hypertension management seminar– executive summary · replace the beta-blocker in this case. when...
TRANSCRIPT

1
Hypertension
Management Seminar–
executive summary
Dr C P Ho20060204
Definition and classification
of hypertension: JNC VII
Hypertension is defined as blood pressure ≥140/90 mmHg
or ≥100≥160Stage 2 hypertension
or 90-99140-159Stage 1 hypertension
or 80-89120-139Prehypertension
and <80<120Normal
Diastolic
(mmHg)
Systolic
(mmHg)
Category
JNC VII. JAMA 2003;289:2560-2572

2
Prevalence of hypertension*:
North America and Europe
0
10
20
30
40
50
60
70
80
United
Sta
tes
Canad
a
Europ
eIta
ly
Sweden
Englan
dSpa
in
Finlan
d
Germ
any
Pre
vale
nce
(%)
MenWomenTotal
Wolf-Maier K, et al. JAMA 2003;289:2363-2369* BP ≥140/90 mmHg or treatment with antihypertensive medication

3
Prevalence of hypertension:
Asia
01020304050607080
China
(200
0/20
01)
Taiwan
(199
4)
Hong K
ong
(199
7)
Singap
ore
(199
8)
Mala
ysia
(199
6)
Thaila
nd (1
991)
Philipp
ines
(199
9)
Indo
nesia
(199
4)
India
(Mum
bai, 1
999)
Japa
n (19
92-9
5)
Pre
vale
nce
(%)
Men
Women
Total
Gu DF, et al. Hypertension 2002;40:920-927; Singh RB, et al. J Hum Hypertens 2000;14:749-763; Janus ED. Clin Exp Pharmacol Physiol1997;24:987-988; National Health Survey 1998, Singapo re. Epidemiology and Disease Department, Ministry of Health, Singapore.; Lim TO, et al.
Singapore Med J 2004;45:20-27; Tatsanavivat P, et al. Int J Epidemiol 1998;27:405-409; Muhilal H. Asia Pacific J Clin Nutr 1996;5:132-134; Gupta R. J Hum Hypertens 2004;18:73-78; Asai Y, et al. Nippon Koshu Eisei Zasshi 2001;48:827-836 [in Japanese]
Goals of treatment: JNC VII
The SBP and DBP targets are <140/90 mmHg The primary focus should be on achieving the SBP goalIn patients with hypertension and diabetes or renal disease, the BP goal is <130/80 mmHg
JNC VII. JAMA 2003;289:2560-2572SBP, systolic blood pressure; DBP, diastolic blood pressure; BP, blood pressure

4
<90 (DBP)
<90 (DBP)
<160/90
(SBP/DBP)
<90 (DBP)
<95 (DBP)
<160 (SBP)
Treatment failures
Study Blood pressure goal (mm Hg)
Patients not achieving goal on
active treatment (%)
HDFP
Australian Trial
EWPHE
IPPSH
HAPPHY
SHEP
23–37
36.1
22–32
34.6
23
28–35
Reference
HDFP, 1979
ANBP, 1980
Amery et al, 1991
IPPSH, 1985
Wilhelmsen et al, 1987
SHEP, 1991
24-h average blood pressure is correlated with:
Hypertension and
cardiovascular disease
Overall target organ damage score
Left ventricular mass
Impaired left ventricular function
(Micro) albuminuria
Brain damage
Retinopathy
Opsahl et al, 1988; Giaconi et al, 1989; Shimida et al , 1990; Hansen et al, 1992; White et al, 1993; Mancia et al, 1997

