hodgkins lymphoma
TRANSCRIPT

Management of Hogdkin’s Lymphoma
By Dr Parneet Singh
Moderator-Dr Amal Roy Chaudhoory

Treatment RecommendationsStage Recommended
TreatmentFavorableIA/IIA (no bulky disease,<3 sites,ESR<50)
ABVD ×4 then IFRT [20 Gy−30 Gy)
Alternative chemo = 8 week Stanford V + IFRT(30-36 Gy)
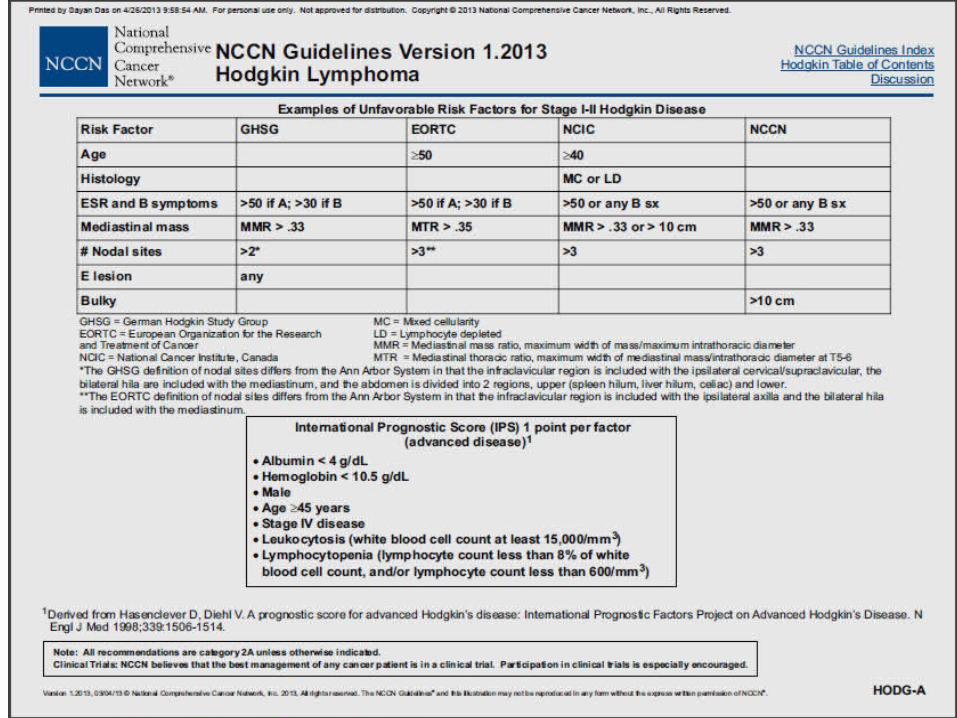
Unfavorable IA/IIA (bulky disease, >3 sites, or ESR>50), IB/IIB
ABVD ×4–6 then IFRT (30–36 Gy)
Alternative: 12 weeks Stanford V + IFRT 36 Gy
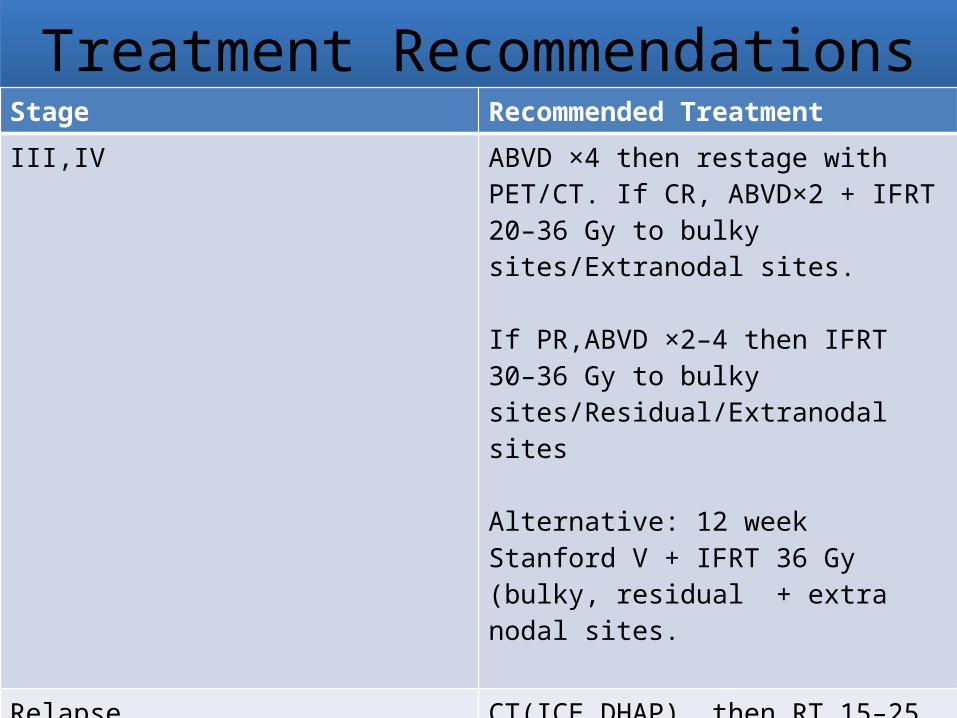
Treatment RecommendationsStage Recommended TreatmentIII,IV ABVD ×4 then restage with
PET/CT. If CR, ABVD×2 + IFRT 20–36 Gy to bulky sites/Extranodal sites.
If PR,ABVD ×2–4 then IFRT 30–36 Gy to bulky sites/Residual/Extranodal sites
Alternative: 12 week Stanford V + IFRT 36 Gy (bulky, residual + extra nodal sites.
Relapse CT(ICE,DHAP), then RT 15–25 Gy to previously irradiated sites or30–40 Gy to not previously irradiated sitesIf relapse after initial stage III/IV, then autologous bone marrow transplant
Bulky Disease
• No agreed definition
• 10 cm or more in size
• In some centres taken cut off taken as 8 cm
• >1/3 involvement of thoracic diaphragm at any level
Treatment Modalities
• Chemotherapy
• Radiotherapy
• Combined Modality Treatment
• Autologous Stem Cell Transplant
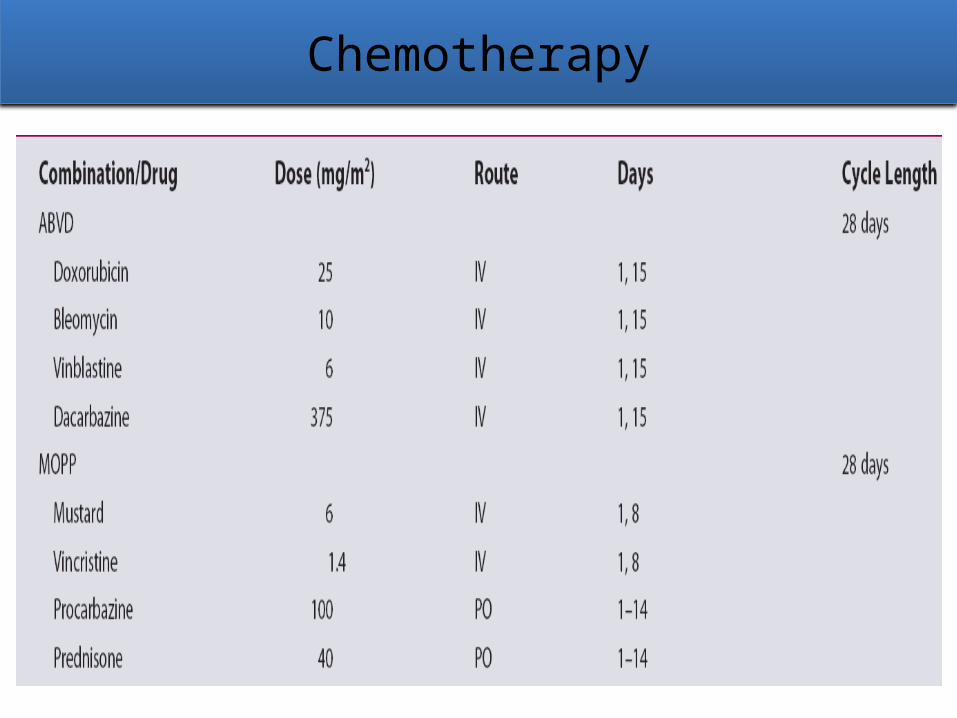
Chemotherapy
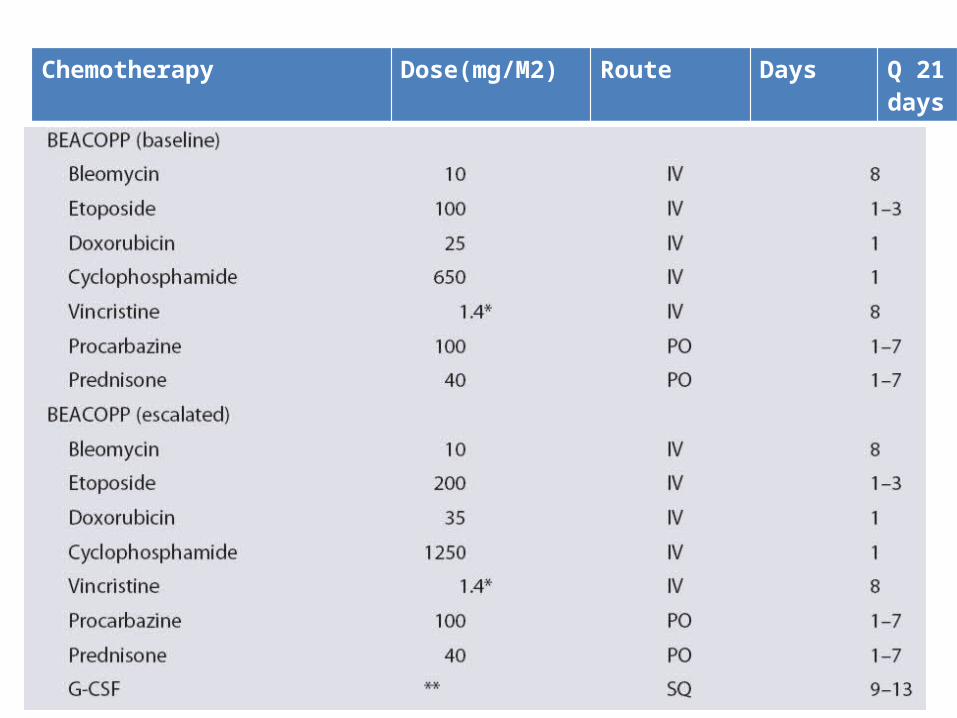
Chemotherapy Dose(mg/M2) Route Days Q 21 days
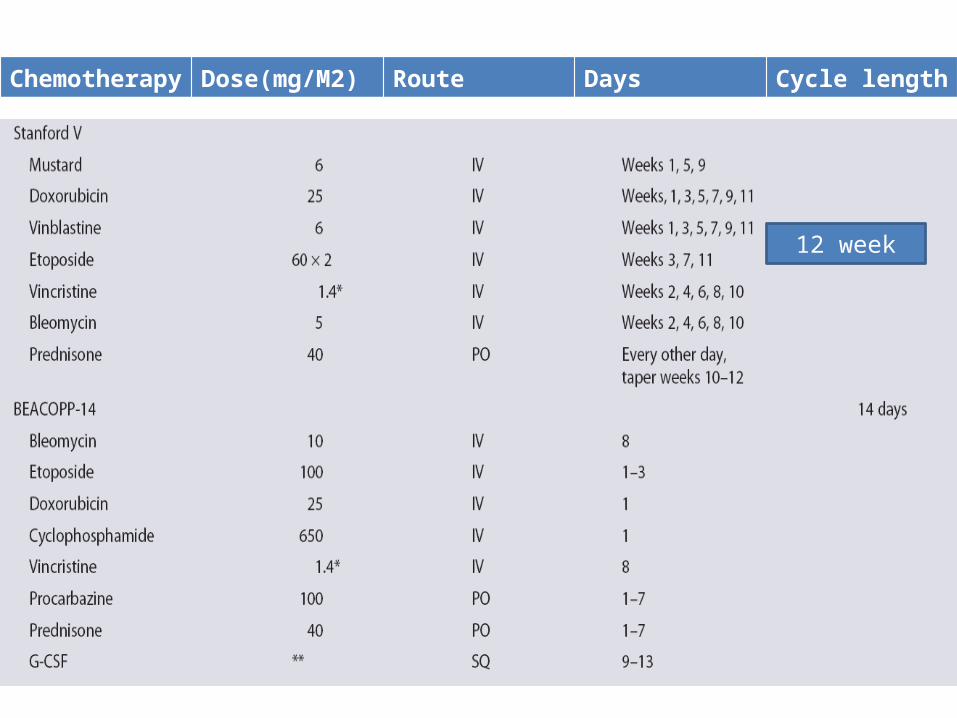
Chemotherapy Dose(mg/M2) Route Days Cycle length
12 week
Complications of Chemotherapy• Nausea and Vomiting more with MOPP
• Sterility was a major adverse effect of the MOPP regimen.
