hematopoietic stem cell transplantation in autoimmune disease dominique farge thomas kozak zora...
TRANSCRIPT

HEMATOPOIETIC STEM CELL
TRANSPLANTATION IN AUTOIMMUNE DISEASE
Dominique FargeThomas Kozak
Zora Marjanovic
The European Group for Blood and Marrow Transplantation
Autoimmune Diseases (ADs):
- family of more than 100 heterogeneous diseases, which affect 5 to 8 % of the population worldwide
- characterised by aberrant activation of the immune system with failure of immune regulation to maintain adapted tolerance
- most patients can be treated with drugs suppressing the immune mediated inflammation, but when these fail or are too toxic, alternative strategies are needed
- severe forms of systemic ADs, such as multiple sclerosis (MS), systemic sclerosis (SSc), lupus erythematosus (SLE), Crohn’s disease, inflammatory arthritis as rheumatoid arthritis (RA) or juvenile idiopathic arthritis (JIA) and haematological immune cytopenia (HIC) could be difficult to treat
Dysthyroïdies Arthritis
RA/JIA
Sjögren
PM DM CBI
Scleroderma vasculitis
SLE
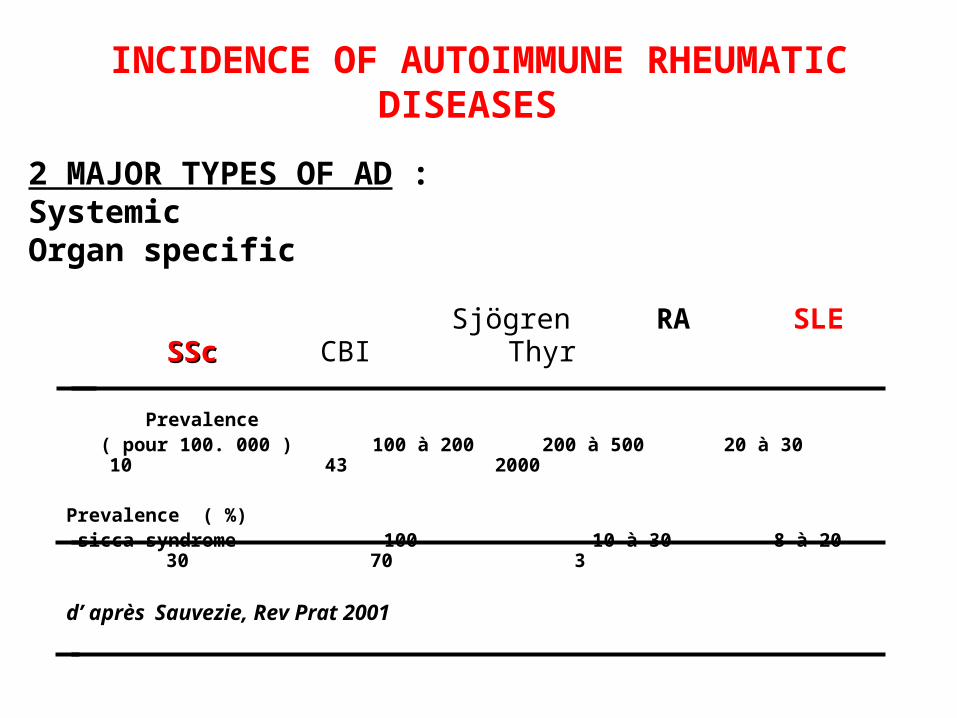
INCIDENCE OF AUTOIMMUNE RHEUMATIC DISEASES
Sjögren RA SLE SScSSc CBI Thyr
Prevalence ( pour 100. 000 ) 100 à 200 200 à 500 20 à 30 10
43 2000
Prevalence ( %) sicca syndrome 100 10 à 30 8 à 20 30
70 3
d’ après Sauvezie, Rev Prat 2001
2 MAJOR TYPES OF AD : SystemicOrgan specific
HSCT for treating severe ADsThe first consensus statement concerning the use of HSCT for treating severe ADs in 1995 stipulated:- the basic principles with regard to disease categories, patient selection, mobilisation, in vitro manipulation, conditioning and treatment
- Autologous was largely preferred to allogeneic transplantation due to lower risk of severe toxicity
- Patients should be considered for HSCT if: a) diagnosed with an AD severe enough to have an increased risk of mortality or advanced and irreversible disability; b) the ADs has been unresponsive to conventional treatments; c) the HSCT can be undertaken before irreversible organ damage, so that significant clinical benefit can be achieved
