how to create an attractive and supportive working environment for
TRANSCRIPT

POLICY BRIEF 15
HEALTH SYSTEMS AND POLICY ANALYSIS
How to create an attractiveand supportive workingenvironment for healthprofessionals
Christiane Wiskow, Tit Albreht and Carlo de Pietro

© World Health Organization 2010 and World HealthOrganization, on behalf of the European Observatoryon Health Systems and Policies 2010
Address requests about publications of the WHORegional Office for Europe to:
PublicationsWHO Regional Office for EuropeScherfigsvej 8DK-2100 Copenhagen Ø, Denmark
Alternatively, complete an online request form fordocumentation, health information, or for permissionto quote or translate, on the Regional Office web site(http://www.euro.who.int/pubrequest).
All rights reserved. The Regional Office for Europe ofthe World Health Organization welcomes requests forpermission to reproduce or translate its publications,in part or in full.
The designations employed and the presentation ofthe material in this publication do not imply theexpression of any opinion whatsoever on the part ofthe World Health Organization concerning the legalstatus of any country, territory, city or area or of itsauthorities, or concerning the delimitation of itsfrontiers or boundaries. Dotted lines on mapsrepresent approximate border lines for which theremay not yet be full agreement.
The mention of specific companies or of certainmanufacturers’ products does not imply that they areendorsed or recommended by the World HealthOrganization in preference to others of a similarnature that are not mentioned. Errors and omissionsexcepted, the names of proprietary products aredistinguished by initial capital letters.
All reasonable precautions have been taken by theWorld Health Organization to verify the informationcontained in this publication. However, the publishedmaterial is being distributed without warranty of anykind, either express or implied. The responsibility forthe interpretation and use of the material lies with thereader. In no event shall the World HealthOrganization be liable for damages arising from itsuse. The views expressed by authors, editors, or expertgroups do not necessarily represent the decisions orthe stated policy of the World Health Organization.
This policy brief is one of anew series to meet the needsof policy-makers and healthsystem managers.
The aim is to develop keymessages to supportevidence-informed policy-making, and the editors willcontinue to strengthen theseries by working withauthors to improve theconsideration given to policyoptions and implementation.
Keywords:
HEALTH PERSONNEL
PERSONNEL MANAGEMENT
JOB SATISFACTION
WORKPLACE - organizationand administration -standards
Authors
Christiane Wiskow, Independent HealthServices Specialist, Switzerland
Tit Albreht, Centre for Health System Analyses,Institute of Public Health of the Republic ofSlovenia, Slovenia
Carlo de Pietro, Centre for Research on Healthand Social Care Management, Bocconi University,Italy
Editors
WHO Regional Office forEurope and EuropeanObservatory on HealthSystems and Policies
EditorGovin Permanand
Associate EditorsJosep FiguerasManfred HuberJohn LavisDavid McDaidElias Mossialos
Managing EditorsKate Willows FrantzenJonathan NorthCaroline White
Guest EditorsLeen MeulenbergsWilly PalmMatthias Wismar
The authors and editors aregrateful to the reviewerswho commented on thispublication and contributedtheir expertise.
ContentsPage
Key messages
Executive summary
Policy brief
Policy issue: poor work environmentscompromise health-workforce supply and quality of care 1
How can attractive and supportive workenvironments be described? 4
What can be done to improve the health-sector work environment? 6
Implementation considerations 23
Summary 25
References 26
Annexes 33
No: 15
ISSN 1997-8073
How to create an attractive and supportiveworking environment for health professionals

Key messages
Policy issue and context: poor work environments compromise health-workforce supply and quality of care
• Health policy-makers face the challenge of matching increasing demandfor health care with a sufficient supply of health professionals in timesof existing and projected health-workforce shortages.
• The work environment constitutes an important factor in the recruitmentand retention of health professionals, and the characteristics of thework environment affect the quality of care both directly and indirectly.Addressing the work environment, therefore, plays a critical role inensuring both the supply of a health workforce and the enhancement,effectiveness and motivation of that workforce.
• The purpose of providing attractive and supportive work environments isto create incentives for entering – and remaining in – the health professions,and to provide conditions that enable health workers to perform effectively(to achieve high-quality health services).
Policy options
• Given the complexity of the work-environment issues to be addressed,policy responses need to be multidimensional, cross-cutting and inclusive.For coherent policies, policy action has to be considered at four levels:international/regional level; national level; sectoral level; and local/organizational level. Effective solutions are context-related and thereforepriority has to be given to the local and organizational level. The otherlevels provide the legislative and regulatory framework and provideguidance and support for the development of workplace policies.
• Two examples of what can be done to improve the quality of the workenvironment in the health professions include policy approaches to promotea healthy balance between family life and work, and the enhancement ofthe protection of workers’ health.
• In order to encourage health-sector employers to make a commitment topositive work environments, the development of workplace assessment/recognition programmes could be considered.
How to create an attractive and supportive working environment for health professionals
Implementation considerations
• As many factors influencing the work environment operate outwiththe health sector, intersectoral collaboration is required. In particular,the interface between labour and health-policy mandates needs tobe strengthened.
• Here, the use of social dialogue can help to ensure sustainable and cross-sectional implementation with multiple stakeholders.
Policy brief
Executive summary
Policy issue: poor work environments compromise health-workforcesupply and quality of care
European countries face common challenges in ensuring a well-performinghealth workforce in times of existing and projected shortages. One of themultiple aspects that determine the supply and performance of health workersis the work environment, which plays a critical role.
Given the demographic changes expected in the coming decades, labourmarkets will experience increased competition for talent. Recruitment andretention of health professionals are priorities in the health sector. Evidencesuggests that the work environment is an important factor in the recruitmentand retention of health workers.
Furthermore, the work environment can influence the quality of care. Itscharacteristics affect organizational functionality, individual satisfaction, thebalance between work and family life, continuous development, and theorganizational culture. Poor work environments contribute to medical errors,stress and “burn-out”, absenteeism and high levels of staff turnover, which,in turn, compromise the quality of care.
As a working definition, an attractive and supportive workplace can be describedas an environment that attracts individuals into the health professions, encouragesthem to remain in the health workforce and enables them to perform effectively.
In order to develop coherent policies to ensure a work environment thatattracts and retains health professionals, policy responses have to be consideredat four levels: international/regional level; national level; sectoral level; andlocal/organizational level. Improvement of the work environment will requirethe use of measures that are relevant to (and applicable in) the specific contextof a given health system. These measures should also observe internationalstandards and take account of regional harmonization efforts.
Effective solutions are context-related and therefore priority has to be givento the local and organizational level; the other levels provide the legislativeand regulatory framework, guidance and support for the development ofworkplace policies.
Policy options
One main trend observed in the health workforce is the drive towardsan improved work–life balance. A family-friendly work environment is ofparticular concern in the health sector because of the gender dimension ofthis issue. The majority of the health workforce is female, and an increasing
How to create an attractive and supportive working environment for health professionals
feminization of traditionally male-dominated professions can be observed.Work arrangements that allow a reconciling of family and work needs canenhance equal employment and career opportunities at times when familyresponsibilities are largely borne by women. Similarly, maternity protectionis highly relevant with regard to the mainly female health workforce and thepotential exposure to health risks in this workplace sector. Thus, the promotionof “family-friendly” workplace options and the enhancement of workers’health protection are domains in which concerted policy approaches canbe pursued.
More-specific policy responses here include the use of flexible working-timearrangements, specific protection from exposure to occupational risks, jobsecurity, compensation for reduced employment, maternity/parental leave andthe provision of child-care opportunities. These areas primarily require actionat organizational level, with support from national policies and legislation.
Additionally, health workers are exposed to a broad range of occupationalhealth risks because of the nature of their work: one-third of health workersperceive their health to be at risk because of their work. Thus it is crucial toimplement policies to ensure that the health work environment is as safe aspossible. The following areas are of particular relevance to the health workplace:exposure to biological risks, including infections caused by “sharps” injuries;and psychosocial risks, including stress and violence at work. Consequencesat the organizational level include absenteeism, reduced productivity, accidentsand errors.
There is a consensus that comprehensive occupational safety and healthmanagement systems are a solid way of establishing sustainable healthprotection at organizational level. Central to such systems are the preventionand control of health risks.
In terms of helping to advance work-environment issues, a promising approachlies in the development and adoption of processes and tools capable of assessingwork environments at organization level, comparing them, recognizing bestpractice and applying them across the system. This approach ideally combineselements that address the attractiveness of an organization for recruitmentand retention of health staff with elements of quality assurance for betterhealth outcomes.
More specifically, the use of workplace assessment and certification programmescould be considered. While some existing schemes may demonstrate certainlimitations regarding their application within the health sector (such as focusingon a single professional group, lacking a quality-of-care aspect or emphasizinghealth promotion in hospital settings), the development of a new frameworkfor assessment and certification programmes that could be used in the health
Policy brief
sector in different European countries might be useful. The role of national- andsectoral level measures is to encourage commitment (by health-sector employers)to improvements in work environments, for example through the support ofbenchmark studies and recognition programmes.
Implementation considerations
Many factors influencing the work environment operate outwith the healthsector. Intersectoral collaboration is therefore indispensible for approaches thatare effective at improving the working environment for the health workforce. Inparticular, the interface between labour and health-policy mandates should bestrengthened. Health policy-makers need to ensure that a systematic capacityfor addressing labour issues is available at all levels of the health system.
Social dialogue is a major means of achieving sustainable improvements inhealth services, and it is positively associated with improvement in workingconditions at the organizational level. At the European level, the SocialDialogue Committee for Hospitals of the European Union (EU) aims to improvethe quality of employment and the quality of services in the hospital sector bymeans of constructive social dialogue. There is a need to build the capacity ofthe social partners at national, sectoral and organizational levels in a numberof European countries.
How to create an attractive and supportive working environment for health professionals


1
How to create an attractive and supportive working environment for health professionals
Policy brief
Policy issue: poor work environments compromise health-workforcesupply and quality of care
European countries face common challenges in ensuring a well-performinghealth workforce in times of existing and projected shortages (1). Among themultiple aspects that determine the supply and performance of health workers,the work environment plays a critical role.
This Policy Brief considers policy approaches that can be employed to helpcreate positive work environments, thus improving the recruitment andretention of health professionals and contributing to the achievement of high-quality health services. Work-environment issues generally apply to all healthworkers in all types of health services – with variations according to thecharacteristics of professional functions or work settings. Without excludingtheir relevance for other professional groups in the health sector, this PolicyBrief focuses on approaches for physicians and nurses, as they represent thelargest constituents of the health workforce.
Recruitment and retention
The recruitment and retention of health professionals are priorities in the healthsector. In particular, the global debate on the international migration of healthprofessionals has triggered an increased interrogation of the reasons why healthworkers leave or stay. Related research has shown that the work environmentis an important factor in the recruitment and retention of health workers.
The main drivers for departure, the so-called “push factors”, are related tothe work environment, and include low pay, poor working conditions, limitededucational and career opportunities, unsafe workplaces and a lack of resourcesfor effective working. Also, elements of the wider socioeconomic environment– such as political and economic instability, the impact of the humanimmunodeficiency virus, or security issues – influence decisions to move. Healthworkers move to where they can find better conditions for work and life, so the“pull factors” mirror the push factors, and include higher pay, better-resourcedhealth systems, and opportunities for professional development (2,3).
Shortages in the health workforce induced research into the determinants ofearly exits from the health professions and the reasons why young people donot choose a health career. While dissatisfaction with pay levels is particularlypronounced in the nursing professions (58–90% in several European countries),other factors such as low esteem, limited work control and dissatisfaction withworking conditions appear to be even more-decisive reasons for leaving theprofession. With regard to physicians, a study from Germany found that
decision-making, recognition, job security, continuous education and collegialrelationships directly affected the level of job satisfaction (4).
