hiv/aids treatment pharmacists can make a difference · hiv/aids treatment –pharmacists can make...
TRANSCRIPT
HIV/AIDS Treatment – Pharmacists Can Make a Difference
© 2010 Pharmaceutical Education Consultants, Inc. unless otherwise noted. All rights reserved.
Reproduction in whole or in part without permission is prohibited.
Page 1
HIV/AIDS Treatment- Pharmacists can
make a Difference
A Patient Centered Approach to HIV
for Pharmacists & Techs
Peter A. Kreckel
Adjunct Assistant Professor of Pharmacology
Department of Physician Assistant Sciences
St Francis University
PharmCon is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing
pharmacy education
Legal Disclaimer: The material presented here does not necessarily reflect the views of Pharmaceutical Education Consultants (PharmCon) or the companies that support
educational programming. A qualified healthcare professional should always be consulted before using any therapeutic product discussed. Participants should verify all
information and data before treating patients or employing any therapies described in this educational activity.
This program has been
supported by an educational
grant from Boehringer-Ingelheim
HIV/AIDS Treatment- Pharmacists can make a Difference
A Patient Centered Approach to HIV for Pharmacists & Techs
Accreditation:
Pharmacists: 0798-0000-10-062-L02-P
Pharmacy Technicians: 0798-0000-10-062-L02-T
CE Credits: 1 contact hour
Target Audience: Pharmacists & Technicians
Program Overview:
Pharmacists can make a difference in the management and treatment of HIV/AIDS. However, many pharmacists find
themselves uncomfortable with their level of knowledge in the area of HIV either because they did not receive any HIV
training in their formal education or simply because of the rapid on-going advancements in this therapeutic area. This
program will educate pharmacists and pharmacy technicians on HIV treatment principles, provide an update on
pharmacotherapy, and the challenges associated with HIV treatment so they can more comfortable respond to HIV patients
and providers in their role as pharmacist and technician.
Objectives:
• Describe the primary goals of antiretroviral (ARV) treatment and the rationale for prescribing combination therapy.
• Provide an update on antiretroviral therapy (ARV) for HIV to include their mechanisms of action, efficacy, dosing, safety and
tolerability profiles.
• Recognize possible drug interactions between different antiretrovirals and interactions between antiretrovirals and other
medications.
• Describe the pharmacist’s critical role in counseling and educating HIV patients on drug treatment strategies to improve the
patient outcomes and medication adherence.
This program has been
supported by an educational
grant from Boehringer-Ingelheim
HIV/AIDS Treatment- Pharmacists can make a Difference
A Patient Centered Approach to HIV for Pharmacists & Techs
PharmCon is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing
pharmacy education
Legal Disclaimer: The material presented here does not necessarily reflect the views of Pharmaceutical Education Consultants (PharmCon) or the companies
that support educational programming. A qualified healthcare professional should always be consulted before using any therapeutic product discussed.
Participants should verify all information and data before treating patients or employing any therapies described in this educational activity.
This program has been
supported by an educational
grant from Boehringer-Ingelheim
Speaker: Peter A. Kreckel R.Ph. is a graduate of the University of Pittsburgh, Bachelor of Science in Pharmacy, Magna
Cum Laude, Class of 1981. He served as the President of the Pharmacy School Class of 1981 for 3 years, and President
of the Pharmacy School Student Council for 2 years. During this time he received the Upjohn Achievement Award for
leadership and academic achievement. In addition to managing a retail pharmacy, pharmacist Kreckel is an Adjunct
Assistant Professor of Pharmacology, Department of Physicians Assistant Sciences, St. Francis University. His
assignments include teaching a HIV pharmacotherapy course for Physician Assistant students, currently doing their
clinical rotations, that are pursuing a Masters of Medical Science Degree from St. Francis University.
Speaker Disclosure: Mr. Kreckel has no actual or potential conflicts of interest in relation to this program.
