healthy mind healthy body - oxford health plans€¦ · · 2005-11-07healthy mind healthy body,...
TRANSCRIPT
MS-05-216
Living with diabetes
How time heals
Power foods
Managingyour back pain
healthy mindhealthy body
S P R I N G 2 0 0 5 YO U R OX FO R D®
G U I DE TO LIVI NG WELL
Did you know?As of October 1, 2004, 100 percent of primary carephysicians (PCPs) participating in Oxford’s network in the tri-state
service area are either board certified or board eligible (89 percent board
certified and 11 percent board eligible). In addition, 99.9 percentof specialists in Oxford’s tri-state network are either board certified
or board eligible (85.6 percent board certified and 14.3 percent board eligible).
Board certification is the medical profession’s formal recognition of a physician’s
advanced expertise in a medical specialty or subspecialty (e.g., pediatrics,
neurology, dermatology, orthopedics). To earn this certification, a physician
must complete extensive additional training in an accredited, university-affiliated postgraduate program and pass
comprehensive examinations in his or her chosen specialty. Board eligible physicians have five years in which to
complete the board certification process. O
Olive oil has joined nuts, fish and omega-3 fatty acids in the Food and Drug
Administration’s (FDA) carefully considered list of “heart healthy”foods permitted to use a qualified health claim on their labels.
Specifically, the FDA has declared there is “limited and not conclusive
evidence” that substituting about two tablespoons (23 grams) of
monounsaturated olive oil daily for saturated fats (butter or other vegetable
oils) “may reduce the risk of coronary heart disease.” Olive oil, which is basic
to the culinary traditions of Italy, France, Spain, and virtually every other
Mediterranean country, has long been thought to play an important role in
the lower incidence of heart disease among these populations. O
Raising bilingual children may have benefits beyond giving them the
ability to communicate in two languages. In a recent issue of the journal
Psychology and Aging, researcher Ellen Bialystok described the results
of tests conducted on over 100 older people. She found that people
who have been fluent in two languages from an early age tend to have
quicker minds than those who speak one language. She
concluded that the challenges involved in a lifetime of juggling two
languages make bilingual people more elastic in their thinking, a habit
that continues in their later years when the tendency is to become
somewhat more rigid in processing thoughts and memories. O

healthy mindhealthy body
S P R I N G 2 0 0 5 YO U R OX FO R D®
G U I DE TO LIVI NG WELL
President and CEO Charles G. BergChief Medical Officer and EVP Alan M. Muney, MD, MHAVice President, Marketing Chuck GreenVice President, Marketing Communications Rebecca MadsenSenior Marketing Manager Meg DedmanCopy Editor Starlet ColemanEditor Justin Colby
Healthy Mind Healthy Body® is published exclusively for Oxford Health Plans by:Onward Publishing, Inc.10 Lewis Road, Northport, NY 11768Fax 631-754-0522
Publisher Jeffrey BaraschCreative Director Melissa BaraschEditorial Director Wendy MurphyArt Director Bruce McGowinDesigner Lisanne SchnellAssociate Creative Director Tamyra ZieranProject Director Bret BaraschBusiness Manager Liz Lynch
Oxford Health Plans, LLC and Onward Publishing, Inc., are not responsible for typographical errors.
This magazine provides general health information and, as such, is neither intended to replace the advice of yourphysician nor to imply coverage of referenced treatments or medications. Please consult with your physician regarding any treatment or medication that could impactyour health before proceeding with it, and refer to your benefit documents for specific coverage information.
© 2005 Onward Publishing, Inc. All rights reserved.
C O V E R S T O R Y
Managing your back pain
F E E D B A C K
Member Satisfaction Survey results
O F V A L U E
Do you know your A-B-Cs?
P R O V I D E R P R O F I L E
Living with diabetes
M E R G E R U P D A T E
New Oxford ID cards
L I V I N G W E L L
Power foods
N E W S Y O U C A N U S E
Oxford benefits update
S P E C I A L T O P I C
Helping time heal
W E L L N E S S
Bone basics
4
9
10
12
15
16
18
24
26
C O N T E N T S
Healthy Mind Healthy Body, which is designed to give you the latest information on a wide range of health topics
and your plan benefits, is available on our web site. Simply log in to your personalized account page at www.oxfordhealth.com.
As always, we encourage you to e-mail your comments to us at [email protected], or write to: Oxford Health
Plans, c/o Member Publications, 55 Corporate Drive, Trumbull, CT 06611.
4
2 6
1 8
C O V E R S T O R Y 4
Managing
If prizes were given out for most common medical disorders, back
pain would surely be a winner. Statistics show that back pain is
second only to persistent cough as the reason Americans seek medical
care at physicans’ offices and hospital emergency rooms. It ranks
right after the common cold as a frequent cause of lost work time.
And it’s the leading cause of disability among Americans age 45
and under. Eight out of 10 adults will have a back pain problem
at some time in their life, and most will have more than one episode.
As common as it is, back pain remains one of the more
difficult conditions to diagnose and treat. While most
bouts of back pain resolve in a few days, with or without
medical intervention, none of the treatments currently
available for chronic conditions can promise to eliminate
pain in every case. Rehabilitation rather than cure must
be the goal in those instances.
At Oxford, we are convinced that when it comes to
managing back pain, knowledge is power. The better you
understand the challenges and realities of back pain, the
more effective you can be in teaming up with your med-
ical care givers to find the most appropriate treatment.
Let’s start by examining the structure of the back itself.
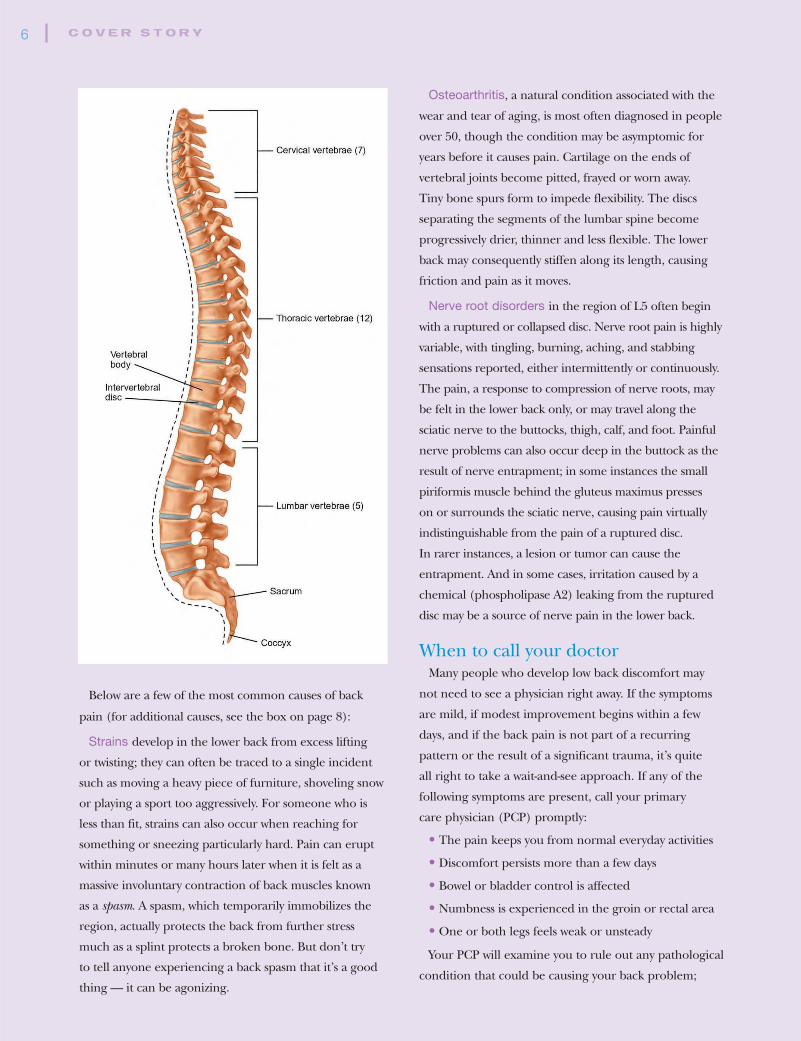
Anatomy 101Your back is a miracle of bioengineering: a complicated
system of nerves, muscles, soft tissue, and vertebrae. The
33 vertebrae stack to form a strong but flexible column
that surrounds and protects your spinal cord, a thick
bundle of many specialized nerves running from the
base of your skull to your extremities. Although every
part of the back is important, it’s the upper 24 vertebrae
that do most of the work. Grouped into three sections,
they are labeled as follows:
• Cervical vertebrae (C1-C7) support the neck and head
• Thoracic vertebrae (T1-T12) connect to the ribs
protecting the heart and lungs
• Lumbar vertebrae (L1-L5) form the lower back
The back’s complex anatomy can make it difficult to
pinpoint the origins of your back trouble. Poor posture,
weak muscle tone, a sports-related injury, sitting for long
periods, excess body weight, and ordinary aging can all
contribute to backache. Less likely causes are a number of
underlying illnesses that incidentally trigger inflammation
and pain in the back area. Smoking and psychological
stress are still other potential factors that may play into
the mix. Diagnosis begins with defining the problem.
Targeting the painBack ailments are typically classified as acute or chronic.
Any back disorder is considered acute if it lasts only a few
days to several weeks. Fortunately, about 90 percent of
patients with acute pain episodes recover spontaneously
within a month, with or without seeking the aid of
their physician. A back problem that continues to cause
symptoms of pain and weakness longer than three
months, or which recurs with regularity is considered
chronic. Such episodes may call for a closer look —
comprehensive diagnostic testing, sophisticated pain relief
methods and the collaborative care of several specialists.
Identifying the source of the discomfort is important
to determining the diagnosis. Symptoms of stiff neck and
shoulder muscles, occasional weakness or numbness in the
arms and hands, usually indicate a problem in the cervical
region. Short of genuine trauma to the cervical spine such
as whiplash, cervical pain events are most often muscular
in origin and heal quickly with rest and mild painkillers.
