hemodialysis adequacy: a complex and evolving … · hemodialysis adequacy: a complex and evolving...
TRANSCRIPT

Hemodialysis Adequacy:A Complex and Evolving
Paradigm
Balazs Szamosfalvi, MDMonday, 08/30/2010 09:00-09:45

Adequacy 1943 - 1970
©Fresenius ©Fresenius
• The patient survived the dialysis session
• Uremia improved
• Volume status improved
• Patient survival to recovery of kidney function or transplant
Source: http://www.homedialysis.org/learn/museum/

Adequacy 1970 - 2000
©Fresenius ©Fresenius
• Safe dialysis sessions in large numbers
• Good control of uremia
• Focus on small solute (urea) kinetics
• Volumetric ultrafiltration
• Patient survival on dialysis for years
• Large clinical studies and guideline development
Source: http://www.homedialysis.org/learn/museum/

Adequacy 2000 → Into the FutureAdequacy 2000 Adequacy 2000 →→ Into the FutureInto the Future
OUTCOME:Quality of Life & RehabilitationReduced Morbidity & Mortality
Adequacy of Dialysis
Better biocompatibility: Improved membranes and
ultrapure dialysate
Blood volume monitoring for safer ultrafiltration
Reduced clotting and inflammation: Automated
regional citrate anticoagulation
Middle molecule removal: Hemo-diafiltration and internal filtration
Daily and or long (nocturnal) dialysis for BP and Ca x P control
Computer-aided HD design and monitoring (Online clearance)
FOCUS ON COST-CONTROL

HD Adequacy1. The uremic syndrome and uremic toxins
• Uremic toxin removal• Volume homeostasis
2. Kinetic studies of solute movement• Solute flux studies on the dialyzer• Online dialyzer flux measurements and computer modeling• Solute flux studies in the patient• Computer modeling of patient solute fluxes and levels
3. New directions after the HEMO and MPO studies• HEMO and MPO interventions failed to improve outcomes• Quality control: online clearance, computerized data collection• Renewed interest in home dialysis: HD duration, frequency• New technology: internal filtration, bio-feedback systems, citrate
anticoagulation

Uremic toxinsI. Small (< 500 D); water soluble
Surrogate marker urea or sodium (ionic dialysance)
Rapidly produced in intracellular fluid compartment
Large variability in intra-patient kinetics (e.g. phosphate)
II. Middle-molecules (500 – 40,000 D); water solubleΒ2-microglobulin, PTH, some cytokines (IL-6, TNF)
Optimized filter design and convection for removal
Complex intra-patient kinetics (generation, compartments)
III.Small (< 500 D); protein-boundPoorly removed with traditional dialysis
Resin adsorption-based therapies are in development
Vanholder et al:Review on uremic toxins; Kidney International, Vol. 63 (2003), pp. 1934–1943Vanholder et al:A bench to bedside view of uremic toxins; J Am Soc Nephrol 19: 863–870, 2008.European Uremic Toxin Work Group (Eutox; http://EUTox.info)

Examples of Uremic ToxinsExamples of Uremic ToxinsExamples of Uremic Toxins
From Primer On Kidney Diseases, 2nd edition

Solute fluxes on the dialyzer1. Nomenclature
• Clearance and dialysance• Efficiency and flux (membrane area and pore size)• Diffusion and or convection (plus adsorption)
2. Analytical mathematical models and solutions• Concept of K0A and the classic diffusive clearance equation• Limitations of K0A: effect of internal filtration and shunting• Bio-fouling: albumin coating, progressive blood clotting
3. Computer models and online measurements• More precise modeling of mathematically complex treatments• Online, multiple measurements of delivered ionic dialysance
(precise surrogate for effective urea clearance)
Depner T and Garred L: Solute transport mechanisms in dialysis; in Replacement of Renal Function by Dialysis, 5th edition; p73-93

Nomenclature1. Dialysance and Clearance
• The volume of blood cleared from the concentration difference ofa solute between the fresh blood and the fresh dialysis fluid entering the filter
• Clearance: special case of dialysance when the fresh dialysate solute concentration is zero
2. Efficiency and Flux• Efficiency: ability to achieve large small solute clearance with
high blood flows (all filters are high efficiency these days)• Flux: ability to achieve high middle molecule clearance and
ultrafiltration rate (determined by the average pore size)
3. Diffusion and Convection• Diffusion: solutes move by diffusion between blocks of fluid
separated by the membrane• Convection: solutes move en mass with a block of fluid across
the membrane (more effective for moving large molecules)

