healthy behaviour, food safety and quality policy comparison fin
TRANSCRIPT

HEALTHY LIFESTYLE, FOOD SAFETY AND QUALITY – POLICIES OF INDONESIA, GHANA,
TANZANIA AND ZIMBABWE
1

GROUP MEMBERS
Pinta LiztiIrene
(Indonesia)
Sophia D. Amenyah
(Ghana)
Josephine T. Kimario
(Tanzania)
Genesis Chevure
(Zimbabwe)
2

OBJECTIVES OF POLICY REVIEW
• Understand current situation of healthy lifestyle, food quality and safety issues
• Reveal and compare ongoing policies in addressing healthy lifestyle, food quality and safety issues.
• Assess quality of policies.
• Delivering recommendation for future policy development.
3

CONTENT
Introduction
Countries Nutrition Situation
Policy Implementation
Policy Comparison
Policy Assessment
Recommendation

INTRODUCTION
Food Safety: all those hazards, whether chronic or acute, that may make food injurious to the health of the consumer. (FAO, 2001)
Food Quality: the totality of features and characteristics of a product, process or service that bear on its ability to satisfy stated or implied needs (Standard ISO 9000:2000), excellence.
Healthy Behaviour: behavior patterns, actions and habits that relate to health maintenance, to health restoration and to health improvement (Gochmann, 1997)
5

RATIONALE BEHIND POLICIES
Protecting public health by reducing risk of underweight and food borne illness, especially for vulnerable groups.
Protecting consumers from unsanitary and unwholesome food.
Promoting healthy body and preventing illness of population.
6

COUNTRIES NUTRITION SITUATIONGhana
• High levels of communicable and pregnancy-related diseases and rising non communicable diseases.
• Malnutrition including under-nutrition in children of poor families, micro-nutrient deficiency in children and pregnant women.
• Over nutrition in adults is known to be underlying the high levels of morbidity and mortality in the country.
Indonesia• Low knowledge and responsibility
from small-scale food producer and low awareness of consumer regarding food quality and safety.
• 9.08-10.23% of food product do not pass food standard.
• 128 reported cases of foodborne diseases in 2011.
• 48.2% of population do not exercise physical activity regularly.
• 93% of population consume fruit and vegetable less than recommended daily amount
7

Tanzania
• High level of stunting, wasting, and underweight children (35%, 4% and 16% respectively).
• High number of children suffered from anaemia (69%).
• Double burden of malnutrition in women (Underweight 11%, Obesity and overweight 22%).
• Only 50% of productive woman gives exclusive breastfeeding.
Zimbabwe
• High level of underweight, stunting, and wasting children (between 30%, 5% respectively)
• Iron and vitamin A deficiency (30 &27% respectively)
• Exclusive breast feeding 45%
• HIV prevalence 5.5%,
• Infant mortality rate 37/1000 births,
• 8% food products are substandard,
• 30% do not do exercise regularly.
8
COUNTRIES NUTRITION SITUATION

POLICY IMPLEMENTATION
HEALTHY LIFESTYLE AND BEHAVIOUR
9

INDONESIA
Strategies• Conducting socialization in the villages to head of villages and chief of local
organizations.
• Collecting the data in each household based on 10 indicators of healthybehaviour in family program.
• Mapping the family based on existence of 10 indicators.
• Planning the problem priority, objectives, intervention, and schedule ofintervention.
• Conducting the intervention with full support by community leaders.
• Monitoring and evaluation the impact of intervention to the indicators.
• Providing awards to the three best villages based on the scoring indicators.
10
• Empower family to practice healthy behaviour and to be actively involved in healthy action in society.
Policy Objectives

Main Actors
Ministry of Health
Private company (CSR Program)
Department of Health, local hospital, local
organizations
• Monitoring using 10 healthy behaviour indicators
• Conducted every year
Monitoring and
Evaluation
11

GHANA
Strategies
• Empower individuals, households and communities to makeinformed choices for their health through provision ofinformation, education and creation of an enabling environment.
• Develop standards for housing and introduce frequent inspectionsaccompanied by sanctions for constructing new houses withoutadequate sanitary facilities.
• Ensure access to safe water and sanitation.
• To promote healthy lifestyles and reduce risk factors of that arise from environmental, economic, social and behavioural causes
Policy Objectives
12

Strategies
• Facilitate the adoption of healthy lifestyles among students through the curriculum, physical education, environmental sanitation and the promotion of healthy eating
• Promote healthy eating programmes in schools and in communities by introducing nutritional education into the school curriculum
• Set up model regenerative health and nutrition facilities as training centres to facilitate changes in lifestyle
• Promote physical exercise, rest and recreation by making physical education mandatory in all schools and making recommendations for adults.
• Ensure adequate levels of funding of health promotion and nutrition in the health budget
13
• Ministry of Health, Ghana Education Service, Local Government, Community Leaders, Town and Country Planning, Rural Development Agencies, Ministry of Employment, National Labour Commission, the Media
Main Actors
• Participatory planning and monitoring process involving relevant stakeholders
• Peer review of cross-sectorial assessment of the implementation
• Periodic evaluation based on annual reviews
Monitoring and
Evaluation
14
TANZANIA
Strategies
• Advise women of reproductive age and other caregivers on how to improve dietary intake for themselves and their young children, including the consumption of low-cost locally available foods and fortified foods, where available and affordable
• Protect appropriate infant and young child feeding practices
• Increase access to quality nutrition services at the community and facility level
• Enhance the nutrition behaviours of women, caregivers, family and community members who influence them
• Strengthen quality of nutrition services
• Integrate nutrition interventions and health services
Policy Objectives
15