Thoracic problems are rare, thanks to the stability of the
upper back and the fact that relatively limited muscular
movement takes place here. It’s the lumbar region
(L1-L5) that is most vulnerable. Here is where the
greatest variety of back problems settle.
5
your back pain
Below are a few of the most common causes of back
pain (for additional causes, see the box on page 8):
Strains develop in the lower back from excess lifting
or twisting; they can often be traced to a single incident
such as moving a heavy piece of furniture, shoveling snow
or playing a sport too aggressively. For someone who is
less than fit, strains can also occur when reaching for
something or sneezing particularly hard. Pain can erupt
within minutes or many hours later when it is felt as a
massive involuntary contraction of back muscles known
as a spasm. A spasm, which temporarily immobilizes the
region, actually protects the back from further stress
much as a splint protects a broken bone. But don’t try
to tell anyone experiencing a back spasm that it’s a good
thing — it can be agonizing.
Osteoarthritis, a natural condition associated with the
wear and tear of aging, is most often diagnosed in people
over 50, though the condition may be asymptomic for
years before it causes pain. Cartilage on the ends of
vertebral joints become pitted, frayed or worn away.
Tiny bone spurs form to impede flexibility. The discs
separating the segments of the lumbar spine become
progressively drier, thinner and less flexible. The lower
back may consequently stiffen along its length, causing
friction and pain as it moves.
Nerve root disorders in the region of L5 often begin
with a ruptured or collapsed disc. Nerve root pain is highly
variable, with tingling, burning, aching, and stabbing
sensations reported, either intermittently or continuously.
The pain, a response to compression of nerve roots, may
be felt in the lower back only, or may travel along the
sciatic nerve to the buttocks, thigh, calf, and foot. Painful
nerve problems can also occur deep in the buttock as the
result of nerve entrapment; in some instances the small
piriformis muscle behind the gluteus maximus presses
on or surrounds the sciatic nerve, causing pain virtually
indistinguishable from the pain of a ruptured disc.
In rarer instances, a lesion or tumor can cause the
entrapment. And in some cases, irritation caused by a
chemical (phospholipase A2) leaking from the ruptured
disc may be a source of nerve pain in the lower back.
When to call your doctorMany people who develop low back discomfort may
not need to see a physician right away. If the symptoms
are mild, if modest improvement begins within a few
days, and if the back pain is not part of a recurring
pattern or the result of a significant trauma, it’s quite
all right to take a wait-and-see approach. If any of the
following symptoms are present, call your primary
care physician (PCP) promptly:
• The pain keeps you from normal everyday activities
• Discomfort persists more than a few days
• Bowel or bladder control is affected
• Numbness is experienced in the groin or rectal area
• One or both legs feels weak or unsteady
Your PCP will examine you to rule out any pathological
condition that could be causing your back problem;
C O V E R S T O R Y 6

7
fortunately, statistics show that only about one patient in
200 has low back pain symptoms that trace to a serious
medical illness.
In arriving at an initial diagnosis, the PCP must rely in
part on information you provide. You will be asked to
describe your pain and its intensity; a pain-rating scale of
1-10 is a favored method. You will also be asked to locate
the discomfort and to recall what you were doing when
the pain first started. Your PCP will examine your gait
and posture, check your reflexes and look for tender
points on your back. He or she may ask what routine
activities make the pain worse or better, what recent
illnesses you may have had, or whether you have
experienced any recent weight loss.
Unless your PCP uncovers a “red flag” (something
that might indicate the need for further testing right
away), the standard for acute back pain is conservative
treatment that addresses symptoms while allowing time
to see if the condition heals itself. This may include
instructions for applying periodic cold packs during
the first 24 hours; intermittent heat on days thereafter.
A few days of limited (not strict) bed rest may also be
in order, followed by a gentle return to normal activities.
Over-the-counter or prescription pain relievers may
help alleviate local discomfort.
Be sure to discuss with your doctor any physical
limitations you should adhere to during the healing
phase. Find out what kinds of exercises you should be
doing to strengthen weakened muscles. (Following some
back injuries, muscle atrophy begins almost immediately
unless addressed with exercise.) Ask about possible side
effects of pain medications (nausea, vomiting, dizziness,
sleepiness) or contraindications (no driving, no operating
machinery, no alcohol). And learn what to do if the pain
worsens or continues beyond a measured time.
Stepped up treatmentWhen conservative treatment does not bring expected
relief in a reasonable time, you and your PCP may want
to consider more advanced diagnostic imaging (MRI or
CT scans, for example) or one of several alternative and
complementary treatments, including physical therapy,
acupuncture, massage therapy, chiropractic, biofeedback,
and transcutaneous nerve stimulation (TENS).
The latter, which involves the delivery of low-level
electrical impulses over the skin of the affected area,
can be self-administered at home using a portable
TENS device. It produces a numbing or vibrating
sensation that releases the body’s own pain-modulating
chemicals (endorphins) and overloads nerve paths.
TENS interrupts pain sensations in some, but not all,
patients. (For more information on complementary
and alternative treatments, see the box on page 8.)
More potent medications may also be indicated
when non-narcotic medications are insufficient; your
physician may try a short-term regimen of opioid drugs
(morphine, codeine and other narcotic substances)
while your body heals.
Another possible course of action is referral to a
specialist in orthopedics, neurology or physiatry,
especially in a chronic pain situation. One approach
to treating severe back pain that these specialists
occasionally use is the epidural injection. A mixture
of corticosteroids and anesthetics are injected by
needle into the layer surrounding the spinal cord
at the site of a swollen and irritated nerve; the steroids
reduce the inflammation while the anesthetic provides
local pain relief.
C O V E R S T O R Y 8
C o m m o n s o u r c e s o f l o w b a c k p a i n
• Muscular weakness; poor coordination of “core” muscles
• Tear in muscles and ligaments that support the back
• Muscle spasm
• Injuries and small fractures in the spine
• Rupture or bulging (herniation) in a weakened disc
• Misalignment of vertebrae due to instability or deteriorated vertebral surfaces (spondylolisthesis)
• Narrowed spinal canal (stenosis)
• Scar tissue that entraps and presses upon nerves
• Long-term postural deformities (scoliosis, lordosis, etc.)
Surgery to repair or fuse damaged sections of the spine,
common as it was a decade ago, is seen increasingly as an
intervention of last resort. Recent studies show that spinal
surgery provides long-term relief in only one in 100 cases of
low back problems. And it can sometimes make the condition
worse. If your healthcare provider recommends surgery, be
sure you fully understand his or her reasons, as well as the
inherent risks and benefits of the recommended procedure.
Although back pain is a complicated condition to diagnose
and treat, it’s still very important for you to take responsibility
for the care you receive. If your doctor sticks to a single
conservative treatment over a prolonged period, without your
experiencing significant relief, you may want to seek a second
opinion. And, if you and your doctors have tried several
approaches over an extended period and none of them yields
“a cure,” you may have to accept the fact that some back pain
is never going to be fully resolvable. In such instances,
effective pain management and the healing effects of physical
and psychological adaptation may offer you your best hope.
Prevention The good news is that prevention and self-care will go a
long way in reducing your lifetime risks of back pain. Start
with a serious effort to stay fit and trim. If you aren’t there
yet, keep working at it. Ask your PCP to recommend exercises
that condition the muscles in your body, especially those
supporting your back and abdomen. Make these and ordinary
walking exercises part of your weekly routine. Pay attention
to good nutrition and maintain appropriate levels of calcium
and Vitamin D in your diet to keep your bones strong and
resilient. And learn the fundamental physics of back safety:
• Lift objects close to your body rather than at
arm’s length
• Lift with your back straight and knees bent rather
than bending over with knees straight
• Lift only when your feet are securely positioned
and your path is clear
• Use slow, steady movements rather than hurried,
jerky movements
• Don’t rely on back belts; there’s no proof as yet
that they offer protection
• Know your personal limits; never ask your back
to do more than it should O
C o m p l e m e n t a r y a n d a l t e r a t i v e t r e a t m e n t s f o r b a c k p a i n
Back pain is your body’s way of telling you that you’ve
been neglecting your back’s health. So part of rehabilitation
should include a closer look at your lifestyle, including diet,
physical activity and levels of mental stress. Below are just
some of the many mind-body therapies that can help ease
the pain. Before beginning any of these, however, discuss
the idea with your physician. Some specific activities may be
contraindicated where stretching and bending are involved,
or in the case of back instability.
Acupuncture, acupressure and transcutaneous nerve
stimulation are all forms of pain distraction. They can help
in defusing a painful flare-up by stimulating the release of
endorphins, chemicals naturally produced in the body to
block pain signals.
Bodywork, including the Alexander Technique, Pilates
Method, Feldenkrais Method, and Heller Method, can do
wonders for back pain that stems from poor posture and
lack of physical conditioning.
Heat and cold therapies can bring temporary relief. For acute
“hot” pain, try a cold pack. For a stiff lower back, a heat pack
can be a comforting way to loosen up tight, tense back muscles.
Spinal manipulation therapies, practiced by chiropractors
and osteopaths, have been shown to improve acute flare-ups
of low back pain. In most cases, such treatments should be
accompanied by stretching and other routine forms of exercise.
Yoga works to stretch and loosen muscle tightness while
easing the mind to cope with pain. If pain is severe, find a
class in rehabilitative yoga; these classes are offered by
many hospitals and private studios.
Oxford Members have access to a credentialed network of
complementary medicine providers including chiropractors,
massage therapists, acupuncturists, naturopaths, and yoga
instructors that can help to manage pain, or to help to prevent
the onset of chronic back pain. To find a complementary
medicine provider in your area, log into www.oxfordhealth.com
and use our Doctor Search tool, or call our Customer Service
Department at the number on your Oxford ID card and request
a Roster of Participating Physicians and Providers.
F E E D B A C K 9
How are we doing?
Your satisfaction is important to us. As part of Oxford’s
commitment to quality healthcare, we strive to provide you
with a positive experience, from your contact with our Customer
Service Department to your ongoing encounters with the
physicians and hospitals in our provider network. And we know
from objective reports that our overall efforts are working well.
