how do clinicians learn to request permission for autopsies?
TRANSCRIPT

231 MEDICAL EDUCATION 1995, 29, 231-234
How do clinicians learn to request permission for autopsies?
S J Shemood', R D Stad, K S Bird?, D W K Cotton' G, D Bunce' 'MRC/ESRC Social and Applied Psychology Unit, Department of Psychology and 'Department of PathologyUniversity of Sheffield, UK
SUMMARY by which clinicians learn to request autopsies and to assess the preferred techniques and timing of appropriate communication skills training. A postal survey of 434 clinicians at four local hospitals
was undertaken in order to identify the methods by which clinicians learn how to request permission for hos- pital autopsies and to assess the preferred techniques and timing of relevant communication skills training. The majority of 128 responding clinicians had learnt through personal experience with some assistance from senior colleagues and peers. Few clinicians appeared to have learnt through formal training. The preferred methods for the provision of communication skills training were training in small groups (such as seminars or tutorials) and observation of clinicians at work. The most desirable time for the provision of this training was considered to be between the beginning of the final undergraduate year and the end of the pre-registration house officer year. The communication skills training provided within medical education is in need of improvement. More emphasis should be given to clinical-task- or situation- specific applications such as requesting permission for autopsies.
METHODS
The study was conducted in four local hospitals in which permission for autopsy is requested by clinicians of all grades. Information obtained from a review of the litera- ture and preliminary semi-structured interviews with clinicians was used to construct a postal questionnaire. The clinicians were asked to indicate the level of their personal exposure to seven methods of learning how to make an autopsy request. The clinicians were then asked to indicate the desirability of various teaching methods for communication skills relevant to requesting autop- sies and the preferred timing of such training. Responses were measured using 7-point Likert scales. A within-sub- jects analysis of variance was used to detect differences between the mean response scores for each item. Post-hoc comparisons of the mean response scores were performed using the Tukey HSD test.
Keywords
clinical medicine/*educ; *education, medical, under- RESULTS graduate; *autopsy; *informed consent; persuasive com- munication; England A total of 134 clinicians (50 consultants, 19 senior regis-
trars, 20 registrars, 26 senior house officers, 10 house
INTRODUCTION
Clinicians have a central role in determining clinical autopsy rates (Peacock et al. 1988). Some clinicians are reluctant to request autopsies because of the personal dis- comfort experienced when approaching bereaved rela- tives for consent (Lundberg 1984; Sherwood 1993). Those clinicians who do seek permission for autopsies often cannot provide adequate reassurance regarding the fears and reservations expressed by relatives.
Many studies have highlighted the problems of obtain- ing permissions for autopsies but these have generally not appreciated the importance of how clinicians learn to request autopsies (Chana et al. 1990; Champ et al. 1992). This study was conducted in order to identify the methods
officers and 9 other clinicians) completed the question- naire after a single reminder. This represented a response rate of 31%. Six incomplete questionnaires were excluded from the study. The number of clinicians marking each item response is indicated in Tables 1-3.