GOALS of HIV DRUG THERAPY
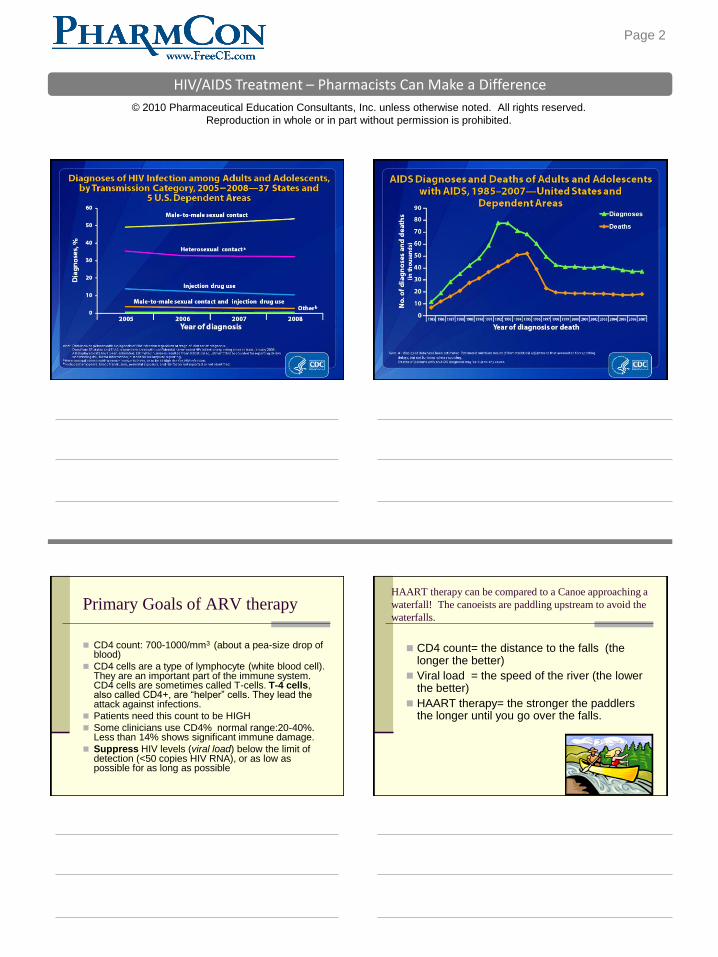
GOAL: to extend life and the quality of life
1981- 1991: only 44% were living after
diagnosis.
1996-2000: 85% of patients were living after
diagnosis
HIV/AIDS Treatment – Pharmacists Can Make a Difference
© 2010 Pharmaceutical Education Consultants, Inc. unless otherwise noted. All rights reserved.
Reproduction in whole or in part without permission is prohibited.
Page 2
Primary Goals of ARV therapy
CD4 count: 700-1000/mm3 (about a pea-size drop of blood)
CD4 cells are a type of lymphocyte (white blood cell). They are an important part of the immune system. CD4 cells are sometimes called T-cells. T-4 cells, also called CD4+, are “helper” cells. They lead the attack against infections.
Patients need this count to be HIGH
Some clinicians use CD4% normal range:20-40%. Less than 14% shows significant immune damage.
Suppress HIV levels (viral load) below the limit of detection (<50 copies HIV RNA), or as low as possible for as long as possible
HAART therapy can be compared to a Canoe approaching a
waterfall! The canoeists are paddling upstream to avoid the
waterfalls.
CD4 count= the distance to the falls (the longer the better)
Viral load = the speed of the river (the lower the better)
HAART therapy= the stronger the paddlers the longer until you go over the falls.
HIV/AIDS Treatment – Pharmacists Can Make a Difference
© 2010 Pharmaceutical Education Consultants, Inc. unless otherwise noted. All rights reserved.
Reproduction in whole or in part without permission is prohibited.
Page 3
CD4 Levels and opportunistic
infections
Most health care providers prescribe drugs to prevent opportunistic infections at the following CD4 levels:
Less than 200: pneumocystis pneumonia (PCP)
Less than 100: toxoplasmosis
Less than 50: mycobacterium avium complex (MAC)
Because they are such an important indicator of the strength of the immune system, official treatment guideline in the US suggest that CD4 counts be monitored every 3 to 4 months.
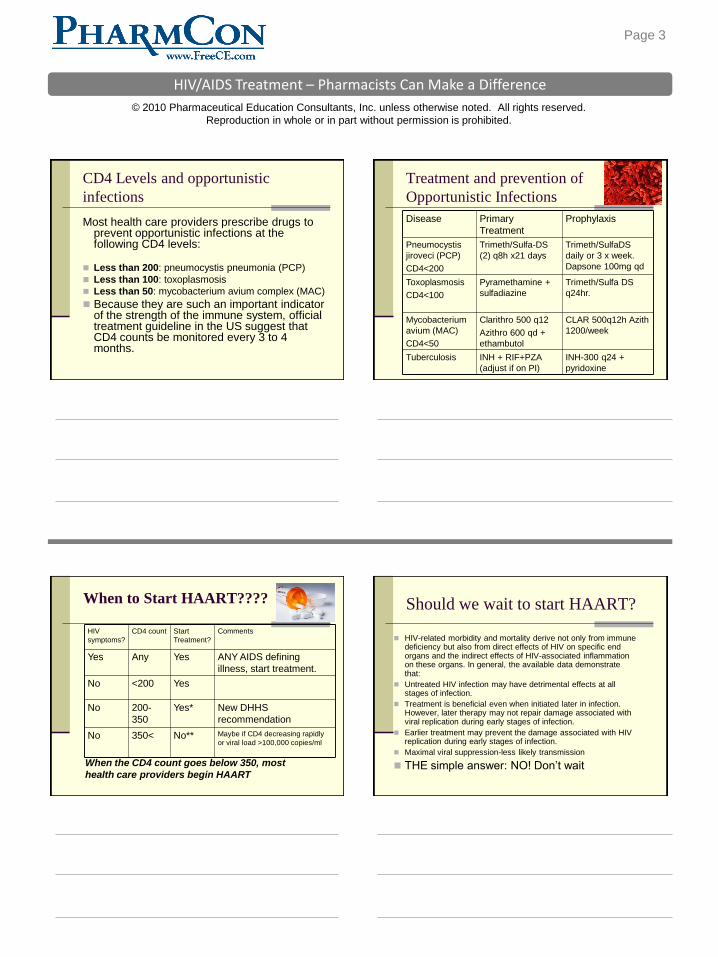
Treatment and prevention of
Opportunistic Infections
Disease Primary
Treatment
Prophylaxis
Pneumocystis
jiroveci (PCP)
CD4<200
Trimeth/Sulfa-DS
(2) q8h x21 days
Trimeth/SulfaDS
daily or 3 x week.