Again this past year, the National Committee for Quality
Assurance (NCQA), the most respected independent
rating organization in the healthcare industry, awarded
Oxford ratings of “Excellent,” NCQA’s highest level of
accreditation, in three of our service areas — New York,
New Jersey and Connecticut. Although pleased with this
rating, we know there is always room for improvement,
so we will continue to ask you for feedback on ways to
enhance specific details of your healthcare experience.
In our latest annual surveys, conducted among 1,100
Members by independent research organizations, we
received a number of helpful suggestions. You can expect
improvements in your healthcare in 2005, and beyond,
based on these suggestions.
One area on which we are now focused is processing
claims and appeals more quickly. We are also making
improvements in our Member education efforts, both
in our written materials and on our Internet site,
www.oxfordhealth.com, by giving you more information
regarding how your plan works and how you can make
the most of it, in language that is clearly understandable.
Lastly, we’re working with our providers — your
physicians and their office staffs — to improve patient-
doctor communication, all of which should help ensure
that you get the care you need at the right time and place.
We will keep you informed through Healthy Mind
Healthy Body and www.oxfordhealth.com about the
steps that we are taking to provide you with a better
healthcare experience. And please continue to let us
know how we can serve you better. We’re listening!
If you have a suggestion about how we can improve
your satisfaction with Oxford, contact us via e-mail
at [email protected] or at the
address below:
Member Satisfaction Oxford Health Plans QM Department44 South BroadwayWhite Plains, NY 10601
O F V A L U E 10
ABCDo you know your
A varied, balanced diet of whole foods is always going
to be your best source of vitamins and minerals, but
surveys show that most people’s eating habits do not
provide adequate amounts of several nutrients considered
essential to good health. Meeting the recommended
daily allowances (RDAs) for these nutrients is very
important not just to help us feel good today, but to
prevent and manage a wide range of chronic diseases —
from heart disease and osteoporosis to macular
degeneration and diabetes — that may develop over time.
An estimated 40 percent of Americans take at least
one vitamin or mineral supplement as a form of
“nutrition insurance.” Far and away the most popular
forms of supplementation are multivitamin and multi-
mineral compounds. Each pill or tablet typically contains
microamounts of as many as two dozen active ingredients,
including vitamins A, B2, B6, B12, C, D, E, folic acid,
niacin, and thiamin, at levels approaching or exceeding
RDAs for adults or, for some formulations, a more
targeted audience, such as children, seniors or women.
Many of the same vitamins and minerals are also widely
taken as single-ingredient products, mostly by people
who have specific risks or deficiencies. Calcium and
iron are recommended at levels too great to include at
100 percent of their RDA in multivitamins, so additional
amounts may be taken as single ingredient supplements.
The good, the bad and the unessential Selecting a course of supplements can be tricky. First,
there is the matter of which supplements and the amount
of each that is appropriate for your age, gender and
health situation. While vitamin and mineral supplements
are generally beneficial, some of them can interfere with
medications or interact with an existing medical condition
to make it worse. And contrary to some advertising claims,
taking megadoses of anything has risks even for healthy
people; too much of one nutrient can cause
a deficiency in another. It is always best to
talk to your physician before embarking
on a new regimen of nutritional supple-
mentation. For any vitamin or mineral,
never exceed the “upper limit” (UL)
that may appear on the label, which
indicates that more of this ingredient
poses a risk of adverse health effects.
There is also the question of product quality and
consistency. Because vitamins, minerals, herbs, and other
nutritional boosters are not classified as prescription
drugs by the Food and Drug Administration, their
labeling, contents and manufacturing practices are not
government-regulated. Some studies have shown that
among multivitamin and multimineral compounds in
the United States, one in three fail to deliver on one or
more of their claims, frequently containing substances
well above or below the amounts listed on their labels.
Information is just a click awayFortunately, Oxford Members can get objective
information on all these matters from ConsumerLab.com,
which provides Oxford Members with independent
evaluations of nearly all nutritional supplements sold
in the United States. To access these resources, and to
sign up for a newsletter exclusive to Oxford Members,
simply log in to your personalized account page at
www.oxfordhealth.com. For an overview of nutritional
supplements, see the chart at right.
Most importantly, you should try to eat a healthy,
well-balanced diet. Nothing in a bottle or a pill can
match the health benefits of a diet rich in brightly
colored fresh fruits, deeply pigmented vegetables and
fiber-filled grains. O
A-B-Cs?
11
RR E S O U R C E S
Read more about nutritional supplements inConsumerLab.com’s Guide to Buying Vitamins &Supplements, available to Oxford Members throughthe Healthy Bonus® program. Call 1-800-431-1579and mention the promotional code Oxford to receive20 percent off on the $17.95 cover price of this veryinformative paperback. Oxford Members can also receive a 10 percent discount on all products from Puritan’s Pride,®
including vitamin and mineral supplements throughOxford’s Healthy Bonus program. Just visitwww.puritan.com and enter coupon code EOX8JUat the checkout page.
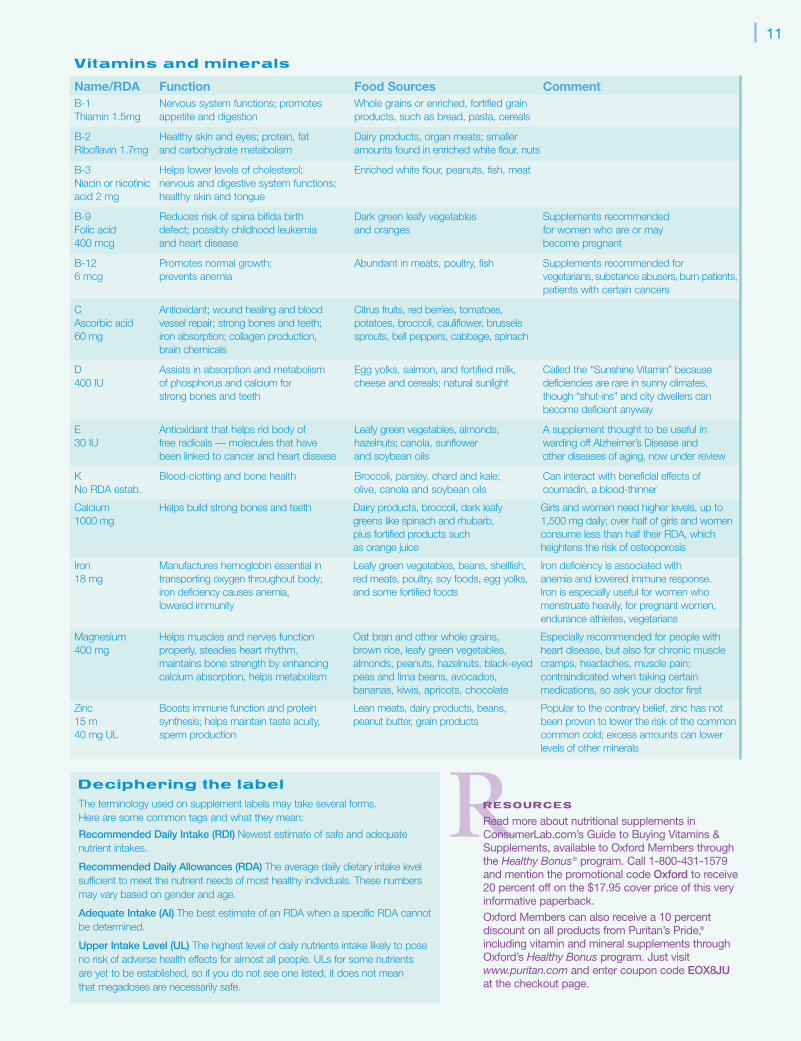
D e c i p h e r i n g t h e l a b e l
The terminology used on supplement labels may take several forms. Here are some common tags and what they mean:
Recommended Daily Intake (RDI) Newest estimate of safe and adequate nutrient intakes.
Recommended Daily Allowances (RDA) The average daily dietary intake level sufficient to meet the nutrient needs of most healthy individuals. These numbersmay vary based on gender and age.
Adequate Intake (AI) The best estimate of an RDA when a specific RDA cannotbe determined.
Upper Intake Level (UL) The highest level of daily nutrients intake likely to poseno risk of adverse health effects for almost all people. ULs for some nutrients are yet to be established, so if you do not see one listed, it does not mean that megadoses are necessarily safe.
V i t a m i n s a n d m i n e r a l s
Name/RDA Function Food Sources CommentB-1 Nervous system functions; promotes Whole grains or enriched, fortified grainThiamin 1.5mg appetite and digestion products, such as bread, pasta, cereals
B-2 Healthy skin and eyes; protein, fat Dairy products, organ meats; smaller Riboflavin 1.7mg and carbohydrate metabolism amounts found in enriched white flour, nuts
B-3 Helps lower levels of cholesterol; Enriched white flour, peanuts, fish, meatNiacin or nicotinic nervous and digestive system functions; acid 2 mg healthy skin and tongue
B-9 Reduces risk of spina bifida birth Dark green leafy vegetables Supplements recommended Folic acid defect; possibly childhood leukemia and oranges for women who are or may400 mcg and heart disease become pregnant
B-12 Promotes normal growth; Abundant in meats, poultry, fish Supplements recommended for 6 mcg prevents anemia vegetarians, substance abusers,burn patients,
patients with certain cancers
C Antioxidant; wound healing and blood Citrus fruits, red berries, tomatoes, Ascorbic acid vessel repair; strong bones and teeth; potatoes, broccoli, cauliflower, brussels 60 mg iron absorption; collagen production, sprouts, bell peppers, cabbage, spinach
brain chemicals
D Assists in absorption and metabolism Egg yolks, salmon, and fortified milk, Called the “Sunshine Vitamin” because 400 IU of phosphorus and calcium for cheese and cereals; natural sunlight deficiencies are rare in sunny climates,
strong bones and teeth though “shut-ins” and city dwellers canbecome deficient anyway
E Antioxidant that helps rid body of Leafy green vegetables, almonds, A supplement thought to be useful in 30 IU free radicals — molecules that have hazelnuts; canola, sunflower warding off Alzheimer’s Disease and
been linked to cancer and heart disease and soybean oils other diseases of aging, now under review
K Blood-clotting and bone health Broccoli, parsley, chard and kale; Can interact with beneficial effects of No RDA estab. olive, canola and soybean oils coumadin, a blood-thinner
Calcium Helps build strong bones and teeth Dairy products, broccoli, dark leafy Girls and women need higher levels, up to 1000 mg greens like spinach and rhubarb, 1,500 mg daily; over half of girls and women
plus fortified products such consume less than half their RDA, which as orange juice heightens the risk of osteoporosis
Iron Manufactures hemoglobin essential in Leafy green vegetables, beans, shellfish, Iron deficiency is associated with 18 mg transporting oxygen throughout body; red meats, poultry, soy foods, egg yolks, anemia and lowered immune response.