- Standard techniques, as used in autologous HSCT for haematological malignancies were employed
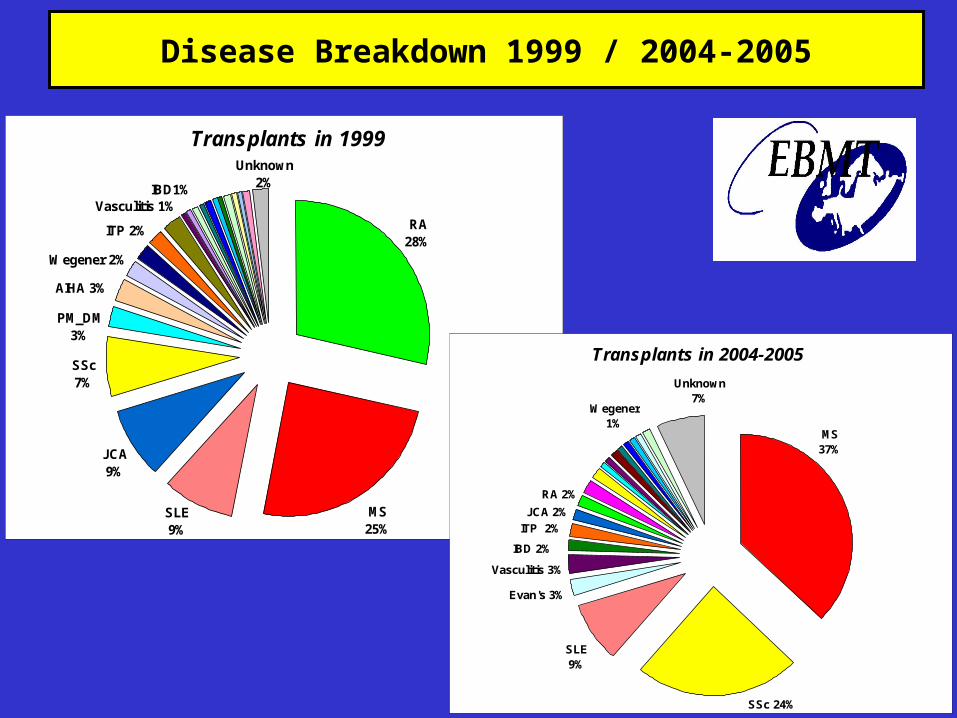
Transplants in 1999
RA28%
MS25%
JCA9%
Unknown2%
Vasculitis 1%
Wegener 2%
AIHA 3%
PM_DM 3%
SLE9%
SSc7%
ITP 2%
IBD1%
Transplants in 2004-2005
MS37%
Wegener1%
ITP 2%
IBD 2%
JCA 2%
RA 2%
Vasculitis 3%
Evan's 3%
SLE9%
SSc 24%
Unknown7%
Disease Breakdown 1999 / 2004-2005
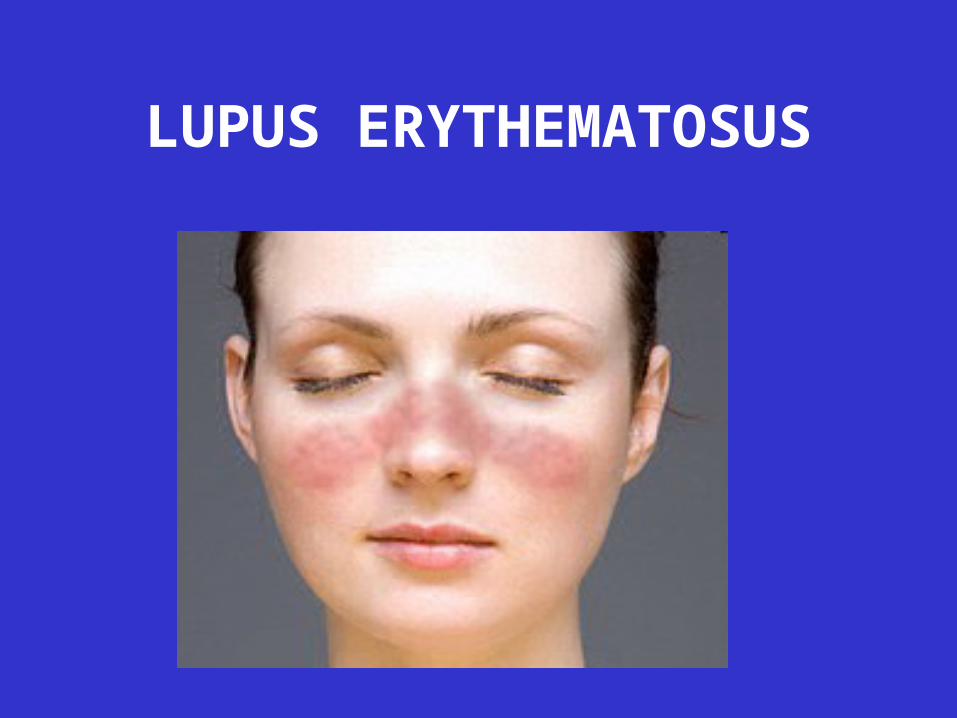
LUPUS ERYTHEMATOSUS
Systemic Lupus Erythematosus (SLESystemic Lupus Erythematosus (SLE)
Cutaneous Lupus Erythematosus
Drug-Induced Lupus
Neonatal Lupus
Types of Lupus
Systemic Lupus Erythematosus - Systemic Lupus Erythematosus (SLE) is a chronic autoimmune disease that can be fatal, the immune system attacks the body’s cells and tissue, resulting in inflammation and tissue damage
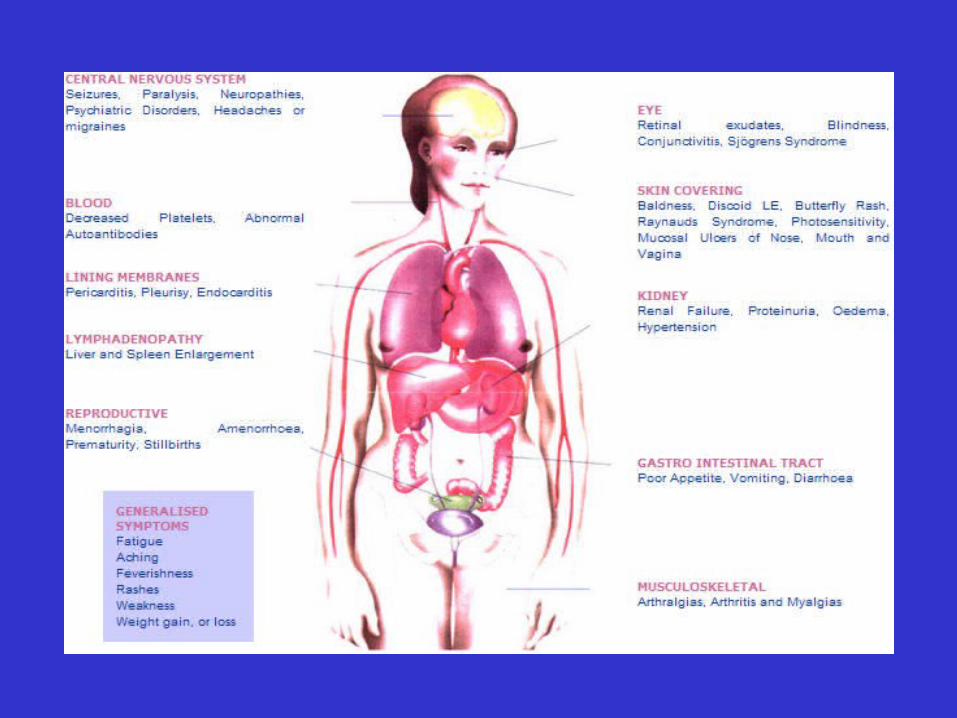
- SLE can affect any part of the body, but most often harms the heart, joints, skin, lungs, blood vessels, liver, kidneys and nervous system
-The course of the disease is unpredictable, with periods of illness called flares, alternating with remissions
- Can occur at any age, most common in young women (9/1)
SLE
- Cause of the disease remains unknown
- There are three mechanisms by which lupus is thought to develop: genetic predisposition, environmental triggers and drug reaction
SLE
• Common symptoms :- fatigue- hair loss- sensitivity to the sun- painful and swollen joints- unexplained fever- skin rashes- kidney problems
SLEDiagnosis made by a careful review of:
•Current symptoms•Laboratory test results•Medical history•Medical history of close family members
American College of Rheumatology (ACR) ClassificationCriteria (1982)
• 4/11criteria, either at present or in the past - strong chance for lupus
SLEACR 1982 Classification Criteria:
• Malar Rash• Discoid Rash• Photosensitivity• Oral Ulcers• Arthritis• Serositis• Renal Disorder• Neurological Disorder• Hematological Disorder• Immunological Disorder• Antinuclear Antibody
Tan EM, et al. The 1982 Revised Criteria for the Classification of Systemic Lupus Erythematosus. Arthritis Rheum 1982;25:1271-7.