Dapsone 100mg qd
Toxoplasmosis
CD4<100
Pyramethamine +
sulfadiazine
Trimeth/Sulfa DS
q24hr.
Mycobacterium
avium (MAC)
CD4<50
Clarithro 500 q12
Azithro 600 qd +
ethambutol
CLAR 500q12h Azith
1200/week
Tuberculosis INH + RIF+PZA
(adjust if on PI)
INH-300 q24 +
pyridoxine
When to Start HAART????
HIV
symptoms?
CD4 count Start
Treatment?
Comments
Yes Any Yes ANY AIDS defining
illness, start treatment.
No <200 Yes
No 200-
350
Yes* New DHHS
recommendation
No 350< No** Maybe if CD4 decreasing rapidly
or viral load >100,000 copies/ml
When the CD4 count goes below 350, most
health care providers begin HAART
Should we wait to start HAART?
HIV-related morbidity and mortality derive not only from immune deficiency but also from direct effects of HIV on specific end organs and the indirect effects of HIV-associated inflammation on these organs. In general, the available data demonstrate that:
Untreated HIV infection may have detrimental effects at all stages of infection.
Treatment is beneficial even when initiated later in infection. However, later therapy may not repair damage associated with viral replication during early stages of infection.
Earlier treatment may prevent the damage associated with HIV replication during early stages of infection.
Maximal viral suppression-less likely transmission
THE simple answer: NO! Don’t wait
HIV/AIDS Treatment – Pharmacists Can Make a Difference
© 2010 Pharmaceutical Education Consultants, Inc. unless otherwise noted. All rights reserved.
Reproduction in whole or in part without permission is prohibited.
Page 4
Successful HAART Therapy
Cocktails?? The rationale for Combo therapy
Need to have at 3 active drugs from
MULTIPLE drug classes.
When maximal suppression is NOT
achieved or LOST changing to a new
regimen with at least two active drugs is
required.
NEVER change only 1 drug in a
failing regimen.
AIDS DEFINING
CONDITIONS A-I
Candidiasis of bronchi, trachea, or lungs
Candidiasis, esophageal
Cervical cancer, invasive
Coccidioidomycosis, disseminated or extrapulmonary
Cryptococcosis, extrapulmonary
Cryptosporidiosis, chronic intestinal (greater than 1 month's duration)
Cytomegalovirus disease (other than liver, spleen, or nodes)
Cytomegalovirus retinitis (with loss of vision)
Encephalopathy, HIV-related
Herpes simplex: chronic ulcer(s) (greater than 1 month's duration); or bronchitis, pneumonitis, or esophagitis
Histoplasmosis, disseminated or extrapulmonary
Isosporiasis, chronic intestinal (>1 month's duration)
AIDS DEFINING
CONDITIONS K-W Kaposi's sarcoma
Lymphoma, Burkitt's (or equivalent term)
Lymphoma, immunoblastic (or equivalent term)
Lymphoma, primary, of brain
Mycobacterium avium complex or M. kansasii, disseminated or extrapulmonary
Mycobacterium tuberculosis, any site (pulmonary or extrapulmonary) Mycobacterium, other species or unidentified species, disseminated or extrapulmonary
Pneumocystis carinii pneumonia
Pneumonia, recurrent
Progressive multifocal leukoencephalopathy
Salmonella septicemia, recurrent
Toxoplasmosis of brain
Wasting syndrome due to HIV
HIV/AIDS Treatment – Pharmacists Can Make a Difference
© 2010 Pharmaceutical Education Consultants, Inc. unless otherwise noted. All rights reserved.
Reproduction in whole or in part without permission is prohibited.