iron deficiency causes anemia, and some fortified foods Iron is especially useful for women who lowered immunity menstruate heavily, for pregnant women,
endurance athletes, vegetarians
Magnesium Helps muscles and nerves function Oat bran and other whole grains, Especially recommended for people with 400 mg properly, steadies heart rhythm, brown rice, leafy green vegetables, heart disease, but also for chronic muscle
maintains bone strength by enhancing almonds, peanuts, hazelnuts, black-eyed cramps, headaches, muscle pain; calcium absorption, helps metabolism peas and lima beans, avocados, contraindicated when taking certain
bananas, kiwis, apricots, chocolate medications, so ask your doctor first
Zinc Boosts immune function and protein Lean meats, dairy products, beans, Popular to the contrary belief, zinc has not15 m synthesis; helps maintain taste acuity, peanut butter, grain products been proven to lower the risk of the common40 mg UL sperm production common cold; excess amounts can lower
levels of other minerals
P R O V I D E R P R O F I L E12
“My central task with diabetes patients,”
Dr. George Liu explains, “is education. I
spend a lot of time talking to my patients
because I have to make them understand
that their future with this disease depends as
much on them as on what I do as a doctor.”
“Some patients get very discouraged at the outset,”
Dr. Liu continues. “Others are determined to keep
a certain emotional distance from their disease, hoping
to leave everything to their doctor to solve. But no
doctor can make them better single-handedly. I tell
them that the best outcome is possible only when
they get fully involved and take responsibility for their
care every day.” (For more information on diabetes,
see Just what is diabetes? on page 14.)
Dr. Liu’s commitment to patient self-management and
education is based on years of experience observing
which patients do well and which patients succumb to
the complications associated with uncontrolled diabetes.
His record of success has won him the respect of his
medical peers and of his patients alike. A board certified
specialist in internal medicine with a sub-specialty in
endocrinology, Dr. Liu is also one of 30 physicians in the
New York region who have been selected to participate
in Oxford’s Diabetes Best Practices Network. This network
is the key component to Oxford’s Diabetes Best Practices
Program. The program works with PCPs to match high-
risk diabetic Members with endocrinologists who have
received, or will soon apply for, recognition from the
National Committee for Quality Assurance (NCQA) for
the quality of care they provide to patients with diabetes.
A balancing act“Living successfully with diabetes is a constant balancing
act, for the patient and the doctor” says Dr. Liu. People
with diabetes are usually advised to eat meals on a regular
schedule, to have a snack before bedtime, and to take
medications at precise dosages and hours. Change any one
of the elements of diet, exercise and insulin supply, stray
far from the well-regulated routine, and the patient’s blood
glucose levels may soar (hyperglycemia), or drop suddenly
and dangerously, causing insulin shock (hypoglycemia).
“Handling all these requirements is especially trouble-
some for adolescents,” Dr. Liu continues. “Their lives
aren’t normally geared to so much regularity nor do they
like to dwell on their health.” By way of example, he cites
a 16 year-old patient named Akeem King. “Akeem has type
1 diabetes, so he needs replacement insulin daily. He plays
Living withdiabetes
Dr. George Liu
13varsity basketball at his school, which requires intense physical
activity. Like most young men his age, he’s self-conscious about
doing anything that might be perceived by his teammates as
‘different.’ Ideally, Akeem is a great candidate for an insulin
pump, but he doesn’t want to wear one because of the way it
looks under his team jersey. He also doesn’t want to be seen at
school injecting himself with a needle, as his previous doctor
wanted him to do. Akeem often skipped his insulin rather
than interrupt his activities. He was not doing well at all.”
“Akeem was referred to me as someone who needed to
come to better terms with his disease,” Dr. Liu explains.
“After getting to know him, I was able to develop a treat-
ment plan that Akeem is willing to follow. It took some time
to get it right, but now he’s able to self-inject his medications
just twice a day — before he goes to school and when he
gets home. He’s also paying closer attention to what he
eats. I’ve told him that so long as he can show me that he’s
managing his blood sugar levels safely, we can continue to
do it his way. I’ve also told him, I feel good when he
feels good, so we have a kind of pact.”
Akeem’s judgment is more direct: “Dr. Liu
is cool. He talks to me and my parents a
lot about what can happen when I mess up.
He makes me come in to his office often
to see how I’m doing. He makes me show
him my test results for each day and
lets me know right away when I’m
not scoring points with him. I
was angry at first about all the
rules he gave me to follow
and, in the beginning, I
tried faking the blood sugar
numbers sometimes, but
now I’m getting so I
really understand why
I have to be careful.
My goal is to play
competitive
basketball and
so far I’m
doing it.
Dr. Liu
doesn’t let me
get away with
much, but I’m not
complaining.” O
A r e y o u a t r i s k f o r
t y p e 2 d i a b e t e s ?
You may be at an elevated risk for type 2 diabetes if:
• You are overweight
• You are age 65 or older
• You have a parent, brother or sister with diabetes
• Your family background is African American, AmericanIndian, Asian American, Pacific Islander, or HispanicAmerican/Latino
• You have had gestational diabetes, or have given birth to at least one baby weighing more than 9 pounds
• Your blood pressure is 140/90 or higher, or you have beentold that you have high blood pressure
• Your cholesterol levels are not normal; your HDL cholesterol(“good” cholesterol) is 35 or lower, or your triglyceride levelis 250 or higher
• You are fairly inactive; exercising fewer than three times a week
The more factors that apply to you, the higher your risk. Some factors are, of course, beyond your control, but weight,exercise and diet are all factors you can change for the better.
If you are concerned that you may be at risk for diabetes, or have other questions about the disease, speak with yourprimary care physician.
Healthy Bonus ® resources
for managing diabetes
This year, Oxford’s Healthy Bonus program has beenexpanded to include many offers that can help Memberswith diabetes manage their condition, including no-sugaradded candies, snacks and foods, cooking supplies and
much more. Here are a few of the offers available:
Diabetic Express Save 10 percent on all sugar-free candies, foods, cooking supplies, lotions and creams, and carrying cases.
Diabetic Candy.com Save 10 percenton all items.
Foot Solutions Receive 10 percent off on products, including specialfootwear for people with foot and lower leg conditions
Russell Stover 10 percent on all sugar-free candies
TCBY® Save $1.00 on any no-sugaradded menu item
Active Forever Save 10 percent on a selection of products to help make living with special conditions easier
For information on how to obtain these and other Healthy Bonus offers available to Oxford Members, visitwww.oxfordhealth.com or call ourCustomer Service Department at the number on your Oxford ID card.

P R O V I D E R P R O F I L E14
Diabetes has the potential to trigger a host of serious
complications, from skin ulcerations, foot infections
and periodontal disease, to high blood pressure, high
cholesterol, heart disease, stroke, kidney malfunction,
damage to the eyes (diabetic retinopathy), and extensive
nerve damage. These factors all add up to a chronic
disease that can be devastating. Under the right circum-
stances, however, diabetes can sometimes be prevented,
sometimes delayed and most certainly managed.
The Centers for Disease Control (CDC), which broadly
tracks America’s health, reports that type 2 diabetes, once
known as adult-onset diabetes, is rising sharply among
Americans; a situation related to the growing incidence
of overweight and obesity in all age groups. The most
recent survey reports that in the last 20 years, the number
of Americans with diagnosed diabetes has more than
doubled, from 5.8 million to 13.3 million, and another
5.2 million people have diabetes but do not know it.
More than 90 percent of these people have type 2
diabetes. Older Americans are especially hard hit, with
more than 18 percent of Americans over 65 being treated
for diabetes. Type 1 diabetes, formerly known as juvenile
diabetes, is far less common, accounting for roughly five
percent of the entire diabetes community. But type 1
takes a substantial toll, nonetheless, in that it usually
develops in the formative childhood years, becoming
a chronic condition that must be lived with for many
decades. A third kind of diabetes, known as “gestational,”
occurs infrequently during pregnancy and disappears
after the pregnancy is completed. More than 50,000
pregnant women have gestational diabetes each year,
and, although temporary, it signals a heightened risk for
developing type 2 diabetes within 10 years.
Doctors now screen for diabetes as part of routine
physicals and obstetric care. A blood screening for
diabetes may also be done on a patient presenting
unexplained symptoms of extreme thirst, urination,
persistent hunger, weakness and fatigue, frequent
infections, or slow wound healing. Certain known risk
factors (See Are you at risk for type 2 diabetes? on page
13) may also prompt a blood test for blood sugar levels.
A test result that indicates blood sugar levels higher than
the 70 to 110 milligrams per deciliter (mg/dL) range is
a standard indicator of diabetes for people under 50;
only slightly higher numbers in people above that age.
For more information on diabetes, visit the American
Diabetes Association’s web site at www.diabetes.org. O
Just what is diabetes?
OOX F O R D I N F O
Oxford’s Living with DiabetesSM program offers educationalmaterials and case management support to help Membersunderstand and improve control of their diabetes. For moreinformation about the program, please call 1-800-665-4686,Monday through Friday, 8:00 AM to 4:30 PM.
Diabetes is a condition in which the body’s pancreas either fails to produce a sufficient supply of the hormone insulin (type 1 diabetes), or the bodybecomes resistant to the insulin that is available (type 2 diabetes). The resultis that the simple sugars and carbohydrates taken in as food and turnedinto glucose cannot be fully metabolized, and the millions of cells within the body that depend on them for energy cannot do their work. The unusedglucose builds up in the bloodstream and urine, creating dangerously highlevels of blood glucose, the principal markers of diabetic disease.