The demographic changes (ageing populations and the decline of youngcohorts) in many countries in Europe (3,4) suggest that European labourmarkets will experience increased competition for talent in the coming decades.Health sectors are vital parts of national economies and constitute an importantlabour market in Europe: health-sector employment accounts for 10% ofoverall employment (5). Health professionals can compete well in the labourmarket and are much sought after. Moreover, the health labour market willhave to compete with other employers for the younger generations takingdecisions about their careers. As the health sector cannot change some of theunfavourable working conditions that characterize it, such as night work andwork during weekends and holidays, it will have to provide other incentivesthat will encourage young people to consider it.
Attracting more young candidates is also important in view of the fact thatthe health workforce is ageing in tandem with the overall population. This isnecessary partly because of the differences in age cohorts and partly becauseof the oscillating numbers of students across different periods (6). In mostcountries, more restrictions were introduced for admission to health studies atthe end of the twentieth century. These factors may affect developments withinindividual professional groups and could further complicate planning for humanresources in health.
Health services also face the paradoxical challenge of having to meet increasingdemand with reduced or limited resources. Demographic and epidemiologicaltransitions have an important impact on the development of health needs.Health care systems are still largely adjusted to the needs and expectations ofthe patterns commonly seen in acute patients with slow responsiveness anddifficult logistics. An alternative approach will have to be provided, not onlyin integrating different aspects of medical and health care, but also in offeringintegration across the different sectors, relevant for the needs of such patients.
At present, the health workforce in Europe is not structured to meet healthneeds and demands together with the challenges of the current and (short-term) projected epidemiological situations. It appears that the followingneeds will require consideration: more skills (predominantly in nursing care)for dealing with patients with chronic conditions; specialization of key healthprofessionals (medical doctors, nurses, physiotherapists) to deal with newdemands; and long-term care services (human resources as well as skills).These, in turn, should offer greater flexibility in organizing working time and,in particular, regarding working in different environments (such as patients’homes, homes for the elderly and nursing homes).
2
Policy brief
In Europe, approximately 70% of the health budget is allocated to salaries andemployment-related costs (7). Consequently, the focus on cost containmenthas marked many health-sector reforms with direct implications for the healthworkforce, such as increased employment insecurity (accompanying the moreflexible employment practices) and increased workloads (because of staffcuts or greater performance pressures) (WHO unpublished document 2005).Recent examples of responses to a loss of public funding include measuressuch as increased working hours for Estonian clinical staff, freezing of salariesin Bulgarian and Hungarian public hospitals, and cuts announced for public-service salaries in Ireland (with 14% losses in income expected for mid-levelcadre nurses and midwives) (8).
The costs associated with improvements in work environments need to bebalanced against the costs arising from turnover, absenteeism and medicalerrors caused by poor work environments. It has been estimated that the directand indirect costs of turnover, per nurse, accounted for US$ 16 600 in Australia,US$ 10 100 in Canada, US$ 10 200 in New Zealand and US$ 33 000 in theUnited States (4).
Work environment and quality of care
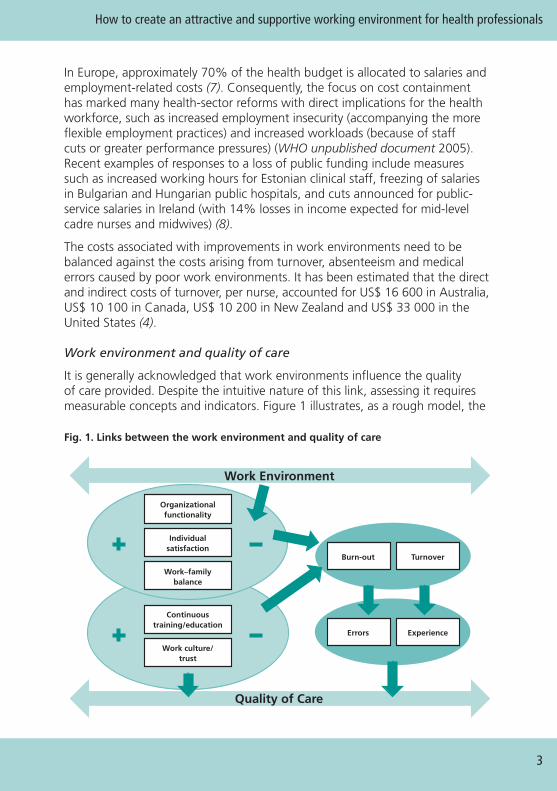
It is generally acknowledged that work environments influence the qualityof care provided. Despite the intuitive nature of this link, assessing it requiresmeasurable concepts and indicators. Figure 1 illustrates, as a rough model, the
3
How to create an attractive and supportive working environment for health professionals
Work Environment
Quality of Care
Organizationalfunctionality
Burn-out Turnover
Errors Experience
Individualsatisfaction
Work–familybalance
Continuoustraining/education
Work culture/trust
Fig. 1. Links between the work environment and quality of care
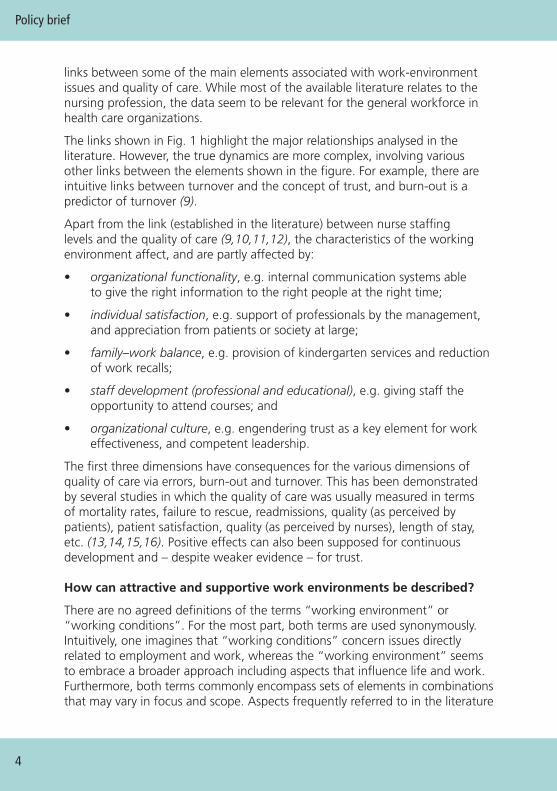
links between some of the main elements associated with work-environmentissues and quality of care. While most of the available literature relates to thenursing profession, the data seem to be relevant for the general workforce inhealth care organizations.
The links shown in Fig. 1 highlight the major relationships analysed in theliterature. However, the true dynamics are more complex, involving variousother links between the elements shown in the figure. For example, there areintuitive links between turnover and the concept of trust, and burn-out is apredictor of turnover (9).
Apart from the link (established in the literature) between nurse staffinglevels and the quality of care (9,10,11,12), the characteristics of the workingenvironment affect, and are partly affected by:
• organizational functionality, e.g. internal communication systems ableto give the right information to the right people at the right time;
• individual satisfaction, e.g. support of professionals by the management,and appreciation from patients or society at large;
• family–work balance, e.g. provision of kindergarten services and reductionof work recalls;
• staff development (professional and educational), e.g. giving staff theopportunity to attend courses; and
• organizational culture, e.g. engendering trust as a key element for workeffectiveness, and competent leadership.
The first three dimensions have consequences for the various dimensions ofquality of care via errors, burn-out and turnover. This has been demonstratedby several studies in which the quality of care was usually measured in termsof mortality rates, failure to rescue, readmissions, quality (as perceived bypatients), patient satisfaction, quality (as perceived by nurses), length of stay,etc. (13,14,15,16). Positive effects can also been supposed for continuousdevelopment and – despite weaker evidence – for trust.
How can attractive and supportive work environments be described?
There are no agreed definitions of the terms “working environment” or“working conditions”. For the most part, both terms are used synonymously.Intuitively, one imagines that “working conditions” concern issues directlyrelated to employment and work, whereas the “working environment” seemsto embrace a broader approach including aspects that influence life and work.Furthermore, both terms commonly encompass sets of elements in combinationsthat may vary in focus and scope. Aspects frequently referred to in the literature
Policy brief
4
include terms of employment (e.g. types of contracts), income (payment andbenefits), working time, safety and health at work, professional development(including education and training) and work organization (including staffingand division of work). Nevertheless, the work environment generally could bedescribed as the place, conditions and surrounding influences in which peoplecarry out an activity (17,18).
An “attractive and supportive work environment” refers to the quality dimensionof work. In this regard, an attractive and supportive work environment can bedescribed as an environment that attracts individuals into the health professions,encourages them to remain in the health workforce and enables them to performeffectively. The purpose of providing attractive work environments is to createincentives for entering the health professions (recruitment) and for remainingin the health workforce (retention). In addition, supportive work environmentsprovide conditions that enable health workers to perform effectively, makingbest use of their knowledge, skills and competences and the available resourcesin order to provide high-quality health services. This is the interface of the workenvironment and quality of care.
In the EU, improvement of the quality of work has been an integrative part ofthe European Social Agenda and the European Employment Guidelines since2000, as illustrated in the strategy motto “more and better jobs” (19,20). Sincethen there has been debate as to what “quality of work” encompasses andhow it could be measured, reflecting the changes in socioeconomic realitiesand developments in the world of work (21).
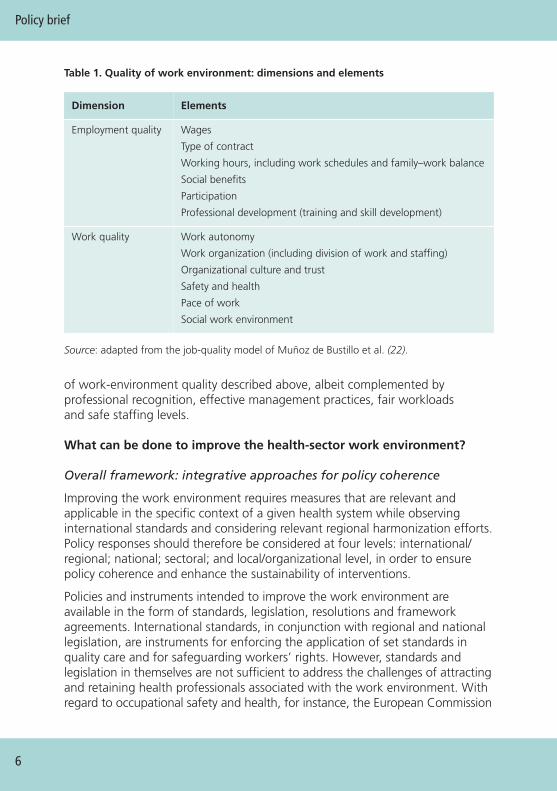
In this context, a recent review of quality indicators proposed a general modelfor the quality of work (22). The authors distinguished two main dimensions:“work quality” – the material characteristics of the task performed and theenvironment within which it is performed; and “employment quality”, referringto the contractual relationship between employer and employee. Both areasinfluence the overall quality of the work environment or, as the authors calledit, “job quality”. Table 1 captures the main dimensions and elements of work-environment quality.
With regard to the health sector, different approaches for describing the qualityof work can be used. They may tackle the subject from different angles accordingto the viewpoints from which they are derived; for example, in the case of theMagnet hospitals concept, the emphasis is on aspects that are particularlyimportant from the perspective of nursing professionals.
The Positive Practice Campaign, jointly launched by world health-professionalassociations in 2008, describes characteristics of work environments that ensurethe health, safety and well-being of staff, while simultaneously supportinghigh-quality patient care (23). These characteristics mainly reflect the elements
5
How to create an attractive and supportive working environment for health professionals
Policy brief
6
of work-environment quality described above, albeit complemented byprofessional recognition, effective management practices, fair workloadsand safe staffing levels.
What can be done to improve the health-sector work environment?
Overall framework: integrative approaches for policy coherence
Improving the work environment requires measures that are relevant andapplicable in the specific context of a given health system while observinginternational standards and considering relevant regional harmonization efforts.Policy responses should therefore be considered at four levels: international/regional; national; sectoral; and local/organizational level, in order to ensurepolicy coherence and enhance the sustainability of interventions.