5
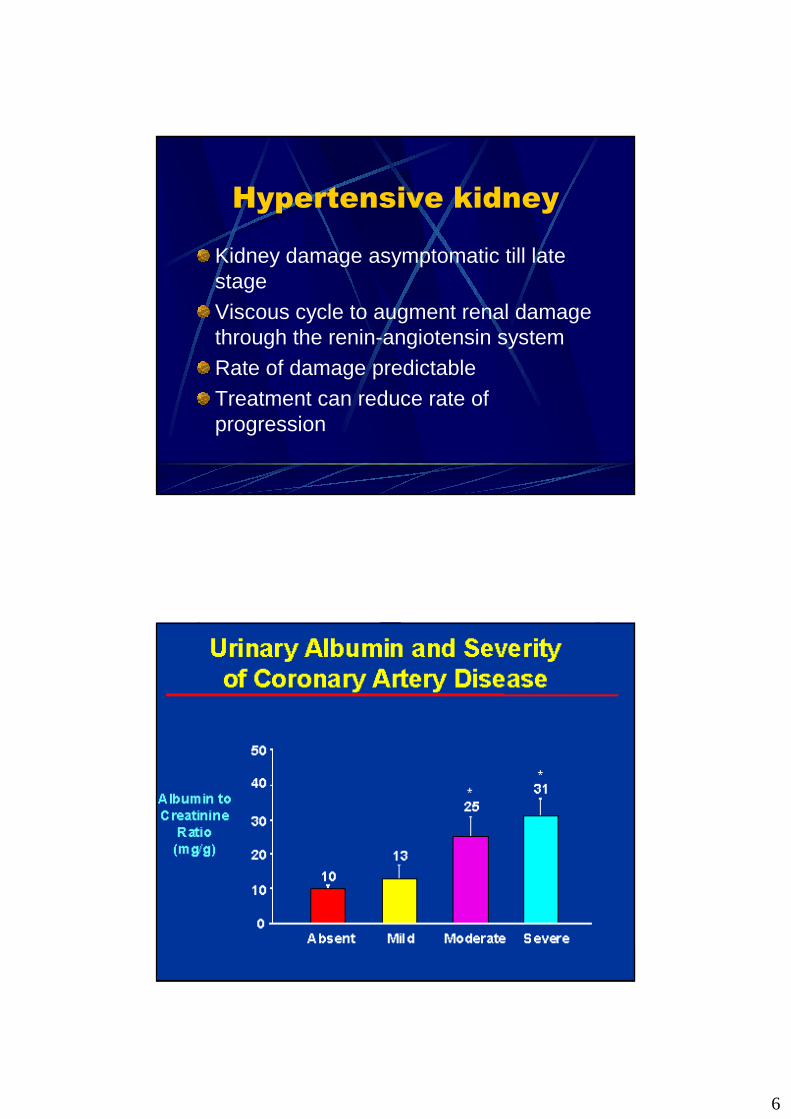
Hypertensive kidney
Kidney damage asymptomatic till late stageViscous cycle to augment renal damage through the renin-angiotensin systemRate of damage predictableTreatment can reduce rate of progression
6
Hypertensive kidney
Kidney damage asymptomatic till late stageViscous cycle to augment renal damage through the renin-angiotensin systemRate of damage predictableTreatment can reduce rate of progression

7
The cost of cardiovascular
diseases and stroke
Heart Disease and Stroke Statistics – 2006 Update, American Heart Association
Millimetres matter …
“A 2-mmHg reduction in DBP would
result in … a 6% reduction in the risk
of
CHD and a 15% reduction in the risk of
stroke and TIAs”
Cook NR, et al. Arch Intern Med 1995;155:701-709DBP, diastolic blood pressure; CHD, coronary heart disease; TIA, transient ischaemic attack

8
Millimetres matter …
“For individuals 40-70 years of age, each
increment of 20 mmHg in systolic BP or
10 mmHg in diastolic BP doubles the risk
of CVD across the entire BP range from
115/75 to 185/115 mmHg ”
JNC VII. JAMA 2003;289:2560-2572BP, blood pressure; CVD, cardiovascular disease
24-h blood pressure profile
in (dipper and non-dipper)Blood pressure (mm Hg)
7:00 11:00 15:00 19:00 23:00 3:00 7:00
Sleep
Dipper
Non-dipper
Time of day
175
135
115
95
75
55
155
Redman et al, 1976; Mancia et al, 1983; Kobrin et al, 1984; Baumgart et al, 1989; Imai et al, 1990; Portaluppi et al, 1991

9
Current evidence suggests that:
� Measures of 24-h blood pressure more closely predict target organ damage than do clinic or casual measurements� There is a higher incidence of cardiovascular compl ications when
night-time blood pressure remains elevated
� Blood pressure variability is an additional and in dependent
determinant of target organ damage
� The highest incidence of cardiovascular events occu rs in the
morning at (approximately) 24 h post dose
Blood pressure and
target organ damage
Sokolow et al, 1966; Devereux et al, 1983; Devereux et al, 1987; Parati et al,1987; Mancia , 1990
Current evidence suggests that:
� Measures of 24-h blood pressure more closely predic t target organ
damage than do clinic or casual measurements
� There is a higher incidence of cardiovascular compl ications when
night-time blood pressure remains elevated
� Blood pressure variability is an additional
and independent determinant of target organ
damage
� The highest incidence of cardiovascular events occu rs in the morning
at (approximately) 24 h post dose
Blood pressure and
target organ damage
Sokolow et al, 1966; Pessina et al, 1985; Stanton et al, 1993; Veermanet al, 1993

10
“The optimal formulation should provide 24-hourefficacy with a once- daily dose with at least 50% ofthe peak effect remaining at the end of the 24 hour s”
“Agents with a duration of action beyond 24 hoursare attractive because many patients inadvertentlymiss at least 1 dose of medication each week”
JNC-VI, 1997
JNC-VI Hypertension
Management Guidelines
Dippers *
(n=20)
BP: Night vs Day: *>10%; †<10%
*†Matched for age, sex, BMI, office BP, creatinin, li pids, antihypertensive R x
Fall in Cr Cl (ml/min.month)
Level of proteinuria (mg/24 h)
Night-time BP vs Cr Cl
Night-time BP vsproteinuria
Timio et al, 1993
-0.19
390
<0.001
<0.01
The importance of night-
time blood pressure
Non-dippers †
(n=28)
-0.33
659
r2=0.45
r2=0.22
<0.01
<0.01
Pvalue

11

12
2 Important Directions
1. Life-Style Management2. Medical Therapy
General issues when
prescribingPrescribe drugs taken only once a day if possible.
Prescribe non-proprietary drugs if these are appropriate and minimise cost.
Give information about the benefits and side effects of drugs so that patients can make informed choices.

