hemodynamics 1
TRANSCRIPT
HEMODYNAMIC DISORDERS(OEDEMA)-
PART-IDr. Babai Halder
Asst. Professor(Pathology)
Overview• HEMODYNAMIC deals with the circulation of the blood/ the
forces or mechanisms involved in circulation.• Hemodynamic Disorders-• Edema (increased fluid in the ECF)• Hyperemia (INCREASED flow)
• Congestion (INCREASED backup)
• Hemorrhage (extravasation)• Thromboembolic Disease-• Thrombosis (clotting blood)• Embolism (downstream travel of a clot)
• Infarction (death of tissues w/o blood or ischemia)
• Shock-
• Shock (circulatory failure/collapse)
HOMEOSTASIS
• The mechanism by which the constancy of the internal environment is maintained and ensured is called the homeostasis.
• Claude Bernarde (1949) – internal environment or milieu interieur
• Internal envt – water and electrolytes
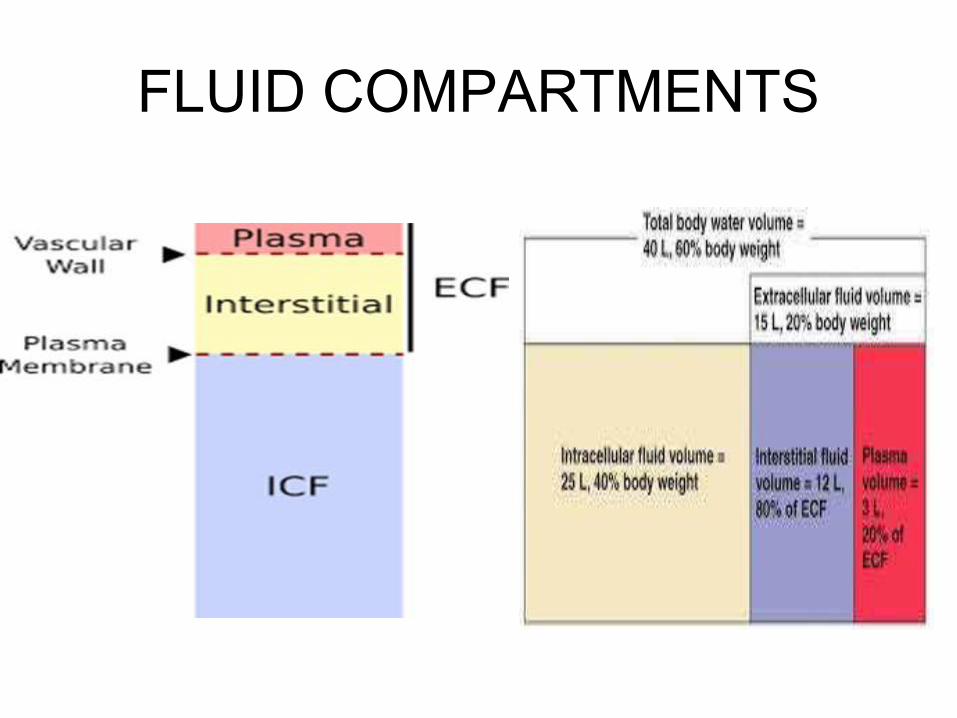
FLUID COMPARTMENTS
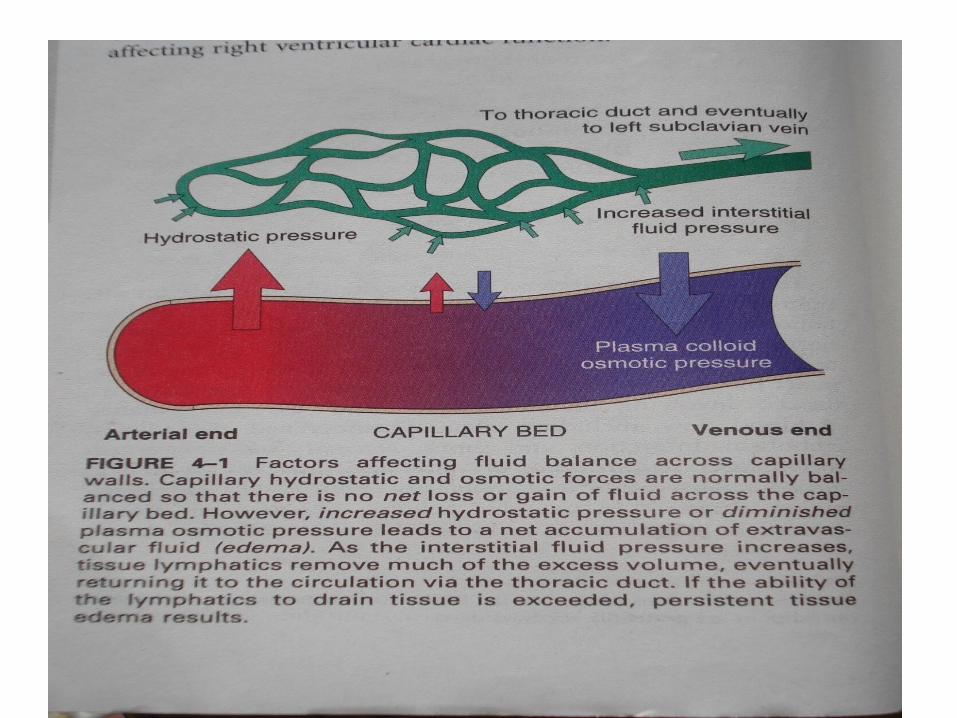
• STERLING’S FORCES• HYDROSTATIC PRESSURE - capillary blood pressure -
drives fluid through the capillary wall into the interstitial space.