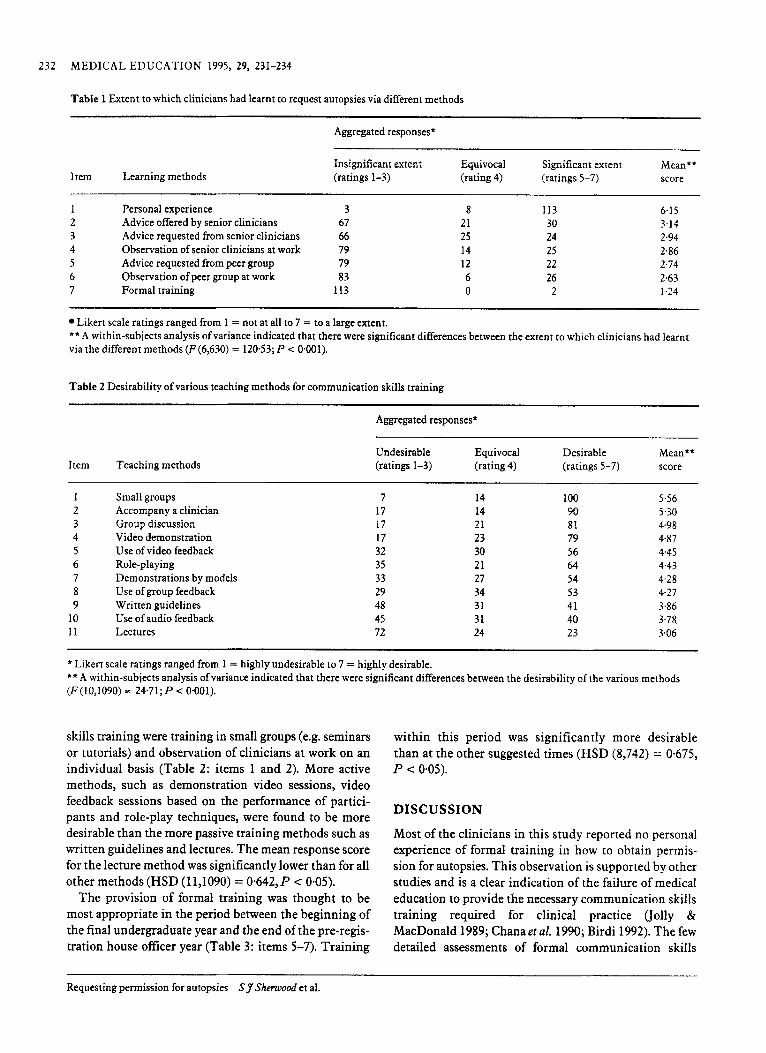
Many respondents reported that they had learnt to request autopsies through personal experience with some assistance from senior colleagues (Table 1 : items 1-3). The mean response score for personal experience was sig- nificantly higher than the scores for all other methods (HSD (7,630) = 0.568, P < 0.05). Few clinicians appeared to have learnt through formal training (Table 1: item 7) and the mean response score for this item was signifi- cantly lower than for all other methods (HSD (11,1090) = 0.642, P < 0.05).
The preferred methods of providing communication
Correspondence: R D Start, Department of Pathology, University of Sheffield Medical School, PO Box 596, Beech Hill Road, Sheffield S10 ZUL, UK
232 MEDICAL EDUCATION 1995, 29, 231-234
Table 1 Extent to which clinicians had learnt to request autopsies via different methods
Aggregated responses*
Item Learning methods Insignificant extent Equivocal Significant extent Mean** (ratings 1-3) (rating 4) (ratings 5-7) score
1 Personal experience 3 2 Advice offered by senior clinicians 67 3 Advice requested from senior clinicians 66 4 Observation of senior clinicians at work 79 5 Advice requested from peer group 79 6 Observation of peer group at work 83 7 Formal training 113
8 113 21 30 25 24 14 25 12 22 6 26 0 2
6.1 5 3.14 2.94 2.86 2.74 2.63 1.24
Likert scale ratings ranged from 1 = not at all to 7 = to a large extent. **A within-subjects analysis of variance indicated that there were significant differences between the extent to which clinicians had learnt via the different methods (F(6,630) = 12053; P < 0.001).
Table 2 Desirability of various teaching methods for communication skills training
Aggregated responses*
Item Teaching methods Undesirable Equivocal Desirable Mean** (ratings 1-3) (rating 4) (ratings 5-7) score
1 2 3 4 5 6 7 8 9
10 11
Small groups Accompany a clinician Group discussion Video demonstration Use of video feedback Role-playing Demonstrations by mo Use of group feedback Written guidelines Use of audio feedback Lectures
'dels
7 17 17 17 32 35 33 29 48 45 72
14 14 21 23 30 21 27 34 31 31 24
100 90 81 79 56 64 54 53 41 40 23
5.56 5.30 4.98 4.87 4.45 4.43 4.28 4.2 7 3.86 3.78 3.06
* Likert scale ratings ranged from 1 = highly undesirable to 7 = highly desirable. **A within-subjects analysis of variance indicated that there were significant differences between the desirability of the various methods (F(lOJ090) = 24.71;P < 0.001).
skills training were training in small groups (e.g. seminars or tutorials) and observation of clinicians at work on an individual basis (Table 2: items 1 and 2). More active methods, such as demonstration video sessions, video feedback sessions based on the performance of partici- pants and role-play techniques, were found to be more desirable than the more passive training methods such as written guidelines and lectures. The mean response score for the lecture method was significantly lower than for all other methods (HSD (11,1090) = 0.642, P < 0-05).
