hiatus hernia children - pmj.bmj.com · hiatus hernia in children 503 phagitis the degree ofacidity...
TRANSCRIPT

Postgraduate Medical Journal (August 1972) 48, 501-506.
Hiatus hernia in children
JAMES LISTERF.R.C.S.
Children's Hospital, Western Bank, Sheffield
THE term congenital diaphragmatic hernia tends tobe applied to the dramatic herniation of small intes-tine and other abdominal organs through the for-amen of Bochdalek into the left pleural cavity withconsequent acute respiratory disturbances. Suchchildren commonly present as acute emergenciesduring the first few days of life. However, hiatushernia is also frequently of congenital origin andthis is not only a much more common condition butalso one that can lead to much more morbidity andeven mortality.
Hiatus hernia can be defined as a displacementof the cardio-oesophageal junction above the levelof the diaphragm, or a protrusion of part of thestomach through the oesophageal hiatus. Both thesetypes of the abnormality have been demonstratedin the newly born and are being demonstrated withincreasing frequency in young children. It is difficultto regard similar conditions presenting in olderpatients as an entirely different disease but at thesame time an explanation must be given to the factthat so many of these cases do not present until thepatients reach the age of 50-60 years. The diagnosiscan only be made positively by demonstrating cardio-oesophageal displacement or herniation of thestomach through the oesophageal hiatus; such de-monstration may be achieved at necropsy, at surgicalexploration or at radiological examination. The re-ported incidence of the condition thus tends to varywith the enthusiasm of the radiologist and the avail-ability of special equipment but there is no doubtthat continuing improvement in radiological tech-niques have brought to light many more cases ofhiatus hernia in children than had previously beendemonstrated as well as many more cases occurringin adults.The increased frequency with which supra-
diaphragmatic pouches of stomach have beendemonstrated on radiological examination has led toan acceptance of the idea that gastro-oesophagealreflux in the newly born and young child is probablyan early stage of hiatus hernia; indeed it might bethat a hiatus hernia was present but had not beendemonstrated. Both in adults and children it is in-creasingly accepted that the actual hiatus hernia is
of far less importance than the consequent func-tional disturbance at the cardio-oesophageal junctionleading to free gastro-oesophageal reflux, oeso-phagitis and possibly oesophageal stricture.
IncidenceIt is thus difficult to estimate the true incidence of
hiatus hernia since almost certainly a number ofcases are not demonstrated radiologically and equallya number of clinical diagnoses are made withoutradiological demonstration. Skinner & Belsey, how-ever, in 1967 reported 119 children in their series ofsome 1500 cases operated on and Carre in 1970suggests that in the United Kingdom the incidenceof the disease in children is 1 in 1000.There is no doubt that the condition is a great deal
more common than is generally suspected andwarrants rather more attention than it is given in theaverage textbook of paediatrics. While probablymore than two-thirds of the children with the con-dition even untreated become symptom-free by theage of 2 years, usually improving when they get onto a weaning diet (Carre, 1959), there is neverthelessa three-fold increase in pulmonary infections inchildren who vomit during the night, and the othercommon complication of oesophagitis can lead tosevere stenosis of the oesophagus necessitating majorreplacement surgery.
AetiologyThe common surgical finding in these children is
that there is an abnormally large oesophageal hiatuswith lax margins. It is possible that this may beassociated with delay in the developmental descent ofthe stomach relative to the closing of the variouselements of the diaphragm which occurs about theseventh week of foetal development; if this were sothe descent of the stomach must continue after theinadequate closing of the diaphragm because theoccurrence of a congenitally short oesophagus isalmost universally accepted as occurring excessivelyrarely, if at all. Free gastro-oesophageal reflux is analmost universal feature of the neonatal period andit is perhaps rather more attractive to suggest anendocrine factor relating this to the loosening up of
copyright. on 30 M
arch 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.48.562.501 on 1 A
ugust 1972. Dow
nloaded from
502 James Lister
mesenchymal tissues in pregnancy and in the meno-pause, which may play a part in the development ofhiatus hernia in adults (Allison, 1970). The newlyborn child shows evidence at birth of the effect of itsmother's hormones in its enlarged genitalia and thefree gastro-oesophageal reflux in the newborn periodwhich lasts only a few days may be similarly pro-duced.