• COLLOID OSMOTIC PRESSURE - exerted by proteins present in the ECF - tends to draw fluid into the vessels.
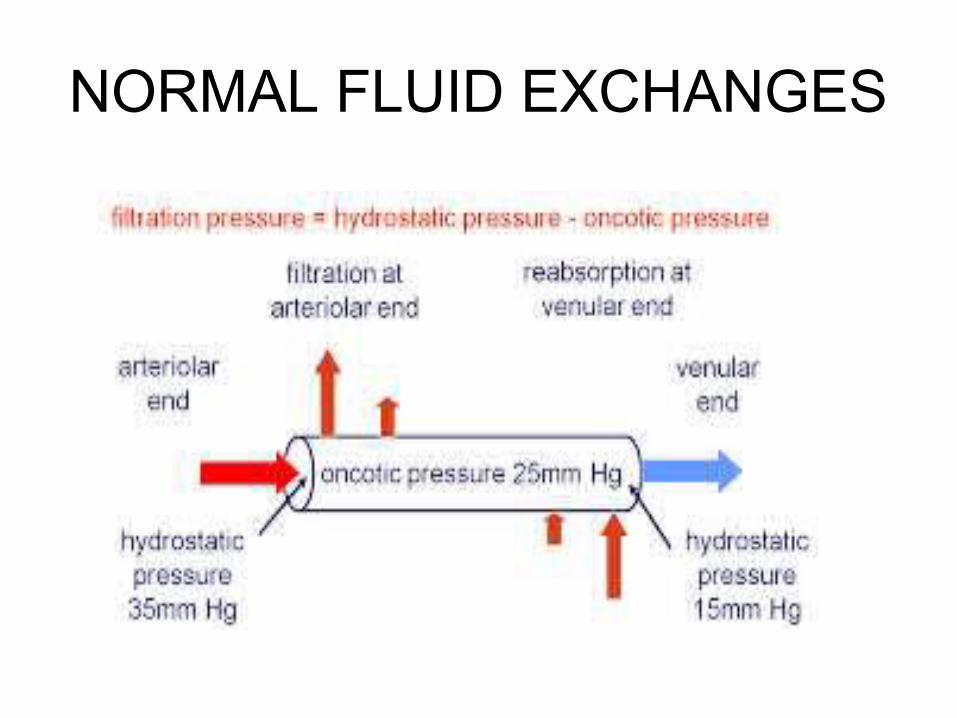
NORMAL FLUID EXCHANGES
OEDEMA- DEFINITION
The greek word ‘oidema’ means swelling. Edema is defined as abnormal and excessive accumulation of “free fluid” in the interstitial tissue spaces and serous cavities.
-Edema occurs in both extracellular and intracellular fluid compartment (mainly in the ECF)
-Depending on its cause and mechanism,edema may be localized or have a generalized distribution-Depending on the composition of fluid: transudate & exudate oedema
PATHOPHYSIOLOGICAL CATEGORIES OF EDEMA A) ↑ed hydroststic pressure : • Impaired venous return : CHF Constrictive pericatditis Ascites (liver cirrhosis) Venous obstruction or compression(thrombosis, external pressure etc.) •Arteriolar dilation : Heat Neurohumoral dysregulation B) ↓ed plasma osmotic pressure( hypoproteinemia): •protein-losing glomerulopathies( nephrotic syndrome) • liver cirrhosis (ascites) • malnutrition •protein-losing gastroenteropathy
C)Lymphatic obstruction •Inflammatory •Neoplastic •Postsurgical •PostirradiationD)Sodium retention •Excessive salt intake with renal insufficiency •↑ed tubular reabsorption of sodium •Renal hypoperfusion •↑ed renin-angiotensin-aldosterone secretionE)Inflammation •Acute inflammation •Chronic inflammation
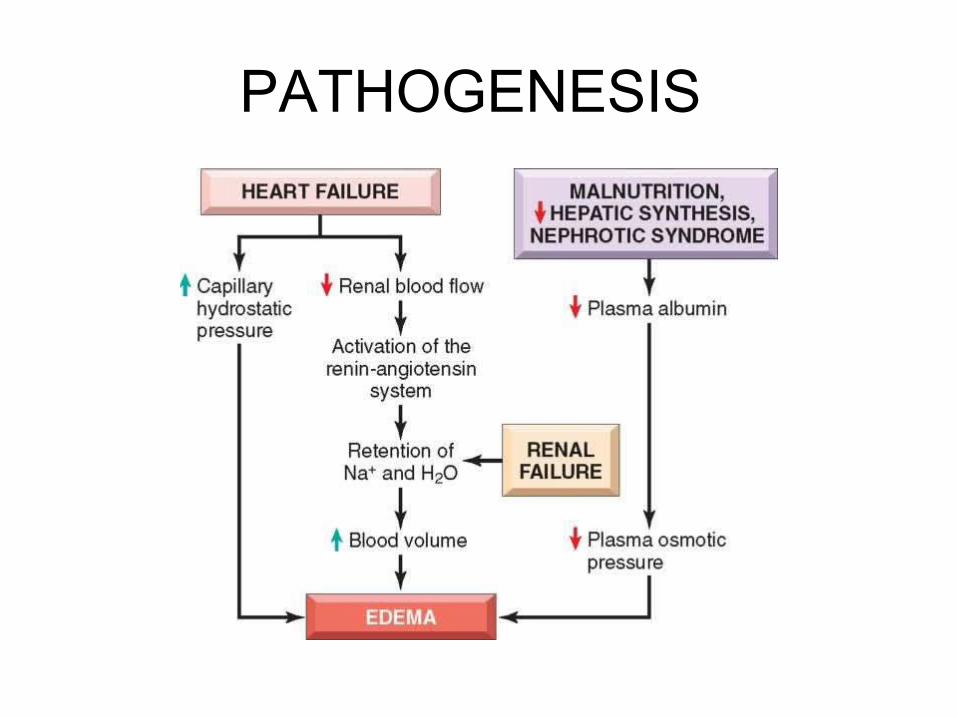
PATHOGENESIS:-
• The following mechanisms may be operating singly or in
combination to produce oedema:
1. Decreased plasma oncotic pressure
2. Increased capillary hydrostatic pressure
3. Lymphatic obstruction
4. Tissue factors (increased oncotic pressure of interstitial
fluid, and decreased tissue tension)