M E R G E R U P D A T E 15
New OxfordID Cards
In the Fall 2004 issue of Healthy Mind Healthy
Body, we announced the merger between Oxford
Health Plans and UnitedHealthcare, and promised
to keep you posted in future issues about what this
merger means to you.
Throughout the months of April and May 2005, new
identification cards will be mailed to Oxford Members.
You will notice that key information is clearly displayed
on the cards and the new color of the ID cards will
make photocopying easier for your providers. The
merger of Oxford Health Plans and UnitedHealthcare
has produced a new corporate logo, which is also
prominently displayed on the new cards.
If you are a Member of a PPO or POS plan,
your card may indicate that you have access to
UnitedHealthcare’s Choice Plus network, outside
of the tri-state area. The Choice Plus network provides
nationwide in-network access to care, and will be
available on May 1, 2005 to eligible Members.
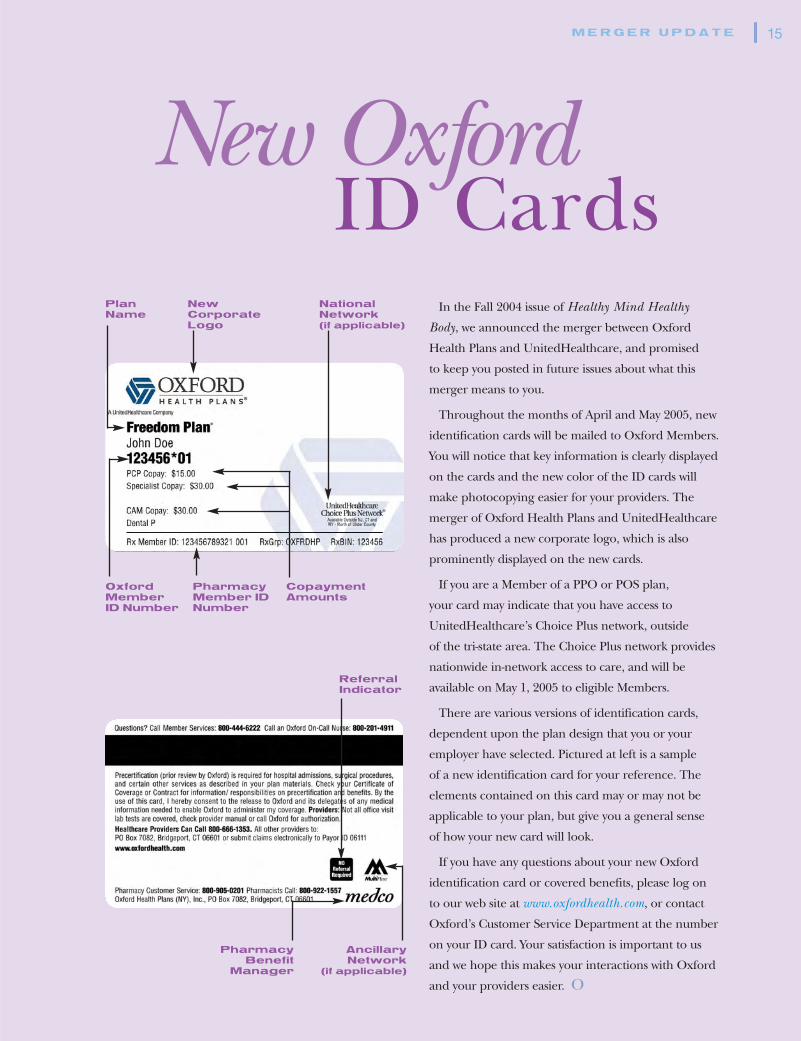
There are various versions of identification cards,
dependent upon the plan design that you or your
employer have selected. Pictured at left is a sample
of a new identification card for your reference. The
elements contained on this card may or may not be
applicable to your plan, but give you a general sense
of how your new card will look.
If you have any questions about your new Oxford
identification card or covered benefits, please log on
to our web site at www.oxfordhealth.com, or contact
Oxford’s Customer Service Department at the number
on your ID card. Your satisfaction is important to us
and we hope this makes your interactions with Oxford
and your providers easier. O
PlanName
OxfordMember ID Number
PharmacyMember IDNumber
CopaymentAmounts
ReferralIndicator
AncillaryNetwork
(if applicable)
PharmacyBenefit
Manager
NewCorporateLogo
NationalNetwork (if applicable)
L I V I N G W E L L16
B l u e b e r r y P o w e r M u f f i n s
w i t h A l m o n d S t r e u s e l
These are called “power” muffins because they’re
loaded with B vitamins from whole wheat flour, calcium
from milk and yogurt, antioxidants from blueberries,
and heart-friendly monounsaturated fat from almonds
and canola oil. You can freeze the muffins for up to
a month, then thaw them at room temperature, or
microwave each muffin at HIGH 15 to 20 seconds.
Muffins:
1 1⁄2 cups all-purpose flour, divided
1 cup whole wheat flour
1 cup quick-cooking oats
1 cup granulated sugar
1 tablespoon baking powder
1 teaspoon baking soda1⁄4 teaspoon salt
2 cups vanilla low-fat yogurt1⁄2 cup 2% reduced-fat milk
3 tablespoons canola oil
2 teaspoons vanilla extract
1 large egg
1 1⁄2 cups fresh blueberries
Cooking spray
Streusel:1⁄4 cup all-purpose flour1⁄4 cup slivered almonds, chopped
1 tablespoon brown sugar
1 tablespoon butter, melted
Directions:
Preheat oven to 400°.
To prepare muffins, lightly spoon flours into dry
measuring cups; level with a knife. Combine 1 1⁄2 cups
all-purpose flour, whole wheat flour, oats, granulated
sugar, baking powder, baking soda, and salt in a large
bowl, stirring with a whisk. Make a well in center of
mixture. Combine yogurt, milk, oil, vanilla, and egg,
stirring with a whisk. Add yogurt mixture to flour
mixture; stir just until moist. Fold in blueberries.
Spoon 2 rounded tablespoons batter into each of
30 muffin cups coated with cooking spray.
To prepare streusel, combine 1⁄4 cup all-purpose flour,
almonds, brown sugar, and butter. Sprinkle evenly over
batter. Bake at 400° for 15 minutes or until muffins
spring back when touched lightly in center. Cool in
pans 10 minutes on a wire rack; remove from pans.
Serve warm or at room temperature.
Yield: 15 servings (serving size: 2 muffins)
Nutrition per serving
CALORIES 244 (23% from fat); FAT 6.1g (sat 1.3g, mono 2.9g, poly
1.4g); PROTEIN 6.1g; CHOLESTEROL 18mg; CALCIUM 136mg;
SODIUM 260mg; FIBER 2.5g; IRON 1.5mg; CARBOHYDRATE 42.3g
Enjoying a healthy diet means more than just including foods low in fat and sodium. Since weeat so many processed foods, it is important to make sure that our diets include whole, fresh foodsrich in vitamins and minerals — “power foods.” To get you started, we have included two deliciousrecipes from Cooking Light magazine: both include high levels of many important vitamins andminerals. To find out the potential benefits of some of these nutrients, consult the chart on page 11.
Power foods

17
S i z z l i n g S a l m o n - a n d - S p i n a c h
S a l a d w i t h S o y V i n a i g r e t t e
The spinach in this recipe provides folic acid while the
salmon is an excellent source of heart-healthy Omega-3
oil and vitamins A and B.
Dressing:
3 tablespoons thinly sliced green onions
3 tablespoons rice vinegar
3 tablespoons low-sodium soy sauce
1 tablespoon water
1 teaspoon sesame seeds, toasted
1 teaspoon bottled minced garlic
1 teaspoon dark sesame oil1⁄2 teaspoon chile paste with garlic or 1⁄4 teaspoon crushed red pepper
Salad:
2 teaspoons dark sesame oil, divided
4 cups thinly sliced shiitake or button mushroom caps (about 8 ounces)
1 cup (1-inch) sliced green onions
1 cup fresh or frozen corn kernels, thawed
4 (6-ounce) salmon fillets (about 1 inch thick)
8 cups baby spinach
1 cup fresh bean sprouts
1 cup red bell pepper strips
Directions:
Preheat broiler.
To prepare dressing, combine first 8 ingredients in a small
bowl, and stir well with a whisk.
To prepare salad, heat 1 teaspoon oil in a large nonstick
skillet over medium-high heat. Add mushrooms and 1 cup
onions; sauté 8 minutes. Stir in corn; remove from heat.
Place the fish on a foil-lined baking sheet; brush evenly
with 1 teaspoon oil. Broil 8 minutes or until fish flakes
easily when tested with a fork.
Place 2 cups spinach on each of 4 plates; top each serving
with 1⁄4 cup bean sprouts, 1⁄4 cup red bell pepper, 1⁄2 cup
mushroom mixture, and 1 fish fillet. Drizzle about 2
tablespoons dressing over each salad.
Yield: 4 servings
Nutrition per serving
CALORIES 418 (40% from fat); FAT 18.8g (sat 3.2g, mono 8.3g, poly
5.1g); PROTEIN 42.9g; CHOLESTEROL 111mg; CALCIUM 163mg;
SODIUM 549mg; FIBER 7.8g; IRON 6.1mg; CARBOHYDRATE 21.8g
Healthy Bonus® savings
As an Oxford Member, you can
receive 11 issues of Cooking
Light for only $16, a savings of
more than 65 percent off the
cover price. To order your
subscription, available at this
price for Oxford Members only,
call toll-free at 1-877-300-7177
and mention the promotional
code OXHP. Or, log on to
www.cookinglight.com/oxhp.