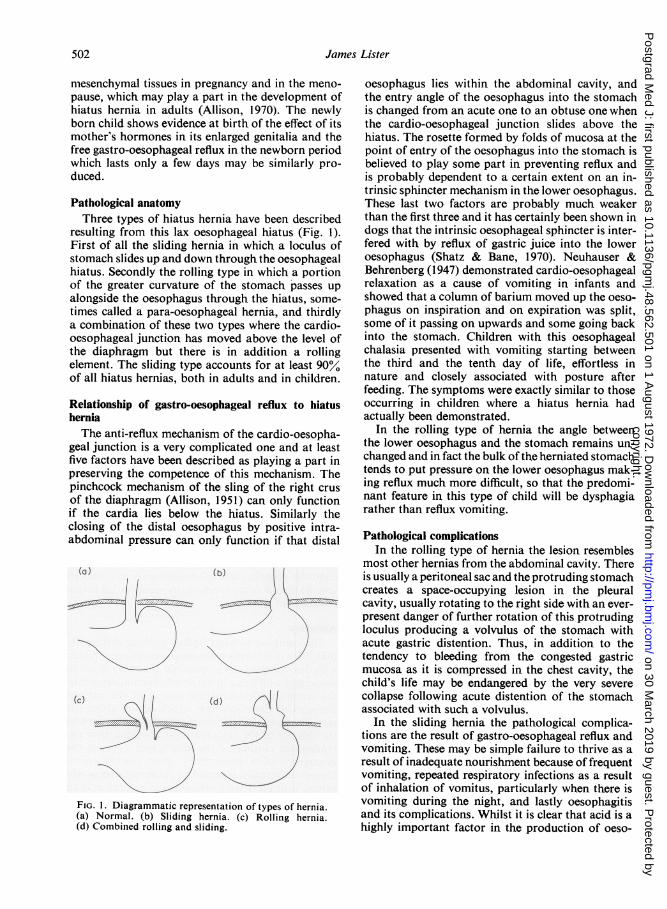
Pathological anatomyThree types of hiatus hernia have been described
resulting from this lax oesophageal hiatus (Fig. 1).First of all the sliding hernia in which a loculus ofstomach slides up and down through the oesophagealhiatus. Secondly the rolling type in which a portionof the greater curvature of the stomach passes upalongside the oesophagus through the hiatus, some-times called a para-oesophageal hernia, and thirdlya combination of these two types where the cardio-oesophageal junction has moved above the level ofthe diaphragm but there is in addition a rollingelement. The sliding type accounts for at least 90/0of all hiatus hernias, both in adults and in children.
Relationship of gastro-oesophageal reflux to hiatusherniaThe anti-reflux mechanism of the cardio-oesopha-
geal junction is a very complicated one and at leastfive factors have been described as playing a part inpreserving the competence of this mechanism. Thepinchcock mechanism of the sling of the right crusof the diaphragm (Allison, 1951) can only functionif the cardia lies below the hiatus. Similarly theclosing of the distal oesophagus by positive intra-abdominal pressure can only function if that distal
:"L-;:-.'..!... ..... ... .. :~ .. .. ?. ,;: ................