SLE• Antinuclear antibody (ANA) testing and anti-extractable nuclear antigen
(anti-ENA) form the mainstay of serologic testing for SLE
• Several techniques are used to detect ANAs
• Clinically the most widely used method is indirect immunofluorescence
• The pattern of fluorescence suggests the type of antibody present in the patient's serum
• Present in about 5% of the general population
• Indicates that the immune system is altered
• Nearly 100% of people with lupus are ANA positive
• Not everyone with ANAs develops lupus
SLE
As lupus erythematosus is a chronic disease with no known cure, treatment is restricted to dealing with the symptoms
This involves preventing flares and reducing their severity and duration when they occur
SLE• Corticosteroids • Hydroxychlorquine (Plaquenil®)• Aspirin• Antimalarials • Cytotoxics including cyclophosphamide, azathioprine,
methotrexate• Plasmapharesis/PE• Thalidomide• Anticoagulants• Diaminodiphenylsulfone• NSAIDs• DHEA
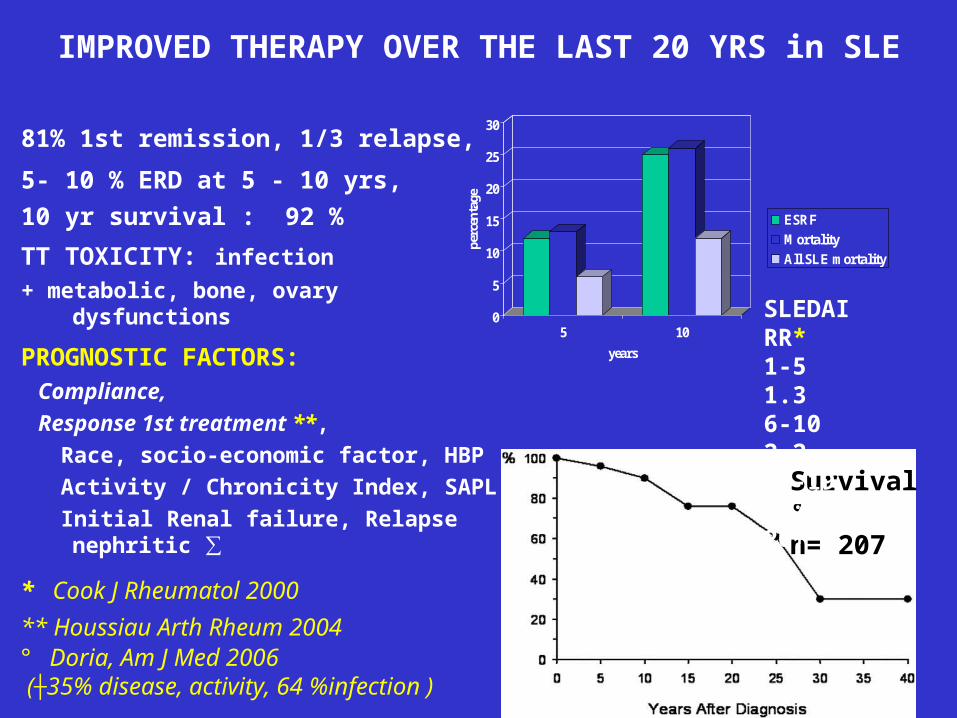
IMPROVED THERAPY OVER THE LAST 20 YRS in SLE
81% 1st remission, 1/3 relapse,
5- 10 % ERD at 5 - 10 yrs, 10 yr survival : 92 %
TT TOXICITY: infection
+ metabolic, bone, ovary dysfunctions
PROGNOSTIC FACTORS: Compliance,
Response 1st treatment **,
Race, socio-economic factor, HBP
Activity / Chronicity Index, SAPL
Initial Renal failure, Relapse nephritic ∑
0
5
10
15
20
25
30
perc
enta
ge
5 10
years
ESRF
Mortality
All SLE mortality
Survival °n= 207
SLEDAI RR*1-5 1.36-10 2.211-19 4.720+ 14.1
* Cook J Rheumatol 2000
** Houssiau Arth Rheum 2004 ° Doria, Am J Med 2006 (┼35% disease, activity, 64 %infection )
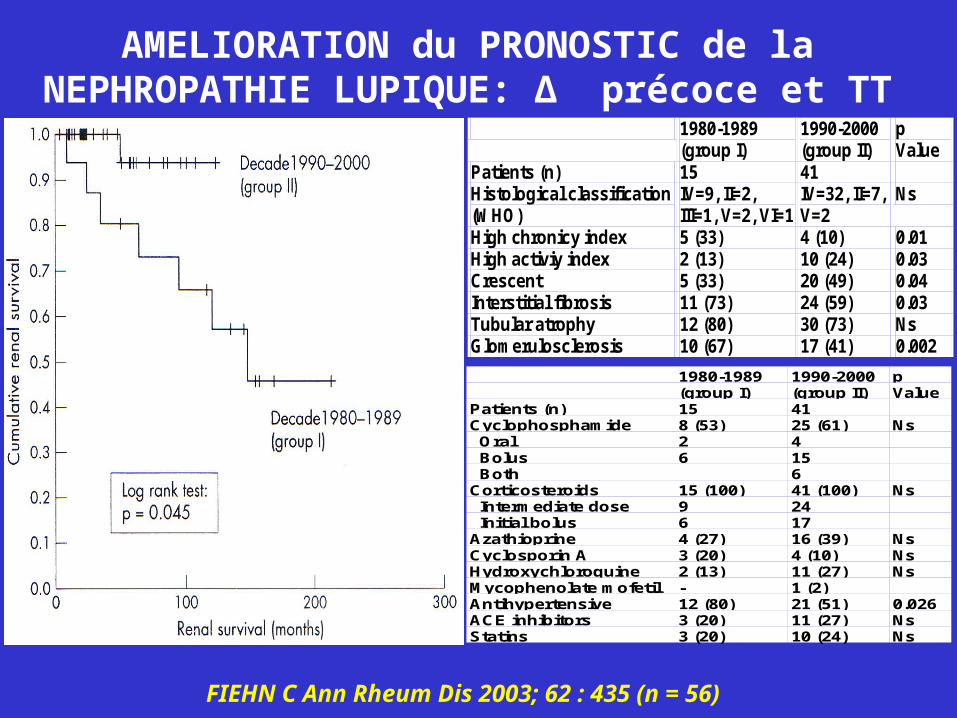