• ABVD causes temporary cessation of menstrual cycle in women and temporary oligospermia in men.
• BEACOPP chemotherapy sterilizes males and many young females.
• Semen preservation must take place before chemotherapy.
• BEACOPP chemotherapy has an increased risk of secondary AML due to etoposide
• ABVD chemotherapy does not increase the risk ofsecondary AML above baseline.
• Pulmonary toxicity related to bleomycin .
• Bone toxicity in the form of osteoporosis due to prednisone
• Skin necrosis if nitrogen mustard extravasated
• Main dose limiting toxicity is myelopsuppresssionHough et al Lippincott
&wilkins 2007
ABVD vs MOPP
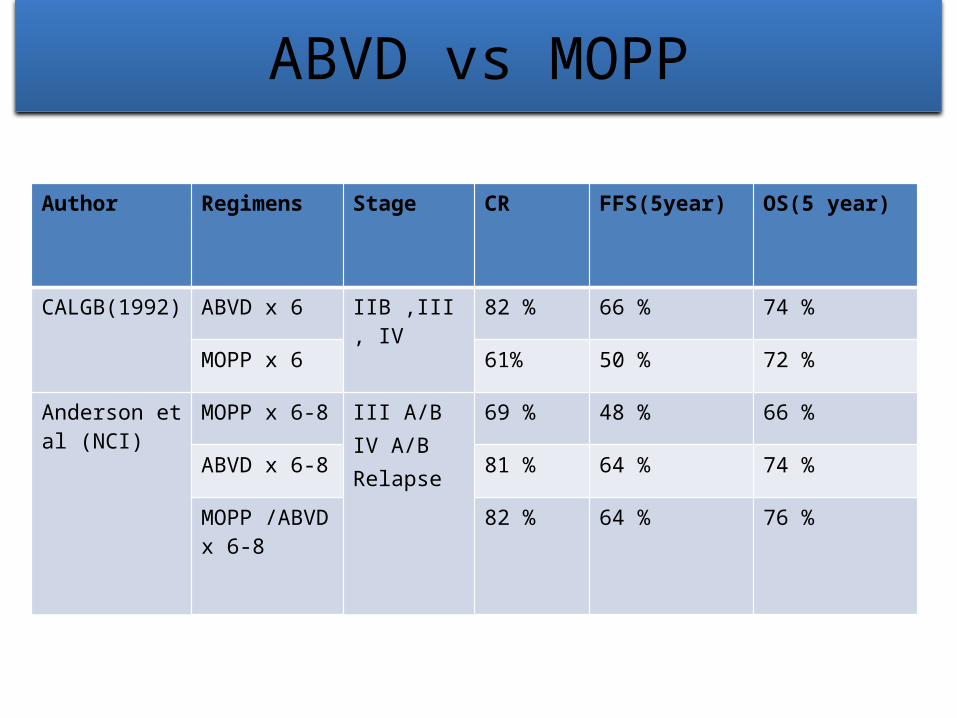
Author Regimens Stage CR FFS(5year) OS(5 year)
CALGB(1992)
ABVD x 6 IIB ,III, IV 82 % 66 % 74 %
MOPP x 6 61% 50 % 72 %
Anderson et al (NCI)
MOPP x 6-8 III A/BIV A/BRelapse
69 % 48 % 66 %
ABVD x 6-8 81 % 64 % 74 %
MOPP /ABVD x 6-8
82 % 64 % 76 %
ABVD vs MOPP vs ABVD/MOPP
• Hodgkin's disease in Stages IIIA, IIIB, and IVA or IVB
• (1) MOPP alone given for 6 to 8 cycles, (2) MOPP alternating with ABVD for 6 cycles, and (3) ABVD alone for 6 to 8 cycles
• The overall response rate was 93 %, with complete responses in 77%: 67% for MOPP group, 82% in the ABVD group, and 83% in the MOPP—ABVD group (P = 0.006 MOPP vs 2 regimes)
Canellos et al NEJM 1992
• FFS at five years were 50% for MOPP, 61% for ABVD and 65% for MOPP—ABVD
• OS at 5 years was 66% for MOPP, 73% for ABVD and 75% for MOPP—ABVD (P = 0.28 MOPP vs 2 regimes)
• MOPP had more severe toxic effects on bone marrow than ABVD and was associated with greater reductions in the prescribed dose.
Canellos et al NEJM 1992
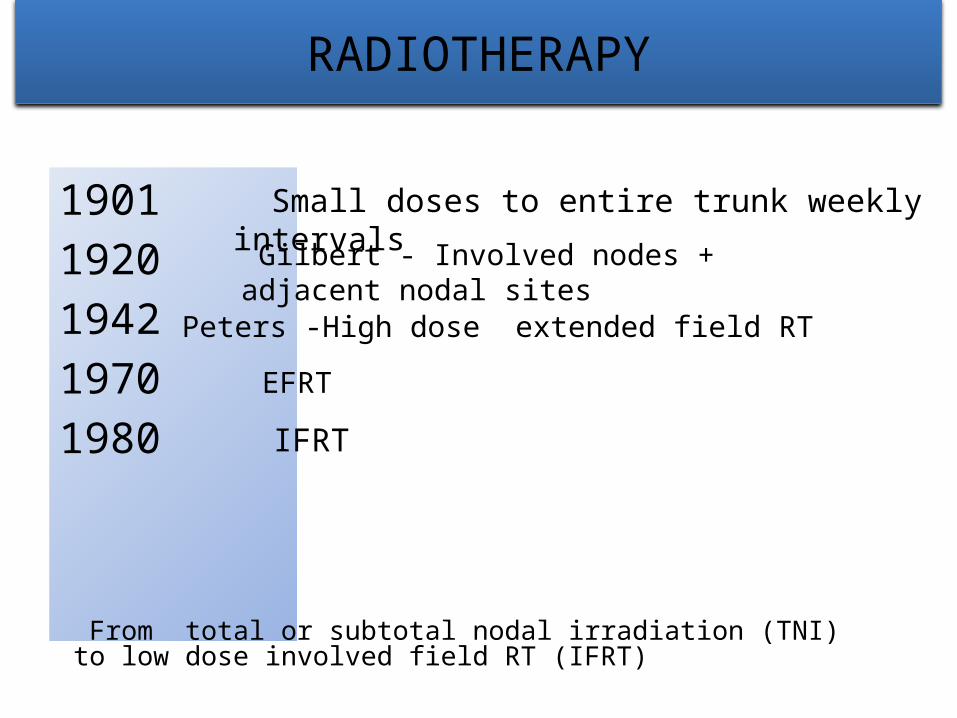
RADIOTHERAPY
190119201942 19701980
Small doses to entire trunk weekly intervals Gilbert - Involved nodes + adjacent nodal sites
Peters -High dose extended field RT
From total or subtotal nodal irradiation (TNI) to low dose involved field RT (IFRT)
EFRT IFRT
Radiotherapy Indications
• In early stage I and II favourable and unfavourable following CT
• In III and IV in case of bulky disease ,residual disease or extra nodal sites
• In cases of relapse
• Role in Hematopoietic Stem cell transplant
• Earlier extended field RT was done as sites adjacent to sites clinically involved are at high risk for further involvement if left untreated
• Now IFRT is used which includes complete involved lymphoid region , when any portion of that region is involved
• If extra nodal and no lymph nodes then only whole organ is treated
• Involved Node RT-Involves treatment of only involved LN before CT
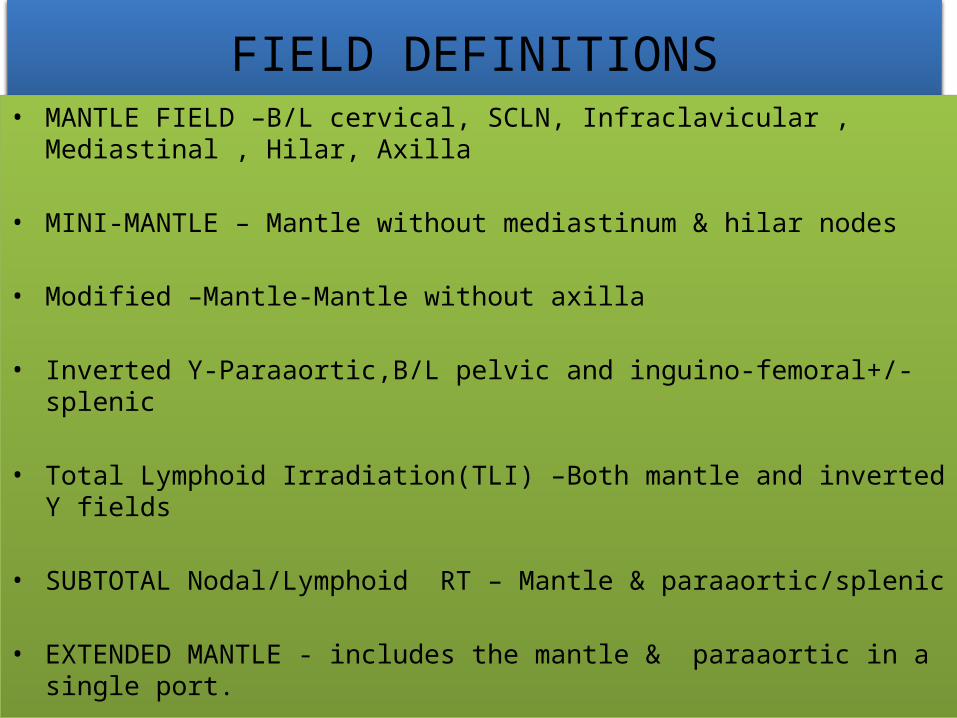
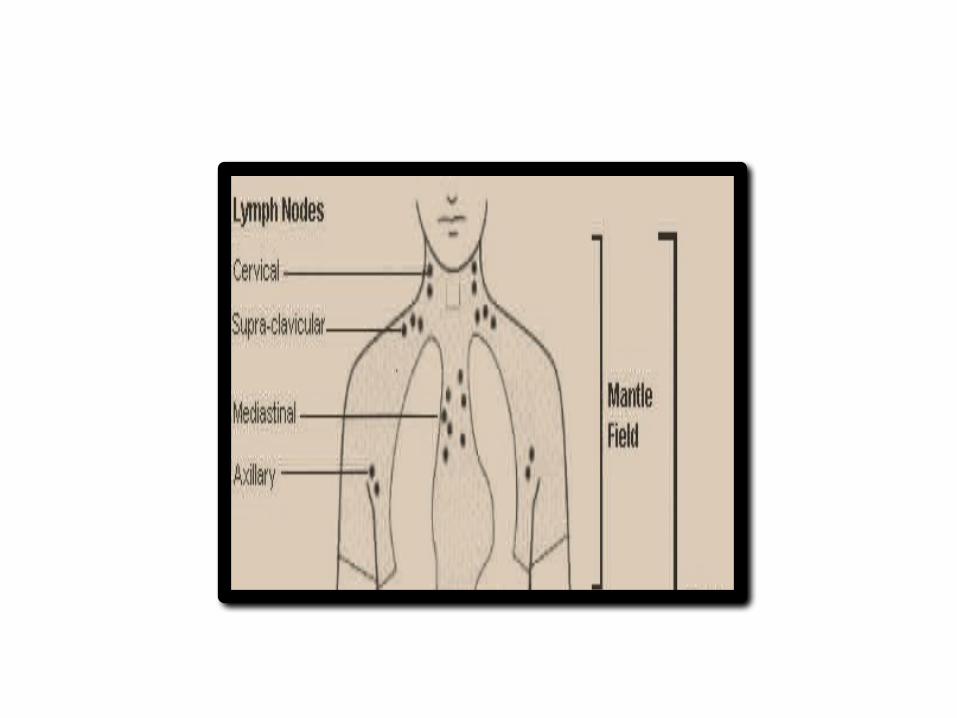
FIELD DEFINITIONS• MANTLE FIELD –B/L cervical, SCLN, Infraclavicular , Mediastinal ,
Hilar, Axilla
• MINI-MANTLE – Mantle without mediastinum & hilar nodes
• Modified –Mantle-Mantle without axilla
• Inverted Y-Paraaortic,B/L pelvic and inguino-femoral+/- splenic
• Total Lymphoid Irradiation(TLI) –Both mantle and inverted Y fields
• SUBTOTAL Nodal/Lymphoid RT – Mantle & paraaortic/splenic
• EXTENDED MANTLE - includes the mantle & paraaortic in a single port.