:.".:.'.'1,; :'"' .. .;.:.i'........... ", .............. t;. ,,.': .- :'
;.. .......... .. i · : .:
; ;r |
;i--,,... : . . --.;.:~ '.i ."..~'.;· .. .4-. :,.;.,'....:........·.........,.,....','FIG. 1. Diagrammatic representation of types of hernia.(a) Normal. (b) Sliding hernia. (c) Rolling hernia.(d) Combined rolling and sliding.
oesophagus lies within the abdominal cavity, andthe entry angle of the oesophagus into the stomachis changed from an acute one to an obtuse one whenthe cardio-oesophageal junction slides above thehiatus. The rosette formed by folds of mucosa at thepoint of entry of the oesophagus into the stomach isbelieved to play some part in preventing reflux andis probably dependent to a certain extent on an in-trinsic sphincter mechanism in the lower oesophagus.These last two factors are probably much weakerthan the first three and it has certainly been shown indogs that the intrinsic oesophageal sphincter is inter-fered with by reflux of gastric juice into the loweroesophagus (Shatz & Bane, 1970). Neuhauser &Behrenberg (1947) demonstrated cardio-oesophagealrelaxation as a cause of vomiting in infants andshowed that a column of barium moved up the oeso-phagus on inspiration and on expiration was split,some of it passing on upwards and some going backinto the stomach. Children with this oesophagealchalasia presented with vomiting starting betweenthe third and the tenth day of life, effortless innature and closely associated with posture afterfeeding. The symptoms were exactly similar to thoseoccurring in children where a hiatus hernia hadactually been demonstrated.
In the rolling type of hernia the angle betweenthe lower oesophagus and the stomach remains un-changed and in fact the bulk of the herniated stomachtends to put pressure on the lower oesophagus mak-ing reflux much more difficult, so that the predomi-nant feature in this type of child will be dysphagiarather than reflux vomiting.
Pathological complicationsIn the rolling type of hernia the lesion resembles
most other hernias from the abdominal cavity. Thereis usually a peritoneal sac and the protruding stomachcreates a space-occupying lesion in the pleuralcavity, usually rotating to the right side with an ever-present danger of further rotation of this protrudingloculus producing a volvulus of the stomach withacute gastric distention. Thus, in addition to thetendency to bleeding from the congested gastricmucosa as it is compressed in the chest cavity, thechild's life may be endangered by the very severecollapse following acute distention of the stomachassociated with such a volvulus.
In the sliding hernia the pathological complica-tions are the result of gastro-oesophageal reflux andvomiting. These may be simple failure to thrive as aresult of inadequate nourishment because of frequentvomiting, repeated respiratory infections as a resultof inhalation of vomitus, particularly when there isvomiting during the night, and lastly oesophagitisand its complications. Whilst it is clear that acid is ahighly important factor in the production of oeso-
copyright. on 30 M
arch 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.48.562.501 on 1 A
ugust 1972. Dow
nloaded from

Hiatus hernia in children 503
phagitis the degree of acidity of the gastric contentsand the duration of exposure of theloweroesophagusto that gastric content has not been shown in adults,at least, to have much relationship to the severityof the oesophagitis (Collis, 1970). This unexplainedvariation in response to persistent gastro-oesopha-geal reflux is a most important feature of the diseasein children because whilst it is true that in a largenumber of cases the symptoms settle without leavingany permanent damage to the lower oesophagus andeven of those cases operated upon a simple procedureis sufficient to bring the majority under control,there remains a small number, probably less than10% of all cases, in whom peptic oesophagitis pro-duces severe results with scarring and eventuallydemands resection of the lower oesophagus.Management of these children is designed to avoid
the pathological complication in the rolling hernia orthe combined type. Spontaneous regression will notoccur and surgical correction is indicated in all cases.In the sliding hernia, however, when as many as two-thirds of the cases may be expected to resolve spon-taneously, surgical treatment in all cases would beunjustifiable. At the same time it is very importantthat those children likely to develop severe oesopha-gitis should be dealt with before irreversible changeshave occurred in the oesophageal mucosa; and lessobviously, recurrent inhalational respiratory infec-tions and failure to thrive must be recognized beforethey interfere seriously with the child's ultimatedevelopment.These then are the indications for surgical inter-
vention. The institution of conservative managementand its various aspects depends on the diagnosis ofthe condition and a knowledge of its natural history.