13
Drug treatment
Key issues in updating the recommendations
Beta-blockers : In head-to-head trials, beta-blockers were usually less effective than a comparator drug at reducing major cardiovascular events, particularly stroke. Beta-blockers were also less effective than an ACE inhibitor or a calcium channel blocker at reducing the risk of diabetes, particularly in patients taking a beta-blocker and a thiazide-type diuretic.
Calcium-channel blockers or thiazide-type diuretics : These are the most likely drugs to confer benefit as first-line treatment for most patients aged 55 or older.
Pharmacological
interventions
In hypertensive patients younger than 55 , the first choice for initial therapy should be an angiotensin-converting enzyme (ACE) inhibitor (or an angiotensin-II receptor antagonist if an ACE inhibitor is not tolerated).

14
Pharmacological
interventions
In hypertensive patients aged 55 or older or black patients of any age, the first choice for initial therapy should be either a calcium-channel blocker or a thiazide-type diuretic . For this recommendation, black patients are considered to be those of African or Caribbean descent, not mixed-race, Asian or Chinese.

15
Beta-blocker
Beta-blockers are no longer preferred as a routine initial therapy for hypertension
But consider them for younger people, particularly:� women of childbearing potential� patients with evidence of increased sympathetic drive� patients with intolerance of or contraindications to ACE
inhibitors and angiotensin-II receptor antagonists
If a patient taking a beta-blocker needs a second drug, add a calcium-channel blocker rather than a thiazide-type diuretic, to reduce the patient’s risk of developing diabetes.
Beta-blockerIf a patient’s blood pressure is not controlled by a regimen that includes a beta-blocker (that is, it is still above 140/90 mmHg), change their treatment by following the flow chart above.
If a patient’s blood pressure is well controlled (that is,140/90 mmHg or less) by a regimen that includes a beta-blocker, consider long-term management at their routine review. There is no absolute need toreplace the beta-blocker in this case.
When withdrawing a beta-blocker, step down the dose gradually.
Beta-blockers should not usually be withdrawn if a patient has a compelling indication for being treated with one, such as symptomatic angina or a previous myocardial infarction.

16
Pharmco-economic
Analysis
For 1st line treatment of essential hypertension (people at low risk of heart failure)Calcium Channel Blockers are the most cost effective option because they are associated with a low risk of diabetes and they also have a good effectiveness profileacross the range of other cardiovascular disease risks.
Target for blood
pressure control in CKD
With ACEI or ARB, reduce blood pressure to 130/80 mm HgIf urine protein >1 g/day, 120/75 mm HgIn type 2 diabetics, renal protection more clearly proven with ARB

17
Angiotensin converting
enzymes inhibitor
For the same degree of BP reduction, also reduce proteinuriaPreservation of renal function (small study)� Lisinopril (Zestril) slows renal deterioration� Can be combined with verapamil or
diltiazem
Angiotensin Receptor
Blocker
Irbesartan Diabetic nephropathy TrialRENAAL Trial (Reduction of end-points in NIDDM with AA Losartan)
Clear renoprotection in diabetic nephropathy in type 2 diabeticsNo head to head comparison with ACEI

18
Combination of ACEI and ARB Combination of ACEI and ARB Combination of ACEI and ARB Combination of ACEI and ARB
therapytherapytherapytherapy
Candesartan 16 mg and Lisinopril 20 mg Microalbuminuria Study (CALM)Combination therapy afforded greater reductions in blood pressure and albuminuria than either treatment alone. More complete blockage of the renin angiotensin system
K/DOQI Clinical practice
guidelines
Target� Reduction of proteinuria <1 g/day� blood pressure <130/80 mm Hg
Start with ACEI/ARBAdd DiureticsAdd non-dihydropyridine (verapamil or diltiazem)Add ARB/ACEI

19
Dialysis outcome
Blood pressure controlCa and phosphate controlHb around 11 – 12 g/dlNutrition of the patient, serum albumin >30 g/lDialysis dose

20
How to improve dialysis
outcome
The most important determinant is the FREQUENCY of dialysisProvide quality dialysis Affordable DialysisThree times per week
Daily dialysis in home HD case

21

22