Policies and instruments intended to improve the work environment areavailable in the form of standards, legislation, resolutions and frameworkagreements. International standards, in conjunction with regional and nationallegislation, are instruments for enforcing the application of set standards inquality care and for safeguarding workers’ rights. However, standards andlegislation in themselves are not sufficient to address the challenges of attractingand retaining health professionals associated with the work environment. Withregard to occupational safety and health, for instance, the European Commission
Table 1. Quality of work environment: dimensions and elements
Dimension Elements
Employment quality Wages
Type of contract
Working hours, including work schedules and family–work balance
Social benefits
Participation
Professional development (training and skill development)
Work quality Work autonomy
Work organization (including division of work and staffing)
Organizational culture and trust
Safety and health
Pace of work
Social work environment
Source: adapted from the job-quality model of Muñoz de Bustillo et al. (22).
observed shortcomings in the application of Community legislation, especiallyin sectors at risk and for vulnerable workers (24). As many instruments atinternational and national levels are general in their scope, the role of thesectoral level is to identify relevant standards and policies and adapt themto the specificities of a given health-sector work environment.
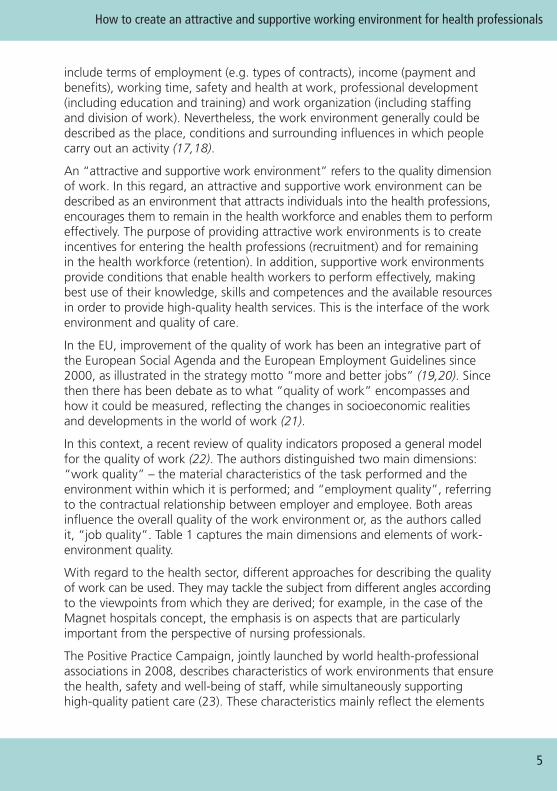
In view of the pace of socioeconomic and technological changes and theirconsiderable impact on employment and working conditions, policy responsesneed to reflect emerging challenges on a continuous basis. It is the organizationallevel that faces the challenge of translating policies into practice and adaptinginterventions (in a timely manner) to trends and changes in the work realities.Effective solutions are context-related and so priority has to be given to the localand organizational level; the other levels provide the legislative and regulatoryframework, guidance and support for the development of workplace policies.The organizational level is concerned with monitoring trends and providingfeedback on emerging new challenges that require action at other levels.Figure 2 summarizes examples of interventions and issues relating to eachof the four levels.
Fig. 2. Levels of policies and interventions
There are a multitude of challenges concerning the work environment andthey can be responded to using a variety of policies. Improving remunerationis one of the obvious policy options that are usually discussed. However, payincreases alone are not the solution, as other factors appear to be even moreimportant (4). Indeed, the factors influencing the work environment aremultidimensional and often interrelated, so strategies should include differentsets of combined interventions – perhaps including remuneration – and mightimply action at different policy levels at the same time. Box 1 illustrates twoexamples of national policies intended to improve the supply of nurses.
7
How to create an attractive and supportive working environment for health professionals
• Standards• Codes of practice• Directives• Guidelines
• Legislation• Regulation• Guidelines• Compliance with international/ regional legislation and policies• Surveillance
• Identification of relevant standards/ legislation• Translating standards/ legislation to health sector• Tailoring guidelines to health sector and health occupations• Monitoring application
• Implementation in the work setting:• Compliance with legislation and standards• Measures tailored to health facility and workplaces• Monitoring and feedback on trends and emerging needs
International/regional National
Sectoral(health sector) Organizational
Policy brief
8
Box 1. Examples of national policies designed to improve nurse recruitmentand retention
Czech Republic
To address a serious shortage of nurses, the Czech Republic launched a programmeof “stabilization measures” in 2008. The mix of interventions included the following:
• financial measures – grading nurses into higher salary grades and improving benefitsin public-health facilities;
• professional development – better access to nurse-specialist education, withsubsidies from government; support of modern continuous professionaldevelopment programmes;
• professional autonomy – negotiations and legislative changes to broaden nursecompetences;
• family–work balance – support to assist return from maternity leave, includingprovision of child-care facilities, flexible working hours and part-time contracts; and
• workforce data – monitoring of workforce and student numbers via a register ofhealth care professionals.
By 2009, the shortage was reduced by half, partly as a result of these measures,but probably also because of the economic situation (increased unemployment).
Belgium
With the aim to improving the attractiveness of the nursing profession and the qualityof care, a four-year national plan was launched in 2008, supported by significant publicinvestment. A combination of interventions are being implemented in the following fourmain action areas.
• Workloads and stress levels of nurses are being eased (via more staff, supportive actionfor upgrading auxiliary qualifications, and provision of information technology systemsfor reducing administrative work).
• Qualifications are being addressed (using more continuous training, more specialization,and the introduction of master’s degrees).
• Remuneration is being changed (i.e. bonuses were paid for work done during “unsocialhours”, and pay was increased for recognized specialties and nurse-executive positions).
• Social recognition and participation in decision-making are being addressed (throughsupport of nurse representation within health authorities and bodies).
Sources: presentations by national experts at the Policy Dialogues, Leuven, April 2010 (unpublished);(Safrankova A, Di Cara V, Czech Republic; Lardennois M, Belgium).
This section explores two policy approaches designed to address specific work-environment issues. It focuses on selective examples of issues illustrating thepossibilities at a pragmatic level, i.e. in terms of the work/family-life balanceand health and safety at work.
The aspiration towards work–life balance models is one of the main trendsobserved in the literature, and it has been noted that family-friendly policiesimprove the retention of health professionals (25). Safety/health concernsare major reasons for early exit from the health professions, and can resultin considerable costs in relation to ill-health, absenteeism and staff turnover.These two examples are relevant for all professional groups and work settingsand also offer a low-threshold entry point with possibilities for action at theorganizational level.
Promotion of family-friendly workplace options to improve thework environment
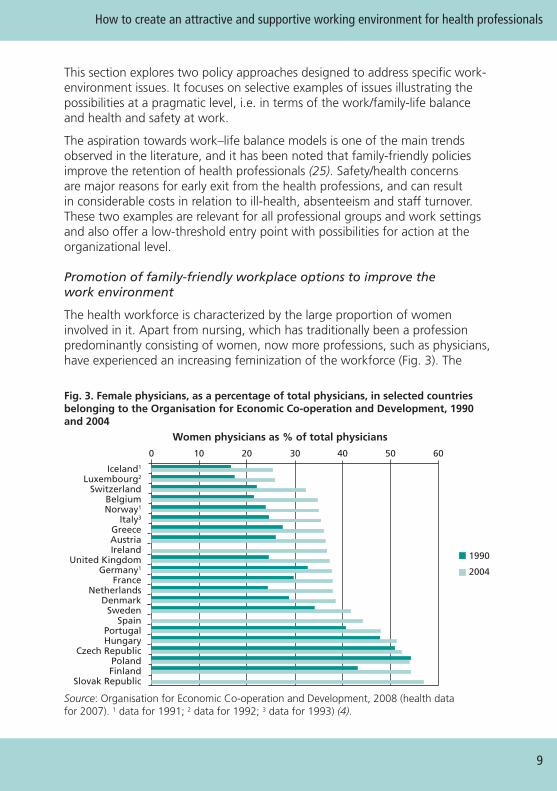
The health workforce is characterized by the large proportion of womeninvolved in it. Apart from nursing, which has traditionally been a professionpredominantly consisting of women, now more professions, such as physicians,have experienced an increasing feminization of the workforce (Fig. 3). The
9
How to create an attractive and supportive working environment for health professionals
Women physicians as % of total physicians
1990
2004
0 10 20 30 40 50 60
Iceland1
Luxembourg2
SwitzerlandBelgiumNorway1
Italy3
GreeceAustriaIreland
United KingdomGermany1
FranceNetherlands
DenmarkSweden
SpainPortugalHungary
Czech RepublicPolandFinland
Slovak Republic
Source: Organisation for Economic Co-operation and Development, 2008 (health datafor 2007). 1 data for 1991; 2 data for 1992; 3 data for 1993) (4).
Fig. 3. Female physicians, as a percentage of total physicians, in selected countriesbelonging to the Organisation for Economic Co-operation and Development, 1990and 2004
majority of medical students in most European countries are women: womenconstitute 70% of the medical school intake in the United Kingdom andrepresent 59.5% of new graduates in Belgium (26,27). This is a result of moreequal opportunities in career choice. Such a development, however, brings newchallenges, as it requires the consideration of the specific needs of women andmen at work. Indeed, women participate in the health workforce differently incomparison with men. Female physicians tend to work fewer hours, to leavepractice completely (or practice at low levels), particularly during childbearingage, and are more likely to leave early for retirement (28).
As women carry the major part of family responsibilities, they often face moreobstacles in their career development compared to their male colleagues. Thisis often evidenced by the expectations that a career-oriented person shouldwork longer hours, not be absent due to various family obligations, and so on.Such attitudes can cause major disadvantages for professionals with familyresponsibilities, notably women. An equal-opportunity approach is thereforenecessary in order not to discriminate against female health professionals,especially in the early phases of their careers. The conflict between the demandsof work and those of family life is also affecting men where they share child-care and other family duties. The pressure for change towards a more equitableand gender-balanced workplace is increasing, not just because of the growingnumbers of women pursuing careers, but also because many of them are nowtaking up management roles.
A specific element here is that of maternity-related issues. The work environmentneeds to accommodate pregnancy as a normal event in the career of a femalehealth professional, and offer adequate workplace arrangements to supportthe needs of pregnant women. Only such an organizational culture can providean environment in which female health professionals will feel that they areequal to their male counterparts and that they have an incentive to combinetheir family and work lives. Supporting these needs may become an importantincentive for young people seeking to pursue careers in health care.
Failure to address the conflict between the demands of work and those offamily life may lead to adverse consequences, such as stress and burn-outsyndrome (29), increased absenteeism, the need to leave employment inorder to take care of family responsibilities, and reduced interest in the healthprofessions among young people deciding on their careers. Such developmentshave already been described and are relevant to almost any country in Europe,especially where failure to reconcile family life and professional life ends in“non employment” (30).
By building on existing instruments, positive approaches and experiences,different interventions can be developed at each of the four different levels,as follows.
Policy brief
10
International level
Various international conventions are available that provide frameworks andstandards for family-friendly workplace policies. Besides various conventions onmaternity protection, the 1981 International Labour Organization Conventionon Workers with Family Responsibilities provides for equal opportunities for –and treatment of – women and men with family responsibilities. This Conventionhas been ratified by a number of European countries (31). At EU level, the 2008guidelines for employment policies of the Member States suggested, for example,the use of benchmarks for child-care provision at national level, to promotereconciliation between work life and family life (20).
National level
Maternity protection differs from country to country, but the most importantfeatures of the social state policies with respect to pregnancy include job security,protection at the workplace, maternity leave and financial compensation forreduced employment (32). Regulation may include flexible-hours arrangements,possibilities for reduced working hours, restrictions on work during night shifts,less exposure to risky work conditions, and protection of pregnant women atthe workplace. Box 2 provides an example of how national legislation caninfluence gender equality in the context of parenthood.
Health-sector level
Regulations should be adapted to the specific requirements of a health workplace,with support being provided to organizations that seek to implement family-friendly workplace policies. For example, additional requirements could beprovided to regulate the certification of health care providers with respectto family-friendly workplaces, such as incentives for solutions that supportemployment of parents with small children.