Signs and symptomsVomitingThe classical presentation of hiatus hernia in child-
ren is with a history of vomiting from birth. Over90% of the children will certainly vomit during thefirst month of life and the majority will in fact startduring the first day or two. The vomiting is usuallyforceful in character and may even be projectile,resembling the vomiting due to congenital hyper-trophic pyloric stenosis, but the very early onsettends to differentiate the condition from hypertrophicpyloric stenosis, in addition to the fact that the childwith hiatus hernia frequently vomits early during afeed when taking the first few mouthfuls, and thatposture influences the vomiting which often occursthe moment the child is laid down after a feed. Itmust be remembered that congenital pyloric stenosismay occur as an associated condition with congeni-tal hiatus hernia.The nature of the vomitus is also of some impor-
tance: it consists of mucus or gastric content un-
stained by bile but frequently containing somealtered blood.
Failure to thriveThe vomiting in the neonatal period before treat-
ment may be severe enough to cause considerabledehydration in addition to preventing weight gain.Most children in fact are already underweight whenthey present and show some degree of malnutrition.
AnaemiaAnaemia is a common finding especially in those
patients with oesophagitis. Although the daily lossof blood may be very slight and even though occultblood is not always demonstrable in the stool it islikely that this very small but persistent loss, as inthe child losing a little blood from colostomy dress-ings daily, is sufficient to account for the presence ofanaemia, and that the malnutrition does not playsuch an important part. The poor correlation be-tween the severity of oesophagitis and the degree ofanaemia has led some workers to suggest an ironabsorption deficiency (Michaelides & Philis, 1959).Frank haematemesis is rare and practically con-
fined to those cases with para-oesophageal rollinghernias.
DysphagiaDysphagia again is an uncommon symptom unless
the child with a sliding hiatus hernia has developedoesophagitis. Occasionally a baby is seen to cry onfeeding suggesting the presence of dysphagia. In therolling hernia, dysphagia would be more commonlyexpected because of the pressure of the herniatedfundus of the stomach on the lower oesophagus andindeed this does occur in some older children withthe rolling type of hernia; in the neonate, however,the child with the rolling type of hernia still tends topresent with vomiting.
Progress of the diseaseThere is a strong tendency for the condition to
subside by the time the child reaches a year of ageand in fact the mother commonly will note that, firstwhen the child sits up for more of the time duringthe day, and later when he starts to walk there is anoticeable decrease in the frequency of the vomiting.The time when he sits up is also related to the timewhen he takes more solid foods. Although vomitusmay often be found on the pillow at the end of anight's sleep, the child gradually vomits much lessduring the day. Waterston (1969) rightly warns ofthe danger of too much optimism when dailyvomitus changes to episodic attacks which may indi-cate that the child has developed a stricture in hislower oesophagus, not that the hernia is cured.
copyright. on 30 M
arch 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.48.562.501 on 1 A
ugust 1972. Dow
nloaded from
504 James Lister
OesophagitisOesophagitis with its risk of stricture formation
and the tendency to progress to severe fibrosis is themost undesirable complication, and it is importantthat those cases liable to develop severe oesophagitisshould be dealt with surgically before irreversiblefibrotic changes have been allowed to occur: per-sistent blood-staining of the vomit and dysphagiaare warning signs as are the episodic severe attacksmentioned above.
Respiratory infectionsRecurrent aspiration pneumonia is a well recog-
nized complication and is especially important inthe children with mental retardation who form anappreciable number of most series of hiatus hernias(Moncrieff & Wilkinson, 1954). In addition to this,both in those children who have been operated onand those who have been treated conservatively,there is a notable tendency for the child to have anepisode of vomiting for several days whenever he hasupper respiratory infection.