Page 5
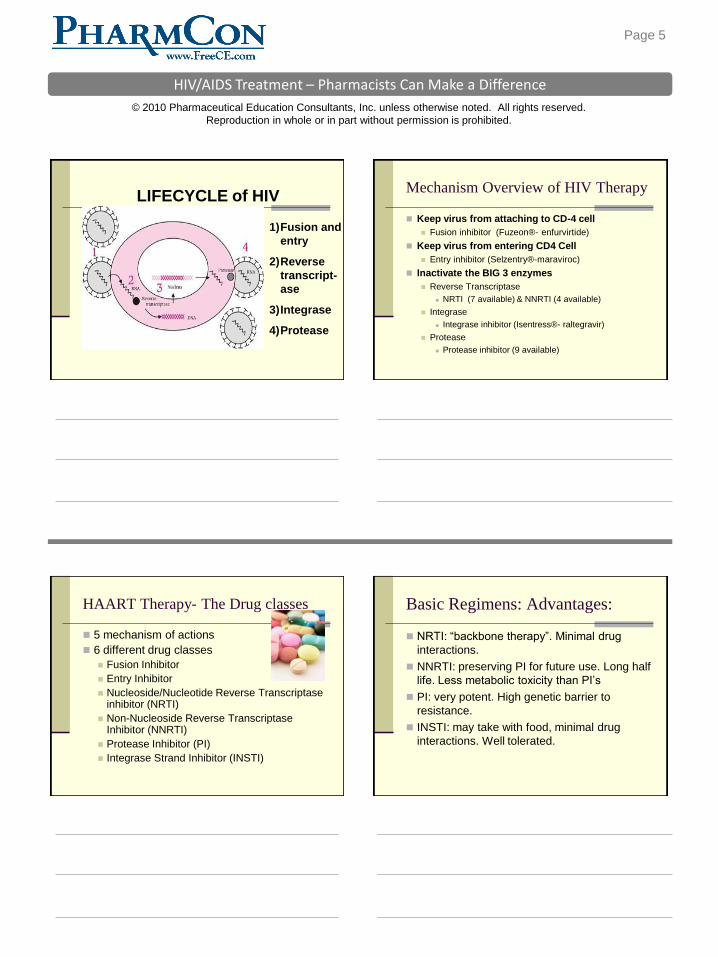
1)Fusion and
entry
2)Reverse
transcript-
ase
3)Integrase
4)Protease
LIFECYCLE of HIVMechanism Overview of HIV Therapy
Keep virus from attaching to CD-4 cell
Fusion inhibitor (Fuzeon®- enfurvirtide)
Keep virus from entering CD4 Cell
Entry inhibitor (Selzentry®-maraviroc)
Inactivate the BIG 3 enzymes
Reverse Transcriptase
NRTI (7 available) & NNRTI (4 available)
Integrase
Integrase inhibitor (Isentress®- raltegravir)
Protease
Protease inhibitor (9 available)
HAART Therapy- The Drug classes
5 mechanism of actions
6 different drug classes
Fusion Inhibitor
Entry Inhibitor
Nucleoside/Nucleotide Reverse Transcriptase inhibitor (NRTI)
Non-Nucleoside Reverse Transcriptase Inhibitor (NNRTI)
Protease Inhibitor (PI)
Integrase Strand Inhibitor (INSTI)
Basic Regimens: Advantages:
NRTI: “backbone therapy”. Minimal drug
interactions.
NNRTI: preserving PI for future use. Long half
life. Less metabolic toxicity than PI’s
PI: very potent. High genetic barrier to
resistance.
INSTI: may take with food, minimal drug
interactions. Well tolerated.
HIV/AIDS Treatment – Pharmacists Can Make a Difference
© 2010 Pharmaceutical Education Consultants, Inc. unless otherwise noted. All rights reserved.
Reproduction in whole or in part without permission is prohibited.
Page 6
Basic Regimens: Disadvantages
NRTI: Lactic acidosis and hepatic steatosis reported with most NRTIs (rare)
NNRTI: Low genetic barrier to resistance. P450 inducers. Cross resistance. Rash. Hepatotoxicity
PI: lots of drug interactions. P450 blockers. GI intolerance. Metabolic complications.
INSTI: headache, diarrhea, nausea, muscle pain, CK elevation. BID dose
INTERACTIVE QUESTION
What is the expected durability of an HIV regimen, when the patient is compliant?
a) 6 months-3 years
b) 3-6 years
c) 6-10 years
TYPE your
answer in
the CHAT
BOX now!
Durability of HIV regimen
With the efavirenz based or PI based
regimens, and GOOD adherence patients are
seeing viral regimens lasting 10 years. Eight
years is the average. ANSWER-C
With even newer potent PI’s and integrase
strand inhibitors, this number could very well
increase
With good adherence HIV can be considered
a manageable chronic disease
Drug Interactions with
anti-Retroviral Drugs
Increases in serum drug levels caused by inhibitors of
metabolism may increase risk of medication toxicity,
while decreases in drug levels caused by inducers of
metabolism may cause treatment failure
Some drug interactions may be exploited, eg, low-dose
ritonavir (a strong CYP3A4 inhibitor) may be used as a
pharmacokinetic enhancer to increase concentrations
and prolong the half-life of other PIs
HIV/AIDS Treatment – Pharmacists Can Make a Difference
© 2010 Pharmaceutical Education Consultants, Inc. unless otherwise noted. All rights reserved.
Reproduction in whole or in part without permission is prohibited.