11
How to create an attractive and supportive working environment for health professionals
Box 2. Family–work balance and equal opportunities
Iceland, which is a country with a female labour participation level of 90% and high birthrates, introduced new legislation in 2000 that structured maternity/paternity leave in a waythat was designed to ensure gender equality. Upon the birth or adoption of a child, bothparents are entitled to three months of paid leave, which is not transferable. Should oneof them decide not to take this leave, then it is lost. Both parents have a joint entitlementto an additional three months of leave at 80% pay, which they can share and use flexibly.After three years, there has been a significant increase in the proportions of men takingpaternal leave (92% of fathers using the first three months of paternal leave).
Sources: presentation by a national expert at the Policy dialogues, Leuven, April 2010 (unpublished);Ministry of Social Affairs and Social Security (33).
Organizational level
With regard to maternity protection measures at organizational level, thefollowing areas can be covered:
• seamless passage from “regular” workplace loads to “adapted”workloads, whenever necessary and required by pregnancy;
• securing of workplaces so that exposure to harmful agents is minimizedto reduce danger for both the mother and the baby; and
• allowing flexible working hours.
Arrangements that encourage a balance between family and work can include:
• parental leave;
• company leave because of a sick child;
• the right to reduced working hours for a period of time; and
• support for, or the offer of, child-care facilities.
Box 3 provides examples of family-friendly policies in practice in variousGerman hospitals.
Policy brief
12
Box 3. Elements of family-friendly policies in German hospitals
Lutherhaus Protestant Hospital, Essen, introduced a scheme of 50 different part-timemodels, including:
• qualified part-time employment (15–93% of full-time employment);
• job-sharing, particularly for managerial functions;
• coordination of duty rosters of couples across different departments;
• establishment of time accounts (plus and minus hours); and
• flexible working hours (“flexitime”), with family-oriented core times.
The University Hospital Charité, Berlin, established a “fathers representative”, who advisesmen on questions concerning family–work balance.
The Medical University, Hannover, provides financial incentives for departments that attractfemale doctors back to work from parental leave within one year.
Northwest Hospital Sanderbusch, Sande, is a member of the network “Success Factor Family”and attracts qualified professionals to its remote area with its “family and children servicedepartment”, supporting child-care solutions, including the option of partly working from home.
Sources: Bundesministerium für Familie, Senioren, Frauen und Jugend, 2009 (34); Müller B, 2005 (35).
Enhancing the protection of health workers’ health to ensure a saferwork environment
Working in health care is hazardous: the health sector has been identified, inparticular, as one of the dangerous employment sectors (36). In 2000, one inthree health and social workers (32%) in the EU15 perceived that their healthat risk because of their work (37), and in 2005, nearly 40% of health workersin the EU27 felt that their work had an impact on their health (38).
Health workers are exposed to a broad range of occupational health risksbecause of the nature of their work, including:
• biological risks, such as infections caused by sharps injuries or othercontact with pathogens;
• chemical risks, such as disinfectants or certain types of drugs;
• physical risks, such as ionizing radiation;
• ergonomic risks, arising from patient handling or extensive standingand walking; and
• psychosocial risks, such as stress, violence and shift work. (39)
Without negating the importance of other hazards, such as ergonomic risks(40, 37), we focus here on two risk categories of particular concern – biologicaland psychosocial risks.
Exposure to biological risks is substantially higher in the health sector comparedto the mean exposure in other EU employment sectors (38), the followingissues being particularly relevant to health workers.
• Re-emerging and drug-resistant types of infectious diseases, such astuberculosis or malaria, pose potential risks.
• Newly emergent infectious diseases pose a threat where transmissionpathways are unknown and protective equipment is inadequate (41) –e.g. the outbreak of SARS (severe acute respiratory syndrome), duringwhich health care workers representing up to 50% of reported cases (42).
• Injuries can be sustained from handling contaminated waste, particularlyneedlesticks and other sharps. It has been estimated that one millionneedlestick injuries occur annually in Europe, each of which has thepotential to transmit more than 20 dangerous blood-borne pathogens,including hepatitis B, hepatitis C and human immunodeficiency virus.Most at risk are nurses and doctors. However, other staff members thathandle waste must also be considered, for example auxiliaries, cleanersand laundry staff (43). A study in Germany found that 500 000 sharpsinjuries occurred in hospitals annually; in the United Kingdom,
13
How to create an attractive and supportive working environment for health professionals
Policy brief
14
100 000 incidents per year were estimated to occur. The Scottish NationalHealth Service estimated the costs associated with needlestick injuries asranging from several thousand Euros per case (for post-exposure prophylaxis)up to one million Euros (for an injury resulting in transfer of a seriousblood-borne virus) (44).
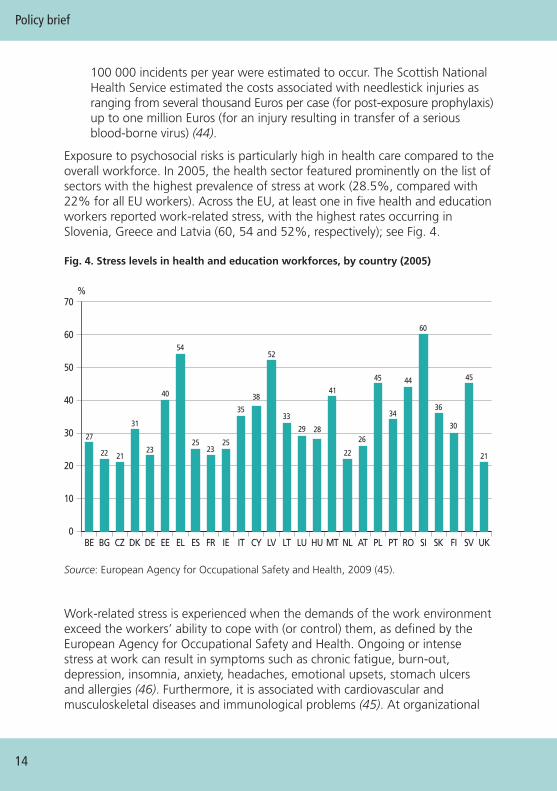
Exposure to psychosocial risks is particularly high in health care compared to theoverall workforce. In 2005, the health sector featured prominently on the list ofsectors with the highest prevalence of stress at work (28.5%, compared with22% for all EU workers). Across the EU, at least one in five health and educationworkers reported work-related stress, with the highest rates occurring inSlovenia, Greece and Latvia (60, 54 and 52%, respectively); see Fig. 4.
Fig. 4. Stress levels in health and education workforces, by country (2005)
Source: European Agency for Occupational Safety and Health, 2009 (45).
Work-related stress is experienced when the demands of the work environmentexceed the workers’ ability to cope with (or control) them, as defined by theEuropean Agency for Occupational Safety and Health. Ongoing or intensestress at work can result in symptoms such as chronic fatigue, burn-out,depression, insomnia, anxiety, headaches, emotional upsets, stomach ulcersand allergies (46). Furthermore, it is associated with cardiovascular andmusculoskeletal diseases and immunological problems (45). At organizational
0
10
20
30
40
50
60
70
UKSVFISKSIROPTPLATNLMTHULULTLVCYITIEFRESELEEDEDKCZBGBE
%
27
22 22
26
21 21
31
23
40 41
45 44
54
25
35 3436
30
45
38
29
33
23
28
52
60
25
level, the consequences include absenteeism, high staff turnover, reducedproductivity, accidents and errors (47).
The job characteristics that contribute to stress are mostly related to theway in which the work is organized (e.g. long hours and irregular work,high workloads, tight time constraints, lack of control, job insecurity). InSwitzerland, for example, one-third of primary care doctors in a representativesurvey reported experiencing excessive stress due to overall workload, patients’expectations, difficulties in balancing professional and private life, economicconstraints in relation to the practice, medical care uncertainty and difficultwork relations (48). According to one model, stress levels are mitigated whereworkers are supported by their colleagues and supervisors, but are increasedwhere social support is missing (45,46).
Work strain can also result from organizational change – such as socioeconomictransformation – in the health-sector context. A Bulgarian survey exploredstress at work in the context of transition, where differing paces in theimplementation of financing reforms led to conflicts between various healthunits, provoked by significant differences in the salaries of health workers.Tension between patients and health staff emerged when a number of freeservices were abolished (49).
It has been highlighted that of all the work sectors in the EU27 MemberStates, the health sector has the highest level of incidents involving violenceand harassment at work (15.2%). Health workers have been shown to be eighttimes more likely to experience the threat of physical violence than workers inthe manufacturing sector (38). The most-affected health professionals includeambulance staff, nurses and doctors. Recognized risk factors – including workingwith the public, working with people in distress, and working alone – are allprevalent in the health sector. Most incidents of aggressive behaviour experiencedby staff were at the hands of patients, while psychological abuse was associatedwith supervisors and colleagues. Psychological violence was more prevalent thanphysical violence as shown in a synthesis of several country case studies (50). InPortugal, for example, a survey of a health-centre complex and a large hospitalfound that 51% and 27% of staff, respectively, had experienced verbal abuse,23% and 16%, respectively, had experienced bullying/mobbing, while theexperience of physical violence was limited to 3% at both study sites
The negative impact on affected staff (as confirmed by case studies in severalcountries) include post-traumatic stress symptoms, such as disturbing memoriesand thoughts, and a tendency to become highly vigilant. At the organizationallevel, the impact is similar to that of stress, causing absenteeism, high staffturnover and reduced productivity (50).
15
How to create an attractive and supportive working environment for health professionals
Policy responses to occupational health challenges
Protecting the health of workers at work is a legal, if not moral, responsibilityof employers. Workers, too, have their own responsibilities here in complyingwith safety regulations and taking care of their health in their own scope ofinfluence. There is a consensus that comprehensive occupational safety andhealth management systems are a solid way of establishing sustainable healthprotection at organizational level. Central to this system is the prevention orcontrol of health risks using a widely applied hierarchy of priorities: eliminationof the risk; control of the risk; minimization of the risk; and provision ofprotective equipment (51).
While priority has to be given to action at organizational level, internationaland regional policies are important for encouraging initiatives in countries. In2007, the World Health Assembly adopted a resolution on the World HealthOrganization’s Global Plan of Action on Workers’ Health, 2008–2017. Thisprovides for the establishment of specific programmes for the occupationalhealth and safety of health care workers (52). With regard to health workers,WHO’s own programme of work for 2009–2012 focuses on six areas, including:
• needlestick/sharps-injury prevention
• musculoskeletal injuries/ergonomics
• stress/work organization
• pharmaceutical-associated risks
• respiratory risks
• risk assessment/risk-management tools and information dissemination.
Examples of projects that have been initiated under this programme in theEuropean region are listed in Table 2.
The initiatives taken to address the insufficient prevention of sharps injuriesare an example of advocacy by health professional associations in influencingpolicies at European level. Following a campaign, a consultation processwas launched which resulted in negotiation and signature of the FrameworkAgreement on the Prevention from Sharp Injuries in the Hospital andHealthcare Sector. The signatories were the following European social partners:the European Hospital and Healthcare Employers’ Association (HOSPEEM) theEuropean Federation of Public Service Unions (EPSU). With the recent adoptionof a European Commission proposal for a Council Directive, it is expectedthat the Framework Agreement will be given legal status, making it bindingfor Member States (54,55). Figure 5 plots the chronology of this prospectiveEU legislation.
Policy brief
16

Fig. 5. Advocacy initiative and process for introduction of European binding measuresfor protection from needlestick injuries and other medical sharps injuries
Source: based on De Raeve, 2010 (56), and EU Issue Tracker, 2009 (54).
17
How to create an attractive and supportive working environment for health professionals
Table 2. WHO projects on occupational health for health workers in Europe, 2009–2012 (53)
Projects Countries
Countries in transition: how to promote health at work in health organizations
Main objective: to raise awareness and improve knowledge and skills of healthcare workers in tackling work-related stress.