ManagementThere is no doubt that a considerable number of
children with gastro-oesophageal reflux settle withconservative methods and are not investigated. If achild is posseting a good deal after feeds it may wellbe that he has gastro-oesophageal reflux but pro-vided none of these possets are blood-stained andthe child's weight-gain is normal then there is littleindication for further investigation, and the motheris encouraged to persist in the simple managementof the child. Investigation is indicated when there isevidence that the child is failing to gain weight orwhen there is some blood-staining of the vomitus.The diagnosis should be suspected in all those
children who present with vomiting in the first weekof life, particularly those who vomit gastric contentsalone and in whom no systemic cause of the vomit-ing has been demonstrated. Confirmation of thediagnosis is achieved by radiographic study after theswallowing of contrast medium, and the type oftreatment is similar whether gastro-oesophageal re-flux alone has been shown or whether a sliding typeof hiatus hernia has been demonstrated. In the firstplace management will be on conservative lines; thechild is nursed in an upright position by day and bynight making use of one of the commercially avail-able plastic baby chairs, and the feeds are thickenedeither by the addition of Benger's food or by the useof Nestargel. Frequent small feeds should be givenand if the child should vomit, either during or atthe end of the feed, he should be given another feedimmediately.The aims of treatment are two-fold-to prevent
loss of nourishment by vomiting and to avoid oeso-
phagitis from the bathing of the lower oesophagusin refluxed acid gastric juice. Medical methods ofavoiding reflux oesophagitis include the use of ant-acids and the more recent introduction of a lowspecific gravity colloidal gel (Gaviscon) designed tofloat on top of the feed in the upper part of thestomach and to form a protective coat adhering tothe lower oesophageal mucosa. Oesophageal ulcera-tion, however, can occur very rapidly with graveconsequences and when there is evidence of oeso-phagitis the possibility of surgical intervention mustbe closely borne in mind.
Surgical interventionIn a review of 3 years in The Children's Hospital,
Sheffield, forty-five cases were referred to the paedia-tric surgical unit. Thirty ofthese children were treatedsuccessfully by medical means, fifteen of them cameto operation.
(a) Rolling hernia. In a rolling hernia the herniatedstomach forms aspace-occupyinglesion inthethoraciccavity. Four of the fifteen cases operated upon fellinto this class and all were symptomatically cured aswell as being shown to be cured radiologically.Three presented under 2 years of age, the fourth wasa child of 8 who developed acute distention of theherniated stomach after trauma and was operatedupon as an emergency. This was the only child whohad an abdominal approach to his lesion, the othershaving been operated upon through the left pleuralcavity, and having had the hernial sac excised andthe oesophageal hiatus narrowed by a few non-absorbable sutures in the right crus posterior to theoesophagus.
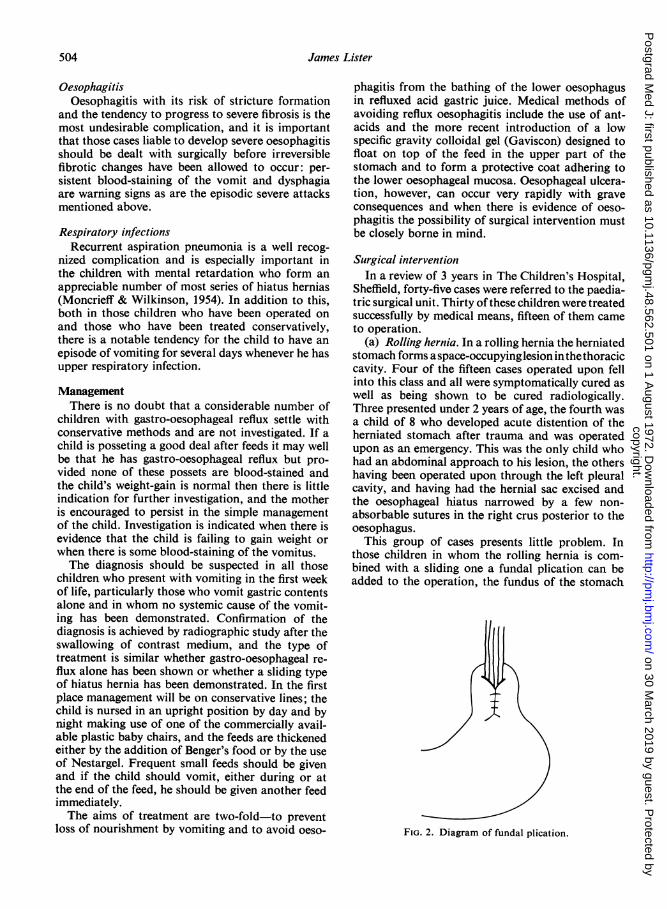
This group of cases presents little problem. Inthose children in whom the rolling hernia is com-bined with a sliding one a fundal plication can beadded to the operation, the fundus of the stomach
FIG. 2. Diagram of fundal plication.
