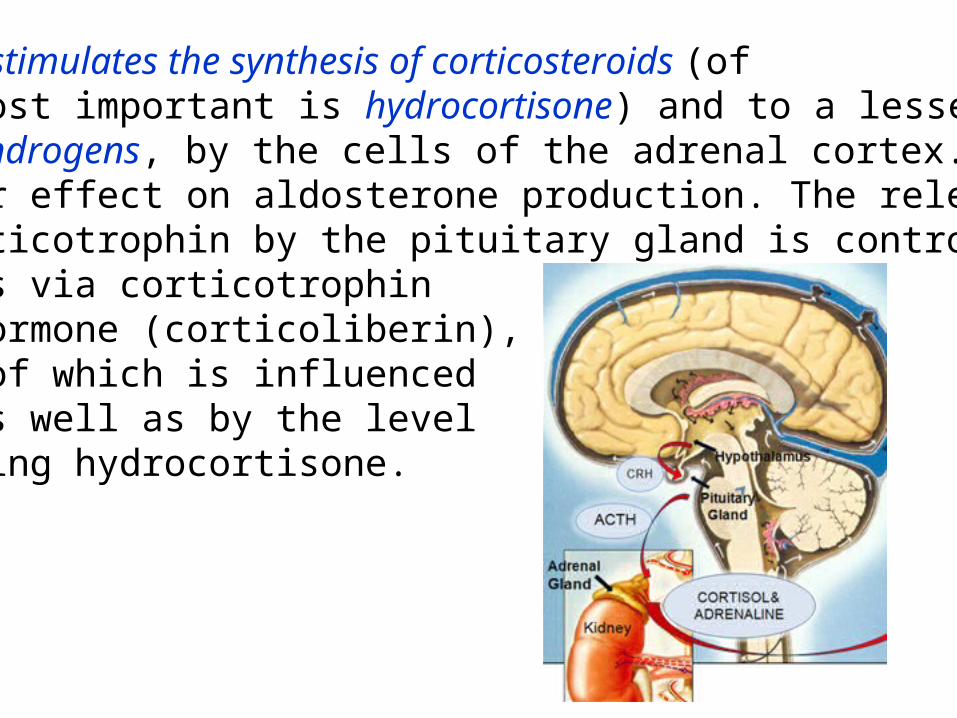
Corticotrophin stimulates the synthesis of corticosteroids (ofwhich the most important is hydrocortisone) and to a lesserextent of androgens, by the cells of the adrenal cortex. It hasonly a minor effect on aldosterone production. The release ofnatural corticotrophin by the pituitary gland is controlled by thehypothalamus via corticotrophinreleasing hormone (corticoliberin),production of which is influencedby stress as well as by the levelof circulating hydrocortisone.
High plasma concentration of any steroid with glucocorticoid effect prevents release of corticotrophin releasing hormone as well as of ACTH, the lack of which in turn results in adrenocortical hypofunction.This is the reason why catastrophe may follow the sudden withdrawal of steroid therapy in the chronically treated patient who has an atrophied cortex.The effects of corticotrophin are those of the steroids (hydrocortisone, androgens) liberated by its action on the adrenal cortex. Prolonged heavy dosage causes Cushing's Cushing's syndromesyndrome.Tetracosactide (Synacthen®) is used as a test of the capacityof the adrenal cortex to produce cortisol (hydrocortisone).
Thyrotrophin releasing hormoneThyrotrophin releasing hormone (TRH) – protirelin, is a thripeptide formed in the hypo-thalamus and controlled by free plasma T4and T3 concentration. It has been synthesizedand can be used in diagnosis to test the capacity of the pituitary to release thyroidstimulating hormone, e.g. to determinewhether hypothyroidism is due to primarythyroid gland failure or is secondary to pituitarydisease or to a hypothalamic lesion. TRH isTRH isalso a potent prolactin-releasing factor.also a potent prolactin-releasing factor.

Thyroid stimulating hormone (TSH)Thyroid stimulating hormone (TSH) thyrotrophinthyrotrophin, a glycoprotein of the anterior pituitary,controls the synthesis and release of thyroid hormone from the gland, and also the uptake of iodide. There is a negative feedback of thyroidhormones on both the hypothalamic secretion of TRH and pituitary secretion of TSH.