Croatia,Macedonia,Montenegro,Serbia
How to maintain health care workers’ workability and quality of life
Main objective: to produce a guidance document that includes a range ofsuccessful initiatives adopted by the Croatian Ministry of Health and SocialWelfare in order to improve health care workers’ work ability and qualityof life.
Croatia
Assessment of exposure to antineoplastic agents in pharmacy andhospital personnel
Objective: examination of safe working conditions related to the handling ofantineoplastic drugs during drug preparation or administration in hospitals.
Germany
2004
2006
2006–2009
2009
• EFN Awareness Campaign European Parliament• Joint EFN–ICN statement: Nurses call for EU action aimed at safer needle devices
• European Commission launches consultation process with social partners• European social partners (HOSPEEM & EPSU) negotiation on a framework agreement
• Framework Agreement on the prevention from sharp injuries in the hospital and healthcare sector signed by HOSPEEM & EPSU • Request to submit the Agreement to the Council for a Council Directive• EC adopts proposal for a Council Directive to give legal effect to the Framework Agreement signed by HOSPEEM & EPSU
• European Parliament resolution with recommendations to the Commission on protecting European healthcare workers from blood-borne infections due to needlestick injuries (2006/2015(INI))
WHO suggests that a combination of measures using a hierarchy of controlsis the most effective way of reducing the number of needlestick injuries. Coreelements include the use of safer instruments, regular training and instruction,and established safe working procedures (57). Accordingly, the FrameworkAgreement recommends establishing an integrative approach at the workplace,consisting of risk assessment, risk prevention, training, information, awareness-raising and monitoring. Both risk assessment and risk prevention should coverthe following areas: technology; organization of work; working conditions;level of qualification; work-related psychosocial factors; and the influence offactors on the work environment. Furthermore, the Framework Agreementprovides for the vaccination of health workers according to national practice (58).
Interventions addressing the complexity of psychosocial risk factors and theircauses are grouped into the following three categories.
• Organizational level interventions aim to reduce the risk of stress,addressing organizational structure, infrastructure or work processes.
• Interventions at the interface between organizational and individuallevels may include improving collegial relationships at work, or trainingindividuals to adapt better to the work-environment measures for optimalprofessional autonomy.
• Individual-level interventions aim to reduce the stress and disease risk ofthose who have already symptoms, by strengthening the capacity to copewith stress (45).
Box 4 presents an example of an approach designed to prevent burn-outamong hospital staff.
In many jurisdictions, violence and harassment continue to be perceived byhealth workers as “part of the job”. Therefore, awareness and recognition ofviolence as a risk at the health workplace are necessary first steps on the wayto violence prevention and the protection of staff. The specific societal andcultural context of the work environment needs to be considered, as well asthe gender dimension, in reaching a shared understanding of the phenomenon.Any approach intended to address workplace violence should be integrated,participative, culture- and gender-sensitive, non-discriminatory and systematic.
The main areas of action include the prevention and control of workplaceviolence and the management and mitigation of its impact, with an emphasison the support of workers affected by workplace violence (60). As Box 5highlights, research initiatives have the potential to raise awareness and actas a trigger for processes of policy development.
Policy brief
18

19
How to create an attractive and supportive working environment for health professionals
Box 4. “Take Care” – a team-based burn-out intervention programme in the Netherlands
The Take Care intervention project was carried out in 1997–1998 in order to prevent burn-out among oncology care workers, through a team-based stress-management approach.The programme consisted of six training sessions of three hours each, one per month,which were supervised by counsellors.
During the first session, the focuses of action were determined. During the training, smallproblem-solving teams were formed that collectively designed, implemented, evaluatedand reformulated plans of action for coping with the most important stressors at work.Counsellors also provided training in more general communication and collaboration skills,and participants were their own “agents of change”, with the counsellors as their “coaches”.
The problems that were most frequently addressed were those concerned with coping withhigh emotional demands in relationships with cancer patients, and those involving dealingwith communication problems between members of different professional disciplines.
The results of a qualitative evaluation showed that participants considered the approach tobe very instructive and useful for charting work stressors and for formulating and evaluatingplans of action designed to tackle these stressors. The most appreciated part of the activitywas the building of a network of (social) support among colleagues.
Source: European Agency for Occupational Safety and Health, 2002 (59).
Box 5. From lack of awareness to the development of measures as part of thenational collective agreement
As part of the ILO/ICN/WHO/PSI Joint Programme (involving the International LabourOrganization, the International Council of Nurses, WHO and Public Services International)on Workplace Violence in the Health Sector, Bulgaria’s first survey in 2001 revealed thathealth workers and the public were unaware of the problem. Results showed that itssignificance was largely underestimated and was interpreted rather as a hardship facingpeople in their daily life, and stress due to the negative consequences of Bulgaria’s thenreform process.
In 2003, a tripartite national workshop was organized by the Federation of Health TradeUnions affiliated to the Confederation of Independent Trade Unions in Bulgaria and theMedical Federation of the Confederation of Labour Podkrepa. The main findings of thecountry study were discussed, and the Bulgarian version of the ILO/ICN/WHO/PSI FrameworkGuidelines on workplace violence was launched. The delegates adopted a 2003–2005 actionplan, with a commitment to further action.
One of the most important achievements at national level was the inclusion of the issue ofworkplace violence in the health-sector collective agreement for 2004. Other activities wereaimed at awareness-raising, capacity-building and prevention of violence, and includedseminars on security measures, reporting procedures and victim support.
Source: Kokalov, 2006 (61).
Advancing work-environment issues among employers, thoughworkplace screening and certification
A third policy approach, this time focusing on the process aspects of how work-environment issues can be taken forward at organizational level, considersprogrammes for workplace assessment and certification. These may provideincentives encouraging employers to commit to the concept of positive workenvironments. The role of national- and sectoral-level actions here could be toprovide a framework, as well as political and financial support. This approachcan be illustrated by the following two examples. The first example involvesranking initiatives, with lists of the best companies, such as those generated bythe Great Place to Work Institute. The second example – the Health PromotingHospitals Network – represents an integrative approach that providespossibilities for self-assessment.
The Great Place To Work® model
The Great Place To Work® model is a method for assessing and optimizingorganizational culture, and was developed by the Great Place To Work Institute,an American consultancy firm. The Institute uses a questionnaire survey foremployees and interviews with the management in order to assess theorganizational culture. Two-thirds of the evaluation is based on the employee-survey results.
The German branch of the Great Place To Work Institute, in collaborationwith the Ministry of Labour and other partners, has carried out an annualbenchmarking survey specifically addressing the health sector. Participatinghealth-service organizations are ranked and the best are awarded the “BestHealth Sector Employer” Certificate (Beste Arbeitgeber im Gesundheitswesen).Sixty-three health-service organizations participated in the 2010 survey onworkplace culture, and the results show that health and well-being, recognitionand work–life balance are critical issues, with remuneration as a key (but lessimportant) element (Great Place to Work Institute Germany, unpublisheddocument 2010).
This model is based on the conviction that organizational culture is a decisivefactor in the productivity of a company. The value-based approach emphasizestrust as a core component of a positive workplace environment. Trustfulrelationships at work, specifically between management and staff, are criticalfor successful operations. Values include credibility, respect, fairness, pride andteam spirit. In this approach, a positive work environment is characterized bytrust in the leadership of an organization, pride in the work carried out, andcooperation with the people in the workplace.
Policy brief
20
The model applies to all industries and, above all, to manufacturing, informationand communication technologies and financial institutions. The strengths of themodel include the following features.
• Its key concept/element, i.e. trust, is fundamental in a workingenvironment involving information asymmetries and professionals(e.g. health care organizations).
• The questionnaires are easy to use but they do not involve self-assessment,as the survey and evaluation are carried out by the Institute.
A weakness of the model is that it does not link to quality of health care orpatient outcomes. However, some health facilities have been using the assessmentas a complementary instrument in combination with the regular quality-management system, sometimes also alternating with patient-satisfaction surveys.
Box 6 profiles the “Magnet hospital” model in the United States, which aimsto improve the work environment for nurses.
21
How to create an attractive and supportive working environment for health professionals
Box 6. “Magnet” hospitals and the Magnet Recognition Program
The concept of the Magnet hospital was developed initially in the 1980s in the UnitedStates by the American Academy of Nursing (62). The initial focus was to identify thehuman-resource practices and organizational characteristics that enabled some hospitalsto attract and retain staff in a context of acute shortages (see Annex 1). The basic featuresof Magnet hospitals involve investment in staff development, quality management, front-line management supervisory ability, and good relationships with physicians (63). Thecharacteristics of “magnetism” have been summarized in a Nursing Work Index, measuredusing questionnaires filled out by nurses (64). This idea has been developed over successivedecades through research and the implementation of a voluntary programme of hospitalaccreditation, the Magnet Recognition Program, undertaken by the American NursesCredentialing Center (a subsidiary of the American Nurses Association) (63).
The nursing practice environment characteristics of Magnet hospitals refer to nurses’participation in hospital affairs, nursing foundations for quality of care (e.g. written, up-to-date nursing care plans for all patients), nurse-manager ability, leadership and support ofnurses, staffing and resource adequacy, and collegial nurse–physician relationships (65).Despite some lack of clarity in study results, along with some counter-intuitive evidence (15),general hospitals possessing the organizational traits of “magnetism” show lower mortalityrates (13), lower rates of 30-day mortality, fewer complications, and reduced “failure torescue” (death following a complication (14)). The Magnet hospital approach also appearsto be able to reduce the likelihood of burn-out and to minimize staff turnover, having apositive impact on the quality of care (66).
The main limits of this programme are its focus on the nursing profession, its concentrationalmost exclusively on the United States (340 accredited hospitals out of 344 were based inthe US; http://www.nursecredentialing.org/MagnetOrg/searchmagnet.cfm) and the sometimesweak evidence of impacts on quality of care. The first Magnet hospital outside the UnitedStates was in England, but it was not supported by the United Kingdom National HealthService and was terminated. Western Europe does not currently have any Magnet hospitals.
Health Promoting Hospitals network
Health promotion is a core dimension of quality in hospital services, along withpatient safety and clinical effectiveness. With the rise in chronic diseases, theprovision of health-promotion services has become an important factor forsustained health, good quality of life and efficiency. The Health PromotingHospitals approach therefore combines specific quality-of-care concerns withaspects of a healthy work environment in hospitals.
The objectives of this network coordinated by the WHO Regional Office forEurope are to:
• change the culture of hospital care towards interdisciplinary working,transparent decision-making and the active involvement of patients, staffand partners;
• evaluate health-promotion activities in the health care setting and buildan evidence base in this area; and
• incorporate standards and indicators for health promotion in existingquality-management systems at hospital level and national level (67).
For quality assurance, a self-assessment manual that formulates five standardsand related indicators is available (68). With regard to the work environment,one of the standards requires that “the management establishes conditionsfor the development of the hospital as a healthy workplace” (see Annex 2).This includes:
• the development and implementation of a healthy and safe workplace;
• the development and implementation of a comprehensive human-resources strategy that includes training and development of the health-promotion skills of the staff; and
• the availability of procedures for developing and maintaining staffawareness about health issues.
For the assessment of the work environment, the manual suggests somecomplementary indicators, including:
• the score from the survey of staff members’ experience of theworking conditions;
• the percentage of short-term absence;
• the percentage of work-related injuries; and
• the score on a burn-out scale.
Policy brief
22
These standards and indicators are meaningful in terms of improving theworking environment and, in conjunction with those for patient outcomes,are elements of a broader health-promoting function of hospitals. Thisframework, developed over more than ten years, can represent an effectivebasis for benchmarking and organizational development of European hospitalsand health services.
These two examples of accreditation schemes designed to improve work-environment issues have their own particular strengths and limits. It maybe worth considering whether the development of a common frameworkfor workplace assessments and certification for organizations in the healthsector would be a helpful option. Such a framework could be based onthe aforementioned quality-of-work elements in combination with quality-of-care standards.