AMELIORATION du PRONOSTIC de la NEPHROPATHIE LUPIQUE: Δ précoce et TT
1980-1989 (group I)
1990-2000 (group II)
p Value
Patients (n) 15 41 Histological classification (WHO)
IV=9, II=2, III=1, V=2, VI=1
IV=32, II=7, V=2
Ns
High chronicy index 5 (33) 4 (10) 0.01 High activiy index 2 (13) 10 (24) 0.03 Crescent 5 (33) 20 (49) 0.04 Interstitial fibrosis 11 (73) 24 (59) 0.03 Tubular atrophy 12 (80) 30 (73) Ns Glomerulosclerosis 10 (67) 17 (41) 0.002
1980-1989(group I)
1990-2000(group II)
pValue
Patients (n) 15 41Cyclophosphamide 8 (53) 25 (61) Ns Oral 2 4 Bolus 6 15 Both 6Corticosteroids 15 (100) 41 (100) Ns Intermediate dose 9 24 Initial bolus 6 17Azathioprine 4 (27) 16 (39) NsCyclosporin A 3 (20) 4 (10) NsHydroxychloroquine 2 (13) 11 (27) NsMycophenolate mofetil - 1 (2)Antihypertensive 12 (80) 21 (51) 0.026ACE inhibitors 3 (20) 11 (27) NsStatins 3 (20) 10 (24) Ns
FIEHN C Ann Rheum Dis 2003; 62 : 435 (n = 56)
20
21
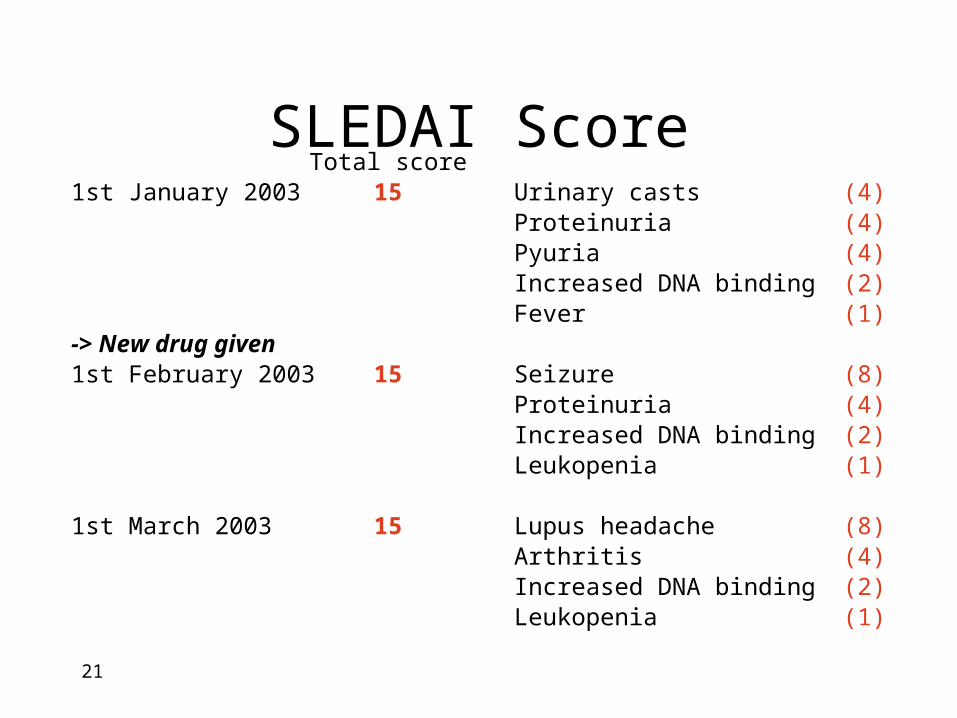
Total score1st January 2003 15 Urinary casts (4)
Proteinuria (4)Pyuria (4)Increased DNA binding (2)Fever (1)
-> New drug given1st February 2003 15 Seizure (8)
Proteinuria (4)Increased DNA binding (2)Leukopenia (1)
1st March 2003 15 Lupus headache (8)Arthritis (4)Increased DNA binding (2)Leukopenia (1)
SLEDAI Score
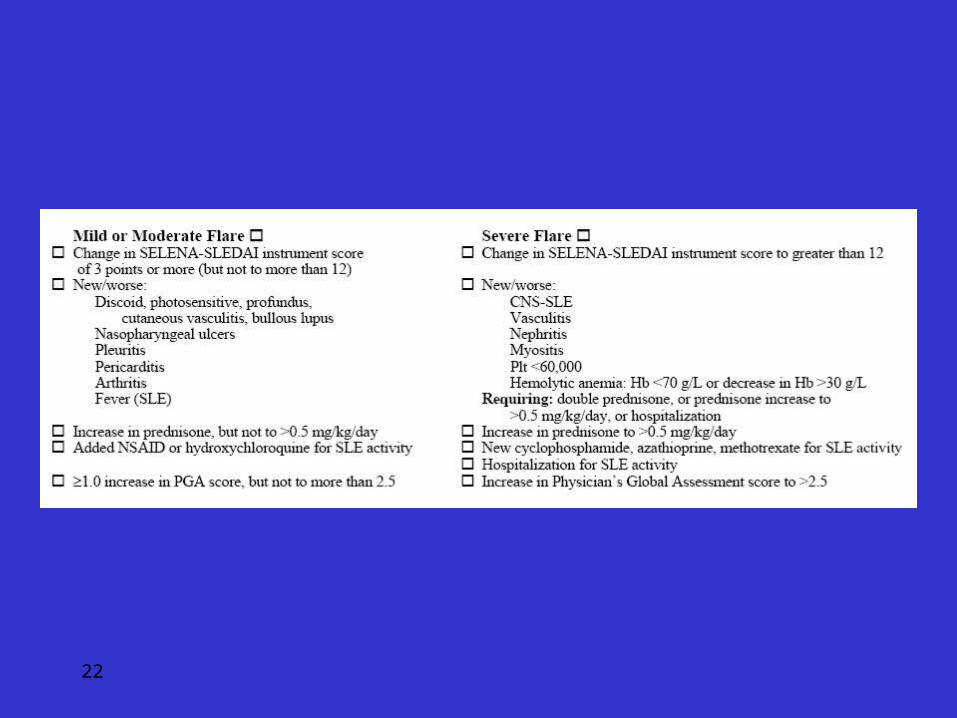
22
23
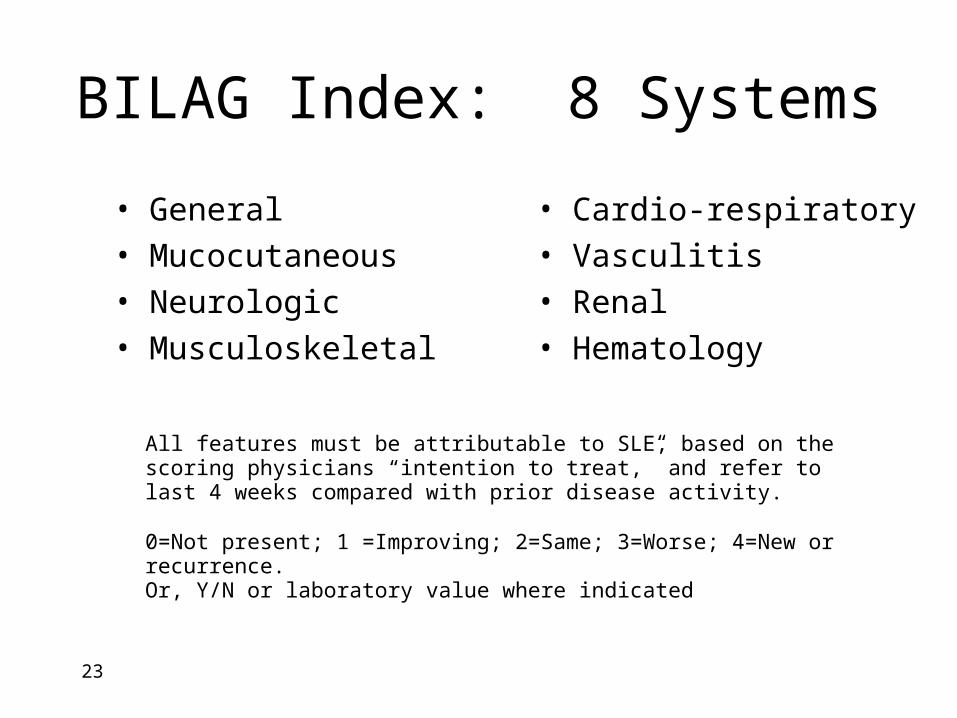
BILAG Index: 8 Systems
• General
• Mucocutaneous
• Neurologic
• Musculoskeletal
• Cardio-respiratory
• Vasculitis
• Renal
• Hematology
All features must be attributable to SLE, based on the scoring physicians “intention to treat,” and refer to last 4 weeks compared with prior disease activity.