SermorelinSermorelin is an analogue of the hypothalamicgrowth hormone releasing hormone (somatorelinsomatorelin).It is used in a diagnostic test for growth hormonesecretion from the pituitary.
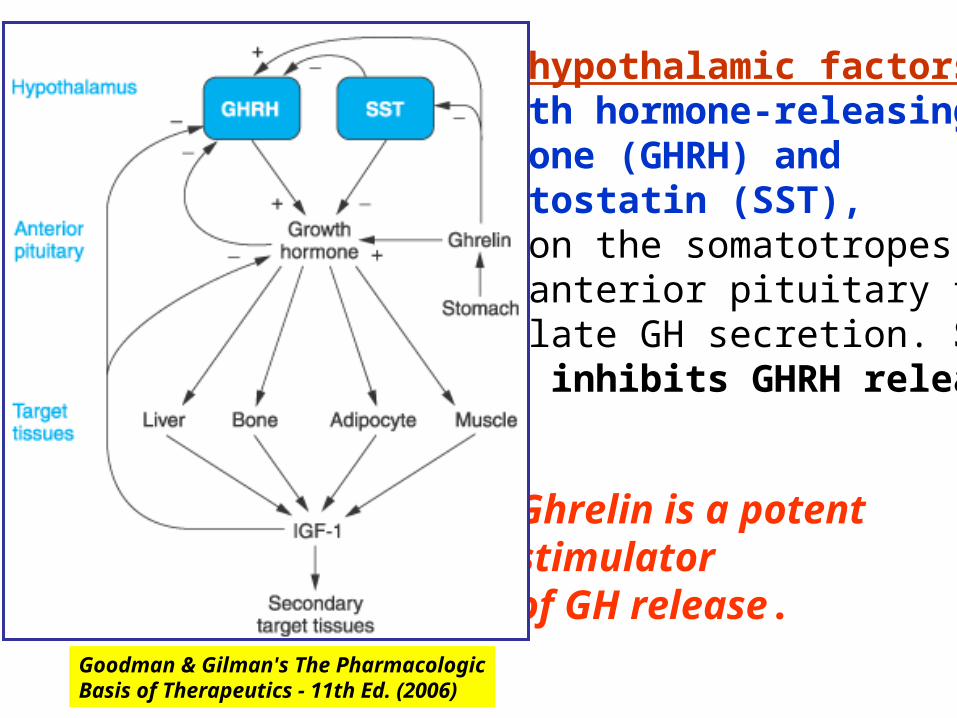
Two hypothalamic factors,growth hormone-releasinghormone (GHRH) andsomatostatin (SST),act on the somatotropes inthe anterior pituitary toregulate GH secretion. SSTalso inhibits GHRH release.
Goodman & Gilman's The PharmacologicBasis of Therapeutics - 11th Ed. (2006)
Ghrelin is a potent stimulatorof GH release.
Growth hormoneGrowth hormone (GH) (GH),, one of the peptide hormones produced by the anterior pituitary, is required duringchildhood and adolescence for attainment of normaladult size and has important effects throughout post-natal life on lipid and carbohydrate metabolism, and on body mass. Its effects are primarily mediated viainsulin-like growth factor 1 (IGF-1) and IGF-2insulin-like growth factor 1 (IGF-1) and IGF-2. Individuals with congenital or acquired deficiency inGH during childhood or adolescence fail to reachtheir predicted adult height and have disproportionatelyincreased body fat and decreased muscle mass.Adults with GH deficiency also have disproportionatelysmall body mass.
GH is a 191-amino-acid peptide. Two types ofrecombinant human growth hormone (rhGH)are approved for clinical use: Somatrophin (identical with the native form of human GH) and Somatrem (with an extra methionine residue at the aminoterminal end). The drugs are used in children with growth hormonedeficiency, while the bone epiphyses are still open,to prevent dwarfism (underdevelopment of the body)and provide normal growth. Treatment improvesexercise performance and increases lean bodymass. It may improve overall quality of life.