Membrane Flux and Pore Size (1)Membrane Flux and Pore Size (1)
Sivasankaran Ambalavanan, Gary Rabetoy & Alfred K. Cheung; www.kidneyatlas.org

Membrane Flux and Pore Size (2)Membrane Flux and Pore Size (2)
A: Ronco et al: Does nanotechnology apply to dialysis? Blood Purif 2001;19:347–352B: Copyright Gambro Lundia; www.gambro.com
A
B

Membrane Flux and Pore Size (3)Membrane Flux and Pore Size (3)Membrane Flux and Pore Size (3)
A: Ronco et al: Does nanotechnology apply to dialysis? Blood Purif 2001;19:347–352
A
B

Mechanisms of Solute Removal in Mechanisms of Solute Removal in Different Blood Purification TechniquesDifferent Blood Purification Techniques
Ronco et al: Continuous renal replacement techniques; in Replacement of Renal Function by Dialysis, 5th edition; p700
ConvectionDiffusion

Diffusion and ConvectionDiffusion and Convection
From Cheung: Hemodialysis and Hemofiltration; in Primer On Kidney Diseases, 4th edition; p465
Replacement Fluid
Dialysate
Blood
Hemofiltration Membrane
Blood
DialyzerMembrane
Blood Compartment
Blood Compartment
Ultrafiltration Compartment
Dialysate Compartment

Clearance as a function of dialysate and effective blood water flow rates and K0A
KD.QB
1
QBQD
eQBQD
QDQB.K0A
eQBQD
QDQB.K0A
K0A = mass transfer area coefficient
Hct = hematocrit in %
QB = effective blood water flow:
QBw = QB[0.72γ(Hct) + 0.93(100 – Hct)]/100
QD = dialysis fluid flow rate
γ = fraction of RBC volume containing the solute

Concept of K0A1.Mathematical construct which predicts filter
clearance with clinically good accuracy• Incorporates solute properties• Incorporates fluid layer resistance to diffusion on both
the blood and dialysate side of the membrane• Incorporates membrane resistance to diffusion
2.Limitations• Bio-fouling and partial clotting changes K0A• KoA may change with blood and dialysate flow
depending on filter geometry (effect of shunting, internal filtration)
• Hemodiafiltration, partially protein-bound solutes require more complex equations

Solute Clearances by K0A: Low Flux FilterSolute Clearances by K0A: Low Flux Filter
Robert W. Hamilton ; www.kidneyatlas.org

Using Clearance and K0A to select Filters 1Using Clearance and K0A to select Filters 1
Product Brochures; Rexeed filter family; Manufacturer Asahi Kasei

Using Clearance and K0A to select Filters 2Using Clearance and K0A to select Filters 2
Product Brochures; Rexeed filter family; Manufacturer Asahi Kasei
The Marketing Trick The Novel Feature
9% 900%
Β2-microglobulin clearance of this 2.5-m2 filter during dialysis (QB 400, QD 800) is as high as achieved in most current hemo-diafiltration protocols

1. Walther et al:Kidney International (2006) 69, 1056–1063.
Downloadable computer models for renal replacement therapy1

1. Walther et al:Kidney International (2006) 69, 1056–1063.
Addis Filter Clearance Calculator1Addis Filter Clearance Calculator1

Heparin Anticoagulation: Scanning Electron Micrograph of Polysulfone Dialyzer MembraneHeparin Anticoagulation: Scanning Electron
Micrograph of Polysulfone Dialyzer Membrane
1a
1b
Hofbauer et al: Effect of anticoagulation on blood membrane interactions during dialysis; Kidney Int, Vol 56 (1999): pp 1578-1583

Dialysis Machine with Online Clearance (Sodium dialysance ≈ urea clearance)
Effluent
Access Catheter
Treatment Data on Machine Display
Display
Internal Balancing Chambers
Dialyzer
Conductivity Sensors