Implementation considerations
It is often the case that issues concerning working conditions lie within themandates of ministries of labour and associated authorities, such as labourinspectorates. Intersectoral collaboration is, therefore, indispensible forimplementing and sustaining effective approaches towards improving thework environment in the health sector. This is not evident everywhere. Creatingattractive and supportive work environments is challenging, not only because ofthe complexity of the issues to be considered, but also because implementationneeds to operate at the interface of health and labour policy mandates withmultiple stakeholders that do not always speak a common language. Usually,labour policies do not take account of the specific needs of particular sectors,such as health, so relevant legislation and regulation need to be adapted to fitthe characteristics of the health sector. At the same time, a lack of awarenessand systematic knowledge of labour issues in the health sector can be observedin many countries. Health policy-makers need to ensure that a systematiccapacity for addressing labour issues is available at all levels of the healthsystem. Moreover, labour-related policy action requires the involvement ofthe core social partners – the employers and workers. One approach, here,concerns the concept of social dialogue.
Social dialogue is a means of achieving sustainable improvements in healthservices, including the work environment, because it aims to involve the keystakeholders. Social dialogue in the health services has been described asinvolving all types of negotiation and consultation, starting with the exchangeof information between and among representatives of governments, employersand workers on issues of common interest relating to economic and socialpolicy (69). Social dialogue requires strong and independent social partners,but this is not available in the health sectors of a number of countries (70).
23
How to create an attractive and supportive working environment for health professionals
While social dialogue has a long tradition in the EU, this has not always been thecase in the health sector, which may reflect the difficulty of organizing this highlyfragmented sector. At the EU level, the establishment of the Social DialogueCommittee for Hospitals was formalized in September 2006. It aims to improvethe quality of employment and the quality of services in the hospital sector andhas proven successful in advancing issues of concern to both employers andworkers. The recognized social partners are HOSPEEM and EPSU.
Evidence confirms that social dialogue is positively associated with improvingworking conditions at the organizational level (21). Yet, against the backgroundof different traditions of industrial relations in Europe, there is considerablevariety in the role of social dialogue in the context of working conditions acrosscountries. Bargaining, for example, takes place principally at the sector level innorth and centre-west European countries (e.g. Sweden, Germany, Austria) andat company level in centre-east countries (e.g. the Czech Republic); it varies insouthern European countries (e.g. Spain, France). The bargaining style has beencharacterized as being conflict-oriented in southern countries, acquiescent incentre-eastern countries and integrating in northern and centre-west countries.While industrial relations are based on social partnership in some countries,others have more state-centred, polarized or fragmented regimes. All thesecharacteristics shape the practice and scope of social dialogue and its impacton working conditions at enterprise level.
A number of case studies in various health facilities in different countries havetestified to the importance of social dialogue processes in management and foremployees. For management, the priority interest is on improving the workingenvironment to achieve high-quality care and enhanced competitiveness – forwhich a qualified and motivated workforce is indispensible. For health workers’representatives, engaging in social dialogue and bargaining serves to counterthe worsening of working conditions from the viewpoint of the individualworker. Lessons learnt from these case studies point to certain factors thatmake social dialogue successful:
• a participatory organizational culture and a cooperative mode of decision-making;
• mutual trust of the stakeholders involved;
• institutionalized dialogue and binding outcomes;
• defined priorities, targets and tasks; and
• the active commitment and competence of employee representatives.
The concrete achievements in terms of improved working conditions covereda broad range of areas, including better occupational health and safety, better
24
Policy brief
working-time schemes, the introduction of conflict-mediation practicesand social-support initiatives, family-friendly work policies and improvedcommunication (21).
Summary
This Policy Brief looked into the question of why a good work environment forhealth professionals matters for policy-makers, and explored options regardinghow to create attractive, supportive, positive work environments. Importantly, ithas also pointed to the importance of the work environment for the recruitmentand retention of health professionals as well as for the quality of care.
There are a multitude of challenges concerning the work environment,and these can be tackled using a variety of policies. This, together with thediversity of the European health systems and socioeconomic situations ofcountries, make it difficult to formulate an off-the-shelf list of actionable policyitems. However, a rough framework can be sketched out, with the following“cornerstones”.
• Whatever issue is identified as a priority concern, it is important toconsider policies that operate at different levels, to ensure a coherentand sustainable approach. Improving the work environment will requiremeasures that are relevant and applicable in the specific context of a givenhealth system while observing international standards and consideringregional harmonization efforts. Effective solutions are context-relatedand therefore priority has to be given to the local/organizational level.
• Policy responses need to be designed with two layers: one layer wouldrelate to the content (what issues need to be addressed), and one wouldrelate to the process (how issues should be tackled).
• Many factors impacting on the work environment of health professionalsare beyond the scope of influence of health policy-makers. Thereforeintersectoral collaboration and social dialogue are core means of developingeffective and sustainable responses.
The aim is to provide a work environment that attracts individuals into thehealth professions, encourages them to remain in the health workforce andenables health workers to perform effectively.
25
How to create an attractive and supportive working environment for health professionals

References
1. WHO Regional Office for Europe. Health workforce policies in the EuropeanRegion. (Report to the Regional Committee, Fifty-seventh session, Belgrade,Serbia, 17–20 September 2007; EUR/RC57/9 + EUR/RC57/Conf.Doc./3;http://www.euro.who.int/__data/assets/pdf_file/0020/74540/RC57_edoc09.pdf,accessed 3 April 2010).
2. Buchan J. How can the migration of health service professionals be managedso as to reduce any negative effects on supply? Copenhagen, WHO RegionalOffice for Europe, 2008.
3. Wiskow C, ed. Health worker migration flows in Europe: overview and casestudies in selected SEE countries – Romania, Czech Republic, Serbia and Croatia.Geneva, International Labour Office, 2006.
4. Organisation for Economic Co-operation and Development. The loomingcrisis in the health workforce- how can OECD countries respond? Paris,Organisation for Economic Co-operation and Development, 2008.
5. WHO Regional Office for Europe. Health workforce policies in the WHOEuropean Region. (Report to the Regional Committee, Fifty-ninth session,Copenhagen, Denmark, 14–17 September 2009; EUR/RC59/9 + EUR/RC59/Conf.Doc./3; http://www.euro.who.int/__data/assets/pdf_file/0008/66977/RC59_edoc09.pdf, accessed 16 July 2010).
6. Wells JS, Norman LJ. The ‘greying’ of Europe – reflections on the stateof nursing and nurse education in Europe. Nurse Education Today, 2009,29(8):811–815.
7. Commission of the European Communities. Green Paper on the EuropeanWorkforce for Health (COM(2008) 725 final). Brussels, Commission of theEuropean Communities, 2008 (http://ec.europa.eu/health/ph_systems/docs/workforce_gp_en.pdf , accessed 16 July 2010).
8. International Labour Office. The sectoral dimension of the ILO’s work –update of sectoral aspects regarding the global economic crisis: tourism,public services, education and health (GB.307/STM/1; ILO Governing Body307th Session, March 2010). Geneva, International Labour Office, 2010(http://www.ilo.org/wcmsp5/groups/public/---ed_norm/---relconf/documents/meetingdocument/wcms_123768.pdf, accessed 10 April 2010).
9. Aiken LH et al. 2002, Hospital nurse staffing and patient mortality, nurseburnout, and job dissatisfaction. JAMA: The Journal of the American MedicalAssociation 2002, 288(16):1987–1993.
26
Policy brief
10. Needleman J et al. Nurse-staffing levels and the quality of care in hospitals.New England Journal of Medicine, 2002, 346(22):1715–1722.
11. Rafferty AM et al. Outcomes of variation in hospital nurse staffing inEnglish hospitals: cross-sectional analysis of survey data and discharge records.International Journal of Nursing Studies, 2007, 44(2):175–182.
12. Dawson J. Does the experience of staff working in the NHS link to thepatient experience of care? An analysis of links between the 2007 acute trustinpatient and NHS staff surveys. Birmingham, Aston School of Business, 2009.
13. Aiken LH, Smith H, Lake ET. Lower Medicare mortality among a set ofhospitals known for good nursing care. Medical Care, 1994, 32(8):771–787.
14. Friese CR et al. Nurse practice environments and outcomes for surgicaloncology patients. Health Services Research, 2008, 43:1145–1163.
15. Tourangeau AE et al. Impact of hospital nursing care on 30-day mortalityfor acute medical patients. Journal of Advanced Nursing, 2007, 57(1):32–44.
16. Unruh L. Licensed nurse staffing and adverse events in hospitals. MedicalCare, 2003, 47(1):142–152.
17. Macmillan Dictionary (http://www.macmillandictionary.com, accessed16 June 2010).
18. Compact Oxford English Dictionary (http://www.askoxford.com, accessed16 June 2010).
19. Commission of the European Communities. Employment and social policies:a framework for investing in quality. Communication from the Commission tothe Council, the European Parliament, the Economic and Social Committee andthe Committee of the Regions (COM(2001) 313 final, 20 June 2001). Brussels,Commission of the European Communities, 2001.
20. Council of the European Union. Guidelines for the employment policiesof the Member States (integrated guidelines 17–24). In: Council Decision onguidelines for the employment policies of the Member States. Legislative Actsand other Instruments (10614/2/08 REV 2). Brussels, Council of the EuropeanUnion, 2008 (http://register.consilium.europa.eu/pdf/en/08/st10/st10614-re02.en08.pdf, accessed 2 July 2010).
21. Voss E. Working conditions and social dialogue – national frameworks,empirical findings and experience of good practice at enterprise level in sixEuropean countries (Draft Report). European Foundation for the Improvementof Living and Working Conditions, 2009 (http://www.eurofound.europa.eu/docs/events/confworkcond09/draftreport.pdf, accessed 8 April 2010).
27
How to create an attractive and supportive working environment for health professionals

22. Muñoz de Bustillo M et al. Indicators of job quality in the European Union.Brussels, European Parliament, 2009 (http://www.europarl.europa.eu/activities/committees/studies.do?language=EN, accessed 17 April 2010).
23. Positive Practice Campaign. Positive practice environments for health careprofessionals [factsheet]. Geneva, International Council of Nurses, InternationalHospital Federation, International Pharmaceutical Federation, WorldConfederation for Physical Therapy, World Dental Federation, World MedicalAssociation, 2008.
24. Commission of the European Communities. Improving quality andproductivity at work: Community strategy 2007–2012 on health and safety atwork. Communication from the Commission to the European Parliament, theCouncil, the European Economic and Social Committee and the Committee ofthe Regions (21.2.2007, COM (2007) 62 final). Brussels, Commission of theEuropean Communities, 2007.
25. WHO. Increasing access to health workers in remote and rural areasthrough improved retention. Background paper for the first expert meeting todevelop evidence-based recommendations to increase access to health workersin remote and rural areas through improved retention; Geneva, 2–4 February2009. Geneva, WHO, 2009 (http://www.who.int/hrh/migration/background_paper.pdf, accessed 20 April 2010).
26. WHO. Working together for health (World Health Report 2006). Geneva,WHO, 2006;
27. Roberfroid D et al. Physician workforce supply in Belgium: current situationand challenges. Health Services Research (HSR). Brussels, Belgian Health CareKnowledge Centre (KCE), 2008.
28. Simoens S, Hurst J. The supply of physician services in OECD countries(OECD Health Working Paper, No. 21). Paris, Organisation for Economic Co-operation and Development, 2006.
29. Hansen N, Sverke M, Naswall K. Predicting nurse burnout from demandsand resources in three acute care hospitals under different forms of ownership:a cross-sectional questionnaire survey. Nursing Studies, 2009, 46(1):96–107.
30. Lombardo E, Sangiuliano M. ‘Gender and employment’ in the Italian policydebates: the construction of ‘non employed’ gendered subjects. Women’sStudies International Forum, 2009, 32(6):445–452.
31. International Labour Organization. ILOLEX Database(http://www.ilo.org/ilolex/, accessed 14 June 2010).
Policy brief
28

32. Peus C. Work–family balance: the case of Germany (WPC #0025).Cambridge (Massachusetts), MIT Workplace Center, Sloane School ofManagement, 2006 (http://web.mit.edu/workplacecenter/docs/wpc0025.pdf,accessed 19 July 2010).