0=Not present; 1 =Improving; 2=Same; 3=Worse; 4=New or recurrence.Or, Y/N or laboratory value where indicated
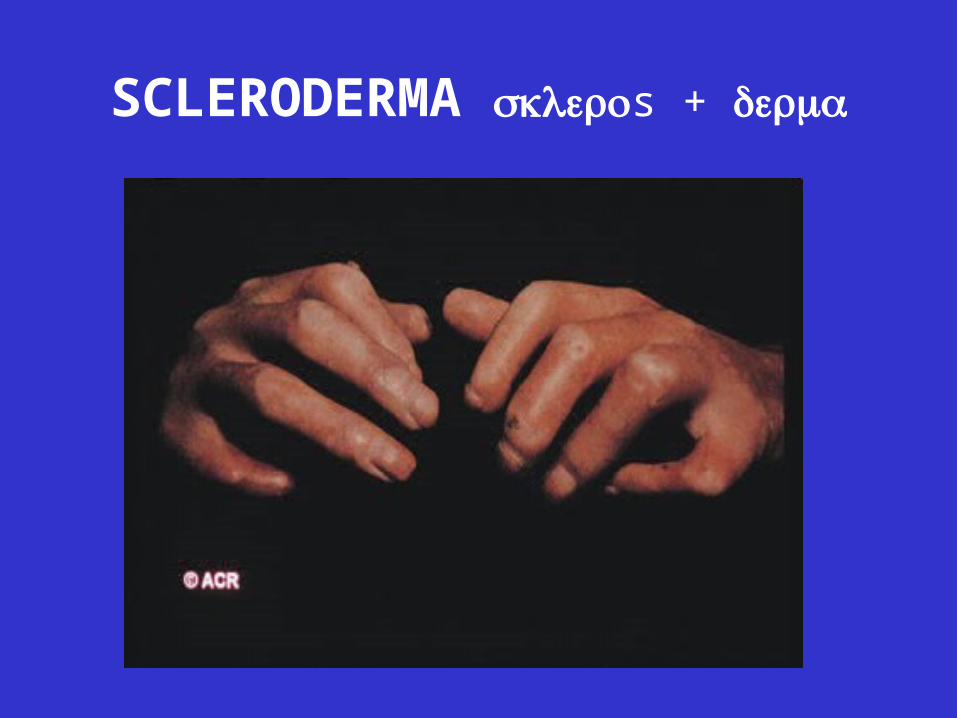
SCLERODERMA s +
SCLERODERMA• Scleroderma is a rare, chronic autoimmune
disease characterized by excessive deposits of collagen in the skin or other organs
• The primary finding in scleroderma is thickening and tightening of the skin.
• It is four times as common in women than in men
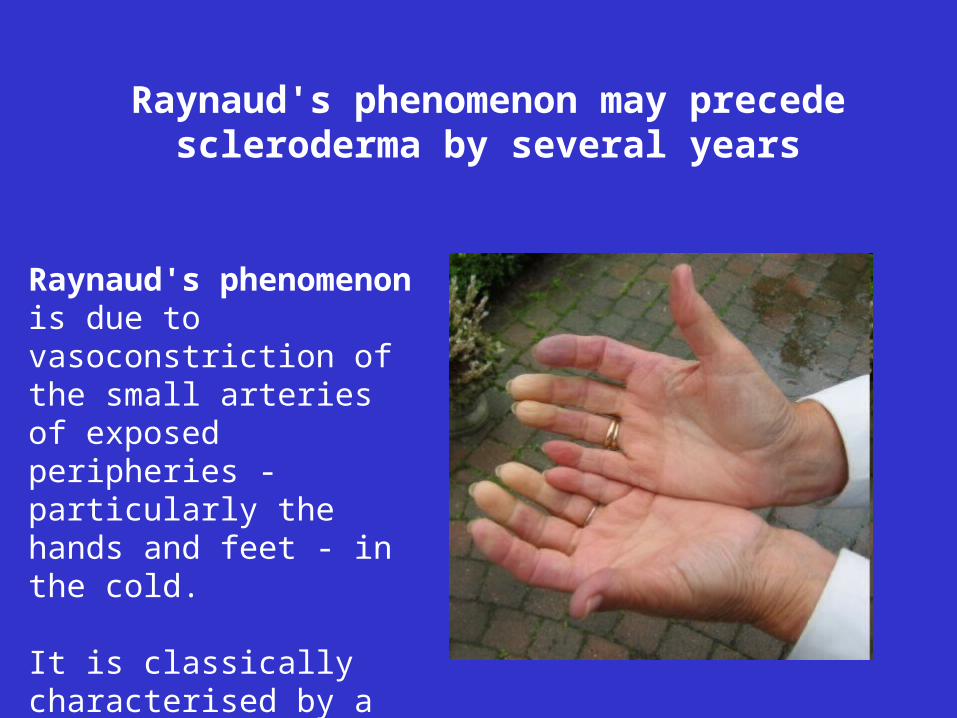
Raynaud's phenomenon is due to vasoconstriction of the small arteries of exposed peripheries - particularly the hands and feet - in the cold.
It is classically characterised by a triphasic colour change - first white, then blue and finally red on rewarming
Raynaud's phenomenon may precede scleroderma by several years
TWO broad categories:
“localized scleroderma” (not to be confused with limited) which indicates distinct skin lesions
“systemic sclerosis” which indicates similar skin symptoms and the potential for internal organ disease; the terms limited and diffuse refer to the extent of skin involvement.
SCLERODERMA
SCLERODERMA
The limited form is much milder:
- slow onset and progression, - skin hardening is usually confined to the hands
and face- internal organ involvement is less severe- much better prognosis is expected
The limited form is often referred to as CREST syndrome
"CREST" is an acronym for the five main features:
CalcinosisRaynaud’s syndrome Esophageal dysmotility Sclerodactyly Telangiectasia
Diffuse scleroderma or systemic sclerosis, the generalized type of the disease
- can be fatal as a result of heart, kidney, lung or intestinal damage
- in diffuse disease the skin changes can affect the whole body
- tightening of the skin around the fingers, the face and other areas of the body causing contractures (fixed joints) and a small mouth (microstomia), ulceration, dryness and irritation, broken blood vessels (telangiectasia) on the face and hands and calcinosis protruding through the skin