copyright. on 30 M
arch 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.48.562.501 on 1 A
ugust 1972. Dow
nloaded from
Hiatus hernia in children 505
i:··:ini:·:
1:Bi%i·
': .3.··i
·:···:iQ::
i....:..:
,if' ·O·:::i
""' Fldli·.
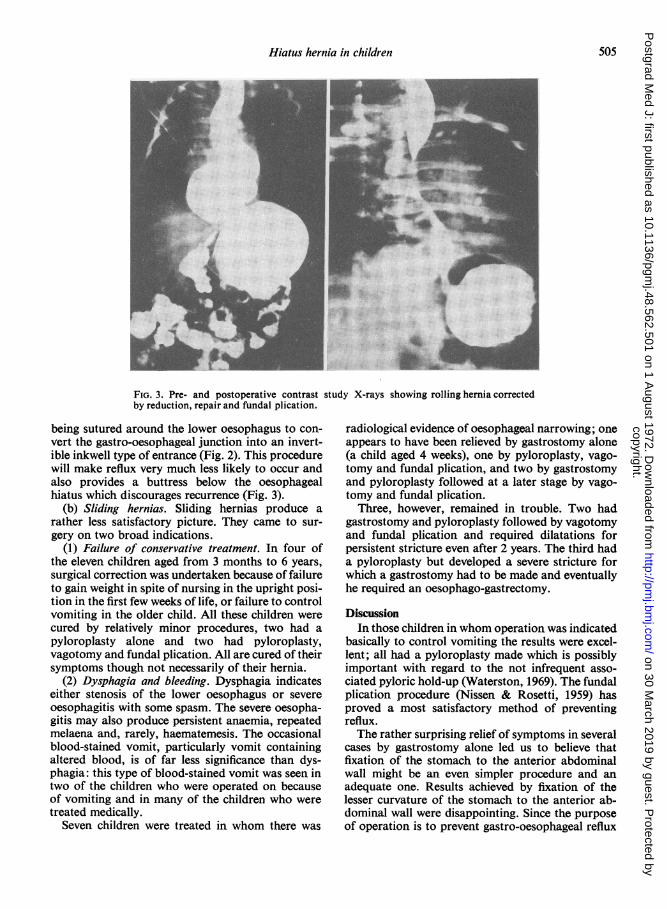
FIG. 3. Pre- and postoperative contrast study X-rays showing rollinghernia correctedby reduction, repair and fundal plication.
being sutured around the lower oesophagus to con-vert the gastro-oesophageal junction into an invert-ible inkwell type of entrance (Fig. 2). This procedurewill make reflux very much less likely to occur andalso provides a buttress below the oesophagealhiatus which discourages recurrence (Fig. 3).
(b) Sliding hernias. Sliding hernias produce arather less satisfactory picture. They came to sur-gery on two broad indications.