Gotch et al:Mechanisms determining the ratio of conductivity clearance to urea clearance; Kidney International, Vol. 66 (2004), pp. S3–24

Online clearance measurement (1)1.Online measured small solute clearance1
• Automatically measured ionic (Na+) dialysance• Inexpensive, highly reproducible and accurate• Very robust, unlikely to malfunction• Clinically insignificant effect on the patient serum [Na+]• Excellent agreement with measured urea clearance
2.Limitations• Slow acceptance into clinical practice• Has not been implemented for low (< 300 ml/min)
dialysate flow• Does not provide urea generation or nPCR data
1. Gotch et al:Mechanisms determining the ratio of conductivity clearance to urea clearance; Kidney International, Vol. 66 (2004), pp. S3–24

The Nursing Staff Documents the The Nursing Staff Documents the Online Clearance (OLC) Data Online Clearance (OLC) Data
Online Clearance Data
Press1st
Press2nd

The National Cooperative Dialysis Study (NCDS; 1981)
1. Significance• First large (n=160) clinical outcomes study of hemodialysis1
• Urea TAC 100 versus 50 mg/dL• Treatment time = 2.5-3.5 h versus 4.5 – 5.5 h• Good nutrition and lower urea TAC together better• Showed pre-HD BUN cannot assess adequacy alone• Fostered urea kinetic modeling after secondary analysis2
2. Limitations• Excluded diabetics, hypertensives and the elderly• Low power to define optimal spKt/V, missed effect of time
1. Lowrie et al: Effect of the hemodialysis prescription on patient morbidity: Report from the National Cooperative Dialysis Study. N Engl J Med 305:1176–1181, 1981
2. Gotch FA, Sargent JA: A mechanistic analysis of the National Cooperative Dialysis Study (NCDS). Kidney Int 28:526–534, 1985

Patient
Kr
G
V
CK
Single Pool Fixed Volume Model
Mass Balance Equation
VVdtdtdCdC
= G - C ( K + Kr )
DialysisMachine

G
Liver
Dialyzer
Kidneys
V (40 L)
C
KD
KR
Single-Compartment Fixed VolumeSolute Kinetic Model
Single-Compartment Fixed VolumeSolute Kinetic Model
Adapted from Depner T and Garred L: Solute transport mechanisms in dialysis; in Replacement of Renal Function by Dialysis, 5th edition; p85
G - C(KD+KR)d(C)dt
V Eq. 1:
(G ≈ 0)(KR ≈ 0)
CtEq. 2: C0. e
.KD
Vt
-

Fixed Volume, Single PoolSolute Kinetic Equation
C(t) = systemic plasma solute concentration
V0 = volume of solute distribution at start of dialysis
K = kidney residual clearance (KR)
K = Sum of filter (KD) and kidney (KR) urea clearanceduring hemodialysis
t = time from start of modeling
C(t) .C0 1.GKD KR
eKR) t
V(KD .
eKR) t
V(KD .

1. Walther et al:Kidney International (2006) 69, 1056–1063.
Coplon Dialysis Simulator1: Urea levels with 3x/week dialysis

• Online measurement of effective dialyzer small solute clearance and treatment effectiveness measured as Kt/V
• Kt/V= (dialyzer clearance x treatment time )/ patient’s water volume (L) ∼0.45-75 x pt weight (Kg)
Dialyzer Performance MonitorDialyzer Performance MonitorDialyzer Performance Monitor
Enter Kinetic Volume

The HEMO Study (2002)1.Significance
• Large, randomized clinical outcomes study for 3x/week intermittent HD
• Compared eKt/V 1.16±0.08 versus 1.53±0.09
• Compared low-flux versus high-flux dialysis (Kβ2M 3±7 versus 34±11 ml/min)
2.Conclusions1
• “Patients undergoing hemodialysis thrice weekly appear to have no major benefit from a higher dialysis dose than that recommended by current U.S. guidelines or from the use of a high-flux membrane”.
1. Eknoyan et al: Effect Of Dialysis Dose And Membrane Flux In Maintenance Hemodialysis; N Engl J Med 2002;347:2010-9.