33. Ministry of Social Affairs and Social Security. Act on Maternity/PaternityLeave and Parental Leave, No. 95/2000. Reykjavik, Ministry of Social Affairsand Social Security, 2000 (http://eng.felagsmalaraduneyti.is/legislation/nr/3697,accessed 20 July 2010).
34. Bundesministerium für Familie, Senioren, Frauen und Jugend. Vereinbarkeitvon Beruf und Familie im Krankenhaus. Aus der Praxis für die Praxis. Berlin,Bundesministerium für Familie, Senioren, Frauen und Jugend, 2009.
35. Müller B. Good solutions in nursing and care. Models of good practice ofhealthy and quality-promoting work design of nursing and care jobs in hospitals,inpatient care facilities and home care services. Dortmund, Bundesanstalt fürArbeitsschutz und Arbeitsmedizin, 2005.
36. Commission of the European Communities. Improving quality andproductivity at work: Community strategy 2007–2012 on health and safety atwork. Communication from the Commission to the European Parliament, theCouncil, the European Economic and Social Committee and the Committeeof the Regions (21.2.2007, COM (2007) 62 final). Brussels, Commission of theEuropean Communities, 2007.
37. Gunnarsdottir S, Rafferty AM. Enhancing working conditions. In: DuboisCA, McKee M, Nolte E, eds. Human resources for health in Europe [Chapter 9].Copenhagen, WHO Regional Office for Europe, 2006 (European Observatoryon Health Systems and Policies Series).
38. European Foundation for the Improvement of Working and LivingConditions. Fourth European working conditions survey. Luxembourg,Office for Official Publications of the European Communities, 2007(http://www.eurofound.europa.eu, accessed 22 March 2010).
39. European Agency on Safety and Health at Work (OSHA). Health andsafety of healthcare staff (http://osha.europa.eu/en/sector/healthcare, accessed4 April 2010).
40. Hasselhorn HM, Müller BH, Tackenberg P. Sustaining working ability in thenursing profession – investigation of premature departure from work (NursesEarly Exit Study (NEXT) Scientific Report). Wuppertal, University of Wuppertal,2005 (http://www.next-study.net, accessed 11 July 2010).
29
How to create an attractive and supportive working environment for health professionals

41. International Labour Organization. 2010 World Day for Safety and Healthat Work: emerging risks and new patterns of prevention in a changing world ofwork [booklet]. Geneva, International Labour Office, 2010 (http://www.ilo.org/safework/info/publications/lang--en/docName--WCMS_123653/index.htm,accessed 15 April 2010).
42. Wiskow C. The impact of SARS on health personnel. (Sectoral WorkingPaper, No. 206.) Geneva, International Labour Office, 2003.
43. European Parliament, Committee on Employment and Social Affairs.Report with recommendations to the Commission on protecting Europeanhealthcare workers from blood borne infections due to needlestick injuries(2006/2015(INI)). European Parliament, A6-0137/2006, final, 25.4, 2006.
44. PCN, EUROFEDOP, EDTNA/ERCA, IAPO, EUCOMED, EOM, EMA resolutioncalling for EU action to prevent medical sharps injuries: Protecting Europeanhealthcare workers from medical sharps injury (RTB, April 2004 DiscussionDocument), 2004. (http://www.efnweb.org/version1/en/documents/EuHealthcareWorkers.pdf , accessed 11 April 2010).
45. European Agency for Occupational Safety and Health. OSH in figures:stress at work – facts and figures. Luxembourg, Office for Official Publicationsof the European Communities, 2009 (European Risk Observatory Report, EN 9;http://osha.europa.eu/en/riskobservatory, accessed 8 April 2010).
46. Di Martino V. Relationship between work stress and workplace violencein the health sector. Geneva, ILO/ICN/WHO/PSI Joint Programme on WorkplaceViolence in the Health Sector, 2003 (http://www.ilo.org/public/english/dialogue/sector/sectors/health/publ.htm, accessed 13 April 2010).
47. European Agency for Occupational Safety and Health. Stress – definitionand symptoms. http://osha.europa.eu/en/topics/stress/index_html/definitions_and_causes, accessed 16 July 2010).
48. Goehring C et al. Psychosocial and professional characteristics of burnoutin Swiss primary care practitioners: a cross-sectional survey (http://www.smw.ch/docs/pdf200x/2005/07/smw-10841.pdf, accessed 16 July 2010). Swiss MedicalWeekly, 2005, 135:101–108.
49. Hristov Z et al. Work stress in the context of transition. A case studyof education, health and public administration in Bulgaria. (Report No. 26).Budapest, International Labour Office, Subregional Office for Central andEastern Europe, 2003.
Policy brief
30

50. Di Martino V. Workplace violence in the health sector: Country case studiesBrazil, Bulgaria, Lebanon, Portugal, South Africa, Thailand and an additionalAustralian study–Synthesis report. ILO/ICN/WHO/ICN Joint Programme onWorkplace Violence in the Health Sector, 2002 (http://www.who.int/violence_injury_prevention/injury/work9/en/index2.html, accessed 15 April 2010).
51. International Labour Office. Guidelines on occupational safety and healthmanagement systems, ILO-OSH 2001. Geneva, International Labour Office, 2001.
52. WHO Resolution WHA60.26 on workers’ health: global plan of action.Geneva, Sixtieth World Health Assembly (Agenda Item 12.13, 23 May 2007,A60/VR/11, Paragraph 9; http://apps.who.int/gb/ebwha/pdf_files/WHA60/A60_R26-en.pdf, accessed 11 April 2010).
53. WHO. Work plan of the Global Network of WHO Collaborating Centres forOccupational Health for the period 2009–2012: Compendium. Geneva: WHO,2009 (http://www.who.int/occupational_health/cc_compendium.pdf, accessed19 July 2010).
54. EU Issue Tracker. Sharp objects in health care. EU Issue Tracker – theregulatory radar, 14 December 2009; http://www.euissuetracker.com/en/focus/Pages/Sharp-Objects-in-Health-Care.aspx, accessed 10 April 2010).
55. European Parliament. Motion for a Resolution pursuant to Rule 84(3)of the Rules of Procedure by Liz Lynne, Pervenche Berès on behalf of theCommittee on Employment and Social Affairs on the proposal for a Councildirective implementing the Framework Agreement on prevention from sharpinjuries in the hospital and healthcare sector concluded by HOSPEEM andEPSU (COM(2009)0577). European Parliament 2009–2014, Session DocumentB7-0063/2010, 1.2.2010 (RE\803453EN.doc; PE432.911v01-00). Strasbourg,European Parliament, 2010.
56. De Raeve, P. Sharps injuries – stepping up to the challenge in Europe.Brussels, European Federation of Nurses Associations, 2010(http://www.efnweb.org/version1/en/networks_articles.html, accessed 6 April 2010).
57. WHO. WHO best practices for injections and related procedures toolkit.Geneva, WHO, 2010 (http://whqlibdoc.who.int/publications/2010/9789241599252_eng.pdf, accessed 2 July 2010).
58. HOSPEEM and EPSU. Framework agreement on prevention from sharpinjuries in the hospital and health care sector. Brussels, HOSPEEM and EPSU,2009 (http://www.epsu.org/a/5581, accessed 4 April 2010).
31
How to create an attractive and supportive working environment for health professionals
59. European Agency for Safety and Health at Work. How to tacklepsychosocial issues and reduce work-related stress. Luxembourg, Officefor Official Publications of the European Communities, 2002.
60. ILO/ICN/WHO/PSI. Framework Guidelines on addressing workplace violencein the health sector. ILO/ICN/WHO/PSI Joint Programme on Workplace Violencein the Health Sector. Geneva, International Labour Office, 2002.
61. Kokalov I. Tackling violence at work in the health sector – unions makea difference in Bulgaria (Focus on Health, No. 1, August 2006). Public ServicesInternational, 2006 (http://www.world-psi.org, accessed 19 April 2010).
62. McClure M et al. Magnet hospitals; attraction and retention of professionalnurses. Kansas City, American Academy of Nursing, 1983.
63. Aiken LH et al. Transformative impact of Magnet designation: England casestudy. Journal of Clinical Nursing, 2008, 17(2):3330–3337.
64. Aiken LH, Patrician P. Measuring organizational traits of hospitals:the revised Nursing Work Index. Nursing Research, 2000, 49(3):146–153.
65. Lake ET. Development of the Practice Environment Scale of the NursingWork Index. Research in Nursing and Health, 2002, 25(3):176–188.
66. O´Brien-Pallas L, Tomblin Murphy G, Shamias J. Final Report: Understandingthe Costs and Outcomes of Nurses´Turnover in Canadian Hospitals. Toronto,University of Toronto, Nursing Health Services Research Unit, 2008.(http://www.hhrchair.ch/research.cfm, accessed 16 July 2010)
67. WHO Regional Office for Europe. Health Promoting Hospitals Network (HPH).Copenhagen, WHO Regional Office for Europe (http://www.euro.who.int/en/what-we-do/health-topics/Health-systems/public-health-services/activities/health-promoting-hospitals-network-hph, accessed 4 June 2010).
68. Groene O, ed. 2006, Implementing health promotion in hospitals: manualand self-assessment forms. Copenhagen, WHO Regional Office for Europe,2006:47–50.
69. International Labour Office. Social Dialogue in the health services: a toolfor practical guidance. Geneva, International Labour Office, Sectoral ActivitiesProgramme, 2004.
70. EPSU and HOSPEEM. Strengthening social dialogue in the hospital sectorin the new Member States and candidate countries. EPSU and HOSPEEM, 2007(http://www.hospitalsocialdialogue.eu, last update 9 July 2007).
Policy brief
32
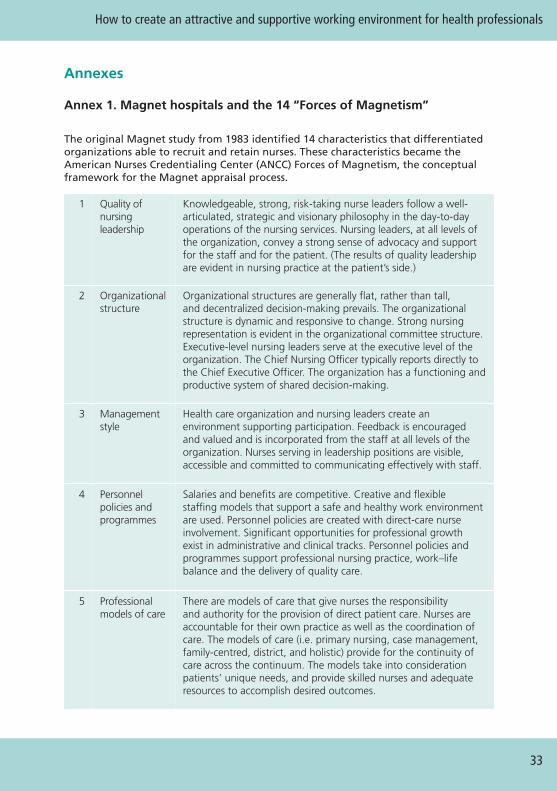
Annexes
Annex 1. Magnet hospitals and the 14 “Forces of Magnetism”
33
How to create an attractive and supportive working environment for health professionals
The original Magnet study from 1983 identified 14 characteristics that differentiatedorganizations able to recruit and retain nurses. These characteristics became theAmerican Nurses Credentialing Center (ANCC) Forces of Magnetism, the conceptualframework for the Magnet appraisal process.
1 Quality ofnursingleadership
Knowledgeable, strong, risk-taking nurse leaders follow a well-articulated, strategic and visionary philosophy in the day-to-dayoperations of the nursing services. Nursing leaders, at all levels ofthe organization, convey a strong sense of advocacy and supportfor the staff and for the patient. (The results of quality leadershipare evident in nursing practice at the patient’s side.)