Possibilities of abuse have also arisen, e.g. creationof “super” sports people. Less dubious, but not yeta licensed indication of GH, is the potential for accelerated wound healing reported in childrenwith large cutaneous burns. GH is a popular compo-GH is a popular compo-nent of anti-aging programmesnent of anti-aging programmes. Serum levels of GH normally decline with aging. GH is one of the drugsGH is one of the drugsbanned by the Olympic Committeebanned by the Olympic Committee..In acromegaly, excess GH causes diabetes, hyperten-sion, and arthritis. Surgery is the treatment of choice. GH secretion is reduced by octreotide and othersomatostatin analogues and to a lesser degree by bromocriptine.

SomatostatinSomatostatin (growth hormone release inhibiting hormone)occurs in other parts of the brain as well as in the hypothalamus, and also in pancreas, stomach, and intestine. It inhibitssecretion of GH, thyrotrophin, insulin, glucagon, gastrin, CCK (cholecystokinine), secretin, motilin, VIP (vasoactive intestinalpeptide), GIP (gastric inhibitory peptide), 5-HT, etc.Radiolabelled somatostatin is used to localise metastases fromneuroendocrine tumours which often bear somatostatin receptors.•OctreotideOctreotide is a synthetic analogue of somatostatin having a longer action (t1/2 1.5 h). •LanreotideLanreotide is much longer acting, and is administered only twice a month. Main indications: acromegaly/gigantism, carcinoid (serotonin secreting) tumours, and other rare tumours of the GIT.

A 22-year-old man with gigantism due to excess growth hormoneis shown to the left of his identical twin. The increased height and prognathism (A) and enlarged hand (B) and foot (C) of the affected twin are apparent. Their clinical features began to diverge at the age of approximately 13 years.

Pituitary adenomaPituitary adenoma•Lacotrophic – secrete prolactin (galactorrhea, infertility, impotence)•Somatotrophic – secrete GH (acromegaly)•Corticotrophic – secrete ACTH (Cushing’s disease)•Gonadotrophic – secrete LH & FSH (no symptoms)•Thyrotrophic – secrete TSH (occasionaly hyperthyroidism)Transsphenoidal resectionof pituitary tumour massvia the endonasal approach
GonadorelinGonadorelin (gonadotrophin releasing hormone – GnRH) releases luteinising hormone (LH) andfollicle-stimulating hormone (FSH). It hasuse in the assessment of pituitary function. Intermittentpulsatile administration evokes secretion ofgonadotrophins (LH and FSH) and is used to treatinfertility. But continuous use evokes tachyphylaxisdue to down-regulation of its receptors, i.e. gonadotrophin release and therefore gonadalsecretions are reduced. Longer-acting analogues – agonists of GnRHLonger-acting analogues – agonists of GnRH(buserelin, goserelin, nafarelin, deslorelin, and leuprorelin)are used to suppress androgen secretionin prostatic carcinoma.
Other uses may include endometriosis,precocious puberty, and contraception. All thesedrugs need to be administered by a parenteralroute, by i.m. injection or intranasally.Follicle stimulating hormone (FSH)Follicle stimulating hormone (FSH) stimulates thedevelopment of ova and of spermatozoa. It is prep-ared from the urine of postmenopausal women.Urofollitrophin (MetrodinUrofollitrophin (Metrodin®®)) contains FSH.Menotrophins (PergonalMenotrophins (Pergonal®®)) contains FSH and LH. These drugs are used in female and male hypopituitary infertility.Chorionic gonadotrophinChorionic gonadotrophin (human chorionic gona-dotrophin – hCG) is secreted by the placenta andis obtained from the urine of pregnant women.
The predominant action of hCG is that of LH.It induces progesterone production by the corpusluteum and, in the male – gonadal testosteroneproduction. It is used in hypopituitary anovular andother infertility in both sexes. It is also usedfor cryptorchidism in prepubertal boys (6 years ofage; if it fails to induce testicular descent, there istime for surgery before puberty to provide maximalpossibility of a full functional testis). It may alsoprecipitate puberty in men where this is delayed.