The internal organs can be affected in both limited and diffuse disease
Heart and lung involvement can also be associated with both forms, although the heart is not as commonly affected as the lung
Lung fibrosis is more common in diffuse patients
A small percentage (15%) of patients with limited form will develop pulmonary hypertension (PHT) a condition affecting the vessels taking blood from the right side of the heart to the lungs
The kidneys are rarely affected in limited disease, however approximately 5% - 10% of diffuse patients will incur some form of renal involvement

Organ INVOLVEMENT EXAMINATIONS
SKIN Scleroderma, necrosis Rodnan, ROM
Digestive tract Gatroesophagal reflux, telangiectasies, constipation/diarrhea , malabsorption, fecal incontinence
ENDOSCOPY, Blood cell count, ferritin, serum electrophoresis
LUNG Alvéolitis, fibrosis X RAY, LUNG FUNCTION TEST, WALKING TEST BLOOD GAZ, CT SCANN
PULMONARY VESSELS PHT ++++ Echocardiopgraphy, VIT LVEFG
right catheter if PHT
HEART fibrosis, conduction /rythm disturbances, necrosis, CY tox
EKG, 24 hr Holter EKG, Echocardiopgraphy
KIDNEY HYPERTENSION, RENAL CRISIS, incontinend
BP + Pulse, serum Creatinin, Urinary sediment and 24 hr protenuria
Neurologicla and pscyhiatric Anxio-depression Mental Status
Mucosal Dryness , sclerosis OPH, dental, gynecological
Genital Sclerosis, impotency Clinical examination
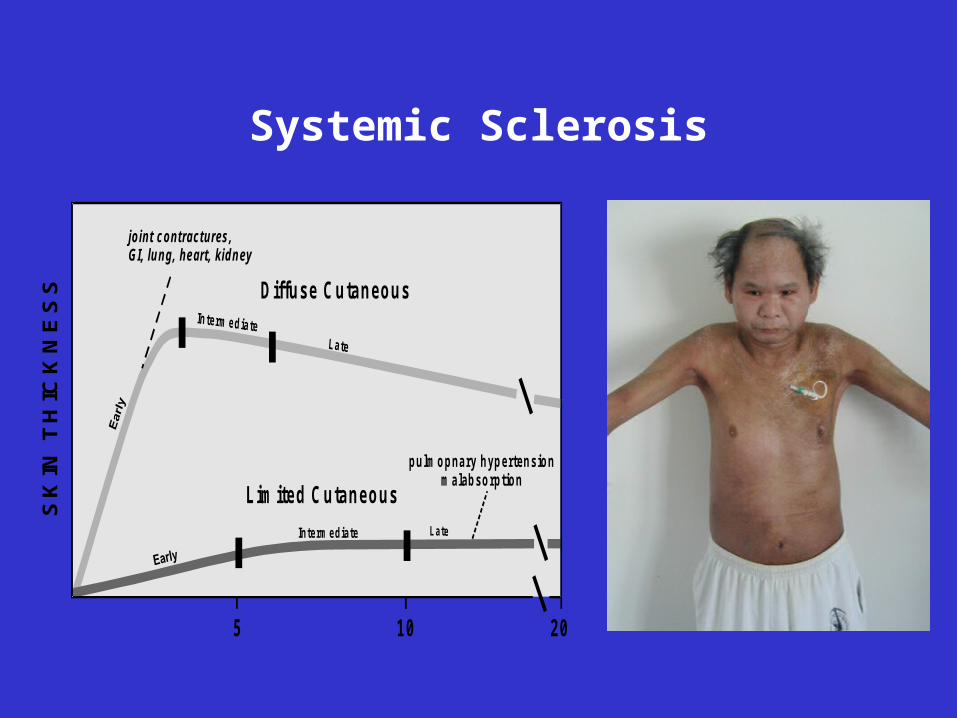
Systemic Sclerosis
Diffuse Cutaneous
Lim ited Cutaneous
pulmopnary hypertensionm alabsorption
Interm ediate
jo int contractures,GI, lung, heart, kidney
5 10 20
SK
IN T
HIC
KN
ES
S


Joints destructions in patient with Scleroderma

Lung involvement in Scleroderma
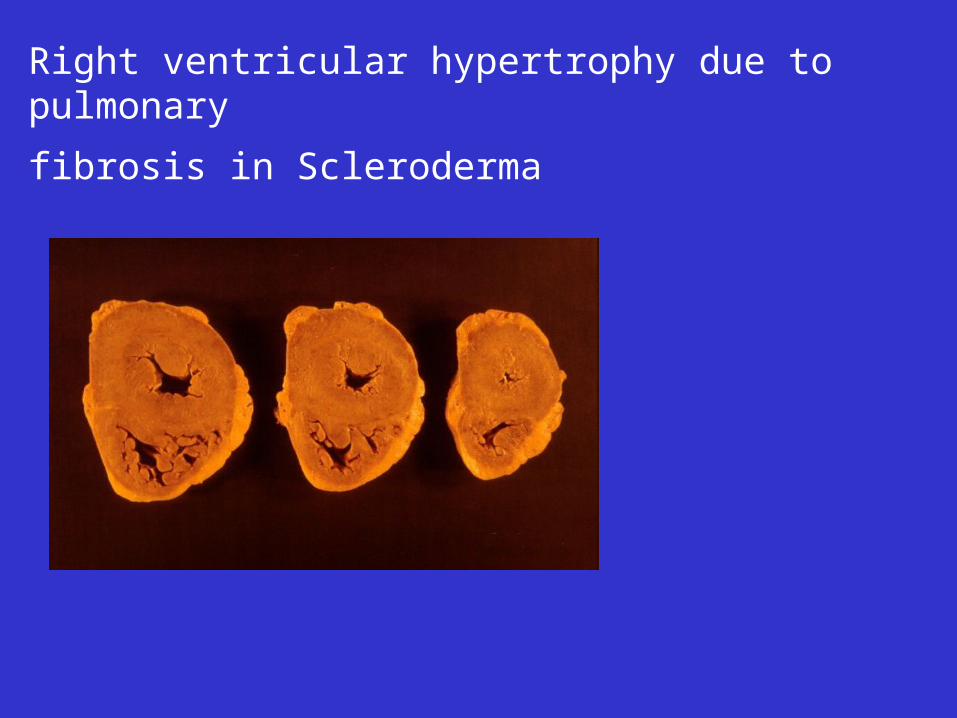
Right ventricular hypertrophy due to pulmonary
fibrosis in Scleroderma
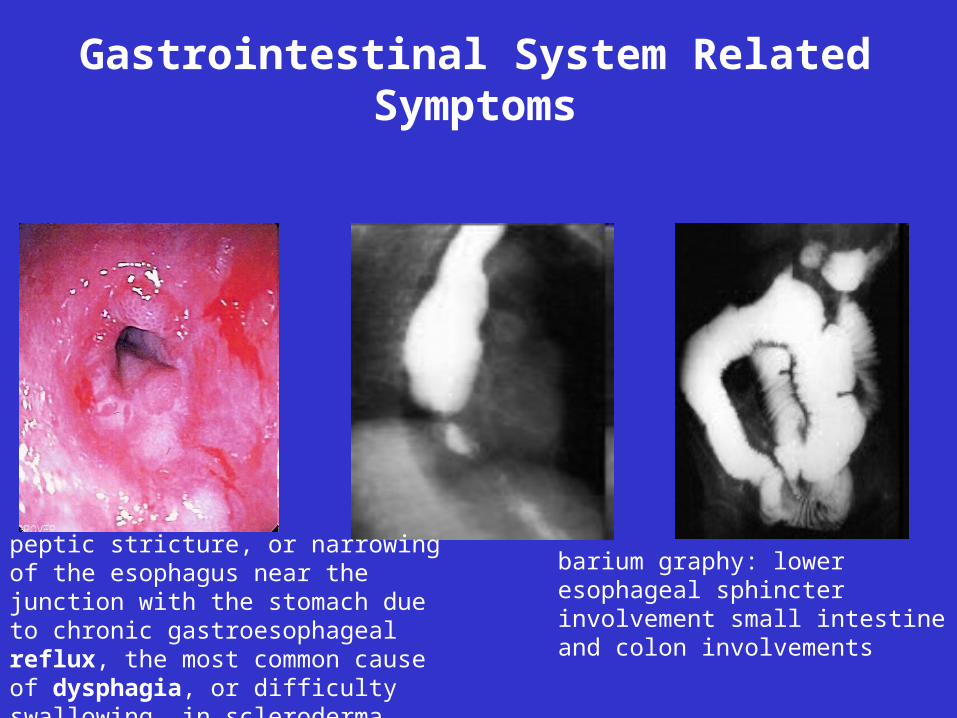
Gastrointestinal System Related Symptoms