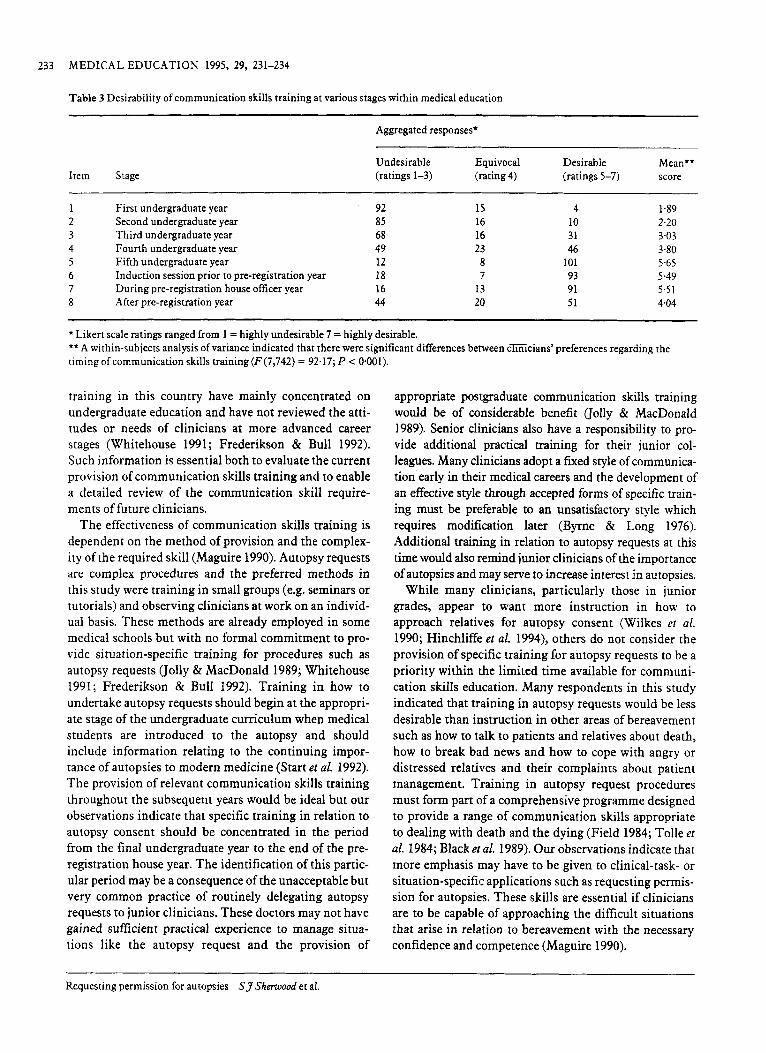
The provision of formal training was thought to be most appropriate in the period between the beginning of the final undergraduate year and the end of the pre-regis- tration house officer year (Table 3: items 5-7). Training
within this period was significantly more desirable than at the other suggested times (HSD (8,742) = 0-675, P < 0-05).
DISCUSSION
Most of the clinicians in this study reported no personal experience of formal training in how to obtain permis- sion for autopsies. This observation is supported by other studies and is a clear indication of the failure of medical education to provide the necessary communication skills training required for clinical practice (jolly & MacDonald 1989; Chana et al. 1990; Birdi 1992). The few detailed assessments of formal communication skills
Requesting permission for autopsies Sy Sherwood et al.