Page 7
Review of Cytochrome P450
Responsible for the metabolism of numerous drugs
Statins (HMGcoA
reductase inhibitors)
Simvastatin (Zocor®), Lovastatin (Mevacor), Atorvastatin
(Lipitor) are extensively metabolized by P450-3A4
Anti epileptic
medications
Phenytoin (Dilantin®), Carbamazepine (Tegretol®),
Phenobarbital
Antibiotics Erythromycin (E-mycin®), Clarithromycin (Biaxin®)
Telithromycin (Ketek®)
Antidepressants Fluoxetine (Prozac®), Sertraline (Zoloft®), Citalopram
(Celexa®), Paroxetine (Paxil®)
Methadone
Azole antifungals Ketoconazole (nizoral®), Fluconazole (Diflucan)
Amiodarone (Cordarone®)
Protease Inhibitors
RITONAVIR BOOSTING “the ultimate beneficial drug-drug interaction”
Ritonavir (Norvir®) by Abbott Labs
(available at capsules or tablets)
Is the most potent inhibitor of the Cytochrome P450 enzyme system
ALL PI are substrates of CYP450-3A4 so their metabolic rate may be
altered in the presence of CYP inducers or inhibitors
Consultation with HIV patients
“Communication skills are essential in any
patient consultation scenario. That being
said, product knowledge is paramount before
any discussion of ANY drug therapy with ANY
patient”
Peter Kreckel- shares this with any pharmacy student.
Viral Fusion Inhibitor(used for treatment experienced patients—salvage therapy)
Mechanism:
Blocks the fusion of the HIV virus into the host cell
Adverse reactions:
Injection site reactions, recurrent pneumonia, diarrhea,
nausea, fatigue
Fuzeon ® Enfuviritide T-20 dose 90mg SQ BID 60 = $2,552.74
HIV/AIDS Treatment – Pharmacists Can Make a Difference
© 2010 Pharmaceutical Education Consultants, Inc. unless otherwise noted. All rights reserved.
Reproduction in whole or in part without permission is prohibited.
Page 8
CCR5 Co-Receptor Antagonist(used for treatment experienced patients)
Mechanism: Binds to a receptor called CCR5 on white
blood cells.
Adverse reactions: hepatotoxicity, cough, pyrexia, upper respiratory infections, abdominal pain, dizziness
Selzentry® maraviroc 300mg BID
(adjust for P450)
$900.00/ month
Brand Generic Abbr Dosage
Emtriva® Emtricitabine FTC 200mg daily
Epivir® Lamivudine 3TC 150mg BID or 300/day
Retrovir® Zidovudine AZT 300mg BID
Videx® Didanosine ddl 250mg or 400mg daily
Viread® Tenofovir DF TDF 300mg/day
Zerit® Stavudine d4T 20, 30 or 40mg BID
Ziagen® Abacabir ABC 300mg BID or 600mg/day
Videx EC ® didanosine 250-400mg daily
NRTI (nucleoside/nucleotide reverse transcriptase inhibitors)
Mechanism: NRTI interfere with viral-RNA dependent DNA-polymerase resulting in chain termination and inhibition of viral replication.
Use 2 drugs from this class for “backbone therapy”)
NOTE: Preferred combo: tenofovir + emtricitabine
for all 4 regimens for treatment naïve patients
NNRTI- non-nucleoside reverse transcriptase
inhibitors.
Brand Generic Abbr Dosage
Viramune® Nevirapine NVP 200mg daily x14 days, then
200q12
Sustiva® Efavirenz EFZ 600mg HS
Rescriptor® Delaviridine DLV 400-600 mg every 8 hours
Intelence® Etravirine 200mg (2x100mg) BID pc
NNRTI preferred agents:
Sustiva is NNRTI of choice unless pregnant- Preg cat-D
Viramune is NNRTI of choice if pregnant.
Sustiva+ Truvada= Atripla one pill daily.
highly selective, noncompetitive inhibitors of HIV-1 reverse
transcriptase. Class cross resistance (except Intelence)
Integrase Inhibitors
Mechanism: Interferes with enzyme needed to integrate
viral DNA into host cell DNA. It transports the proviral
DNA into the host cell nucleus. There it is integrated
into the target cells' DNA.
Adverse reactions: headache, nausea,
diarrhea, pyrexia, CK elevation,
rhabdomyolysis, myopathy.
Isentress® Raltegravir 400mg BID + or -
food
60 = $1072.24
HIV/AIDS Treatment – Pharmacists Can Make a Difference
© 2010 Pharmaceutical Education Consultants, Inc. unless otherwise noted. All rights reserved.
Reproduction in whole or in part without permission is prohibited.