The MPO Study (2009)1.Significance
• Large, randomized clinical outcomes trial for 3x/week intermittent HD for incident patients
• Compared low versus high flux filters (Kuf, β2M-sieving coefficient) with equal urea Kt/V
• Stratified patients based on albumin (≥4 g/dL or <4 g/dL
2.Conclusions• “In summary, we did not detect a significant survival benefit
with either high-flux or low-flux membranes in the population overall, but the use of high-flux membranes conferred a significant survival benefit among patients with serum albumin <4 g/dl.”1
• “the results of the MPO Study can be interpreted as a supporting rationale for the use of high-flux dialysis membranes if they are financially affordable.”2
1. Locatelli et al:Effect of Membrane Permeability on Survival of Hemodialysis Patients; J Am SocNephrol 20: 645–654, 2009
2. Cheung et al:J Am Soc Nephrol 20: 462–464, 2009.

Improving BiocompatibilityImproving BiocompatibilityImproving Biocompatibility1. Technology improvements
Novel membranes with biocompatible inner skin
Ultrapure dialysate generation
2. Regional citrate anticoagulation (RCA)Has the potential to eliminate blood clotting 100%
Maintains filter performance in long dialysis
Blocks WBC, PLT and complement activation in the extracorporeal circuit1
Avoids systemic bleeding tendency or true toxicity
1. Gritters M, Grooteman MP, et al: Citrate anticoagulation abolishes degranulation of polymorphonuclear cells and platelets and reduces oxidative stress during hemodialysis. Nephrol Dial Transplant 2006;21(1): 153-9.
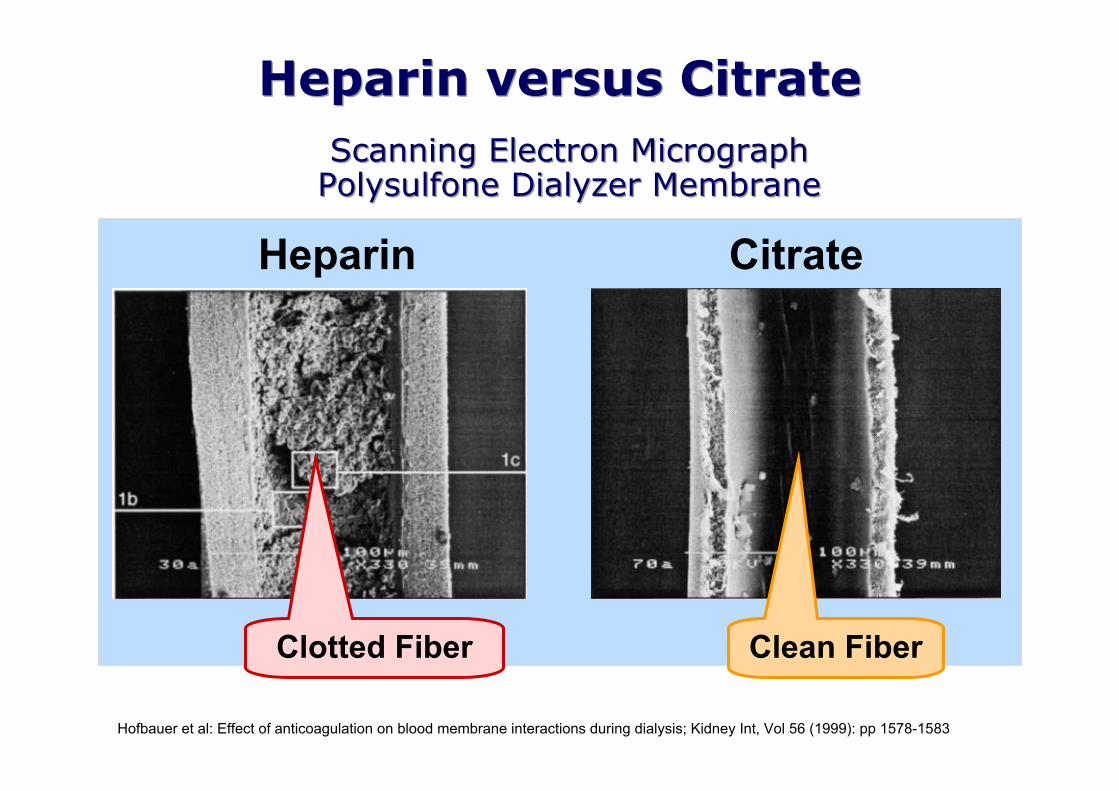
Heparin versus CitrateHeparin versus Citrate
Heparin Citrate
Hofbauer et al: Effect of anticoagulation on blood membrane interactions during dialysis; Kidney Int, Vol 56 (1999): pp 1578-1583
Clean FiberClotted Fiber
Scanning Electron MicrographPolysulfone Dialyzer MembraneScanning Electron Micrograph
Polysulfone Dialyzer Membrane