2 Organizationalstructure
Organizational structures are generally flat, rather than tall,and decentralized decision-making prevails. The organizationalstructure is dynamic and responsive to change. Strong nursingrepresentation is evident in the organizational committee structure.Executive-level nursing leaders serve at the executive level of theorganization. The Chief Nursing Officer typically reports directly tothe Chief Executive Officer. The organization has a functioning andproductive system of shared decision-making.
3 Managementstyle
Health care organization and nursing leaders create anenvironment supporting participation. Feedback is encouragedand valued and is incorporated from the staff at all levels of theorganization. Nurses serving in leadership positions are visible,accessible and committed to communicating effectively with staff.
4 Personnelpolicies andprogrammes
Salaries and benefits are competitive. Creative and flexiblestaffing models that support a safe and healthy work environmentare used. Personnel policies are created with direct-care nurseinvolvement. Significant opportunities for professional growthexist in administrative and clinical tracks. Personnel policies andprogrammes support professional nursing practice, work–lifebalance and the delivery of quality care.
5 Professionalmodels of care
There are models of care that give nurses the responsibilityand authority for the provision of direct patient care. Nurses areaccountable for their own practice as well as the coordination ofcare. The models of care (i.e. primary nursing, case management,family-centred, district, and holistic) provide for the continuity ofcare across the continuum. The models take into considerationpatients’ unique needs, and provide skilled nurses and adequateresources to accomplish desired outcomes.
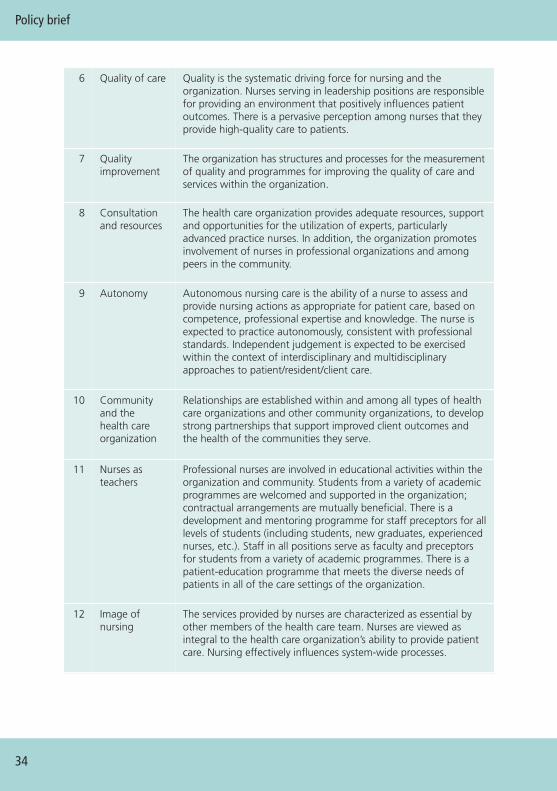
Policy brief
34
6 Quality of care Quality is the systematic driving force for nursing and theorganization. Nurses serving in leadership positions are responsiblefor providing an environment that positively influences patientoutcomes. There is a pervasive perception among nurses that theyprovide high-quality care to patients.
7 Qualityimprovement
The organization has structures and processes for the measurementof quality and programmes for improving the quality of care andservices within the organization.
8 Consultationand resources
The health care organization provides adequate resources, supportand opportunities for the utilization of experts, particularlyadvanced practice nurses. In addition, the organization promotesinvolvement of nurses in professional organizations and amongpeers in the community.
9 Autonomy Autonomous nursing care is the ability of a nurse to assess andprovide nursing actions as appropriate for patient care, based oncompetence, professional expertise and knowledge. The nurse isexpected to practice autonomously, consistent with professionalstandards. Independent judgement is expected to be exercisedwithin the context of interdisciplinary and multidisciplinaryapproaches to patient/resident/client care.
10 Communityand thehealth careorganization
Relationships are established within and among all types of healthcare organizations and other community organizations, to developstrong partnerships that support improved client outcomes andthe health of the communities they serve.
11 Nurses asteachers
Professional nurses are involved in educational activities within theorganization and community. Students from a variety of academicprogrammes are welcomed and supported in the organization;contractual arrangements are mutually beneficial. There is adevelopment and mentoring programme for staff preceptors for alllevels of students (including students, new graduates, experiencednurses, etc.). Staff in all positions serve as faculty and preceptorsfor students from a variety of academic programmes. There is apatient-education programme that meets the diverse needs ofpatients in all of the care settings of the organization.
12 Image ofnursing
The services provided by nurses are characterized as essential byother members of the health care team. Nurses are viewed asintegral to the health care organization’s ability to provide patientcare. Nursing effectively influences system-wide processes.
35
How to create an attractive and supportive working environment for health professionals
13 Interdisciplinaryrelationships
Collaborative working relationships within and among thedisciplines are valued. Mutual respect is based on the premisethat all members of the health care team make essential andmeaningful contributions in the achievement of clinical outcomes.Conflict-management strategies are in place and are usedeffectively, when indicated.
14 Professionaldevelopment
The health care organization values and supports the personaland professional growth and development of staff. In additionto quality orientation and in-service education (addressed earlierin Force 11 –Nurses as teachers), career-development servicesare emphasized. Programmes that promote formal education,professional certification and career development are evident.Competency-based clinical and leadership/management developmentis promoted and adequate human and fiscal resources for allprofessional development programmes are provided.
Source: http://www.nursecredentialing.org/Magnet/ProgramOverview/ForcesofMagnetism.aspx(accessed 8 April 2010).
Annex 2. Health Promoting Hospitals and Health Services network –self-assessment standards
Standard 4: promoting a healthy workplace
The management establishes conditions for the development of the hospitalas a healthy workplace.
Objective
To support the development of a healthy and safe workplace, and to supporthealth-promotion activities by staff.
Sub-standard 4.1The organization ensures the development and implementation of a healthyand safe workplace.
• 4.1.1. Working conditions comply with national/regional directives andindicators (evidence: e.g. national and international (EU) regulationsare recognized).
• 4.1.2. Staff comply with health and safety requirements, and all workplacerisks are identified (evidence: e.g. check data on occupational injuries).
Policy brief
36
Sub-standard 4.2The organization ensures the development and implementation of acomprehensive human-resources strategy that includes training and thedevelopment of the health-promotion skills of staff.
• 4.2.1. New staff receive an induction training that addresses the hospital’shealth-promotion policy (evidence: e.g. interviews with new staff).
• 4.2.2. Staff in all departments are aware of the content of the organization’shealth-promotion policy (evidence: e.g. annual performance evaluationor staff participation in the health-promotion programme).
• 4.2.3. A performance appraisal system and continuing professionaldevelopment including health promotion exists (evidence: e.g. documentedby review of staff files or interview).
• 4.2.4. Working practices (procedures and guidelines) are developed bymultidisciplinary teams (evidence: e.g. check procedures, check with staff).
• 4.2.5. Staff are involved in hospital policy-making, audit and review(evidence: check with staff; check minutes of working groups forparticipation of staff representatives).
Sub-standard 4.3The organization ensures the availability of procedures to develop and maintainstaff awareness about health issues.
• 4.3.1. Policies for awareness about health issues are available for staff(evidence: e.g. check for policies on smoking, alcohol, substance misuseand physical activity).
• 4.3.2. Smoking-cessation programmes are offered (e.g. evidence onavailability of programmes).
• 4.3.3. Annual staff surveys are carried out: these include an assessment ofindividual behaviour, knowledge of supportive services/policies, and use ofsupportive seminars (evidence: check questionnaire used for – and resultsof – staff survey).
Source: Groene O, ed. 2006, Implementing health promotion in hospitals: manual and self-assessment forms. Copenhagen, WHO Regional Office for Europe, 2006:47–50.
Joint policy briefs
1. How can European health systems support investment in and theimplementation of population health strategies?David McDaid, Michael Drummond, Marc Suhrcke
2. How can the impact of health technology assessments be enhanced?Corinna Sorenson, Michael Drummond, Finn Børlum Kristensen, Reinhard Busse
3. Where are the patients in decision-making about their own care?Angela Coulter, Suzanne Parsons, Janet Askham
4. How can the settings used to provide care to older people be balanced?Peter C. Coyte, Nick Goodwin, Audrey Laporte
5. When do vertical (stand-alone) programmes have a place in health systems?Rifat A. Atun, Sara Bennett, Antonio Duran
6. How can chronic disease management programmes operate across care settingsand providers?Debbie Singh
7. How can the migration of health service professionals be managed so as toreduce any negative effects on supply?James Buchan
8. How can optimal skill mix be effectively implemented and why?Ivy Lynn Bourgeault, Ellen Kuhlmann, Elena Neiterman, Sirpa Wrede
9. Do lifelong learning and revalidation ensure that physicians are fit to practise? Sherry Merkur, Philipa Mladovsky, Elias Mossialos, Martin McKee
10. How can health systems respond to population ageing?Bernd Rechel, Yvonne Doyle, Emily Grundy, Martin McKee
11. How can European states design efficient, equitable and sustainable fundingsystems for long-term care for older people?José-Luis Fernández, Julien Forder, Birgit Trukeschitz, Martina Rokosová, David McDaid
12. How can gender equity be addressed through health systems?Sarah Payne
13. How can telehealth help in the provision of integrated care?Karl A. Stroetmann, Lutz Kubitschke, Simon Robinson, Veli Stroetmann, Kevin Cullen, David McDaid
14. How to create conditions for adapting physicians’ skills to new needs andlifelong learningTanya Horsley, Jeremy Grimshaw, Craig Campbell
15. How to create an attractive and supportive working environment for healthprofessionalsChristiane Wiskow, Tit Albreht, Carlo de Pietro
The European Observatory has an independent programme of policy briefs (seehttp://www.euro.who.int/en/home/projects/observatory/ publications/policy-briefs/joint-hen-obs-policy-briefs).
HEN produces synthesis reports and summaries (available athttp://www.euro.who.int/en/what-we-do/data-and-evidence-network-hen).

World Health OrganizationRegional Office for EuropeScherfigsvej 8, DK-2100 Copenhagen Ø, DenmarkTel.: +45 39 17 17 17. Fax: +45 39 17 18 18. E-mail: [email protected] site: www.euro.who.int
This Policy brief was prepared for the Belgian EU Presidency Conferenceon Investing in Europe's health workforce of tomorrow: scope forinnovation and collaboration (La Hulpe, 9–10 September 2010).
This publication is part of the joint policy brief series of the HealthEvidence Network and the European Observatory on Health Systemsand Policies. Aimed primarily at policy-makers who want actionablemessages, the series addresses questions relating to: whether and whysomething is an issue, what is known about the likely consequences ofadopting particular strategies for addressing the issue and how, takingdue account of considerations relating to policy implementation, thesestrategies can be combined into viable policy options.
Building on the Network’s synthesis reports and the Observatory’spolicy briefs, this series is grounded in a rigorous review and appraisalof the available research evidence and an assessment of its relevancefor European contexts. The policy briefs do not aim to provide idealmodels or recommended approaches. But, by synthesizing key researchevidence and interpreting it for its relevance to policy, the series aims todeliver messages on potential policy options.
The Health Evidence Network (HEN) of the WHO Regional Office forEurope is a trustworthy source of evidence for policy-makers in the 53Member States in the WHO European Region. HEN provides timelyanswers to questions on policy issues in public health, health care andhealth systems through evidence-based reports or policy briefs,summaries or notes, and easy access to evidence and information froma number of web sites, databases and documents on its web site(http://www.euro.who.int/en/what-we-do/data-and-evidence/health-evidence-network-hen).
The European Observatory on Health Systems and Policies is apartnership that supports and promotes evidence-based health policy-making through comprehensive and rigorous analysis of healthsystems in the European Region. It brings together a wide range ofpolicy-makers, academics and practitioners to analyse trends in healthreform, drawing on experience from across Europe to illuminate policyissues. The Observatory’s products are available on its web site(http://www.healthobservatory.eu). ISSN 1997-8073