Page 9
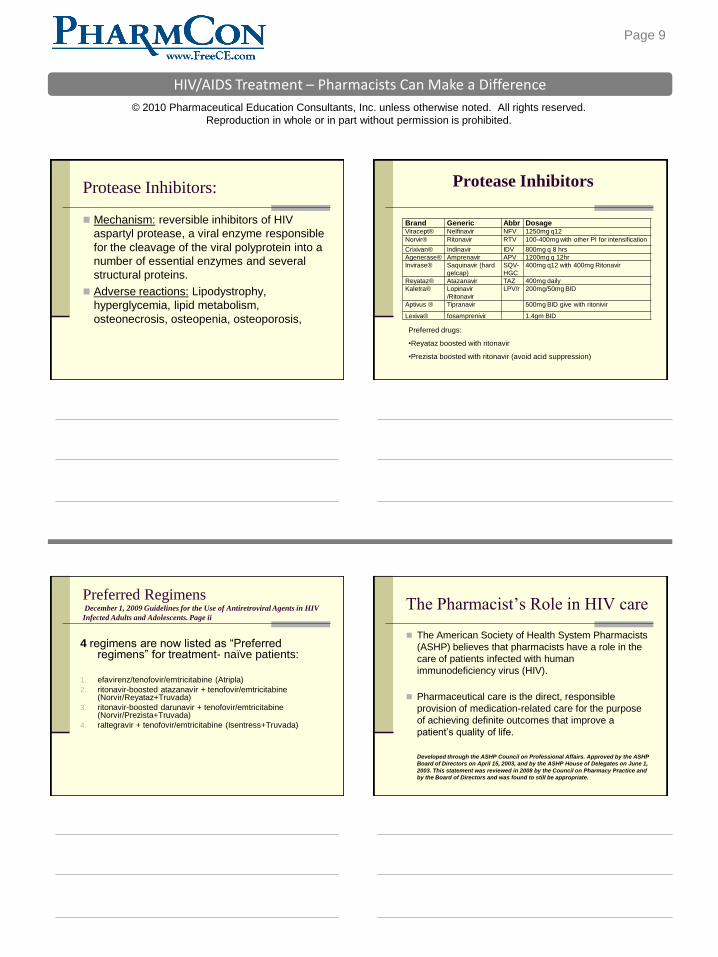
Protease Inhibitors:
Mechanism: reversible inhibitors of HIV
aspartyl protease, a viral enzyme responsible
for the cleavage of the viral polyprotein into a
number of essential enzymes and several
structural proteins.
Adverse reactions: Lipodystrophy,
hyperglycemia, lipid metabolism,
osteonecrosis, osteopenia, osteoporosis,
Protease Inhibitors
Brand Generic Abbr DosageViracept® Nelfinavir NFV 1250mg q12
Norvir® Ritonavir RTV 100-400mg with other PI for intensification
Crixivan® Indinavir IDV 800mg q 8 hrs
Agenerase® Amprenavir APV 1200mg q 12hr
Invirase® Saquinavir (hard
gelcap)
SQV-
HGC
400mg q12 with 400mg Ritonavir
Reyataz® Atazanavir TAZ 400mg daily
Kaletra® Lopinavir
/Ritonavir
LPV/r 200mg/50mg BID
Aptivus ® Tipranavir 500mg BID give with ritonivir
Lexiva® fosamprenivir 1.4gm BID
Preferred drugs:
•Reyataz boosted with ritonavir
•Prezista boosted with ritonavir (avoid acid suppression)
Preferred Regimens December 1, 2009 Guidelines for the Use of Antiretroviral Agents in HIV
Infected Adults and Adolescents. Page ii
4 regimens are now listed as “Preferred regimens” for treatment- naïve patients:
1. efavirenz/tenofovir/emtricitabine (Atripla)
2. ritonavir-boosted atazanavir + tenofovir/emtricitabine (Norvir/Reyataz+Truvada)
3. ritonavir-boosted darunavir + tenofovir/emtricitabine (Norvir/Prezista+Truvada)
4. raltegravir + tenofovir/emtricitabine (Isentress+Truvada)
The Pharmacist’s Role in HIV care
The American Society of Health System Pharmacists
(ASHP) believes that pharmacists have a role in the
care of patients infected with human
immunodeficiency virus (HIV).
Pharmaceutical care is the direct, responsible
provision of medication-related care for the purpose
of achieving definite outcomes that improve a
patient’s quality of life.
Developed through the ASHP Council on Professional Affairs. Approved by the ASHP
Board of Directors on April 15, 2003, and by the ASHP House of Delegates on June 1,
2003. This statement was reviewed in 2008 by the Council on Pharmacy Practice and
by the Board of Directors and was found to still be appropriate.
HIV/AIDS Treatment – Pharmacists Can Make a Difference
© 2010 Pharmaceutical Education Consultants, Inc. unless otherwise noted. All rights reserved.
Reproduction in whole or in part without permission is prohibited.