Online Clearance Measurement (2)Online Clearance Measurement (2)Clinical uses of online ionic dialysance (Kecn)
Continuous, automated HD quality (adequacy) monitoring toolDocument small solute clearance several times, every treatmentDetect partial clotting through decline of KecnMeasure access flow; detect reduced clearance due to access recirculationDetect reverse cannulation of loop graftsAdjust therapy to achieve targeted URR
Gotch et al:Mechanisms determining the ratio of conductivity clearance to urea clearance; Kidney International, Vol. 66 (2004), pp. S3–24

Kecn and or Kt/V below
goal
Confirm “V”value is
appropriate
Check Access Recirculation
Problems fixed; monitor Kecn
Troubleshooting a Low Kecn or Kt/VTroubleshooting a Low Kecn or Kt/V
Check Anticoagulation
Efficiency
Increase duration and or frequency of HD sessions
1. Coyne, DW et al. Impaired delivery of hemodialysis prescriptions: An analysis of causes and an approach to evaluation. J Am Soc Nephrol 1997; 8:1315.
Low Kt/V1
• Low QB or t (40% of cases)
• Access recirculation (25% of cases)
• Other (large V, blood tubing, low QD etc)
Kecn low
Kecn goodKt/V low
1st Kecn low
1st Kecn good, then drops
Kecn improved
Kecn low
Check QB, QD and Filter selection (K0A)

Online Hemodiafiltration (olHDF)Online Hemodiafiltration (olHDF)Online Hemodiafiltration (olHDF)1.Combines dialysis with (usually) post-dilution
hemofiltrationBetter middle molecule clearanceReplacement fluid generated online (not available in US)More complex equipment with higher costs
2.DOPPS observational study (2006)“After adjustment, high-efficiency HDF patients had a significant 35% lower mortality risk than those receiving low-flux HD (relative risk=0.65, P=0.01). These observational results suggest that HDF may improve patient survival independently of its higher dialysis dose.
3.Dutch Convective Transport Study (Contrast)Randomized, controlled olHDF trial until 12/2010
Canaud et al:Mortality risk for patients receiving hemodiafiltration versus hemodialysis: European results from the DOPPS Kidney International (2006) 69, 2087–2093

Internal Filtration: Filter DesignInternal Filtration: Filter DesignInternal Filtration: Filter Design
©Fresenius
Large uniform pore size with very high Kuf and minimal resistance to the transfer of β2M1,2,3
New dialysate flow pathway design reduces stagnant dialysate layers and shunting1,2
New blood header improves flow distribution in the fiber bundle1
New fibers with reduced internal diameter, wall thickness and wavy structure1,2
QD can be reduced 30% without a reduction in KD (QD≤500 ml/min)
A: from Depner T and Garred L: Solute transport mechanisms in dialysis; in Replacement of Renal Function by Dialysis, 5th edition; p85B,1: Ronco et al: FX-class of hemodialyzers; Kidney International, Vol. 61, Supplement 80 (2002), pp. S126–S1422: Yamamoto et al: Technical evaluation of a dialysate flow…; ASAIO Journal 2007; 53:36-40.3: Pellicano et al: FX-E filter; Am J Kidney Dis 2008; 52:93-101.
©Fresenius
A
B

G
Liver
Dialyzer
Kidneys
GKCV1 (3.5-14 L)
C1
V2 (10.5-40 L)
C2
KD
KR
Two-Compartment Variable Volume Solute Kinetic Model
TwoTwo--Compartment Variable Volume Compartment Variable Volume Solute Kinetic ModelSolute Kinetic Model
G - C1(KD+KR) + KC(C2-C1)d(C1V1)
dt
- KC(C2-C1)d(C2V2)
dt
Adapted from Depner T and Garred L: Solute transport mechanisms in dialysis; in Replacement of Renal Function by Dialysis, 5th edition; p85