5. Increased capillary permeability
6. Sodium and water retention.
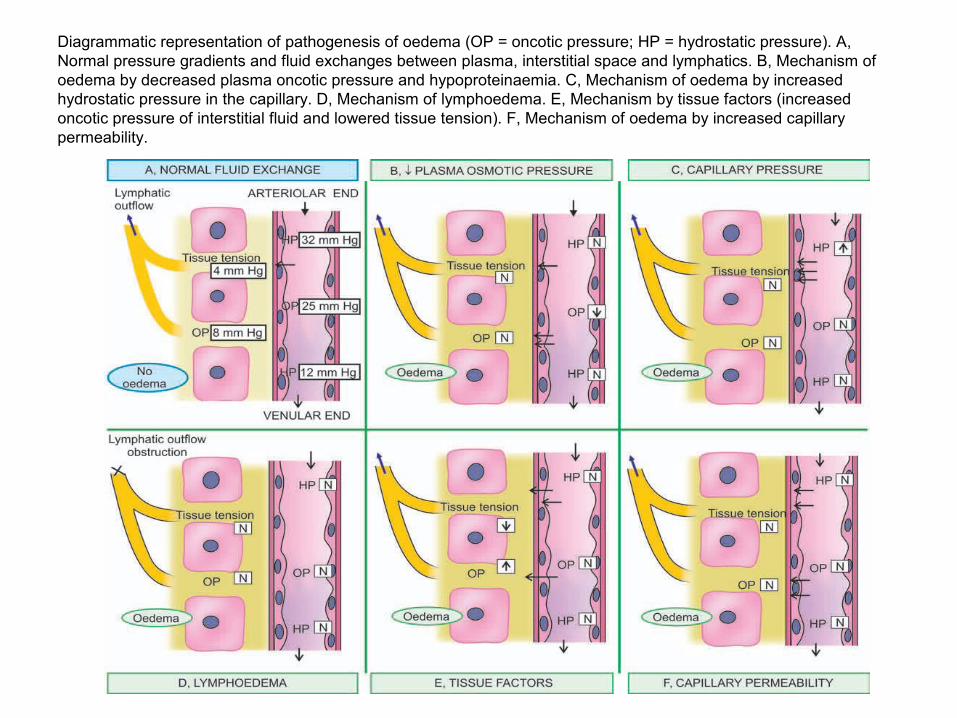
Diagrammatic representation of pathogenesis of oedema (OP = oncotic pressure; HP = hydrostatic pressure). A, Normal pressure gradients and fluid exchanges between plasma, interstitial space and lymphatics. B, Mechanism of oedema by decreased plasma oncotic pressure and hypoproteinaemia. C, Mechanism of oedema by increased hydrostatic pressure in the capillary. D, Mechanism of lymphoedema. E, Mechanism by tissue factors (increased oncotic pressure of interstitial fluid and lowered tissue tension). F, Mechanism of oedema by increased capillary permeability.
1) STERLING FORCES :- ↑ed hydrostatic pressure and ↓ed colloidal oncotic pressure of vascular system movement of fluid from the vascular to the extravascular space
•↑ed hydrostatic pressure – seen in obstruction in venous drainage. It may be generalized,e.g., CHF.•↓ed colloidal osmotic pressure of plasma– seen in cases that induce hypoproteinemia,e.g., nephrotic syndrome, malnutrition.
2)LYMPHATIC OBSTRUCTION:- impaired lymphatic drainage impaired fluid return from interstitial space into vascular compartment lymphedema
It can result from inflammatory,neoplastic,postsurgical, post-irradiation, obstruction of lymphatics ,e.g., filariasis (elephantiasis), carcinoma of the breast(peau d’orange)
3) SODIUM AND WATER RETENTION:- ↓ed effective arterial volume(as seen in heart
failure, nephrotic syndrome,cirrhosis etc.) renal efferent arteriolar constriction and an elevation of filtration fraction ↓ed hydrostatic and ↑ed colloidal osmotic pressure of peritubular capillaries ↑ed tubular reabsorption (proximal tubule and ascending limb of loop of Henle)Na + H2O ↑ ed plasma volume edema
4) RENIN—ANGIOTENSIN—ALDOSTERONE (RAA) SYSTEM In conditions associated with diminished renal blood flow there is release of renin by the renal juxtaglomerular cell.