(1) Failure of conservative treatment. In four ofthe eleven children aged from 3 months to 6 years,surgical correction was undertaken because of failureto gain weight in spite of nursing in the upright posi-tion in the first few weeks of life, or failure to controlvomiting in the older child. All these children werecured by relatively minor procedures, two had apyloroplasty alone and two had pyloroplasty,vagotomy and fundal plication. All are cured of theirsymptoms though not necessarily of their hernia.
(2) Dysphagia and bleeding. Dysphagia indicateseither stenosis of the lower oesophagus or severeoesophagitis with some spasm. The severe oesopha-gitis may also produce persistent anaemia, repeatedmelaena and, rarely, haematemesis. The occasionalblood-stained vomit, particularly vomit containingaltered blood, is of far less significance than dys-phagia: this type of blood-stained vomit was seen intwo of the children who were operated on becauseof vomiting and in many of the children who weretreated medically.
Seven children were treated in whom there was
radiological evidence of oesophageal narrowing; oneappears to have been relieved by gastrostomy alone(a child aged 4 weeks), one by pyloroplasty, vago-tomy and fundal plication, and two by gastrostomyand pyloroplasty followed at a later stage by vago-tomy and fundal plication.
Three, however, remained in trouble. Two hadgastrostomy and pyloroplasty followed by vagotomyand fundal plication and required dilatations forpersistent stricture even after 2 years. The third hada pyloroplasty but developed a severe stricture forwhich a gastrostomy had to be made and eventuallyhe required an oesophago-gastrectomy.
DiscussionIn those children in whom operation was indicated
basically to control vomiting the results were excel-lent; all had a pyloroplasty made which is possiblyimportant with regard to the not infrequent asso-ciated pyloric hold-up (Waterston, 1969). The fundalplication procedure (Nissen & Rosetti, 1959) hasproved a most satisfactory method of preventingreflux.The rather surprising relief of symptoms in several
cases by gastrostomy alone led us to believe thatfixation of the stomach to the anterior abdominalwall might be an even simpler procedure and anadequate one. Results achieved by fixation of thelesser curvature of the stomach to the anterior ab-dominal wall were disappointing. Since the purposeof operation is to prevent gastro-oesophageal reflux
copyright. on 30 M
arch 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.48.562.501 on 1 A
ugust 1972. Dow
nloaded from

506 James Lister
then gastropexy must be designed to have its effectby maintaining an abdominal oesophagus and thuspreserving the exposure of lower oesophagus to thepinchcock action of the right crus and to the positiveintra-abdominal pressure: Woodward, Rayl &Clarke (1970) point out that both these mechanismsare weak elements of the natural sphincteric mech-anism and a high incidence of long-term recurrencewould be expected.
In our series in Sheffield, 20°/ of those operatedon remained in serious trouble from strictures. Onehad already required interposition of colon betweenthe oesophagus and the stomach, and it seems likelythat the other two will also require this procedure.The poor results are in those children in whom severestricture of the lower oesophagus has occurred. Agreat deal of work has been done on the varyingresponse of the oesophageal mucosa to gastric con-tents (Collis, 1970) but it is not clear why oesopha-gitis can be so severe in some cases and so mild inothers. Hyperacidity is not essential but acid ishighly important in the production of this oesopha-gitis and one might therefore suggest that an anti-reflux procedure should be carried out in all cases.This, however, would mean that in approximatelytwo-thirds of children an unnecessary operationwould have been carried out, since thirty out of ourforty-five cases were successfully treated conserva-tively. Nevertheless, it would seem necessary thatsurgical intervention should be considered earlierin some cases than it has been in the past. It isdifficult also to ignore the fact that a number ofchildren who have developed severe strictures havein fact been shown to be high acid secretors (Lari,Lister & Duthie, 1968). It would seem justifiable inthese cases not only to recommend fairly early opera-tion, but also to include vagotomy in the surgicalprocedure. Ideally, then, an antireflux procedure ofa simple nature as provided by the operation offundal plication (Nissen) should be carried out in allthose cases in whom there is evidence of persistentoesophagitis and selective vagotomy should beadded if there is also evidence of high acid secretion.