peptic stricture, or narrowing of the esophagus near the junction with the stomach due to chronic gastroesophageal reflux, the most common cause of dysphagia, or difficulty swallowing, in scleroderma
barium graphy: lower esophageal sphincter involvement small intestine and colon involvements
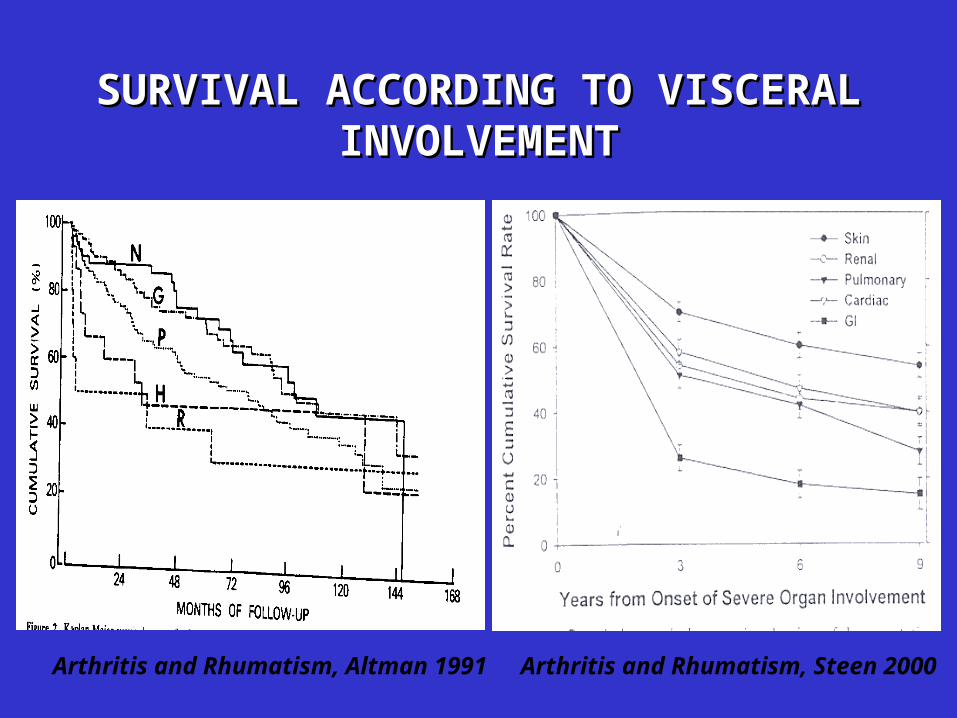
SURVIVAL ACCORDING TO VISCERAL SURVIVAL ACCORDING TO VISCERAL INVOLVEMENTINVOLVEMENT
Arthritis and Rhumatism, Altman 1991 Arthritis and Rhumatism, Steen 2000

SSC Treatment• Current therapies use medications that focus on the four
main features of the disease:
- Inflammation (NSAIDs or corticosteroids)
- Autoimmunity (methotrexate, cyclosporine, antithymocyte globulin, mycophenolate mofetil and cyclophosphamide)
- Vascular disease (calcium channel blockers, bosentan, prostacyclin, or nitric oxide)
- Tissue fibrosis (colchicine, para-aminobenzoic acid (PABA), dimethyl sulfoxide, and D-penicillamine)
CROHN’S DISEASE (27–48 per 100,000)
• Chronic, episodic, inflammatory bowel disease (IBD) that affects the entire wall of the bowel or intestines
• Crohn's disease can affect any part of the gastrointestinal tract from mouth to anus
• The disease is characterized by areas of inflammation with areas of normal lining
• The main gastrointestinal symptoms are abdominal pain, diarrhea, constipation, vomiting, weight loss
• Crohn's disease can also cause complications outside of the GIT: skin rashes, arthritis, and inflammation of the eye.
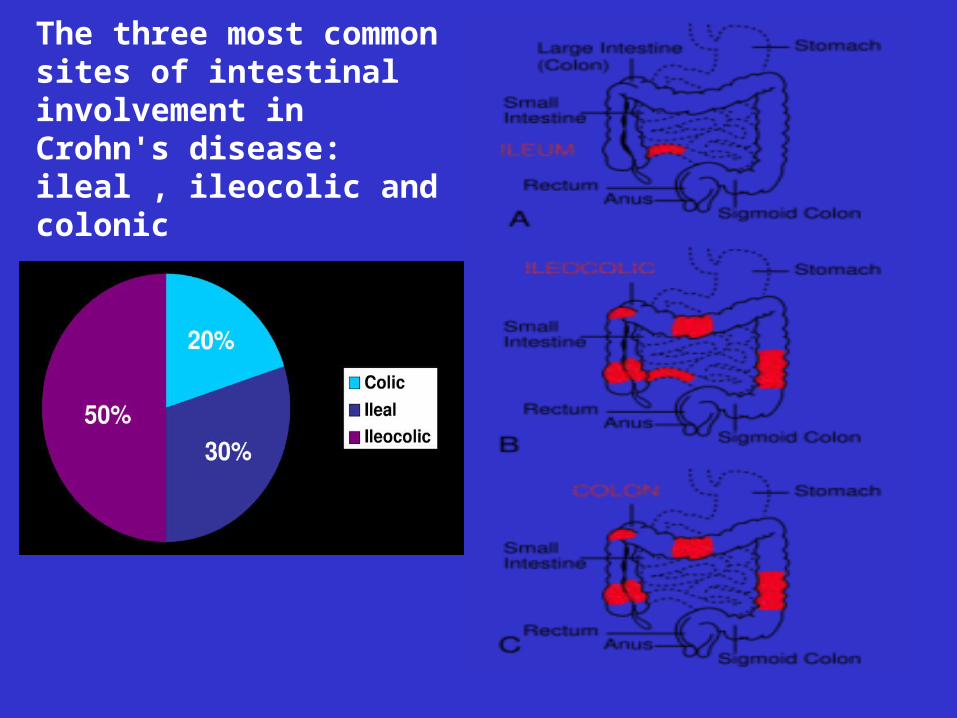
The three most common sites of intestinal involvement in Crohn's disease:ileal , ileocolic and colonic
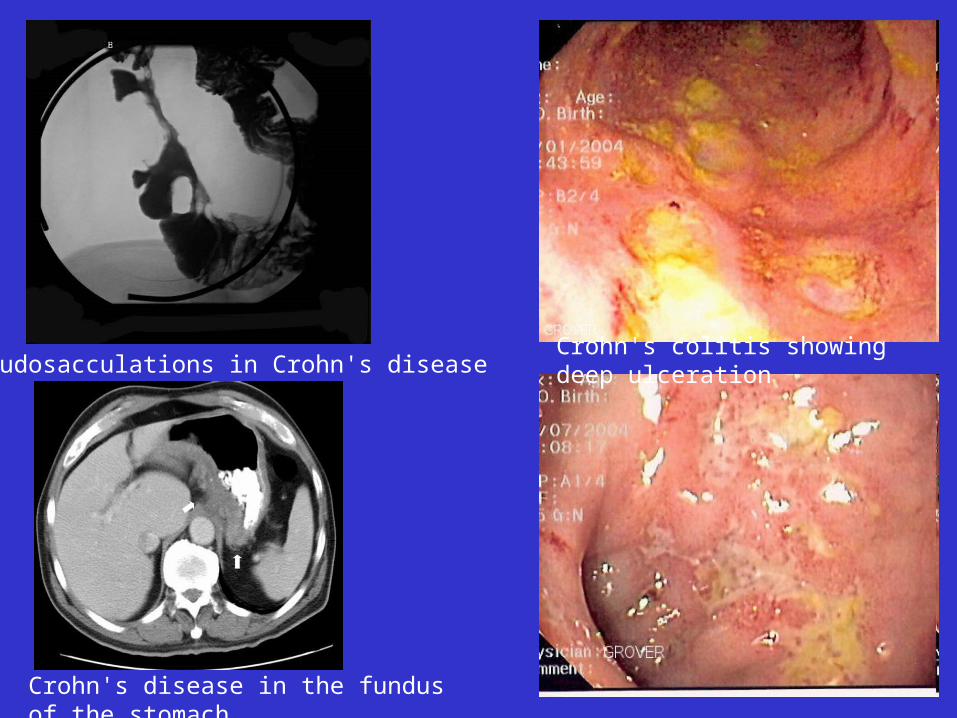
Crohn's disease in the fundus of the stomach
Crohn's colitis showing deep ulceration Pseudosacculations in Crohn's disease
Crohn's disease
• Crohn's disease may also be classified by the behaviour of disease as it progresses (Vienna classification):
Stricturing disease causes narrowing of the bowel which may lead to bowel obstruction or changes in the caliber of the feces