Page 10
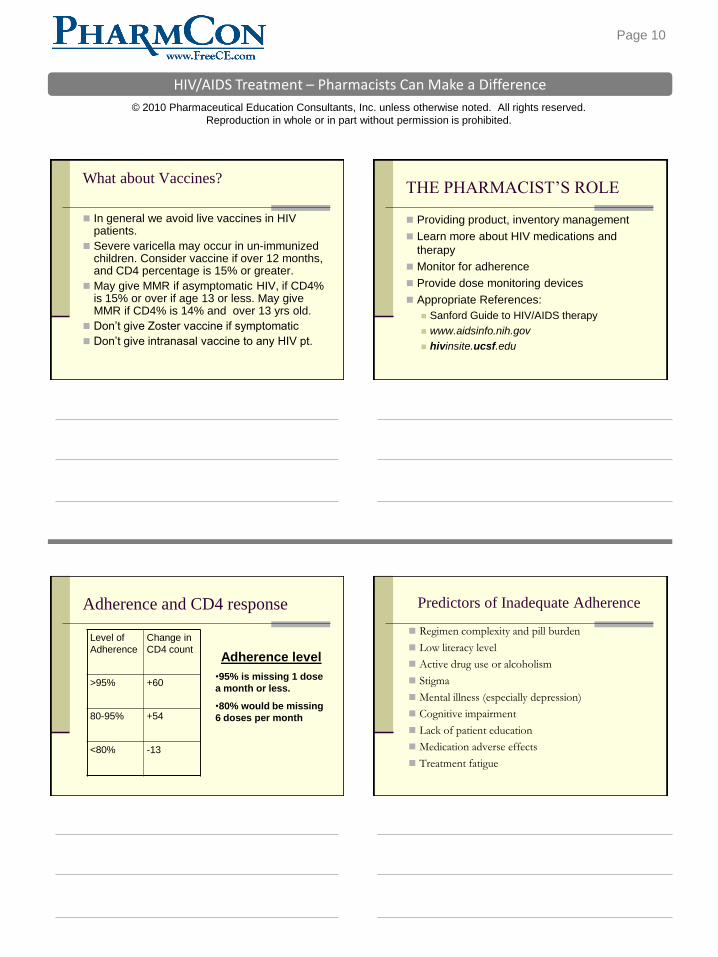
What about Vaccines?
In general we avoid live vaccines in HIV patients.
Severe varicella may occur in un-immunized children. Consider vaccine if over 12 months, and CD4 percentage is 15% or greater.
May give MMR if asymptomatic HIV, if CD4% is 15% or over if age 13 or less. May give MMR if CD4% is 14% and over 13 yrs old.
Don’t give Zoster vaccine if symptomatic
Don’t give intranasal vaccine to any HIV pt.
THE PHARMACIST’S ROLE
Providing product, inventory management
Learn more about HIV medications and
therapy
Monitor for adherence
Provide dose monitoring devices
Appropriate References:
Sanford Guide to HIV/AIDS therapy
www.aidsinfo.nih.gov
hivinsite.ucsf.edu
Adherence and CD4 response
Level of
Adherence
Change in
CD4 count
>95% +60
80-95% +54
<80% -13
Adherence level
•95% is missing 1 dose
a month or less.
•80% would be missing
6 doses per month
Predictors of Inadequate Adherence
Regimen complexity and pill burden
Low literacy level
Active drug use or alcoholism
Stigma
Mental illness (especially depression)
Cognitive impairment
Lack of patient education
Medication adverse effects
Treatment fatigue
HIV/AIDS Treatment – Pharmacists Can Make a Difference
© 2010 Pharmaceutical Education Consultants, Inc. unless otherwise noted. All rights reserved.
Reproduction in whole or in part without permission is prohibited.
Page 11
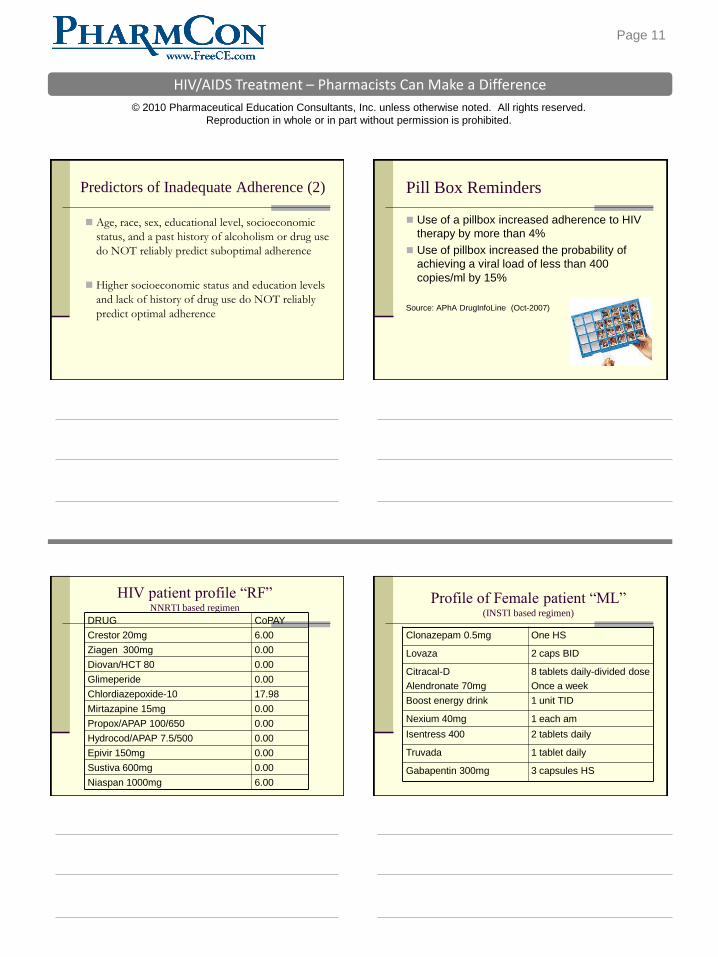
Predictors of Inadequate Adherence (2)
Age, race, sex, educational level, socioeconomic
status, and a past history of alcoholism or drug use