*Offers are valid through June 30, 2005. These discounts are offered in addition to, and separate from, your benefit coverage through Oxford HealthPlans. These arrangements have been made for the benefit of Members, and do not represent an endorsement or guarantee on the part of Oxford.Discounts may change from time to time and without notice and are applicable to the items referenced only. Oxford Health Plans cannot assumeany responsibility for the products or services provided by vendors or the failure of vendors referenced to make available discounts negotiated withOxford; however, any failure to receive discounts should be reported to Oxford Customer Service by calling the number on your Oxford ID card.
OOX F O R D I N F O
To find out more about the array of Healthy Bonus offers availableto Oxford Members, including savings on weight loss programs,fitness, nutrition, and publications, visit www.oxfordhealth.com, orcall Customer Service at the number on your Oxford ID card.*
© 2005 Cooking Light Magazine
N E W S Y O U C A N U S E18
Subimo Hospital Advisor™
now available in Spanish Subimo’s Hospital Advisor is a fast and easy way for you
to get important information that will help you make
informed decisions when choosing a hospital. With this
tool, Oxford Members can research information about
patient safety measures, outcomes, complications, and
the total number of beds at hospitals in their area.
Now, the Hospital Advisor is available to our Spanish-
speaking Members in a Spanish-language format that
is easy to use and understand. The Spanish Language
Hospital Advisor™ also provides access to critical
information on the availability of maternity services,
cardiac procedures and intensive care units. To access
the Hospital Advisor, register for a user name and
password on www.oxfordhealth.com.
Privacy notice concerning financial information
At Oxford, protecting the privacy of the personal
information we have about our customers and Members
is of paramount importance, and we take this responsibility
very seriously. The following notice describes our policy
regarding the confidentiality and disclosure of customer
and Member personal financial information that
Oxford collects in the course of conducting its business.
Our policy applies to both current and former customers
and Members.
The information Oxford collects
We collect non-public, personal financial information
about Members from the following sources:
• Information we receive from you on applications or
other forms (e.g., name, address, Social Security
number, and date of birth)
• Information about your transactions with us, our affiliates (companies under common ownership with, controlled by, or owned by Oxford) or others
• Information we receive from consumer reportingagencies concerning large group customers
The information Oxford discloses
We do not disclose any non-public, personal financial
information about our current and former customers
OO X F O R D | B E N E F I T S U P D A T E
19
and Members to anyone except as permitted by law.
For example, we may disclose information to affiliates
and other third parties to service or process an insurance
transaction, or provide information to insurance
regulators or law enforcement authorities upon request.
Oxford security practices
We emphasize the importance of confidentiality
through employee training, the implementation of
procedures designed to protect the security of our
records, and our privacy policy. We restrict access to
personal financial information of our customers and
Members to those employees who need to know that
information to perform their job responsibilities. We
maintain physical, electronic and procedural safeguards
that comply with federal and state regulations to guard
your non-public, personal financial information.
This notice is being provided on behalf of the following
Oxford affiliates: Oxford Health Plans LLC, Oxford
Health Plans (CT), Inc., Oxford Health Plans (NJ), Inc.,
Oxford Health Plans (NY), Inc., Oxford Health
Insurance, Inc., Investors Guaranty Life Insurance
Company, and Oxford Benefit Management, Inc.
Please note: A copy of Oxford’s Notice of Privacy Practices
can be obtained by logging on to www.oxfordhealth.com.
To request a written copy, please call our Customer Service
Department at the number on your Oxford ID card. You
can also contact us by mail at:
Oxford Health Plans
HIPAA Member Rights Unit
48 Monroe Turnpike
Trumbull, CT 06611
New Jersey primary care physician (PCP)and OB/GYN disenrollment process
If you are a New Jersey Member and your Oxford
PCP or OB/GYN is disenrolled from Oxford’s provider
network, we will provide you with a 30-day advanced
written notification. The notification will inform you of
the disenrollment date and advise you of the procedures
for selecting a new participating PCP or OB/GYN.
Please note: Advance notice is not required if your
PCP or OB/GYN is terminated due to quality of care
concerns, fraud or breach of the Oxford participating
provider agreement.
N E W S Y O U C A N U S E20
New Jersey Independent ConsumerSatisfaction Survey results
If you are a New Jersey Member and would like to
request New Jersey Independent Consumer Satisfaction
Survey results and an analysis of quality outcomes of
healthcare services of managed care plans in the State
you may contact:
Office of Health Care Quality AssessmentNew Jersey Department of Health and Senior ServicesP.O. Box 360Trenton, NJ 08625-03601-800-418-1397
Oxford’s radiology network Radiology services, such as MRI, PET scans and CT
scans, are some of the most expensive services in health-
care today. Fortunately, Oxford has contracted with
numerous freestanding radiology facilities. We require all
freestanding radiology facilities to be accredited by the
American College of Radiology. If you are in need of a
radiology procedure, such as an MRI, PET or CT scan,
ask your doctor about Oxford participating freestanding
facilities nearby. Because a freestanding facility does not
share the same overhead as a hospital, generally the cost
per service is less than the cost charged by a hospital.
Chest x-ray policy updateSeveral medical professional associations, including the
American College of Chest Physicians, the U.S. Preventive
Services Task Force, the National Cancer Institute, and
the American Cancer Society, have concluded that chest
x-rays for screening should not be a part of a routine
periodic physical examination. Please be aware that,
as of July 1, 2004, chest x-rays performed routinely
for screening purposes as part of a periodic health
maintenance examination by your PCP in the absence
of symptoms, signs or disease states are not covered.
Please note: Oxford will continue to provide coveragefor chest x-rays that are medically necessary based onsymptoms, signs or disease states.
Updated Member Handbooks for New York Members
If you are a New York Member and have coverage
through your employer or purchase individual coverage
directly from Oxford, we would like to inform you
that an updated electronic version of your Member
Handbook is available on www.oxfordhealth.com. The
new Member Handbook may contain some language that
differs from the provisions in your current Certificate of
Coverage and Member Handbook (or your individual
contract) and replaces certain sections of your Certificate
of Coverage.
To request a printed copy, please call our Customer
Service Department at the number on your Oxford ID
card. You can also contact us by mail at:
Oxford Health PlansManaged Care Act Request48 Monroe TurnpikeTrumbull, CT 06611
Oxford cares about qualityOxford Health Plans’ Quality Management (QM)
program is devoted to making sure that you have
access to quality healthcare. Our QM program is led
by an Executive Quality Management Committee and
consists of various regional committees in which QM
staff and network providers participate.
Functions include:
• Identifying the scope of care and services availablethrough Oxford
• Developing clinical practice guidelines (e.g., guide-lines regarding treating heart disease) and servicestandards (e.g., processing precertification requests)to measure performance
• Verifying the medical qualifications of providers who participate in Oxford’s network
• Monitoring and evaluating the quality and appropriateness of the services and medical carereceived by Oxford Members (i.e., via ongoingMember satisfaction surveys)
• Pursuing opportunities to improve patient safety and customer service
• Resolving identified quality issues or concerns
If you would like to request more information about
Oxford’s QM program and goals, please call our
Customer Service Department at the number on your
Oxford ID card.
21
Promoting appropriate careThrough the media or your own research, you may have
become aware that some managed care organizations
offer rewards or bonuses to providers who limit and/or
deny care. Please note that decisions about the care you
receive are based only on appropriateness of care, service
and existence of coverage. Oxford does not compensate
providers for denials of service, nor do we offer incentives
to encourage denials. We do encourage the use of
appropriate care and services to prevent and/or treat
illnesses. For details about your specific benefit coverage,
please refer to your Certificate of Coverage.
Commercial Member rights and responsibilities
As an Oxford Member, you have certain National
Committee for Quality Assurance (NCQA) rights and
responsibilities related to your coverage. The following
information is provided for your reference:
Oxford commercial Members have the right to:• Receive information about Oxford, its services,
its practitioners and providers, and Members’ rights and responsibilities
• Be treated with respect and recognition of their dignity and right to privacy
• Participate with practitioners in decision makingregarding their healthcare
• Have candid discussions about appropriate or medically necessary treatment options for their conditions, regardless of cost or benefit coverage
• Voice complaints or appeals about Oxford or the care provided by participating providers
• Make recommendations regarding the organization’sMember rights and responsibilities policies
Oxford commercial Members have the responsibility to:• Provide, to the extent possible, information that
Oxford and its practitioners and providers need in order to care for them
• Follow the plans and instructions for care that theyhave agreed on with their practitioners
• Understand their health problems and participate in developing mutually agreed upon treatment goalsto the degree possible
In addition to the previously noted information,
Members are also entitled to rights and responsibilities
subject to applicable state law. These rights and
responsibilities are outlined in your Certificate of
Coverage. If you have questions concerning your rights
and responsibilities, please call our Customer Service
Department at the number on your Oxford ID card.
Adopting the latest technologiesNew treatment methods are constantly being developed
for conditions ranging from asthma to skin cancer. The
following information will help you understand how
Oxford evaluates these new medical technologies and
how decisions are made regarding their use.
What is new medical technology? New medical
technology is defined as a newly approved drug or
medication, a new surgical procedure or new medical
equipment. Oxford continually assesses new medical
technologies. Two examples of new medical technologies
that were recently approved for coverage by Oxford are
intranasal influenza vaccine (FluMist™) and the wearable
external cardioverter defibrillator (WCD).
What is the evaluation process? Oxford’s Healthcare
Services Department, led by experienced physicians
representing multiple specialties, is responsible for
evaluating new medical technology. The process begins
with a review of the medical literature and other technical
research. The clinical staff also seeks opinions from
leading physicians and specialists in the community —
providers who have knowledge and expertise regarding
how new medical technology will be used on a day-to-day
basis. Once a thorough review of the available informa-
tion has been conducted, Oxford’s senior medical staff
meets to decide whether or not to cover the new medical
technology. They base their decision on the strength of
the scientific evidence published in medical journals.
Representatives from all department areas then meet to
create a policy that outlines the conditions for which the
technology will be covered. Once the policy is finalized,
front-line Oxford employees are trained regarding
precertification, review, benefit application, and claims
payment. When a new policy is implemented, Oxford
notifies physicians through a quarterly publication called
the Provider Program and Policy Update (PPU) and on
our web site, www.oxfordhealth.com.