Penetrating disease creates abnormal passageways (fistulae) between the bowel and other structures such as the skin
Inflammatory disease (or non-stricturing, non-penetrating disease) causes inflammation without causing strictures or fistulae
Crohn's disease• Many patients with Crohn's disease have symptoms for years prior to the
diagnosis
• The usual onset is between 15 and 30 years of age but can occur at any age
• Patients with Crohn's disease will go through periods of flare-ups and remission
• Gastrointestinal symptoms :- abdominal pain - diarrhea which may or may not be bloody,- symptoms caused by intestinal stenosis - vomiting and nausea may indicate the beginnings of small bowel obstruction- fever if abscess - weight loss
Complications:
• Obstruction typically occurs from strictures or adhesions which narrow the lumen, blocking the passage of the intestinal contents
• Fistulae can develop between two loops of bowel, between the bowel and bladder, between the bowel and vagina, and between the bowel and skin
• Abscesses are walled off collections of infection Crohn's disease also increases the risk of cancer in the area of inflammation
• Malnutrition• Malabsorption • Perforation• Hemorrhage
Crohn's disease -Treatment
• 5-aminosalicylic acid
• steroids
• immunomodulators
(azathioprine, mercaptopurine and methotrexate)
• infliximab (Remicade)
• adalimumab (Humira)
• natalizumab (Tysabri)
EBMT registry• The high number of procedures reported to EBMT registry
allows:
- a careful stratification for analysing outcomes on each AD diagnosis
- tight cooperation between transplant teams and the referring specialist is a key factor
- better selection and improved clinical management of the patients
- such a data may be important for further health care decision policy and would support the need for referring centres, with significant levels of activity and resources for adapted clinical care in treating rare ADs
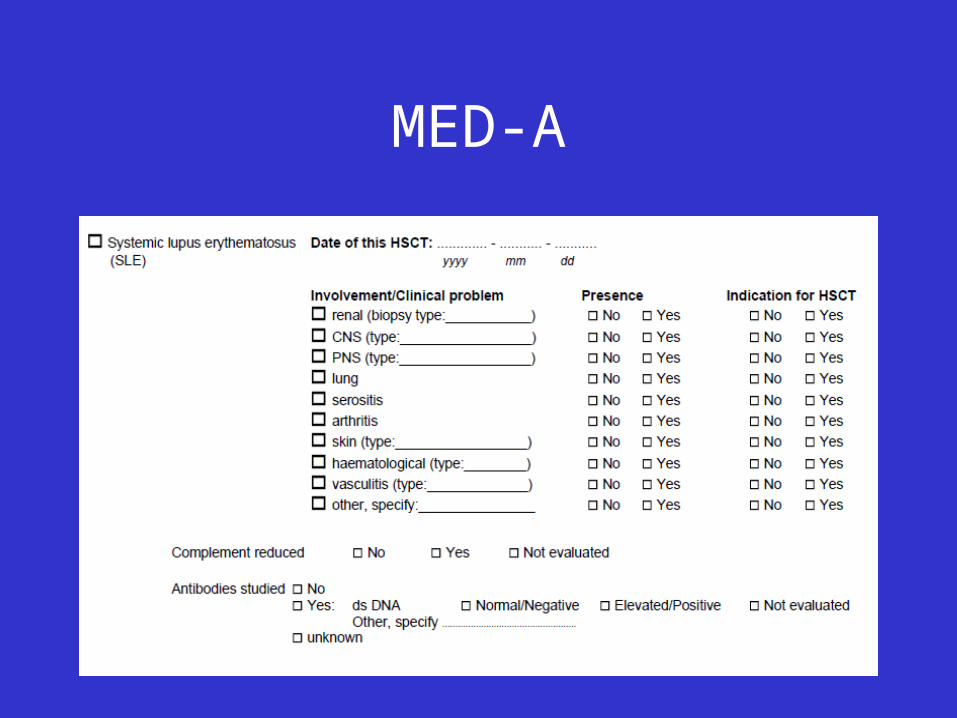
MED-A
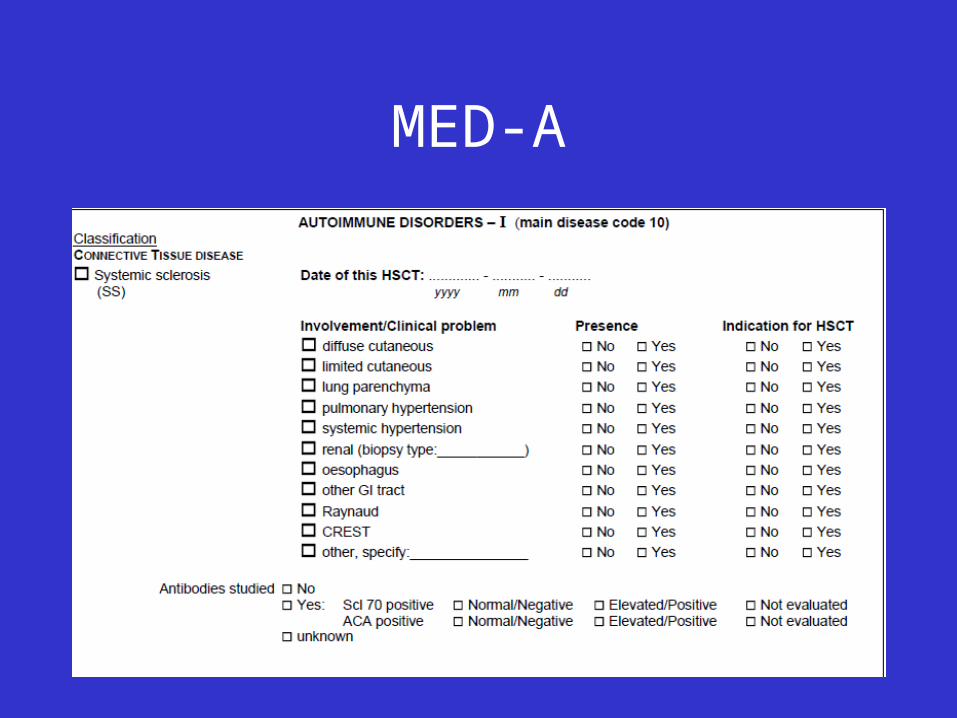
MED-A