233 MEDICAL EDUCATION 1995, 29, 231-234
Table 3 Desirability of communication skills training at various stages within medical education
Item Stage
~~
Aggregated responses*
Undesirable Equivocal Desirable Mean** (ratings 1-3) (rating 4) (ratings 5-7) score
First undergraduate year Second undergraduate year Third undergraduate year Fourth undergraduate year Fifth undergraduate year Induction session prior to pre-registration year During pre-registration house officer year After pre-registration year
92 85 68 49 12 18 16 44
1s 16 16 23
8 7
13 20
4 10 31 46
101 93 91 51
1.89 2.20 3.03 3.80 5.65 5.49 5.51 4.04
~~
* Likert scale ratings ranged from 1 = highly undesirable 7 = highly desirable. ** A within-subjects analysis of variance indicated that there were significant differences between cEicians’ preferences regarding the timing of communication skills training (F(7,742) = 92.17; P c 0.001).
training in this country have mainly concentrated on undergraduate education and have not reviewed the atti- tudes or needs of clinicians at more advanced career stages (Whitehouse 1991; Frederikson & Bull 1992). Such information is essential both to evaluate the current provision of communication skills training and to enable a detailed review of the communication skill require- ments of future clinicians.
The effectiveness of communication skills training is dependent on the method of provision and the complex- ity of the required skill (Maguire 1990). Autopsy requests are complex procedures and the preferred methods in this study were training in small groups (e.g. seminars or tutorials) and observing clinicians at work on an individ- ual basis. These methods are already employed in some medical schools but with no formal commitment to pro- vide situation-specific training for procedures such as autopsy requests (Jolly & MacDonald 1989; Whitehouse 1991; Frederikson & Bull 1992). Training in how to undertake autopsy requests should begin at the appropri- ate stage of the undergraduate curriculum when medical students are introduced to the autopsy and should include information relating to the continuing impor- tance of autopsies to modern medicine (Start et al. 1992). The provision of relevant communication skills training throughout the subsequent years would be ideal but our observations indicate that specific training in relation to autopsy consent should be concentrated in the period from the final undergraduate year to the end of the pre- registration house year. The identification of this partic- ular period may be a consequence of the unacceptable but very common practice of routinely delegating autopsy requests to junior clinicians. These doctors may not have gained sufficient practical experience to manage situa- tions like the autopsy request and the provision of
appropriate postgraduate communication skills training would be of considerable benefit (Jolly & MacDonald 1989). Senior clinicians also have a responsibility to pro- vide additional practical training for their junior col- leagues. Many clinicians adopt a fixed style of communica- tion early in their medical careers and the development of an effective style through accepted forms of specific train- ing must be preferable to an unsatisfactory style which requires modification later (Byrne & Long 1976). Additional training in relation to autopsy requests at this time would also remind junior clinicians of the importance of autopsies and may serve to increase interest in autopsies.
While many clinicians, particularly those in junior grades, appear to want more instruction in how to approach relatives for autopsy consent (Wilkes et al. 1990; Hinchliffe et al. 1994), others do not consider the provision of specific training for autopsy requests to be a priority within the limited time available for communi- cation skills education. Many respondents in this study indicated that training in autopsy requests would be less desirable than instruction in other areas of bereavement such as how to talk to patients and relatives about death, how to break bad news and how to cope with angry or distressed relatives and their complaints about patient management. Training in autopsy request procedures must form part of a comprehensive programme designed to provide a range of communication skills appropriate to dealing with death and the dying (Field 1984; Tolle et al. 1984; Black et al. 1989). Our observations indicate that more emphasis may have to be given to clinical-task- or situation-specific applications such as requesting permis- sion for autopsies. These skills are essential if clinicians are to be capable of approaching the difficult situations that arise in relation to bereavement with the necessary confidence and competence (Maguire 1990).
Requesting permission for autopsies SJSherwood et al.

234 MEDICAL EDUCATION 1995, 29, 231-234
Some communication skills, such as the breaking of bad news, are transferable between different areas of clin- ical practice (Buckman 1984). Autopsy requests repre- sent a clinical-taskhituation-specific application for communication skills training that is probably not directly transferable to other areas and which therefore requires specific attention. The focused nature of clinical- taskhituation-specific communication skills training may serve to facilitate the application of acquired know- ledge and skills to the relevant real-life situations (Jolly & MacDonald 1989). Provision of training in how to request permission for autopsies has been shown to con- tribute to the improvement of autopsy rates (Clayton & Sivak 1992). Clinicians with little or no interest in autop- sies may still have to inform relatives of the requirement for a medico-legal autopsy and all clinicians must there- fore be equally capable of providing adequate reassurance regarding the autopsy to bereaved relatives.