N E W S Y O U C A N U S E22
As a Member, you are notified of important new policies
through this News You Can Use section in Healthy Mind
Healthy Body® magazine. All policies are re-evaluated on
a periodic basis.
Access to careWe recognize that timely access to medical services is
important — whether you need a physical, a colonoscopy
or an appointment to be treated for an unexpected illness.
That’s why we’ve developed provider service standards and
regularly monitor our provider network for compliance
with these standards.
As an Oxford Member, you can expect to see a provider
for urgent care within 24 hours, routine symptomatic care
(non-urgent, but in need of attention) within 72 hours or
a regular physical exam within six weeks. Your wait in a
provider’s office or for a response to an after-hours urgent
phone call should be no more than 30 minutes. We also
set standards for the maximum number of appointments
a primary care physician should have scheduled per
hour, and how many patients he or she can care for in
the practice. Measures like these are designed to help
promote quality care.
An important research study*We would like to make you aware of an ongoing research
study called Action to Control Cardiovascular Risk in
Diabetes (ACCORD), which is looking for adults with type
2 diabetes. This eight-year study, sponsored by the National
Institutes of Health, will be conducted at more than 75
medical facilities throughout the United States and Canada.
Currently, about 17 million Americans have been
diagnosed with diabetes, and more than 90 percent of
those cases are type 2 diabetes (formerly called “adult
onset” or “non-insulin dependent diabetes”). People
with type 2 diabetes are more likely experience high
blood pressure and/or high cholesterol than the general
population. In combination, these factors produce a
higher risk of heart disease and stroke.
The ACCORD study will test the best approaches to
lowering the risk of cardiovascular events for patients
with type 2 diabetes, such as heart attack or stroke.
This is not a study of a new medication.
All ACCORD participants will obtain their diabetes
care and medications, as well as cholesterol or high blood
pressure medications from the study at no cost. Study
participants will continue to receive all other medical
care from their current physicians.
If you are an adult with type 2 diabetes and would
like to be considered for this study, or for further
information, please call the ACCORD central recruiting
number for New York/New Jersey at 212-305-6357 or
visit the web site for the Northeastern Network of
ACCORD, www.accord-ne.org.
* This notice is intended for informational purposes only. Oxford is not a sponsor of this study and is not responsible for its conduct. If you have anyquestions or concerns regarding this study, please consult your physician.
2005 Drug Formulary UpdateEffective January 1, 2005, Oxford has transitioned to
UnitedHealthcare’s Prescription Drug List, which impacts
the tier placement of certain drugs. For a complete
listing of the new Prescription Drug List, please log on to
www.oxfordhealth.com. The Pharmacy and Therapeutics
(P&T) Committee reviews new drug products approved
by the Food and Drug Administration (FDA) and reviews
current products when new information becomes
available. Coverage for the listed items may be limited or
excluded based on a Member’s eligibility or plan design.
23
Endocrine drugs
• Anadrol — 50
• Androderm patches
• Androgel
• Android
• Calderol
• Deca Durabolin
• Delatestryl
• Depo Testosterone
• DHT
• Halotestin
• Hytakerol
• Methyltestosterone
• Oxandrin
• Rocaltrol
• Somavert1
• Striant
• Testim
• Testoderm
• Testosterone
• Testred
• Winstrol
• Zavesca1
Growth hormones
• Serostim
OB/GYN drugs
• Lupron (3.75 mg and 11.25 mg)
Dermatological drugs
• Avita2
• Differin2
• Elidel
• Protopic
• Raptiva1
• Retin A2
Gastrointestinal drugs
• Aciphex
• Lotronex
• Nexium
• Prevacid
• Prilosec
• Protonix
• Zegerid
• Zelnorm
Musculoskeletal and
Rheumatological drugs
• Bextra
• Celebrex
• Enbrel1
• Forteo
• Humira
• Kineret
Psychotherapeutic drugs
• Adderall3
• Concerta3
• Desoxyn3
• Dexedrine3
• Dextrostat3
• Provigil
• Strattera
Pulmonary drugs
• Singulair4
Urological drugs
• Caverject
• Cialis
• Edex
• Levitra
• Muse
• Viagra
Vitamins/Nutritional products
• Drisdol
• Hectorol
• Nutritional therapies1
1 For coverage information, Members shouldcall our Customer Service Department at the number on their Oxford ID card.
2 Applies only to Members age 40 or older.
3 Applies only to Members age 19 or older.
4 Applies only to Members age 12 or older.
Medications requiring precertification
To obtain precertification, please have your physician call Medco Health Solutions, Inc. directly at 1-800-753-2851,
Monday through Friday between 8 AM and 9 PM. This list is subject to change without notice. For the most up-to-date
information, please call Pharmacy Customer Service at 1-800-905-0201. Or log on to www.oxfordhealth.com.
Please note: Precertification requirements may vary, depending on the Member’s benefit. O
S P E C I A L T O P I C24
Ways you can help Whether you have personally experienced a profound
loss or not, it’s normal to feel awkward and unsure of
what to do or say when someone else needs your help.
Here are suggestions from the National Mental Health
Association to guide you at such a time:
Listen patiently and compassionately. Allow the
grieving person to talk freely about feelings of loss
without fear of disapproval or embarrassment.
Share your own memories of the deceased, especially
those memories which may shed a new and loving light on
the person remembered.
Be accepting of tears. Tears will almost certainly come
at some point in the grieving process; they are nature’s
way of literally washing away some of the toxic chemicals
associated with emotional stress and restoring a measure
of balance.
Avoid false comfort. Avoid clichés such as “It was for
the best,” “You’ll get over it in time,” “It was God’s will,” or
“At least she isn’t suffering any more.” Don’t say you know
how it feels to have suffered such a loss. For each person
bereavement is a unique experience.
Offer to take over some simple task that might ease the
grieving person’s burdens, and be sure to follow up with
action. It might be helping to sort out business papers or
taking care of a housekeeping chore around the house
for a few weeks.
Remember holidays and anniversaries, when recent
loss is most likely to make people feel isolated and
abandoned. Look for thoughtful ways to share your
home, yourself and your activities in these especially
difficult times.
Pay attention to signs that the grieving person is in
greater distress than he or she can handle. Dramatic
weight loss or loss of appetite, substance abuse, depression,
excessive sleeping, physical problems, personal neglect,
even talk of suicide, should be taken seriously. If you do
not feel close enough to the individual to raise your
concerns directly, tell a friend or family member who is.
HelpingThe death of a loved one understandably generates feelings of loss and
bereavement, but many other changes in life can also cause us to grieve, from
divorce to the estrangement of a child, to the experience of serious illness and
the uncertain future it brings. Grieving is a natural, inescapable response that
engages our entire being — physically, emotionally and spiritually. If someone
you care about is going through this passage, be patient, tolerant and supportive.
Grieving cannot be rushed. It takes everyone time to adjust to new circumstances
and to heal, each in his or her own way, at his or her own pace.

25
When children grieveIt is important to remember that adults aren’t the only ones who
experience grief. Children deal with very similar feelings, and in most cases,
are less equipped to express them. Children typically experience grief in
ways more appropriate to their age and emotional development:
Children younger than age seven perceive death as separation and they
tend to act out their feelings rather than put them in words. They fear being
alone and worry that when other members of the family leave, even for a
short time, that they too, may not return. Youngsters may refuse to go to
school or to daycare for the same reason. Eating, sleeping, bed-wetting, or
temper tantrums may also erupt.
Children between seven and 12 are more likely to view a loved one’s
death as a threat to their personal safety and dwell on fears that they, too,
may die. Some may want to stay close to a protector while others may
withdraw. Some in this age group will act very brave, while others may
be disruptive. Problems with concentration, following directions or carrying
out familiar tasks are not unusual. This older child frequently imagines that
he or she is somehow responsible for the death of the loved one, through
something done or said.
Teenagers, depending on their level of maturity, may grieve much like
adults. Or they may be drawn to dramatic behavior — embracing religion
with a fervor not previously seen or taking on reckless acts as though to defy
death, or even contemplating suicide.
Overwhelming griefWhile most adults adjust well to the changes that bereavement or other
major loss brings, it must be acknowledged that some may feel truly
overwhelmed. Their grief can rise to the level of clinical depression and
post-traumatic stress disorder. For people undergoing the more severe
responses of traumatic grief, the sooner professional counseling is sought
the better. For some, severe suffering may be as natural as other expressions
of loss, but because it undermines a person’s innate capacity to recover,
those who suffer traumatic stress need skilled support on the road to making
a healthful, life-affirming adjustment. Whatever the situation, your support
will likely go far in making a loved one’s experience with grief easier. O
time heal
W E L L N E S S26
When you are young, it usually takes
something as severe as a major sports
injury, a bad fall or a serious car accident,
to break one of your bones. That’s because
young bones are resilient and strong —
almost rubbery. And given proper nutrition,
exercise, favorable genetics, and no major
accidents, they will continue to serve you
well for years to come. But it’s important
to never take your bones for granted.