MultiMulti--Compartment Solute KineticsCompartment Solute Kinetics1. Computer modeling1
Indispensable to visualize effects of KD, frequency (f), duration (t), compartment sizes (V12), inter-compartmental mass transfer coefficient (KC), and solute generation rate (G)Only as accurate as the model; results need clinical validation
2. Specific solutes of interestPhosphate: multi-compartmental complex kinetics2
Β2-microglobulin: improved KD (olHDF), low KC3
Myeloma light chains: effects of dialyzer, V and KC4
Cytokine mobilization with convection and adsorption5
Creatinine and other non-protein bound plasma solutes6
1. Walther et al:Kidney International (2006) 69, 1056–1063.2. Spalding et al: Phosphate kinetics during dialysis:Kidney Int, Vol. 61 (2002), pp. 655–6673. Leypoldt JK: Kinetics of β2-Microglobulin…; Semin Dial—Vol 18, No 5 2005 pp. 401–4084. Hutchison CA et al:Efficient Removal of Immunoglobulin Free Light Chains by Hemodialysis…; J Am Soc Nephrol 18: 886-895, 20075. Joannes-Boyau et al: Nephrol Dial Transplant (2009) 24: 354–3576. Schneditz et al:Nephrol Dial Transplant (2009) 24: 2218–2224

Variable volume, single pool solute kinetic equation
C(t) = systemic plasma solute concentration
β = rate of fluid gain between and during dialyses
V0 = volume of solute distribution at start of dialysis
K = kidney residual clearance (KR) between dialyses
K = Sum of filter (KD) and kidney (KR) solute clearanceduring hemodialysis
t = time from start of modeling
C(t) .C0 1V0
V0
βtK ββ
K ββ V0
V0
βtK ββ
K ββ
.GK β

1. Walther et al:Kidney International (2006) 69, 1056–1063.2. Raj et al:β2-microglobulin kinetics in nocturnal HD; NDT (2000) 15: pp58-64
Coplon Dialysis Simulator1: Solute with Low KD and Low KC
2Coplon Dialysis SimulatorCoplon Dialysis Simulator11: Solute : Solute
with Low Kwith Low KDD and Low Kand Low KCC22
Conventional HD3 x 3.5 hoursKD= 57 ml/min
Daily Short HD6 x 2.5 hoursKD= 57 ml/min
Daily Nocturnal HD6 x 7 hoursKD= 49 ml/min
G = 140 mg/dayKC = 70 ml/minV1/V2= 3.5/10.5 L

Daily Nocturnal Hemodialysis (DNHD)Daily Nocturnal Hemodialysis (DNHD)Daily Nocturnal Hemodialysis (DNHD)1. Benefits
Provides the best solute removal of all modalitiesThe patient can sleep through the therapy overnightExcellent BP control, BP medications reducedExcellent phosphate control, P-binders often stopped1
Survival may be comparable to cadaveric renal Tx2
2. Barriers to useRequires a very motivated patient (≈ 5% of HD population)Significant safety concerns limit utilizationAccess venous connection monitoring and effective, safe anticoagulation is neededA dedicated, GOOD home nocturnal HD machine should have been developed at least 10 years ago!
1. Mucsi et al: Kidney International, Vol. 53 (1998), pp. 1399-14042. Pauly et al: Nephrol Dial Transplant (2009) 24: 2915–2919

Cost of Improving HD AdequacyCost of Improving HD AdequacyCost of Improving HD Adequacy1. Observation
Cost of 3x/week in-center HD has shown explosive growthNo government wants to spend more per patient
2. In-center HD cost-effectiveness study and subsequent editorial1,2
“In conclusion, given the extraordinarily high costs of the ESRD program, the viability of more frequent hemodialysis strategies depends on significant improvements in the economic model underlying the delivery of hemodialysis.”1
A subsequent editorial raised the issue of even funding clinical studies for >3x/week in center HD considering the projected 75,000-125,000 USD cost/per quality life-year gained2
1. Lee et al: J Am Soc Nephrol 19: 1792–1797, 2008.2. Annemans L: Nephrol Dial Transplant (2009) 24: 1078–1081