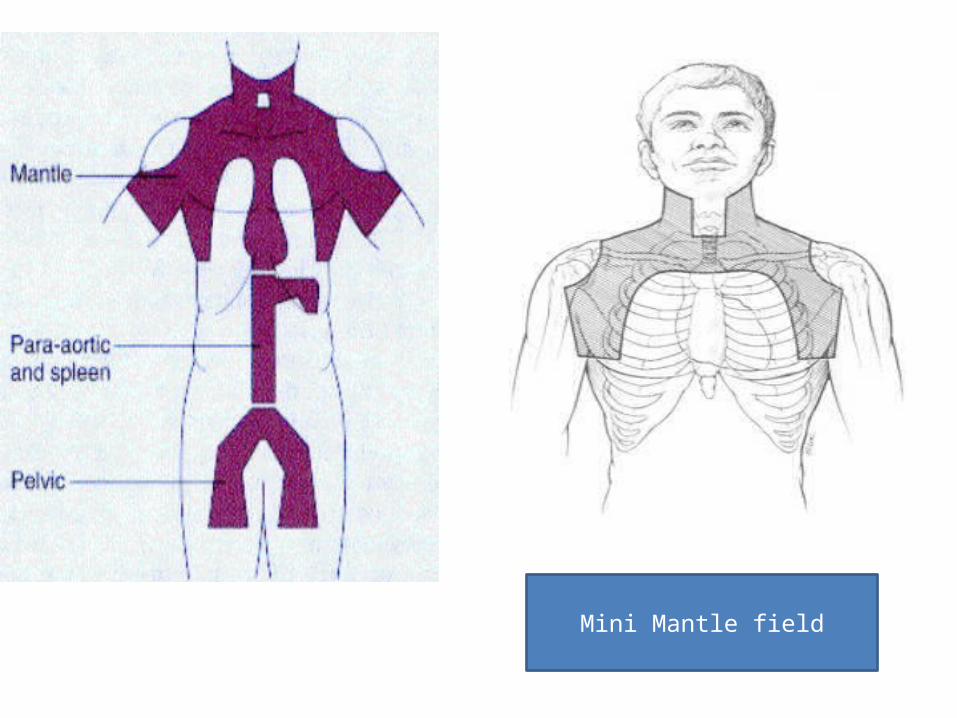
Mini Mantle field
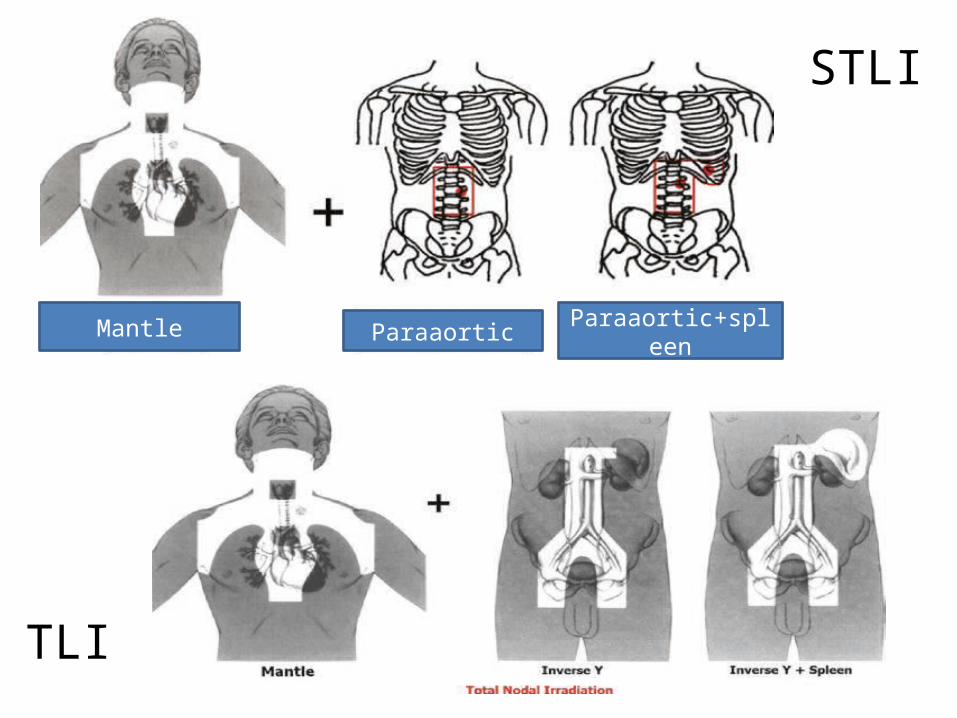
STLI
TLI
Mantle Paraaortic Paraaortic+spleen
MANTLE FIELD• Treatment in contiguity of lymph nodal groups in the cervical,
supraclavicular, infraclavicular, axillary, mediastinal, and hilar regions
• Mantle fields are large fields
• Usually supine.
• Head in hyperextension
• Arms up position pull up the axillary node further from the chest wall so allow better lung shielding.
• Arms down or akimbo position allow better shielding of the humeral head and minimize the effect of tissue folds in supraclavicular region
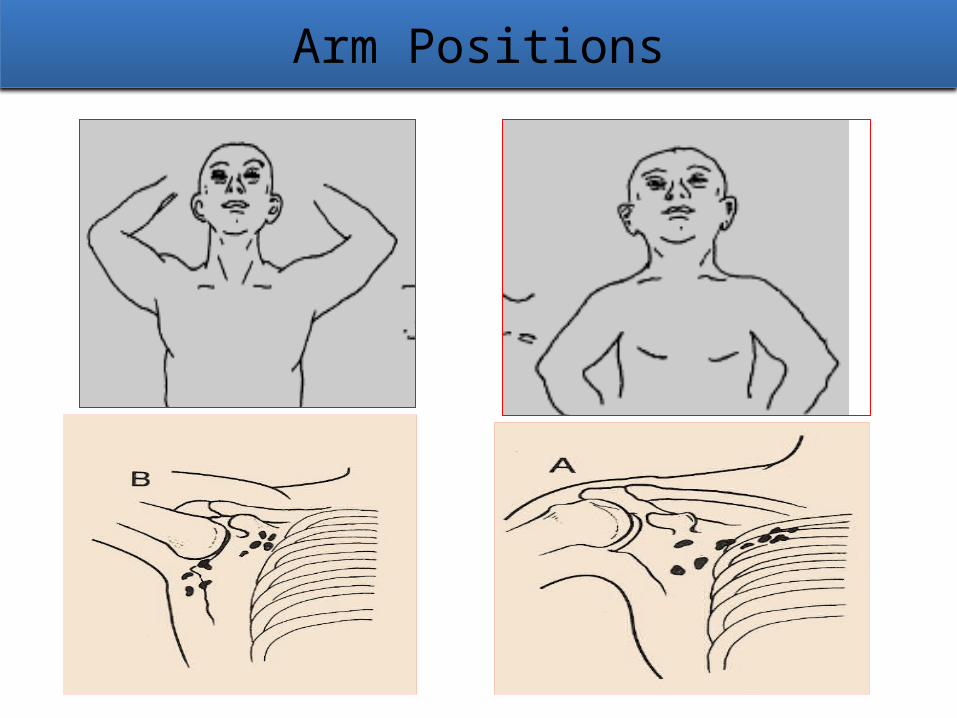
Arm Positions
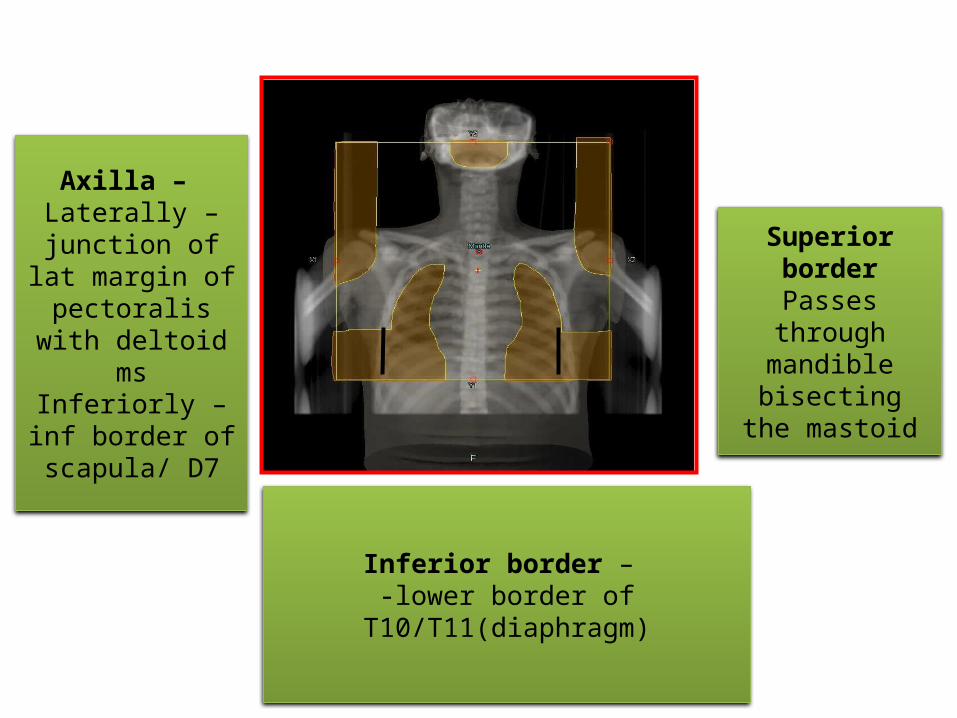
Superior border
Passes through mandible
bisecting the mastoid
Inferior border – -lower border of
T10/T11(diaphragm)
Axilla – Laterally –
junction of lat margin of
pectoralis with deltoid ms
Inferiorly –inf border of
scapula/ D7

Lung block• Superiorly - 1.5 to 2cm below
the clavicle in order to treat the infraclavicular nodes
• Laterally - blocks shield lung & atleast 1cm lung included in lower axilla & 2-4cm of lung in upper axilla in order to treat the axillary lymph nodes
• Medially – 1.5-2cm margin around lateral border of tumor
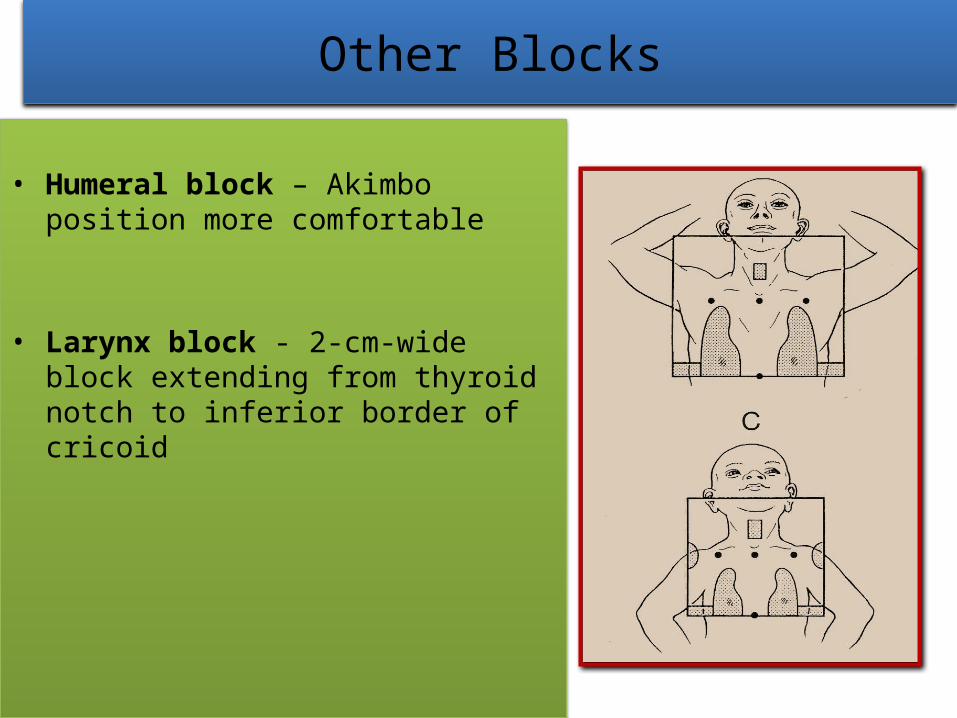
Other Blocks
• Humeral block – Akimbo position more comfortable
• Larynx block - 2-cm-wide block extending from thyroid notch to inferior border of cricoid
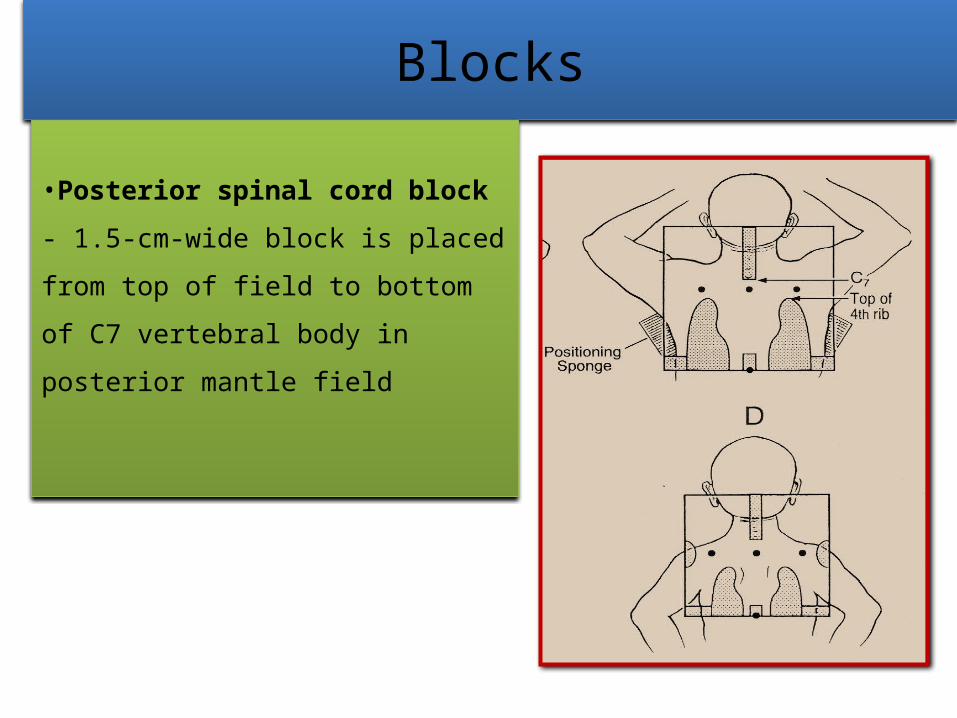
Blocks
•Posterior spinal cord block - 1.5-cm-wide block is placed from top of field to bottom of C7 vertebral body in posterior mantle field

Paraaortic/ spleen fields• Paraaortic field covers the paraaortic, celiac, splenic, & hepatic
portal lymph nodes as well as splenic pedicle or spleen
• T/t delivered with equally weighted daily anterior and posterior 6-MV photon beams
• Upper border – matched with mantle
• Inferior border - at the L4-L5 interspace
• Lateral border – edges of transverse processes or about 1.5-2cm lat to border of vertebral bodies (width of 8-10cm)