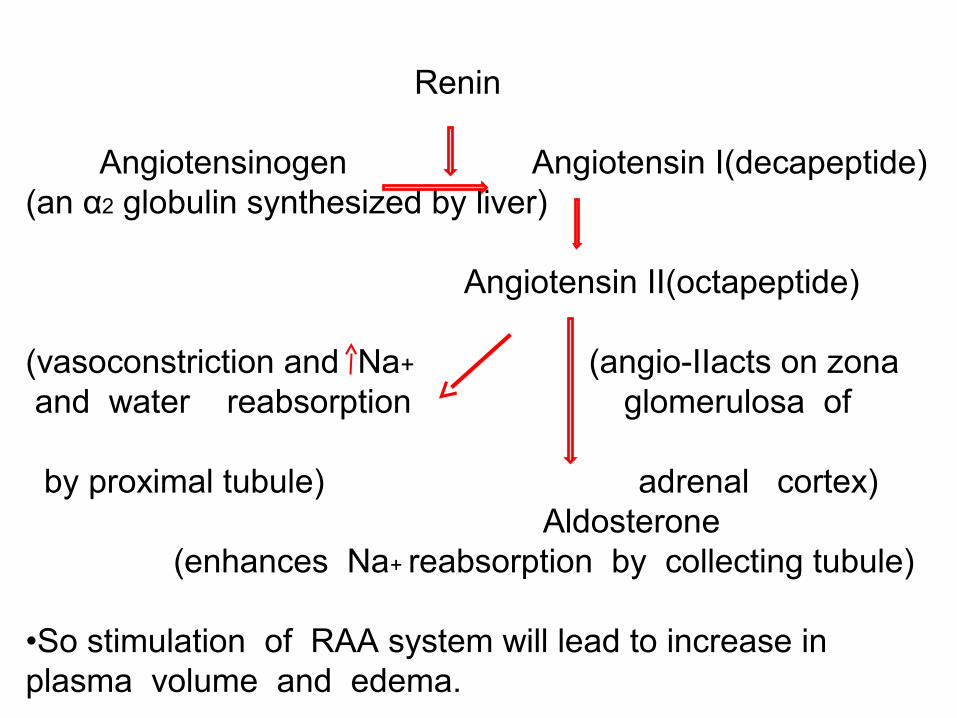
Renin Angiotensinogen Angiotensin I(decapeptide)(an α2 globulin synthesized by liver)
Angiotensin II(octapeptide) (vasoconstriction and Na+ (angio-IIacts on zona and water reabsorption glomerulosa of by proximal tubule) adrenal cortex) Aldosterone (enhances Na+ reabsorption by collecting tubule) •So stimulation of RAA system will lead to increase in plasma volume and edema.
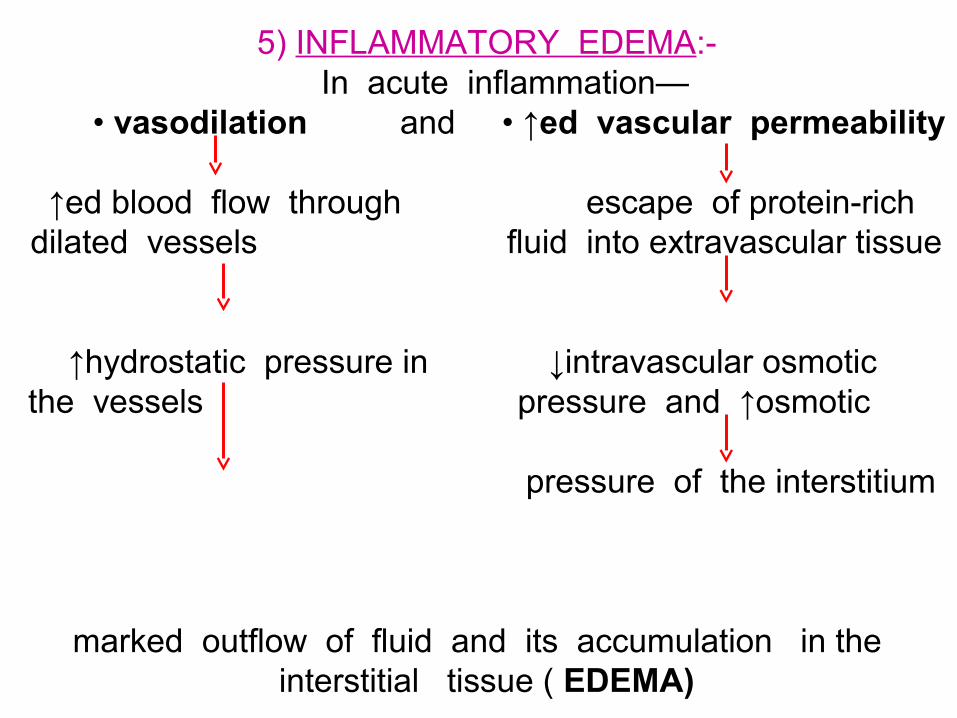
5) INFLAMMATORY EDEMA:- In acute inflammation—
• vasodilation and • ↑ed vascular permeability ↑ed blood flow through escape of protein-rich
dilated vessels fluid into extravascular tissue
↑hydrostatic pressure in ↓intravascular osmotic the vessels pressure and ↑osmotic
pressure of the interstitium
marked outflow of fluid and its accumulation in the interstitial tissue ( EDEMA)
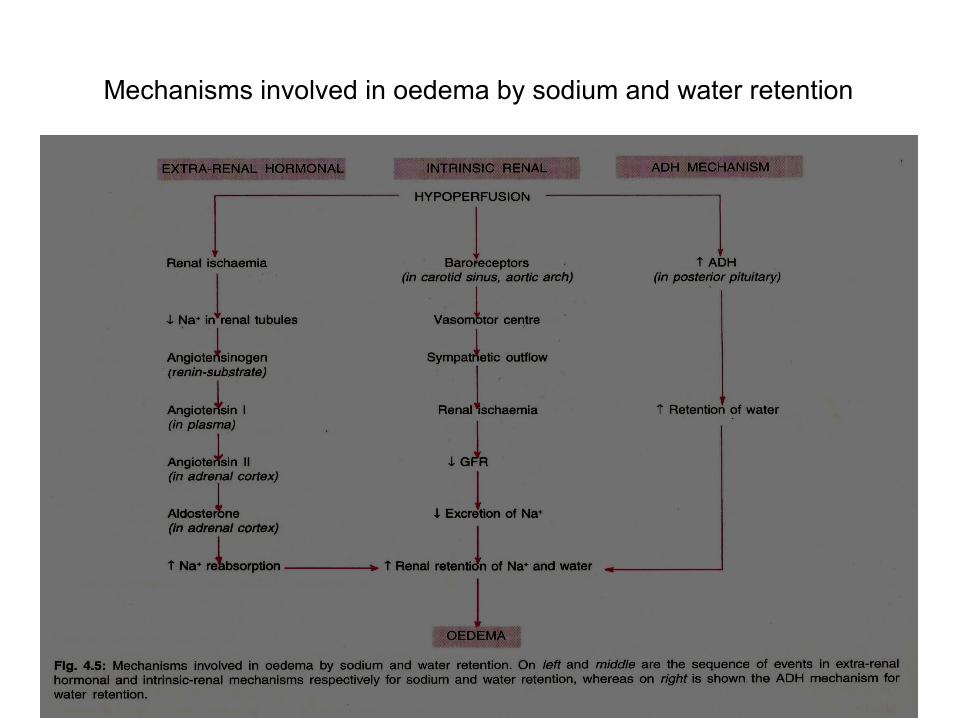
Mechanisms involved in oedema by sodium and water retention
PATHOGENESIS
ACCORDING TO THE DISTRIBUTION ,EDEMA CAN BE GENERALIZED OR LOCALIZED.•Localized edema : causes: a) Venous obstruction : pregnancy, SVCsyndrome, IVC syndrome, varicose veins in
legs, prolonged recumbency,
venous thrombosis etc.
b) Lymphatic obstruction: filariasis, Ca breast, following radical
mastectomy etc.
Localized edema contd…..
c)allergic causes : angioneurotic edema, acute anaphylaxis d)inflammatory : insect bite, snake bite, trauma,ischaemia or