The process of requesting an autopsy from recently bereaved relatives is stressful and any sense of personal discomfort will decrease the motivation of clinicians to request autopsies (Birdi 1992; Sherwood 1993). Those clinicians who have received appropriate training may have more confidence and consequently may be more willing to take the time to educate relatives in the nature and the importance of the autopsy. The manner in which permission for autopsy is sought is important and can influence the decision of the family in approximately one- third of cases (Gardner et al. 1973). Any significant improvement in autopsy requesting techniques should stimulate more autopsy requests of a higher standard. Increasing the number of autopsy requests is probably the only basis upon which autopsy rates will be improved.
REFERENCES
Birdi K S (1992) A comparison of the theory ofphnned behaviour and the theory of reasoned action in the context of requesting hospital auropsies. MSc Thesis, University of Sheffield.
Black D, Hardoff D & Nelki J (1989) Educating medical students about death and dying. Archives of Dkeases in Childhood 64, 750-3.
Byrne P S & Long B E L (1976) Docwrs Talking to Patients. HMSO,
Buckman R (1984) Breaking bad news: why is it still so difficult? London.
Rrirish MedicalJournal288,1597-9.
Chana J, Rhys-Maitland R, Hon P, Scott P, Thomas C & Hopkins A (1990) Who asks permission for an autopsy?Journal ofthe Royal College of Physicians of London 24,185-8.
Champ C, Tyler X, Andrews P S & Coghill S B (1992) Improve your hospital autopsy rate to 40-50 per cent: a tale of two towns. Journal of Pathology 166,405-7.
Clayton S A & Sivak S L (1992) Improving the autopsy rate at a university hospital. Amm‘canJournal of Medicine 92,423-8.
Field D (1984) Formal instruction in United Kingdom medical schools about death and dying. Medical Education 18,429-34.
Frederikson L &Bull P (1992) An appraisal of the current status of communication skills training in British medical schools. Social Science and Medicine 34,515-22.
Gardner R, Peskin L & Katz J L (1973) The physician, the autopsy request and the consent rate.Journa1 of Medical Education 48, 636-44.
Hinchliffe S A, Godfrey H W & Hind C R K (1994) Attitudes of junior medical staff to requesting permission for autopsy. Postgraduate MedicalJoumll70,292-4.
Jolly B S & MacDonald M M (1989) Education for practice: the role of practical experience in undergraduate and general clinical training. Medical Education 23,189-95.
Lundberg G D (1984) Medicine without the autopsy. Archives of Pathology and Laboratory Medicine 108,449-54.
Maguire P (1990) Can communication skills be taught?Brirish JournalofHospital Medicine 43,215-16.
Peacock S J, Machin D, DuBoulay C E H & Kirkham N (1988) The autopsy: a useful tool or an old relic?Journal of Parhologv 156, 9-14.
Shenvood S J (1993) Motivation to request permission for hospital autopsies: the predictive .utility of clinicians’snength of self-eficacy, outcome expectations, and outcome values. MSc Thesis, University of Shefield.
Start R D, Hector-Taylor M J, Cotton D W K, Startup M, Parsons M A & Kennedy A (1992) Factors which influence necropsy requests: a psychological approach.Journa1 of Clinical Pathology 45,254-7.
Tolle S W, Elliot D L & Hickam D H (1984) Physician attitudes and practices at the time of patient death. Archives of Internal Medicine 144,2389-91.
Whitehouse C R (1991) The teaching of communication skills in United Kingdom medical schools. Medical Education 25, 311-18.
Wilkes M S, Link R N, Jacobs T A, Fortin A.H & Felix J C (1990) Attitudes of house officers towards the autopsy.Journal of General Internal Medicine 5,122-5.
Received 13 May 1994; editorial comments to authors 26 Augusr 1994; accepted for publication 27January 1995
Requesting permission for autopsies SJSherwood et al.