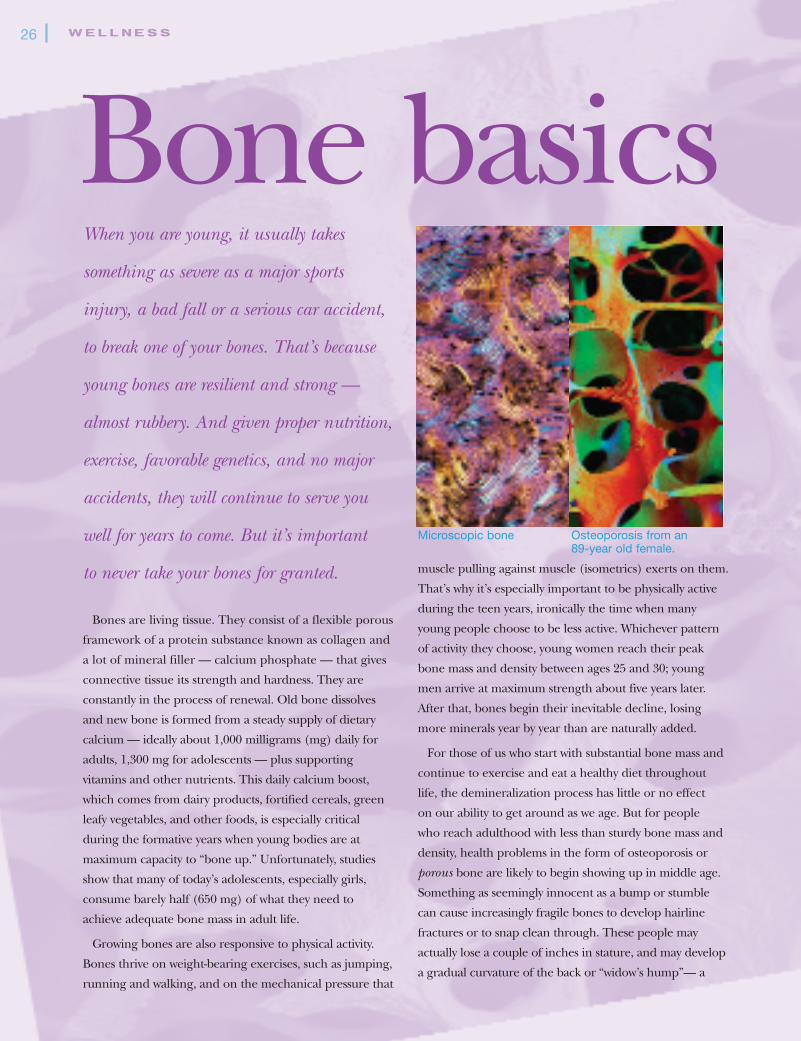
Bones are living tissue. They consist of a flexible porous
framework of a protein substance known as collagen and
a lot of mineral filler — calcium phosphate — that gives
connective tissue its strength and hardness. They are
constantly in the process of renewal. Old bone dissolves
and new bone is formed from a steady supply of dietary
calcium — ideally about 1,000 milligrams (mg) daily for
adults, 1,300 mg for adolescents — plus supporting
vitamins and other nutrients. This daily calcium boost,
which comes from dairy products, fortified cereals, green
leafy vegetables, and other foods, is especially critical
during the formative years when young bodies are at
maximum capacity to “bone up.” Unfortunately, studies
show that many of today’s adolescents, especially girls,
consume barely half (650 mg) of what they need to
achieve adequate bone mass in adult life.
Growing bones are also responsive to physical activity.
Bones thrive on weight-bearing exercises, such as jumping,
running and walking, and on the mechanical pressure that
muscle pulling against muscle (isometrics) exerts on them.
That’s why it’s especially important to be physically active
during the teen years, ironically the time when many
young people choose to be less active. Whichever pattern
of activity they choose, young women reach their peak
bone mass and density between ages 25 and 30; young
men arrive at maximum strength about five years later.
After that, bones begin their inevitable decline, losing
more minerals year by year than are naturally added.
For those of us who start with substantial bone mass and
continue to exercise and eat a healthy diet throughout
life, the demineralization process has little or no effect
on our ability to get around as we age. But for people
who reach adulthood with less than sturdy bone mass and
density, health problems in the form of osteoporosis or
porous bone are likely to begin showing up in middle age.
Something as seemingly innocent as a bump or stumble
can cause increasingly fragile bones to develop hairline
fractures or to snap clean through. These people may
actually lose a couple of inches in stature, and may develop
a gradual curvature of the back or “widow’s hump”— a
Bone basics
Microscopic bone Osteoporosis from an 89-year old female.

27
condition that can cause chronic discomfort and back pain. Other
circumstances can also set the stage for frequent fractures as people
age. Certain disorders such as type 1 diabetes, as well as gastrointestinal
diseases, can interfere with absorption of calcium and weaken bones.
While any bone break can be a nuisance, the consequences of hip
injury — far and away the most common location in older people —
can go well beyond the bother of wearing a temporary cast. Hip
fractures most often occur at the upper end of the femur or thighbone
where it fits into the pelvic hip socket. Repair typically involves invasive
surgery to align and pin the sides of the break. Severely damaged bone
may require partial or total hip replacement with artificial parts. The
surgery and short hospital stay usually go smoothly. Fully successful
recovery depends to a large degree on the ability of the patient to carry
out the demanding rehabilitation that follows, which usually entails an
extended period of supervised exercise and physical therapy at a live-in
rehabilitation center. Patients may also have to adopt new nutritional
patterns and other habits that support better health.
Is there anything to be done to reduce your risk of fragile bones?
Absolutely. Ideally, begin when you are young, and do what it takes
to keep your bones as strong as possible. If you have children, pay
close attention to their stepped up nutritional needs, and as they
become old enough to understand, remind them regularly why good
nutrition and exercise really matter. For your own bone health, include
recommended levels of calcium appropriate to your age and health
in your diet, and ask your primary care physician (PCP) if you should
take supplemental calcium and Vitamin D. (See Do you know your
A-B-Cs? on page 10.) Also, know your individual risk for osteoporosis
before it develops. Your PCP has reliable methods of predicting risk
and screening for bone density in your 30s or 40s; if you turn out to
be at high risk, your PCP may recommend you take one of the
therapeutic drugs available — including Fosamax®, Actonel® and
Evista® — that slow and, in some cases, stop continued bone loss.
Calcitonin, an injectable natural hormone that enhances bone
formation, is another option for some patients.
With a little attention, your bones will carry you into your golden
years without trouble. But remember, when it comes to bone health,
the sooner you begin treating your bones with the respect they
deserve, the better. O
Osteoporosis facts
and f igures
• Over 44 million Americans have osteoporosis,68 percent of them women
• Incidence increases dramatically with age;between ages 55 and 64, 16 percent ofwomen tested have some degree of bonefragility; over 65 the incidence rises to 35 percent and upwards with increasing years;bone loss is most rapid in the first few yearsafter menopause
• One in two women and one in four men over50 will have an osteoporosis-related fracturein their lifetime
• Osteoporosis is responsible for more than 1.5million fractures annually, including 300,000hip fractures, 700,000 vertebral fractures,250,000 wrist fractures, and more than300,000 fractures at other sites
• Risk factors vary with age, gender and ethnicity; small, thin-boned older Caucasianand Asian women are at highest risk; so are people who lose two or more inches inheight as they age, people whose posturetends to be bent with aging, or who have afamily history of osteoporosis or frequent bone breaks; people whose diets are low in calcium, who smoke, who consume alcohol to excess, who are inactive physically, whomust undergo extended bed rest, who havehad eating disorders such as anorexia andbulimia, or who use certain therapeutic medications such as corticosteroids, are also at higher risk
Sources: National Osteoporosis Foundation, The NationalInstitutes of Health and The U.S. Food and Drug Administration
OOX F O R D I N F O
Oxford Members can take advantage of discounted memberships to theWellQuest network of fitness facilities through Oxford’s Healthy Bonus®
program. A WellQuest membership includes a consultation with a fitnessinstructor, and access to Miavita, an online nutrition guidance program. To find out more about WellQuest, including a listing of participating facilities in your area, visit www.wellquestonline.com, or call 1-800-595-8448.

P.O. Box 7081, Bridgeport, CT 06601
HMHBSP/7858
PRESORTED STANDARD
U.S. POSTAGE
PAID
ONWARD PUBLISHING INC.
importantinformation
insideCheck out the latest news
about your Oxford coverage
in the Benefits Update section
of this issue and start
making the most of
your health plan.
CUSTOMER SERVI CE 1-800-444-6222 (8 AM - 6 PM, Monday through Friday)To reach a Service Associate, please call the toll-free Customer Service number on your Oxford ID card, or call 1-800-444-6222. For an interpreter for the hearing impaired, you may call Oxford’s TTY/TDD hotline at 1-800-201-4875. Please call 1-800-303-6719 for assistance in Chinese, 1-888-201-4746 for assistance in Korean, 1-800-449-4390 para ayuda en Español, or the number on your Oxford ID card for assistance in other languages.
OXFORD ON-CALL® 1-800-201-4911 (24 hours a day, seven days a week)Registered nurses offer you healthcare guidance, around the clock.
PHARMACY CUSTOMER SERVICE LINE 1-800-905-0201 (24 hours a day, seven days a week)* Receive answers to your questions about pharmacy benefits, claims, prescriptions, and participating pharmacies in your area.
MEDCO BY MAIL™ 1-800-905-0201 (24 hours a day, seven days a week)* This mail-orderpharmacy service provides a cost-effective, convenient way for Members with a mail-order prescription benefit to order certain maintenance medications.
OXFORD EXPRESS ® 1-800-444-6222 (24 hours a day, seven days a week)Touch-tone phone options let you confirm eligibility, check the status of a claim, request a new Oxford ID card or physician roster, and more.
OXFORD’S FRAUD HOTLINE 1-800-915-1909 (24 hours a day, seven days a week)If you suspect healthcare fraud on the part of Members, employers or providers, please call our confidential fraud hotline.
DIABETES PROGRAM LINE 1-800-665-4686 (8 AM - 4:30 PM, Monday through Friday)Oxford offers educational materials to help Members with diabetes understand their condition and become active participants in its management.
BEHAVIORAL HEALTH LINE 1-800-201-6991 (8 AM - 6 PM, Monday through Friday)Behavioral Health Coordinators provide information such as referrals to behavioral health providers or precertification for mental health or substance abuse services.
ASTH MA PROGRAM LI N E 1-800-665-4686 (8 AM - 4:30 PM, Monday through Friday)Learn about asthma triggers, how to avoid them and the importance of taking appropriate medication(s).
RESOURCES ON THE INTERN ET AT www.oxfordhealth.com
MY OXFORDSM
Log in with your user name and password to access your policy and benefit information, and perform transactions such as checking claims’ status, selecting a primary care physician and ordering materials and Member ID cards.
WELLNESS RESOURCES
Learn more about Oxford’s various wellness resources, such as our Healthy Bonus® program and Self-Help LibrarySM by logging in to our Member web site.
*Except Thanksgiving and Christmas.
OO X F O R D C O N T A C T I N F O