infection e) miscellaneous : bruises, sprains, fracture, gout etc.
•Generalized edema : it is known as anasarca. e .g ., Heart diseases like CHF,
pericardial effusion, constrictive pericarditis.
Cirrhosis of liver, Nephrotic syndrome, Malnutrition, Drugs like nifedipine,
corticosteroids,NSAIDs etc.
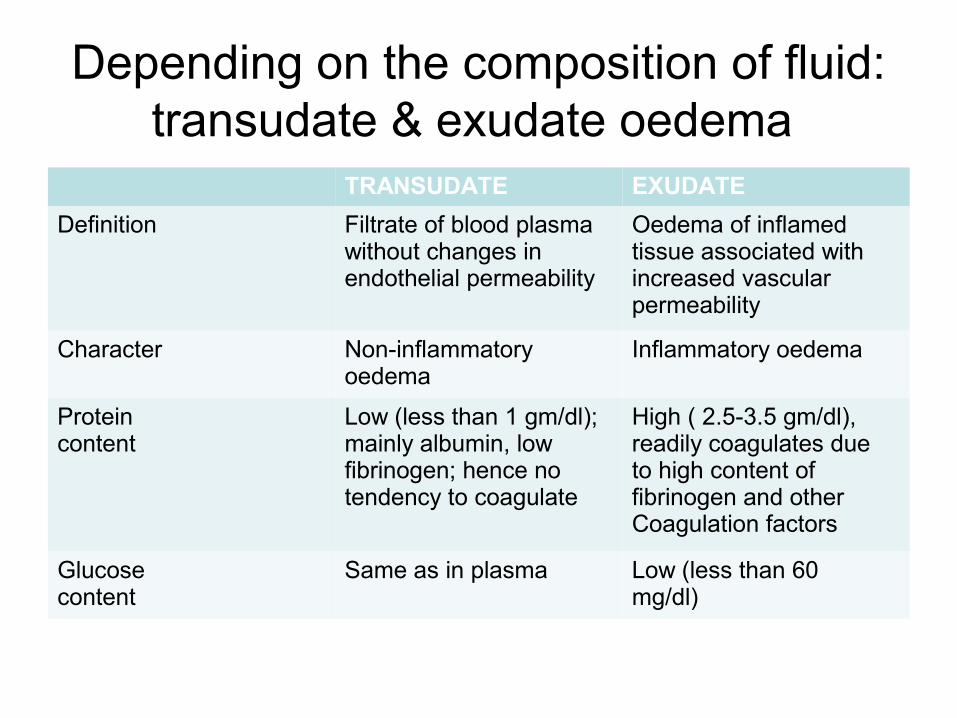
Depending on the composition of fluid: transudate & exudate oedema
TRANSUDATE EXUDATE
Definition Filtrate of blood plasmawithout changes in endothelial permeability
Oedema of inflamedtissue associated withincreased vascularpermeability
Character Non-inflammatory oedema
Inflammatory oedema
Proteincontent
Low (less than 1 gm/dl);mainly albumin, lowfibrinogen; hence no tendency to coagulate
High ( 2.5-3.5 gm/dl),readily coagulates dueto high content offibrinogen and otherCoagulation factors
Glucosecontent
Same as in plasma Low (less than 60mg/dl)
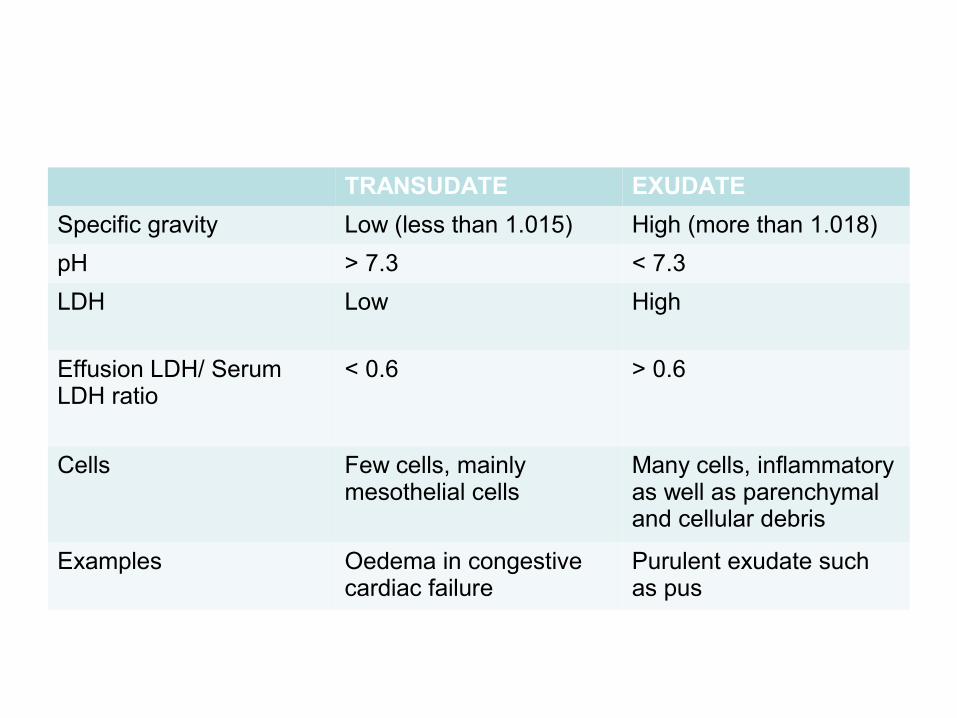
TRANSUDATE EXUDATE
Specific gravity Low (less than 1.015) High (more than 1.018)
pH > 7.3 < 7.3
LDH Low High
Effusion LDH/ SerumLDH ratio
< 0.6 > 0.6
Cells Few cells, mainlymesothelial cells
Many cells, inflammatoryas well as parenchymaland cellular debris
Examples Oedema in congestivecardiac failure
Purulent exudate such as pus
SPECIAL FORMS
RENAL OEDEMA