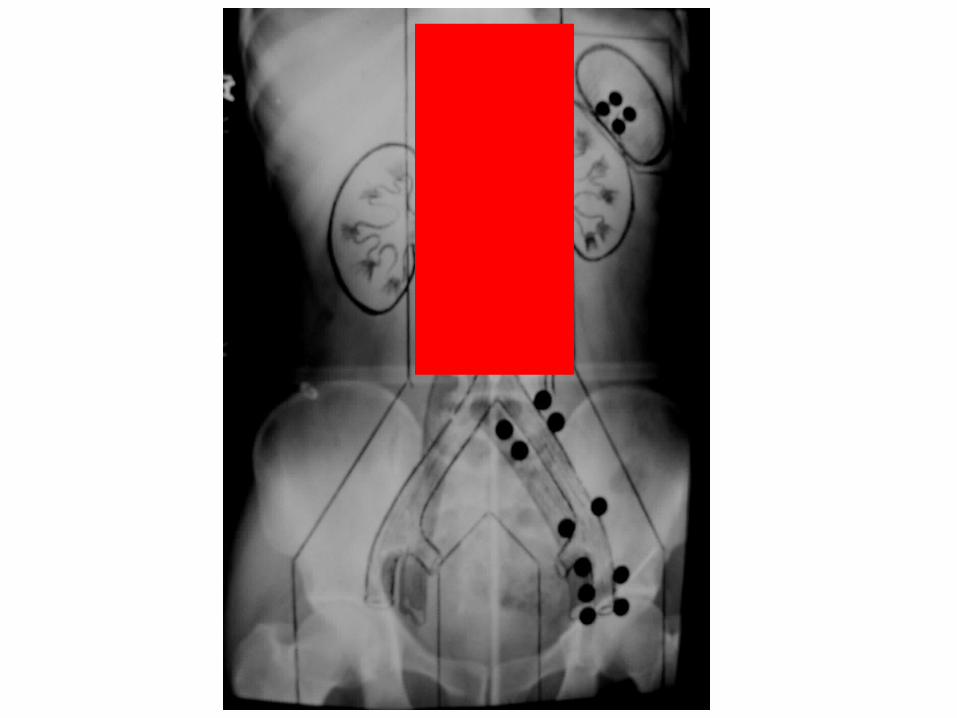
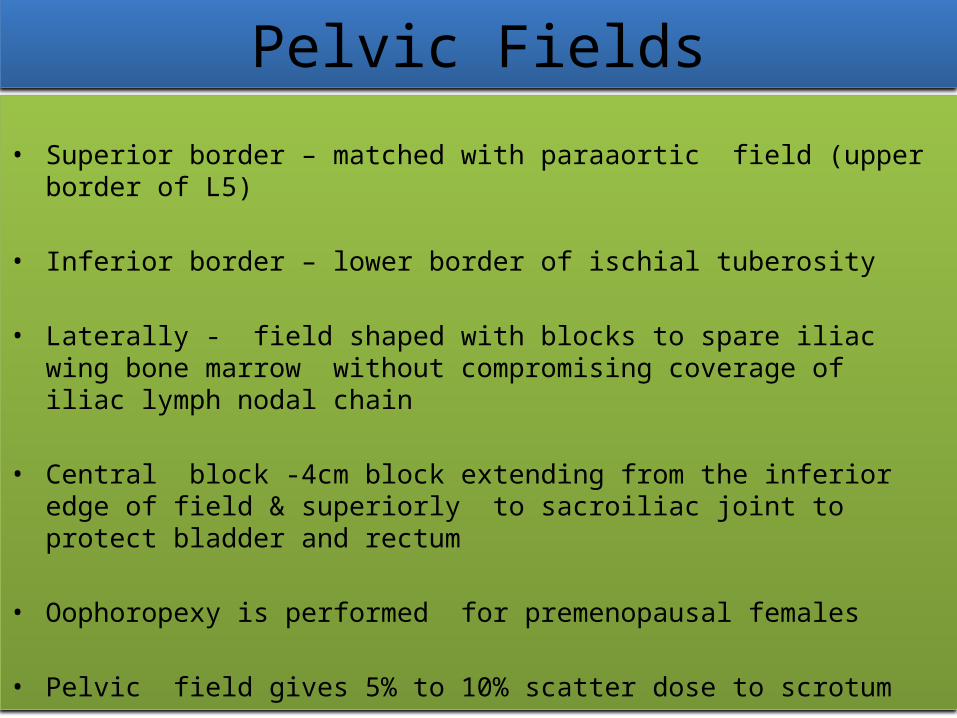
Pelvic Fields• Superior border – matched with paraaortic field (upper border of
L5)
• Inferior border – lower border of ischial tuberosity
• Laterally - field shaped with blocks to spare iliac wing bone marrow without compromising coverage of iliac lymph nodal chain
• Central block -4cm block extending from the inferior edge of field & superiorly to sacroiliac joint to protect bladder and rectum
• Oophoropexy is performed for premenopausal females
• Pelvic field gives 5% to 10% scatter dose to scrotum
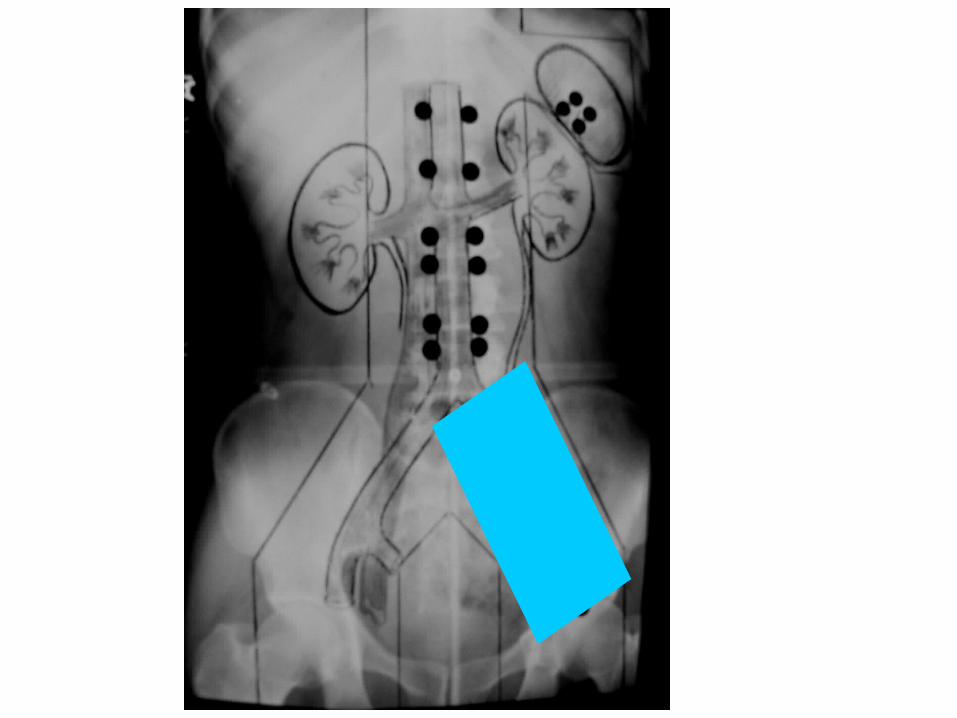
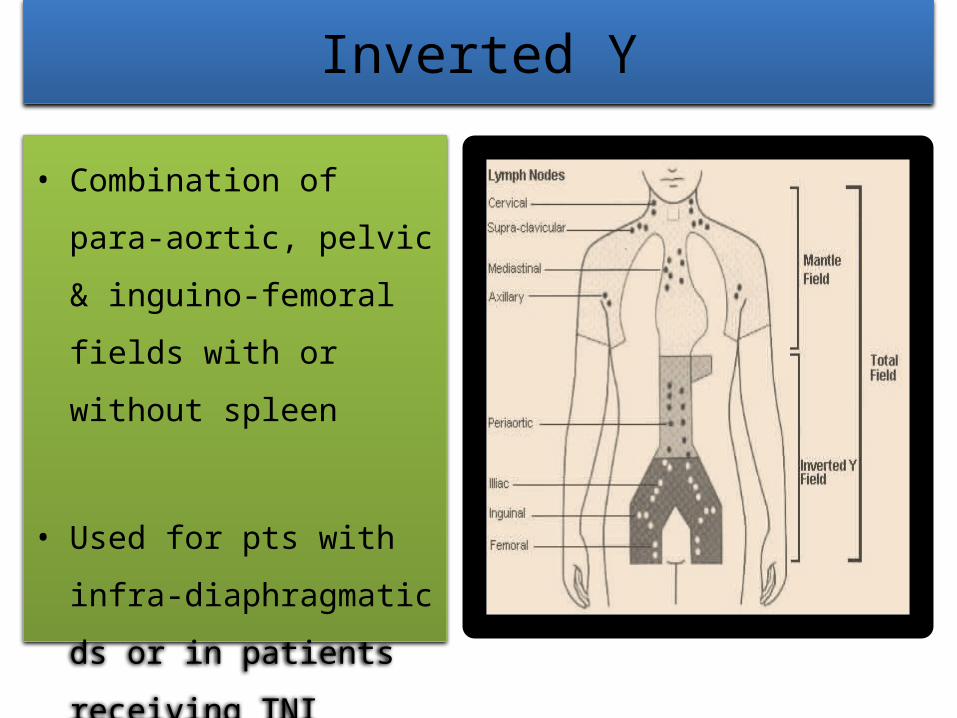
Inverted Y
• Combination of para-aortic, pelvic & inguino-femoral fields with or without spleen
• Used for pts with infra-diaphragmatic ds or in patients receiving TNI
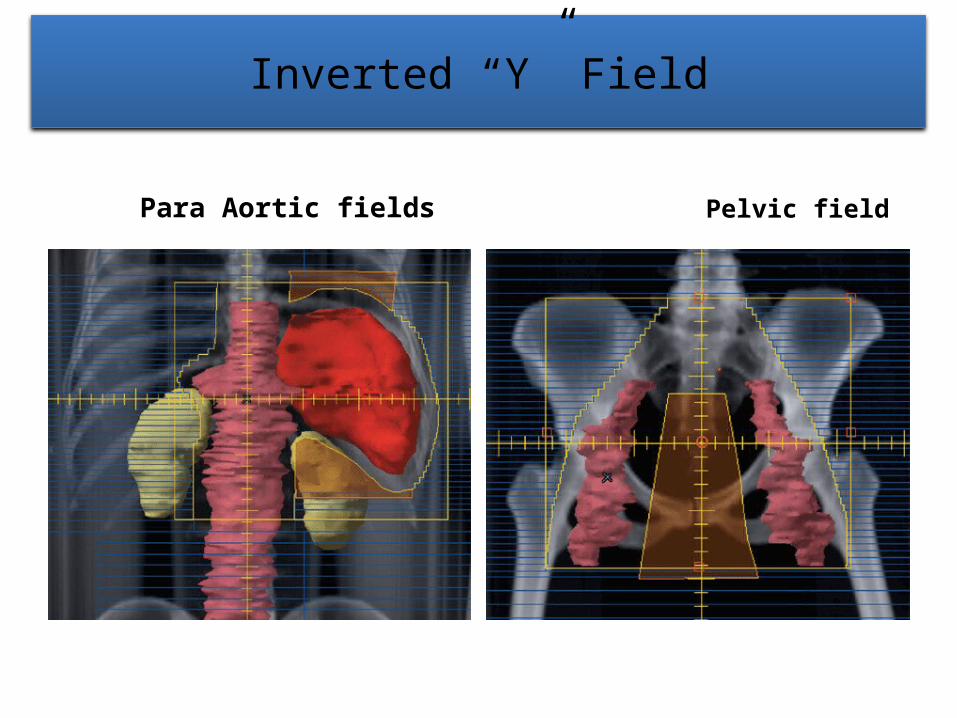
Inverted “Y” Field
Para Aortic fields Pelvic field

Testicular shielding
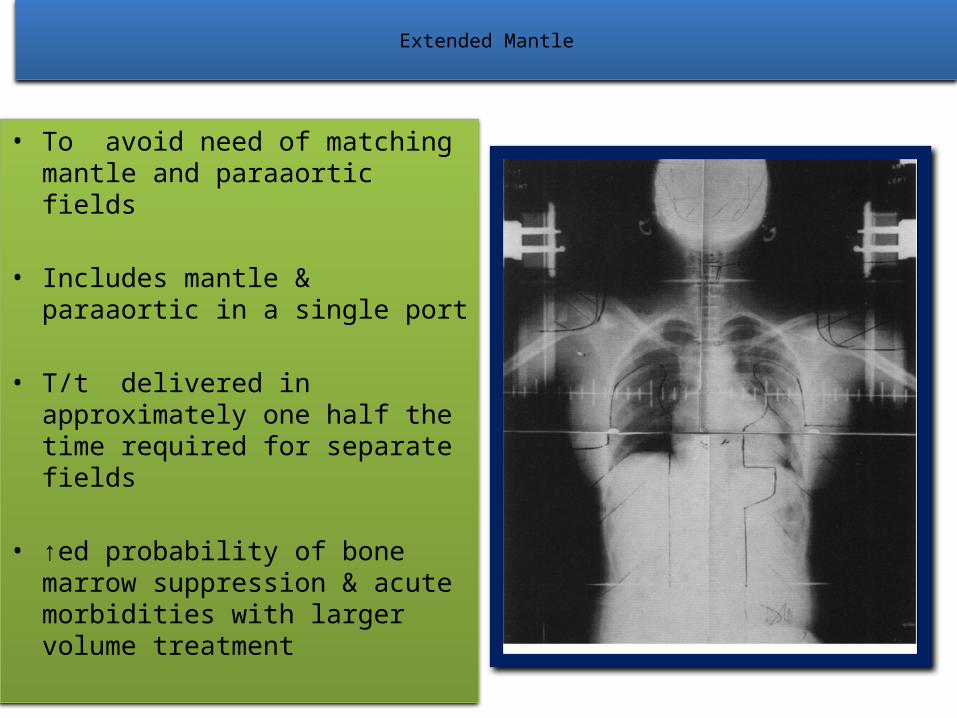
Extended Mantle
• To avoid need of matching mantle and paraaortic fields
• Includes mantle & paraaortic in a single port
• T/t delivered in approximately one half the time required for separate fields
• ↑ed probability of bone marrow suppression & acute morbidities with larger volume treatment
INVOLVED FIELD • Treatment to the complete involved lymphoid region , when any portion of
that region is involved
• If extra nodal involvement then whole organ only if lymph nodes not involved
• Include initially involved pre CT sites & volume , except transverse diameter of mediastinal & paraaortic lymph nodes for which post CCT volume
• Supraclavicular region treated when sup mediastinum involved
• Iliac lymph nodes treated when inguino-femoral nodes involved
• Involved Node RT-Involves treatment of only involved LN before CT

Fields in IFRT
Site LN regions involved
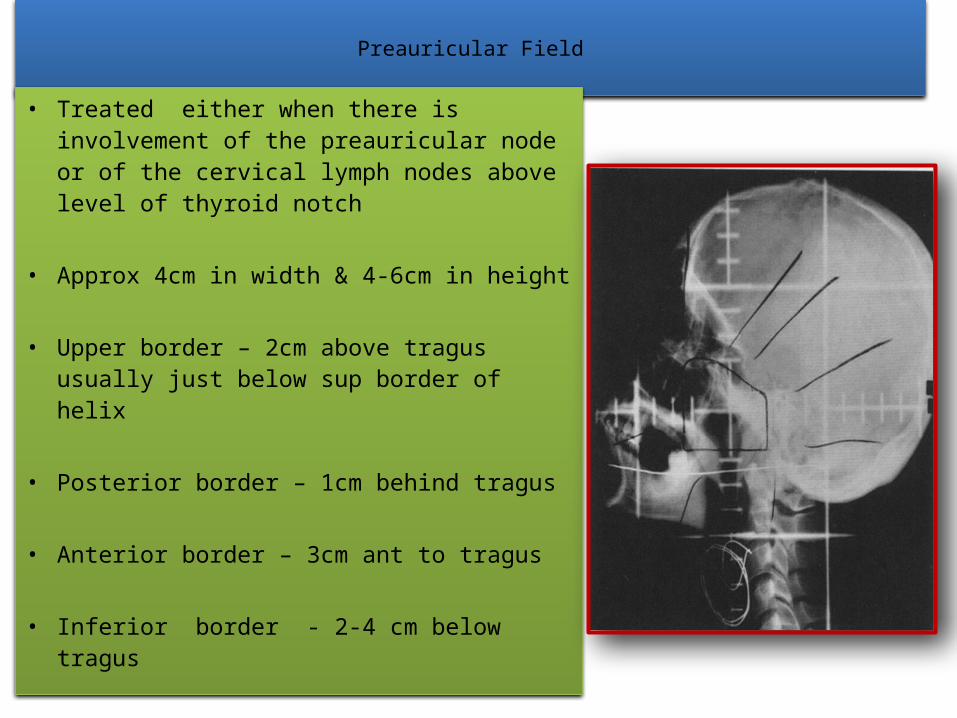
Preauricular Field