ProlactinProlactin is secreted by the lactotroph cells of theanterior pituitary gland. Its control is by tonichypothalamic inhibition through prolactin inhibitoryfactor (PIF), probably dopamine, opposed by aprolactin releasing factor (PRF) in both women andmen and, despite its name, it influences numerousbiological functions. Prolactin secretion iscontrolled by an inhibitory dopaminergic path. Hyper-prolactinaemia may be caused by drugs (with anti-dopaminergic actions e.g. metoclopramide), hypo-thyroidism, or prolactin secreting adenomas. Medicaltreatment is with bromocriptinebromocriptine, , cabergolinecabergoline, or quinagolidequinagolide at bedtime.
In hypopituitarism there is a partial or completedeficiency of hormones secreted by the anteriorlobe of the pituitary. The posterior lobe hormonesmay also be deficient in a few cases, e.g.when a tumour has destroyed the pituitary.Patients suffering from hypopituitarismmay present in coma, in which casetreatment is for a severe acuteadrenal insufficiency. Maintenancetherapy is required, usinghydrocortisone, thyroxine,oestradiol, and progesterone(in women) and testosterone (inmen), or GH analogues (somatrophinor somatrem).
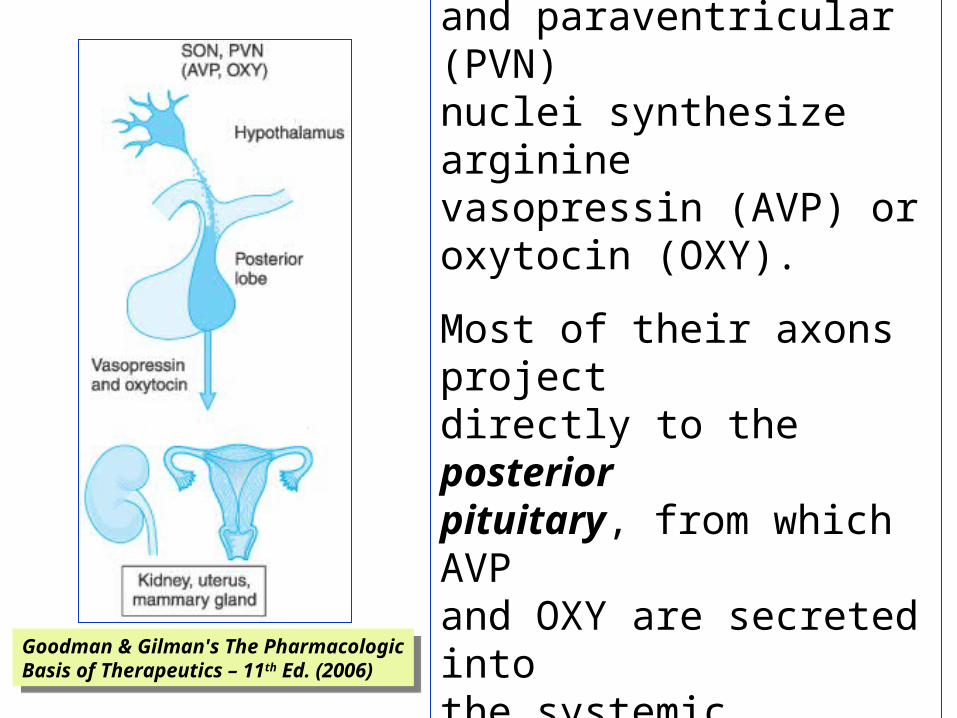
Hypothalamic neurons in the supraoptic (SON)and paraventricular (PVN)nuclei synthesize argininevasopressin (AVP) oroxytocin (OXY).
Most of their axons projectdirectly to the posterior pituitary, from which AVPand OXY are secreted intothe systemic circulation to regulate their target tissues.Goodman & Gilman's The Pharmacologic
Basis of Therapeutics – 11th Ed. (2006)
Goodman & Gilman's The PharmacologicBasis of Therapeutics – 11th Ed. (2006)
VasopressinVasopressin is a nonapeptide (t1/2 20 min) withtwo separate G-protein coupled target receptorsresponsible for its two roles. The V1 receptor onvascular smooth muscle is coupled to calciumentry. This receptor is not usually stimulated byphysiological concentrations of the hormone. The V2 receptor is coupled to adenylyl cyclase, andregulates opening of the water channel, aquaporin,in cells of the renal collecting duct.Secretion of the antidiuretic hormone is stimulatedby any increase in the osmotic pressure of the bloodsupplying the hypothalamus and by a variety ofdrugs, notably nicotine. Secretion is inhibited by a fallin blood osmotic pressure and by alcohol.