• Generalised oedema occurs in certain diseases of renal origin- such as in nephrotic syndrome, some types of glomerulonephritis, and in renal failure due to acute tubular injury.
• Initially manifests in tissues with loose connective tissue matrix – eyelids
• Periorbital edema - characteristic
Types• OEDEMA IN NEPHROTIC SYNDROME- Since there is persistent
and heavy proteinuria (albuminuria) in nephrotic syndrome,there is hypoalbuminaemia causing decreased plasma oncotic pressure resulting in severe generalised oedema(nephrotic oedema). The hypoalbuminaemia causes fall in the plasma volume activating renin-angiotensin-aldosterone mechanism which results in retention of sodium and water.
• The nephrotic oedema is classically more severe and marked and is present in the subcutaneous tissues as well as in the visceral organs. The affected organ is enlarged and heavy with tense capsule.
• Microscopically, the oedema fluid separates the connective tissue fibres of subcutaneous tissues. Depending upon the protein content, the oedema fluid may appear homogeneous, pale, eosinophilic, or may be deeply eosinophilic and granular.
• OEDEMA IN NEPHRITIC SYNDROME- In contrast to nephrotic oedema, nephritic oedema is not due to hypoproteinaemia but is largely due to excessive reabsorption of sodium and water in the renal tubules via renin-angiotensin-aldosterone mechanism. The protein content of oedema fluid in glomerulonephritis is quite low (less than 0.5 g/dl).