• Treated either when there is involvement of the preauricular node or of the cervical lymph nodes above level of thyroid notch
• Approx 4cm in width & 4-6cm in height
• Upper border – 2cm above tragus usually just below sup border of helix
• Posterior border – 1cm behind tragus
• Anterior border – 3cm ant to tragus
• Inferior border - 2-4 cm below tragus
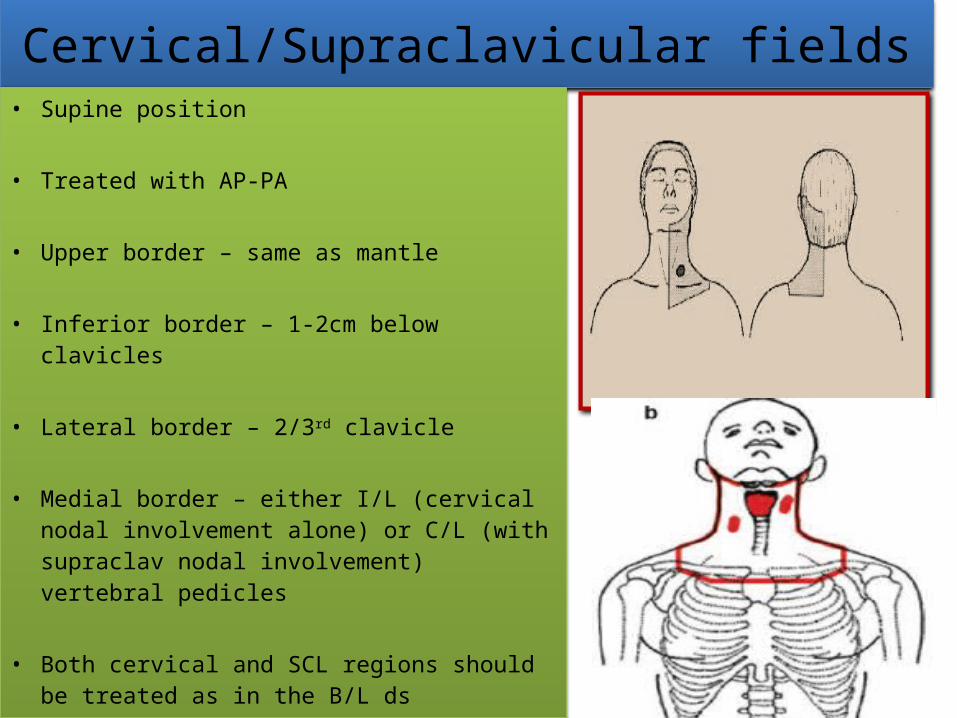
Cervical/Supraclavicular fields• Supine position
• Treated with AP-PA
• Upper border – same as mantle
• Inferior border – 1-2cm below clavicles
• Lateral border – 2/3rd clavicle
• Medial border – either I/L (cervical nodal involvement alone) or C/L (with supraclav nodal involvement) vertebral pedicles
• Both cervical and SCL regions should be treated as in the B/L ds
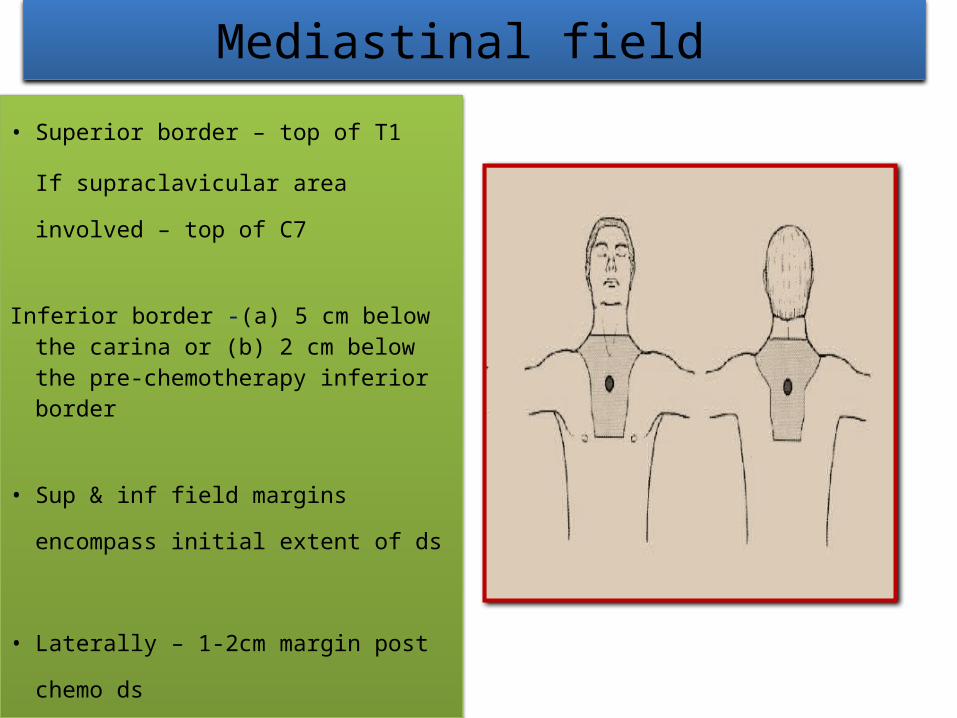
Mediastinal field • Superior border – top of T1
If supraclavicular area involved – top of C7
Inferior border -(a) 5 cm below the carina or (b) 2 cm below the pre-chemotherapy inferior border
• Sup & inf field margins encompass initial extent of ds
• Laterally – 1-2cm margin post chemo ds
Axillary Region
• Arms position: Arms akimbo or arms up.
• Upper Border: C5-6 inter-space.
• Lower Border: The lower of the two: (a) the tip of the scapula or (b) 2 cm below the lowest axillary
node.
• Medial Border: Ipsilateral cervical transverse process.
Abdomen (Para-Aortic Nodes)
• Upper Border: Top of T11 and at least 2 cm above the pre-chemotherapy volume.
• Lower Border: Bottom of L4 and at least 2 cm below pre-chemotherapy volume.
• Lateral Borders: The edge of the transverse processes and atleast 2 cm from the post-chemotherapy volume.
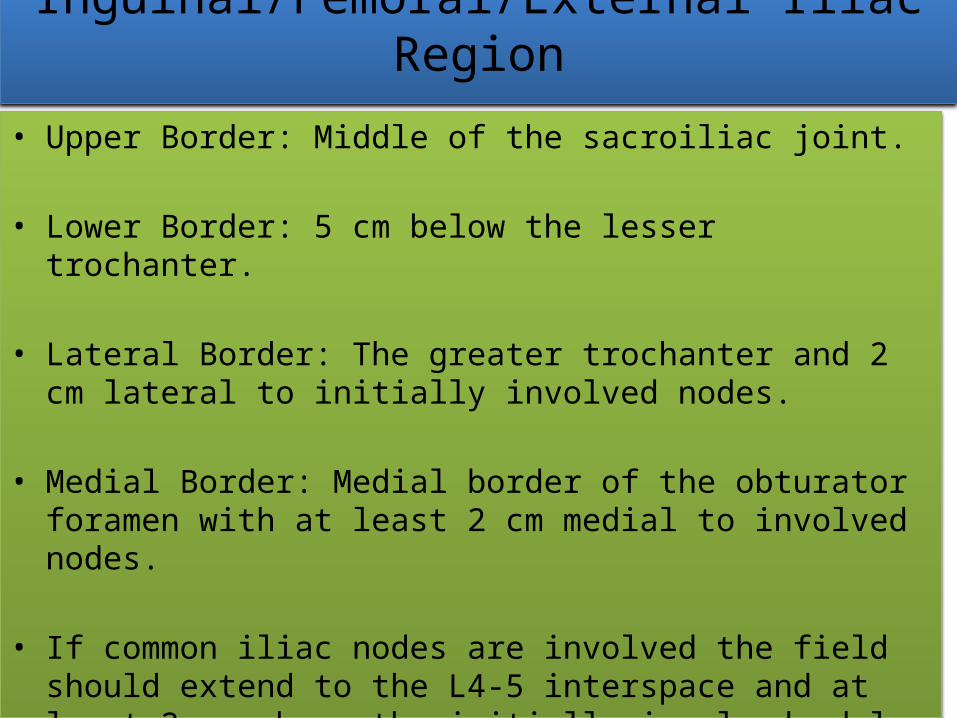
Inguinal/Femoral/External Iliac Region
• Upper Border: Middle of the sacroiliac joint.
• Lower Border: 5 cm below the lesser trochanter.
• Lateral Border: The greater trochanter and 2 cm lateral to initially involved nodes.
• Medial Border: Medial border of the obturator foramen with at least 2 cm medial to involved nodes.