do NOT reliably predict suboptimal adherence
Higher socioeconomic status and education levels
and lack of history of drug use do NOT reliably
predict optimal adherence
Pill Box Reminders
Use of a pillbox increased adherence to HIV
therapy by more than 4%
Use of pillbox increased the probability of
achieving a viral load of less than 400
copies/ml by 15%
Source: APhA DrugInfoLine (Oct-2007)
HIV patient profile “RF”NNRTI based regimen
DRUG CoPAY
Crestor 20mg 6.00
Ziagen 300mg 0.00
Diovan/HCT 80 0.00
Glimeperide 0.00
Chlordiazepoxide-10 17.98
Mirtazapine 15mg 0.00
Propox/APAP 100/650 0.00
Hydrocod/APAP 7.5/500 0.00
Epivir 150mg 0.00
Sustiva 600mg 0.00
Niaspan 1000mg 6.00
Profile of Female patient “ML”(INSTI based regimen)
Clonazepam 0.5mg One HS
Lovaza 2 caps BID
Citracal-D
Alendronate 70mg
8 tablets daily-divided dose
Once a week
Boost energy drink 1 unit TID
Nexium 40mg 1 each am
Isentress 400 2 tablets daily
Truvada 1 tablet daily
Gabapentin 300mg 3 capsules HS
HIV/AIDS Treatment – Pharmacists Can Make a Difference
© 2010 Pharmaceutical Education Consultants, Inc. unless otherwise noted. All rights reserved.
Reproduction in whole or in part without permission is prohibited.
Page 12
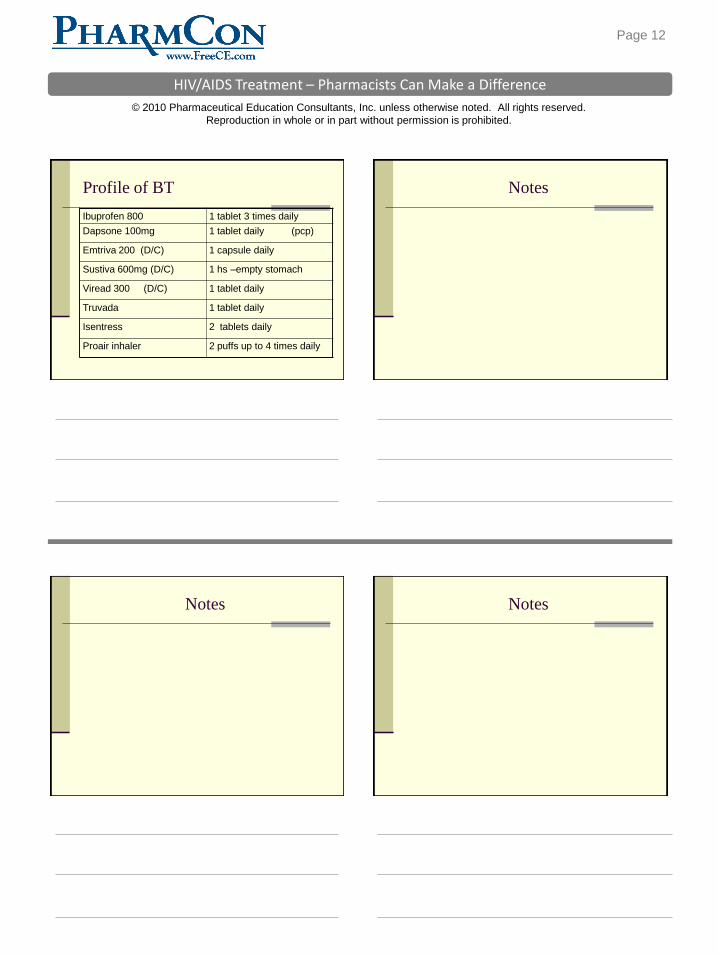
Profile of BT
Ibuprofen 800 1 tablet 3 times daily
Dapsone 100mg 1 tablet daily (pcp)
Emtriva 200 (D/C) 1 capsule daily
Sustiva 600mg (D/C) 1 hs –empty stomach
Viread 300 (D/C) 1 tablet daily
Truvada 1 tablet daily
Isentress 2 tablets daily
Proair inhaler 2 puffs up to 4 times daily
Notes
Notes Notes