In those cases in which some narrowing of thelower oesophagus has already occurred it is impor-tant to recognize whether that narrowing is reversibleor not. Temporary gastrostomy plays a part in thisdifferentiation. On more than one occasion whendealing with a child who had dysphagia, vomitingand malnutrition, we have made a gastrostomy essen-tially for feeding to improve the child's generalcondition before major operation; we have then
found that within a few days the child began to swal-low normally demonstrating that the narrowing ofthe oesophagus was due more to spasm than tofibrotic stricture. This effect may have been due toneutralization of the gastric contents by frequentgastrostomy feeds, to resting the oesophagus, or tofixing the stomach to the anterior abdominal wall,but whatever the mechanism a rapid relaxation ofthe narrowed lower oesophagus would encouragea less radical surgical procedure to be undertaken,and failure of such a response is a good indicationfor proceding to oesophageal resection. Colonicinterposition between the oesophagus and thestomach, whilst being a major procedure, is probablypreferable to the years of dilatation that may berequired to overcome the repeated recurrence ofsevere strictures.
ReferencesALLISON, P.R. (1951) Reflux oesophagitis sliding hiatal
hernia and the anatomy of repair. Surgery, Gynecology andObstetrics, 92, 419.
ALLISON, P.R. (1970) Peptic oesophagitis and oesophagealstricture. Lancet, ii, 199.
CARRE, I.J. (1959) Natural history of the partial thoracicstomach. Archives of Disease in Childhood, 34, 344.
CARRE, IJ. (1970) Further on hiatus hernia. Pediatrics, 45,341.
COLLIS, J.L. (1970) The causes of the variable response togastric reflux in hiatus hernia. Journal of the Royal Collegeof Surgeons of Edinburgh, 15, 77.
LARI, J., LISTER, J. & DUTHIE, (1968) Response to gastrinpentapeptide in children. Journal of Pediatric Surgery, 3,682.
MICHAELIDES, G. J. & PHILIS, H.C. (1959) Pathogenesis andtreatment of the anaemia associated with hiatus hernia.Lancet, i, 552.
MONCRIEFF, A. & WILKINSON, R.H. (1954) Sucrosuria withmental defect and hiatus hernia. Acta Paediatrica, 43,Suppl. 100, 495.
NEUHAUSER, E.B.D. & BERENBURG, W. (1947) Cardio-oesophageal relaxation as a cause of vomiting in infants.Radiology, 48, 480.
NISSEN, R. & ROSETTI, M. (1959) Die Behandlung von HiatusHernian und Reflux Oesophagitis mit Gastropexie undFundoplicatio. Georg Thieme Verlag, Stuttgart.
SHATZ, B. & BAUE, A.E. (1970) Medical and surgical aspectsof hiatus hernia. Journal of the American Medical Associa-tion, 214, 125.
SKINNER, D.B. & BELSEY, R.H.R. (1967) Surgical managementof oesophageal reflux and hiatus hernia: long-term resultswith 1030 patients. Journal of Thoracic and CardiacSurgery, 53, 33.
WATERSTON, D.J. (1969) Pediatric Surgery (Ed. by Mustard,W.T., RAVITCH, M.M., SNYDER, W.H. (JR.), WELCH, K.J.& BENSON, C.D., Vol. 1. Year Book Medical Publishers,Chicago.
WOODWARD, E.R., RAYL, J.E. & CLARKE, J.M. (1970) Eso-phageal hiatus hernia. In: Current Problems in Surgery.Year Book Medical Publishers, Chicago.
copyright. on 30 M
arch 2019 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.48.562.501 on 1 A
ugust 1972. Dow
nloaded from