• If common iliac nodes are involved the field should extend to the L4-5 interspace and at least 2 cm above the initially involvednodal border.
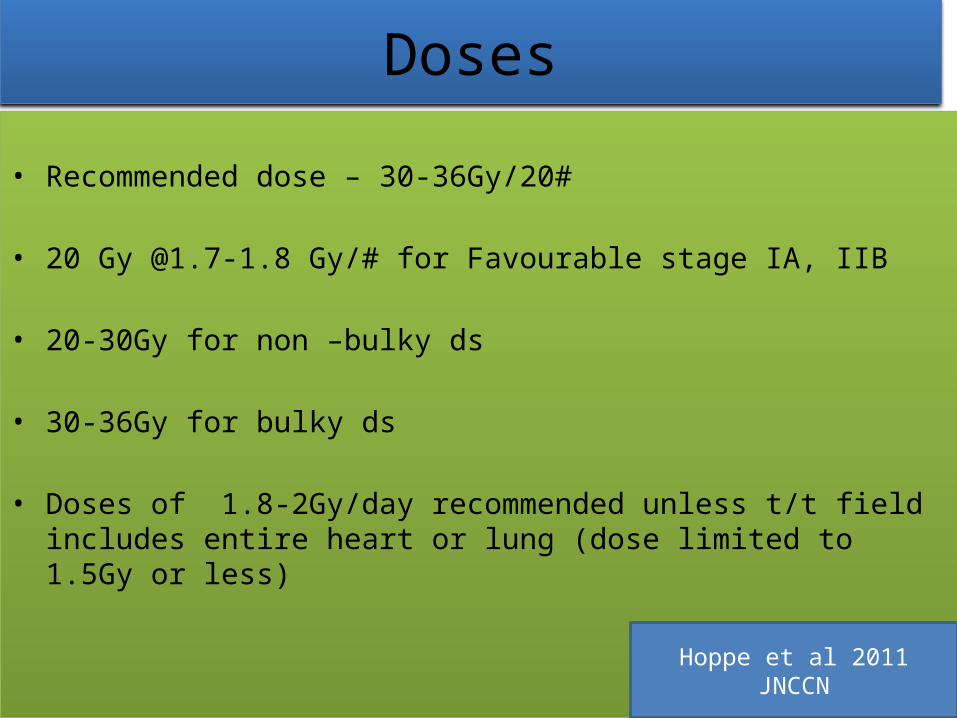
Doses• Recommended dose – 30-36Gy/20#
• 20 Gy @1.7-1.8 Gy/# for Favourable stage IA, IIB
• 20-30Gy for non –bulky ds
• 30-36Gy for bulky ds
• Doses of 1.8-2Gy/day recommended unless t/t field includes entire heart or lung (dose limited to 1.5Gy or less)
Hoppe et al 2011 JNCCN
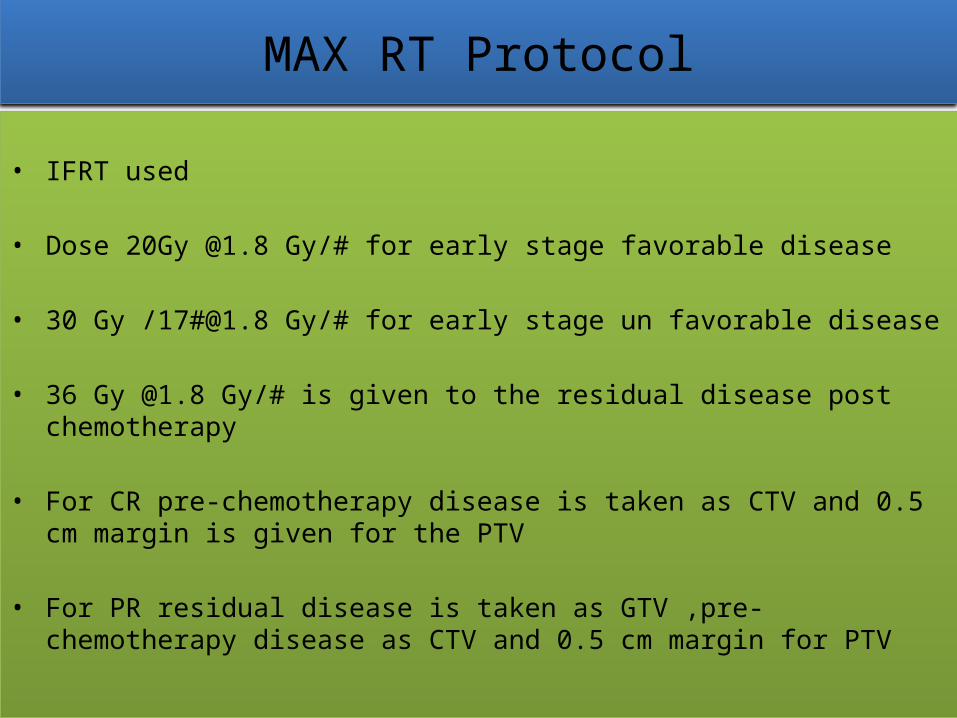
MAX RT Protocol
• IFRT used
• Dose 20Gy @1.8 Gy/# for early stage favorable disease
• 30 Gy /17#@1.8 Gy/# for early stage un favorable disease
• 36 Gy @1.8 Gy/# is given to the residual disease post chemotherapy
• For CR pre-chemotherapy disease is taken as CTV and 0.5 cm margin is given for the PTV
• For PR residual disease is taken as GTV ,pre-chemotherapy disease as CTV and 0.5 cm margin for PTV
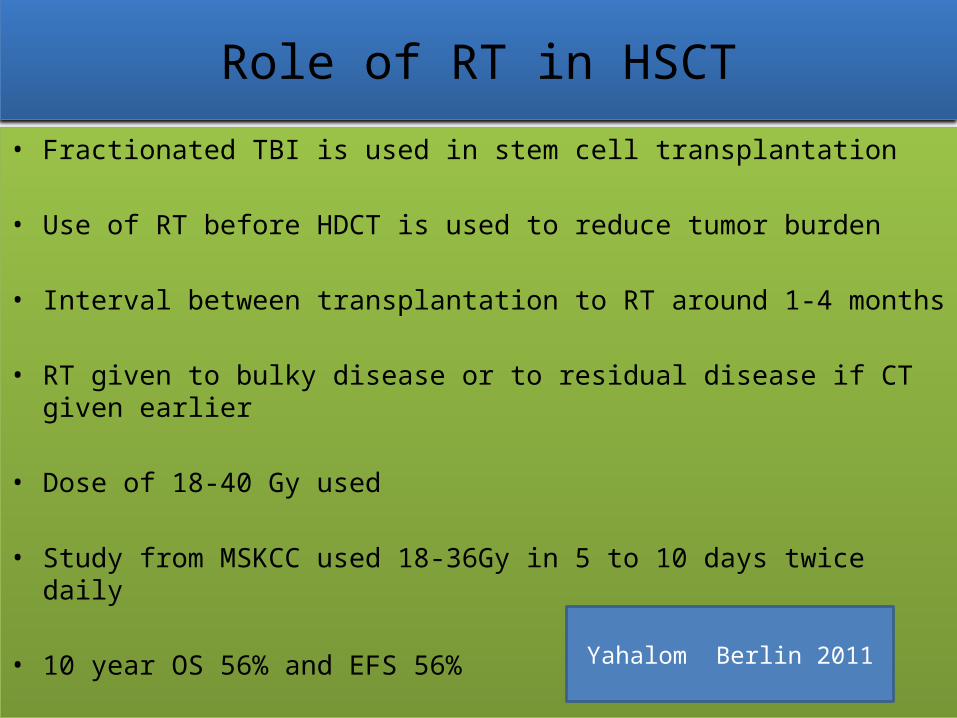
Role of RT in HSCT• Fractionated TBI is used in stem cell transplantation
• Use of RT before HDCT is used to reduce tumor burden
• Interval between transplantation to RT around 1-4 months
• RT given to bulky disease or to residual disease if CT given earlier
• Dose of 18-40 Gy used
• Study from MSKCC used 18-36Gy in 5 to 10 days twice daily
• 10 year OS 56% and EFS 56% Yahalom Berlin 2011

EFRT vs IFRT• Bonadonna et al used IFRT as a part of combined-modality
treatment
• Clinical Stage IA to IIA favorable and unfavorable HL
• The 12-year FFTF rate and overall survival were similar • Thus, four cycles of ABVD→ IFRT effective and safe for Rx of
early-stage favorable and unfavorable HL12 yr FFTF % 12yr OS %
ABVD x4 + STNI 30-40 Gy
93 96
ABVD x4 + IFRT 36-40 Gy
94 94
Bonadonna et al JCO 2004
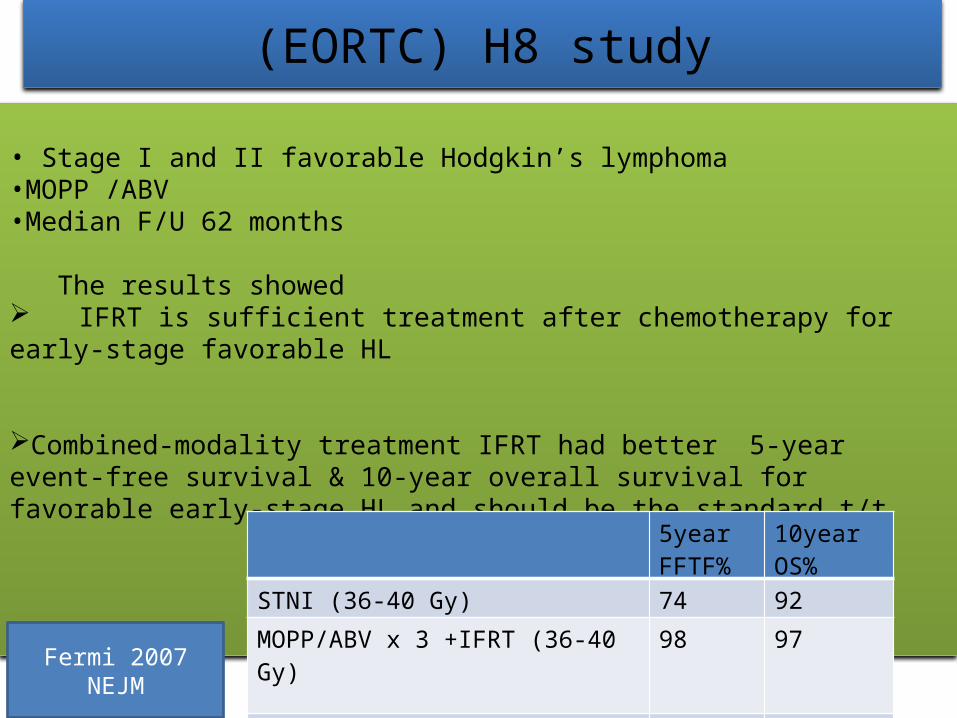
(EORTC) H8 study
• Stage I and II favorable Hodgkin’s lymphoma •MOPP /ABV •Median F/U 62 months
The results showed IFRT is sufficient treatment after chemotherapy for early-stage favorable HL
Combined-modality treatment IFRT had better 5-year event-free survival & 10-year overall survival for favorable early-stage HL and should be the standard t/t