• The nephritic oedema is usually mild as compared to nephrotic oedema and begins in the loose tissues such as on the face around eyes, ankles and genitalia. Oedema in these conditions is usually not affected by gravity.
• OEDEMA IN ACUTE TUBULAR INJURY- damaged tubules lose their capacity for selective reabsorption and concentration of the glomerular filtrate resulting in increased reabsorption.
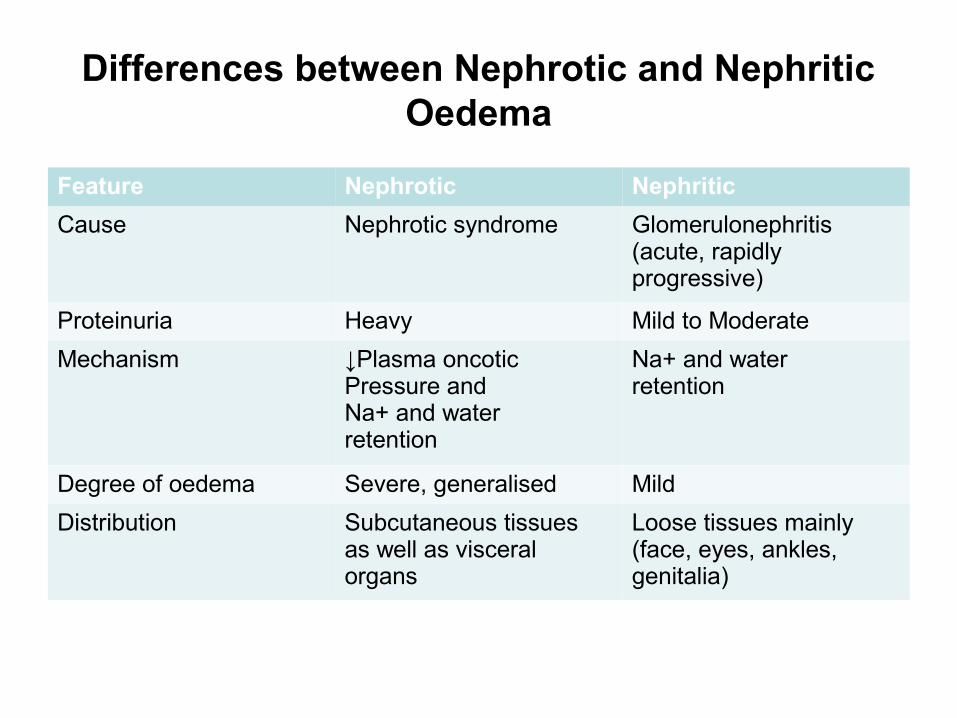
Differences between Nephrotic and Nephritic Oedema
Feature Nephrotic Nephritic
Cause Nephrotic syndrome Glomerulonephritis(acute, rapidlyprogressive)
Proteinuria Heavy Mild to Moderate
Mechanism ↓Plasma oncoticPressure andNa+ and waterretention
Na+ and waterretention
Degree of oedema Severe, generalised Mild
Distribution Subcutaneous tissuesas well as visceralorgans
Loose tissues mainly(face, eyes, ankles,genitalia)
PULMONARY OEDEMA
• CAUSES - left ventricular failure, renal failure, acute respiratory distress syndrome and pulmonary inflammation or infection
• CONSEQUENCES - impede oxygen diffusion- hypoxia – hypercapnia -favorable environment – bacterial infection
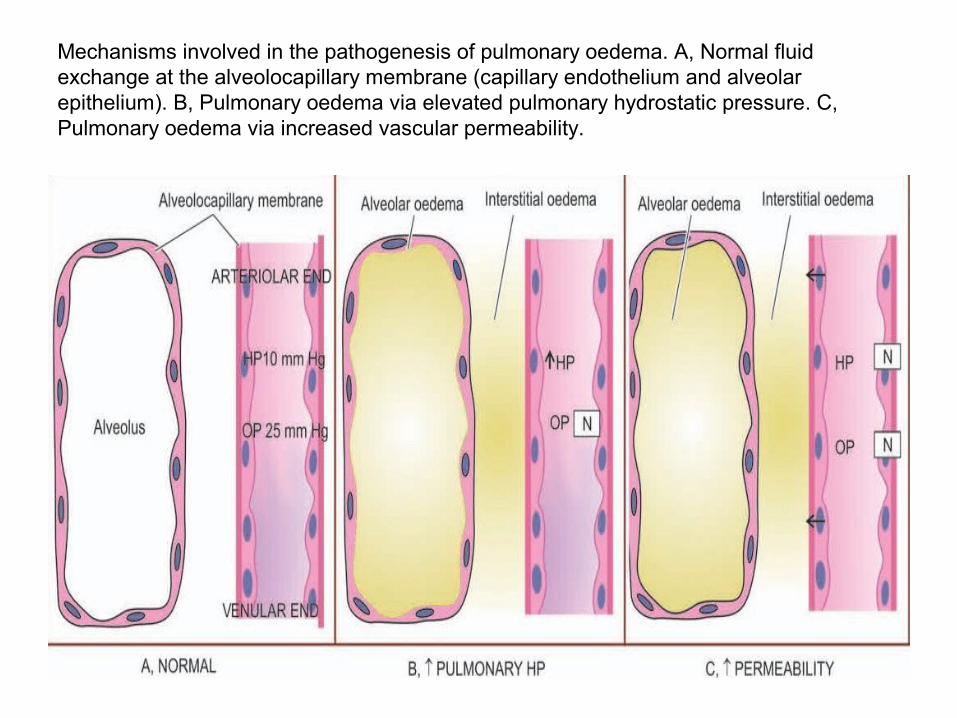
Mechanisms involved in the pathogenesis of pulmonary oedema. A, Normal fluid exchange at the alveolocapillary membrane (capillary endothelium and alveolar epithelium). B, Pulmonary oedema via elevated pulmonary hydrostatic pressure. C, Pulmonary oedema via increased vascular permeability.