In large nonphysiological doses (pharmacotherapy)vasopressin causes contraction of all smoothmuscle, raising the blood pressure and causingintestinal colic. The smooth-muscle stimulant effectprovides an example of tachyphylaxis (frequentlyrepeated doses give progressively less effect). It isnot only inefficient when used to raise the bloodpressure, but is also dangerous, since it causesconstriction of the coronary arteries and suddendeath has occurred following its use.For replacement therapy of pituitary diabetesinsipidus the longer acting analogue desmopressinis used.
DesmopressinDesmopressin (des-amino-D-arginine vasopressin)(DDAVP) has two major advantages: the vasocon-strictor effect has been reduced to near insignificanceand the duration of action with nasal instillation,spray or s.c. injection, is 8–20 h (t1/2 75 min) so that,using it once to twice daily, patients are not incon-venienced by frequent recurrence of polyuria duringtheir waking hours and can also expect to spend thenight continuously in bed. The adult dose forintranasal administration is 10–20 micrograms daily.The dose for children is about half that for adults.The bioavailability of intranasal DDAVP is 10%. It isalso the only peptide for which an oral formulationis available, with a bioavailability of only 1%.
The main complication of DDAVP is hyponatraemiawhich can be prevented by allowing the patientto develop some polyuria for a short periodduring each week. The requirement for DDAVPmay decrease during intercurrent illness.Terlipressin is an analogue of vasopressinused in NA-resistant septic shock andesophageal varices.
OxytocinOxytocin is a peptide hormone of the posteriorpituitary gland. It stimulates the contractions of thepregnant uterus, which becomes much more sensitiveto it at term. Patients with posterior pituitary disease(diabetes insipidus) can, however, go into labour normally.
Oxytocin is structurally close to vasopressinand it is no surprise that it also has antidiureticactivity. Serious water intoxication canoccur with prolonged i.v. infusions, especiallywhere accompanied by large volumes of fluid.The association of oxytocin with neonataljaundice appears to be due to increasederythrocyte fragility causing haemolysis.Oxytocin has been supplanted by the Methylergometrine (Methergin®), as the primetreatment of postpartum haemorrhage.
Neonatal jaundice
Oxytocin is reflexly released from the pituitaryfollowing suckling (also by manual stimulation ofthe nipple) and causes almost immediate contractionof the myoepithelium of the breast; it can be used toenhance milk ejection (nasal spray).Oxytocin is used i.v. in the induction of labour. It produces, almost immediately, rhythmic contractionswith relaxation between, i.e. it mimics normal uterineactivity. The decision to use oxytocin requires specialskill. It has a t1/2 of 6 min and is given by i.v. infusionusing a pump; it must be closely supervised; the doseis adjusted by the results; overdose can cause uterinetetany and even rupture.

Atosiban is a modified form of oxytocin that inhibitsthe action of this hormone on the uterus, leading toa cessation of contractions. It is used i.v. as a tocolytic to halt premature labor.Barusiban is three to four times more potentantagonist than atosiban with higher affinity andselectivity for the oxytocin receptor.

Parathyroid hormoneParathyroid hormone (PTH)
PTH acts chiefly on the kidney increasingrenal tubular reabsorption and bone resorption ofcalcium; it increases calcium absorption from thegut, indirectly, by stimulating the renal synthesis of25-hydroxycholecalciferol (calcifediol). It increases the rate of bone remodelling (mineral andcollagen) and osteocyte activity with, at high doses,an overall balance in favour of resorption (osteoclastactivity) with a rise in plasma calcium concentration(and fall in phosphate); but, at low doses, thebalance favours bone formation (osteoblast activity).

The mainfactorsinvolved inmaintainingtheconcentrationof calcium inthe plasma
Rang et al. Pharmacology – 5st Ed. (2003)