5year FFTF%
10year OS%
STNI (36-40 Gy) 74 92
MOPP/ABV x 3 +IFRT (36-40 Gy) 98 97
P value <.001 .001Fermi 2007 NEJM
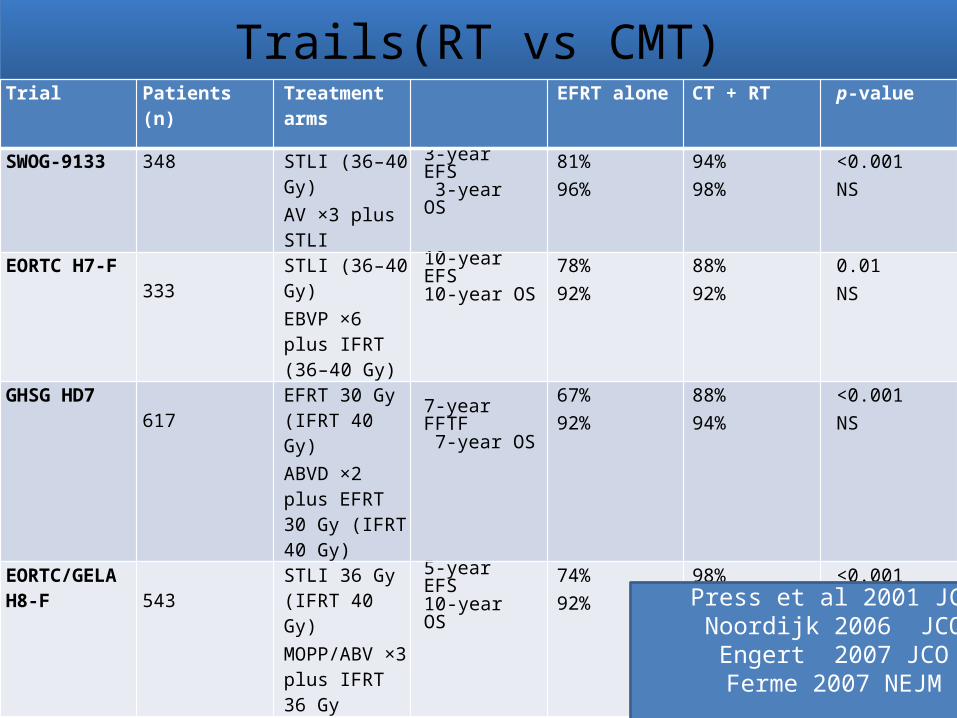
Trails(RT vs CMT)Trial Patients (n) Treatment
armsEFRT alone CT + RT p-value
SWOG-9133 348 STLI (36–40 Gy)AV ×3 plus STLI
3-year EFS 3-year OS 81%
96%94%98%
<0.001NS
EORTC H7-F333
STLI (36–40 Gy)EBVP ×6 plus IFRT (36–40 Gy)
10-year EFS 10-year OS 78%
92%88%92%
0.01NS
GHSG HD7617
EFRT 30 Gy (IFRT 40 Gy)ABVD ×2 plus EFRT 30 Gy (IFRT 40 Gy)
7-year FFTF 7-year OS
67%92%
88%94%
<0.001NS
EORTC/GELA H8-F 543
STLI 36 Gy (IFRT 40 Gy)MOPP/ABV ×3 plus IFRT 36 Gy
5-year EFS 10-year OS 74%
92%98%97%
<0.0010.001
Press et al 2001 JCONoordijk 2006 JCOEngert 2007 JCO
Ferme 2007 NEJM
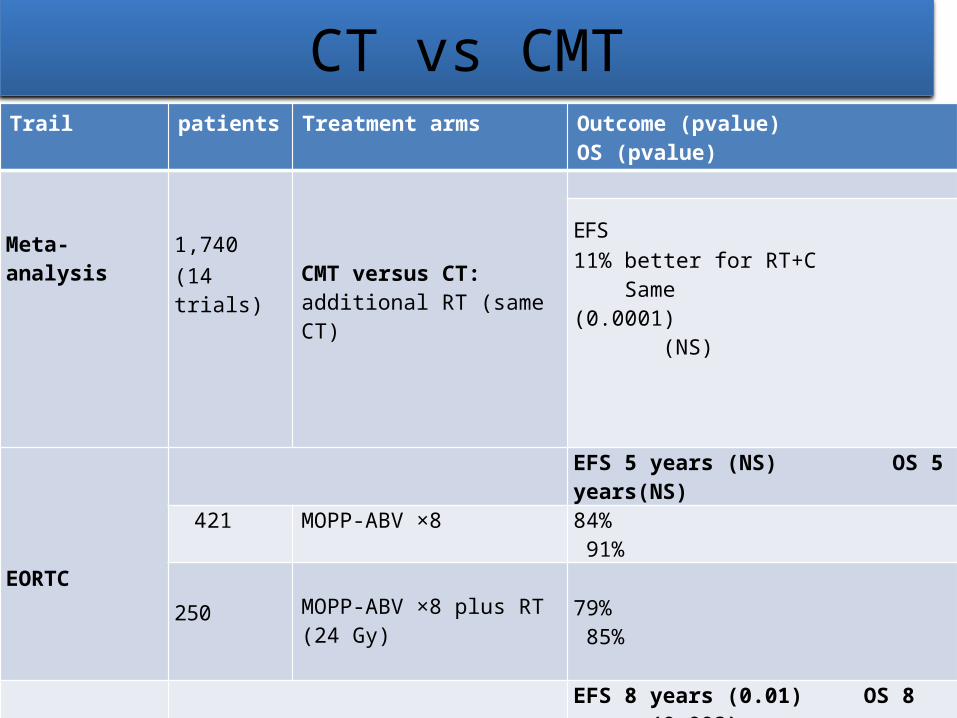
CT vs CMTTrail patients Treatment arms Outcome (pvalue) OS
(pvalue)
Meta-analysis
1,740(14 trials) CMT versus CT:
additional RT (same CT)
EFS11% better for RT+C Same(0.0001) (NS)
EORTC
EFS 5 years (NS) OS 5 years(NS)
421 MOPP-ABV ×8 84% 91%
250 MOPP-ABV ×8 plus RT (24 Gy)
79% 85%
Tata Memorial Hospital
EFS 8 years (0.01) OS 8 years (0.002)
162ABVD ×6 76% 89%
179 ABVD ×6 plus RT 88% 100%
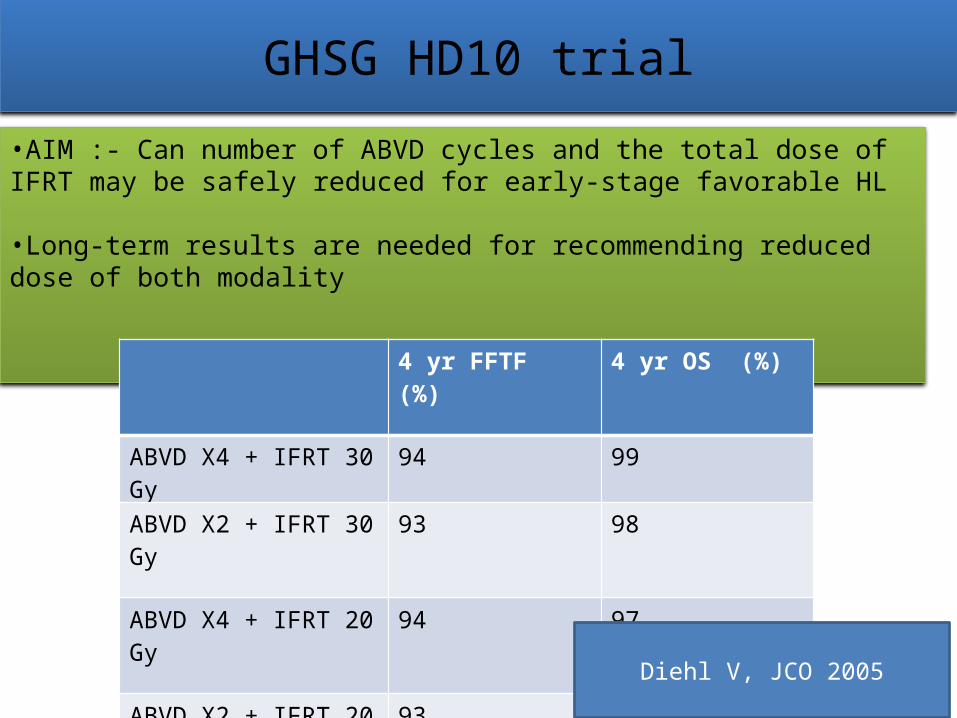
GHSG HD10 trial•AIM :- Can number of ABVD cycles and the total dose of IFRT may be safely reduced for early-stage favorable HL
•Long-term results are needed for recommending reduced dose of both modality
4 yr FFTF (%) 4 yr OS (%)
ABVD X4 + IFRT 30 Gy 94 99
ABVD X2 + IFRT 30 Gy 93 98
ABVD X4 + IFRT 20 Gy 94 97
ABVD X2 + IFRT 20 Gy 93 98
Diehl V, JCO 2005
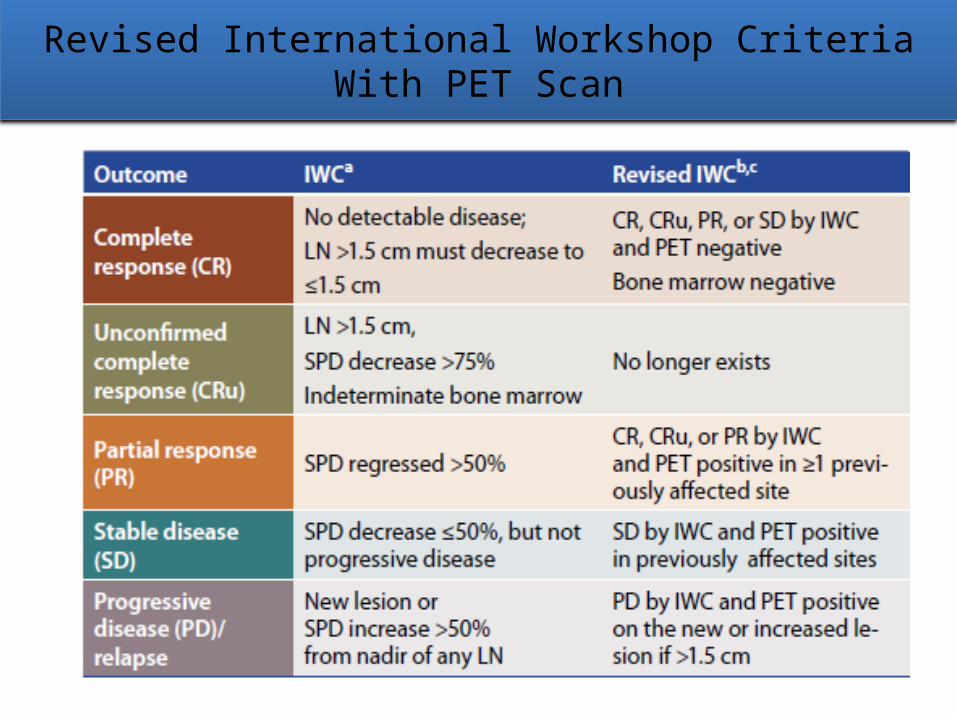
Revised International Workshop Criteria With PET Scan
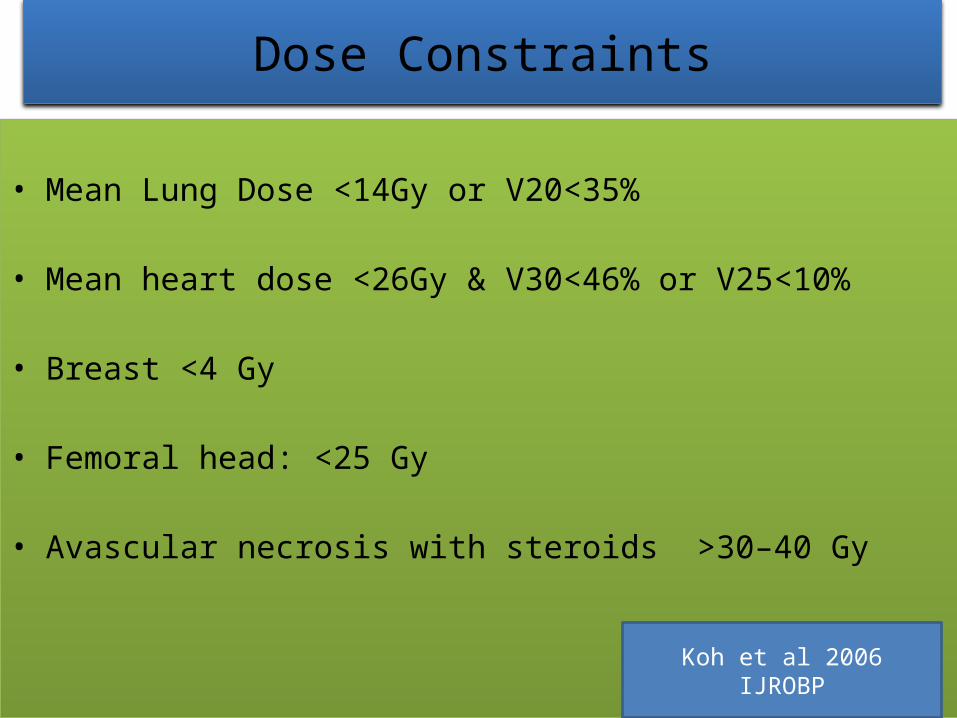
Dose Constraints
• Mean Lung Dose <14Gy or V20<35%
• Mean heart dose <26Gy & V30<46% or V25<10%
• Breast <4 Gy
• Femoral head: <25 Gy
• Avascular necrosis with steroids >30–40 Gy
Koh et al 2006 IJROBP
Sequelae of Treatment• ACUTE REACTIONS:
Fatigue ,nausea,vomiting,dry cough
Occipital hair loss
Sore throat
Skin reactions
Dysphagia
Myelosupression
Sub Acute Side Effects
• Lhermitte's sign: <5% of patients may feel an electric shock sensation radiating down the backs of both legs when the head is flexed (Lhermitte's sign)
• Happens 6 weeks to 3 months after mantle-field RT.
• Pneumonitis and pericarditis: occur in <5% of patients who have extensive mediastinal disease.
Late Side effects
• Subclinical Hypothyroidism in 50% patients who receive >30Gy to neck region
• Herpes zooster in first few years in 10-15% patients
• Streptococcus pneumoniae and H influenzae infection following splenic radiation.
• Infertility: Irradiation to pelvic field effects fertility. It can be prevented by gonadal shielding & oophropexy

• Secondary Malignancies: (1-3%)Increased risk of secondary solid tumors (most commonly, lung, breast, and stomach cancers, as well as melanoma) 10 or more years after treatment.
• Effects on Bone and Muscle Growth: In children, high-dose irradiation affects bone and muscle growth and may result in deformities
• Coronary Artery Disease: Increased risk of coronary artery disease with mediastinal irradiation.
RELAPSE• Most of these relapses (75% to 85%) will occur
during the first 3 years following initial therapy• 3 types of failures known:– Primary Progressive HL– Early relapse ( < 12 months)– Late relapse(>12 months)Early recurrence usually implies resistance to the
original regimen

Treatment Options for Refractory & Relapsed Patients Following Primary Chemotherapy
New Drug
• Recently FDA approved Brentuximab vedotin for HL who relapse after ASCT
• Response rate of 75%
• 1/3rd reaching a complete response
Katz et al Clin Cancer Res 2011
Follow up• Every 3 months for 2 year, then every 6 months for 3–4
years then annually
• With History and physical exam, labs, CXR , CT/PET(once a year).
• Follow thyroid function (annual TSH T3and T4) if in irradiated field.
• Annual mammogram for women <30 years starting 5–8 years