HAPE
• After an altitude of 2500 metres• Without halt or waiting for acclimatisation to set
in• Appearance of oedema fluid -lungs,
congestion – widespread minute haemorrhages• Gross- the lungs are heavy,moist and
subcrepitant.• Cut surface exudes frothy fluid (mixture of air
and fluid).
• M/E: Interstitial oedema -alveolar oedema
• Congestion –alveolar capillaries
• Alveoli filled with a homogeneous,pink-staining fluid permeated by air bubbles

The alveolar capillaries are congested. The alveolar spaces as well as interstitium contain eosinophilic, granular, homogeneous and pink proteinaceous oedema fluid alongwith some RBCs and inflammatory cells.
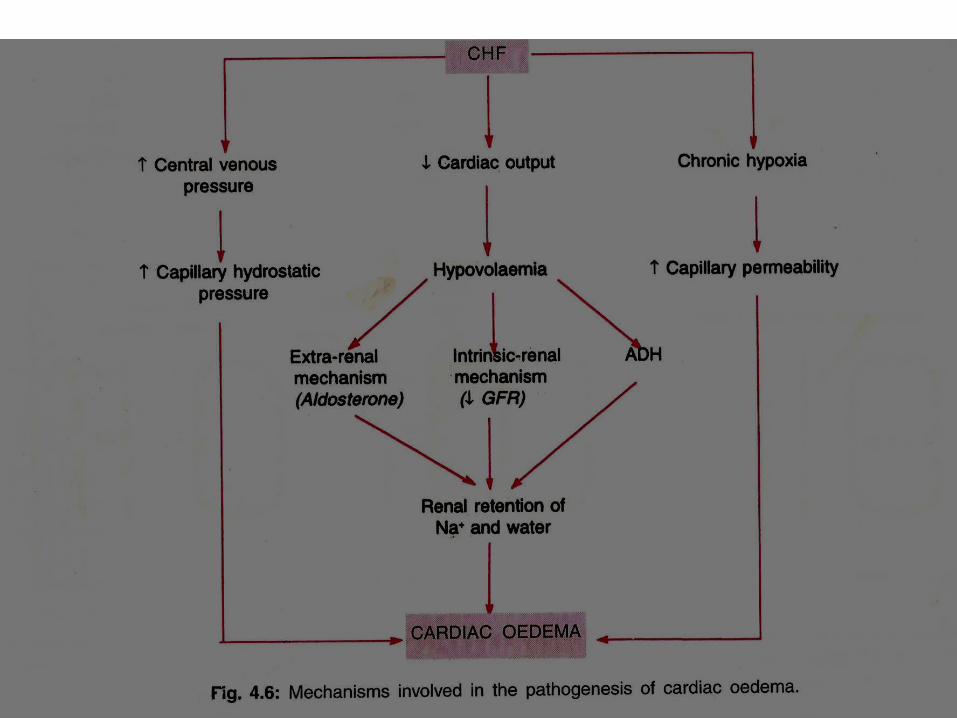
CHF EDEMA• INCREASED VENOUS PRESSURE
DUE TO FAILURE
• DECREASED RENAL PERFUSION, triggering of RENIN-ANGIOTENSION-ALDOSTERONE complex, resulting ultimately in SODIUM RETENTION
HEPATIC OEDEMA• i) Hypoproteinaemia - impaired synthesis of proteins• ii) Portal hypertension - increased venous pressure in
the abdomen - raised hydrostatic pressure.• iii) Failure of inactivation of aldosterone
-hyperaldosteronism.
• iv) Secondary stimulation of RAAS- sodium and water retention.
CEREBRAL OEDEMA
• Brain edema -localized or generalized - nature extent -pathologic process or injury. 3 types-
• VASOGENIC OEDEMA : increased filtration pressure or increased capillary permeability
• CYTOTOXIC OEDEMA : disturbance in the cellular osmoregulation – response to cell injury
• INTERSTITIAL OEDEMA : hydrocephalus
MISCELLANEOUS
• Nutritional Oedema-• Due to nutritional deficiency of Proteins (Kwashiorkor, prolonged
starvation, famine, fasting), Vitamins (beri-beri due to vitamin B1 deficiency) and Chronic alcoholism
• Main contributing factors- Hypoproteinaemia & Sodium-water retention
• Myxoedema-• Hypothyroidism –non pitting oedema occuring on skin of face and
internal organs due to excessive deposition of glycosaminoglycans in the interstitium
• Microscopically –basophilic mucopolysaccharides.

THANK YOU