• Educate school children and caregivers about the importance of nutrition and options for improving dietary intake.
• Promote food preparation and processing technologies that increase bioavailability and absorption of vitamins and minerals.
• Increase the dietary intake of vitamins and minerals, and include supplementation, fortification, and dietary improvement
• Provision of nutritional care of persons living with HIV and AIDS (PLHIV) and the prevention of mother to child transmission (PMTCT) of HIV.
• Strengthen household food security by mobilizing action to improve household food production, harvest and post-harvest handling, storage and preservation, food processing and preparation, animal husbandry and fishery .
16

• Public sector, Research institutes, Higher learning and training institutions, Professional, Private sector, Development partners, Civil society, media and the community
Main Actors
• Participatory through nutritional surveillance, health management information system, periodic surveys and other routine and non-routine data systems
• Periodic evaluation/revision based on the annual review/Joint Health Sector Review
• Mid-term and Post Evaluations
Monitoring and
Evaluation
17

ZIMBABWE
Strategies:
• Country-wide campaigns to educate the people so that they will make informed choices of healthy living.
• Introducing health education in schools and training institutions.
• Providing physical education and sporting facilities in villages and communities and encouraging people to utilise them so as to maintain a healthy lifestyle.
• Making it compulsory for every firm and industry to have the environmental management departments to ensure a pollution free environment.
• To ensure availability of funding to cover logistics costs.18
• To promote healthy living and behaviourPolicy
Objectives

19
• Ministries of Labour and Social Welfare, Health and Child Welfare, Education, Sports and Culture and Agriculture, Standards Association of Zimbabwe
Main Actors
•Periodic monitoring •Active participation across board•Periodic evaluation annually
Monitoring and
Evaluation

POLICY IMPLEMENTATION
FOOD SAFETY AND QUALITY
20

INDONESIA
Policy Objective
To educate school community about safe and nutritious school food and to increase the quality, safety and
nutrition of school food.
Strategies
• Strengthening existing school food programmes
• Increasing awareness of school food community
• Increasing capacity of school caterers in creating healthy and nutritious food.
• Modeling and replication of ideal school canteens
• Optimizing management of the program.
21
Schools Community Food Vendors
Department of HealthNational Agency of Food and
Drug Control , Ministry of Health
Stakeholders
Monitoring and Evaluation
• Conducting sampling and laboratory testing on school food to check for its safety and quality.
• Using increment percentage of school food which passed food safety standard.
22

GHANA
• To enact and enforce legislation regarding food and food standards to ensure enabling environments for healthy lifestyles.
Policy Objective
• Developing and enforcing standards for the production, storage, sale and handling of food and drinks in markets, restaurants and other vendors
• Promoting the adoption of standards and regulation of the health and food industry
Strategies
23

Main ActorsFood and drugs
authority
Food vendors and restaurants
Ministry of trade and industry
Ghana Standards Authority
Ghana Police Service
Association of Ghana industries
Monitoring and Evaluation
Participatory planning process involving relevant sectors and stakeholders
Peer review of cross-sectorial assessment of the implementation
Periodic evaluation based on annual reviews24

TANZANIA O
bje
ctiv
es
Create measures to prevent unethical
marketing of breast milk substitutes
Ensure adequate labelling and quality of products for
infant and child feeding
Provide Tax-exemption of commodities for nutrition
and food fortification
Strategies
Strengthen implementation, monitoring and legislation
enforcement
Developing regulations, standards and guidelines to support the implementation
of legislation
25

Main Actors
Government institutions
Research institutes and institutions of training and
higher learning
Private sector and development partners
Civil society, the media and the communities
Monitoring and Evaluation
Nutrition surveillance, HMIS, periodic surveys, routine and non-routine data collection
Periodic evaluation/revision based on the annual review
26

ZIMBABWE
27
• To ensure all food meets national public health legislation and international standards for quality and safety
Policy Objectives
Strategies
• Putting legal standards in place to control production, processing, storage, handling and trade in food
• Awareness campaign to educate people so they make informed choices with their food consumption.
• Making nutrition education compulsory in schools and tertiary institutions
• Ensuring availability of adequate funding
28
Main Actors
Ministry of Health and Child Welfare, Local government,Community leaders, business community, Office of thePresident and Cabinet, Ministry of Food Agriculture, Foodand Nutrition Council of Zimbabwe
Monitoring and evaluation
- Periodic monitoring
- Active participation across board
- Periodic evaluations annually
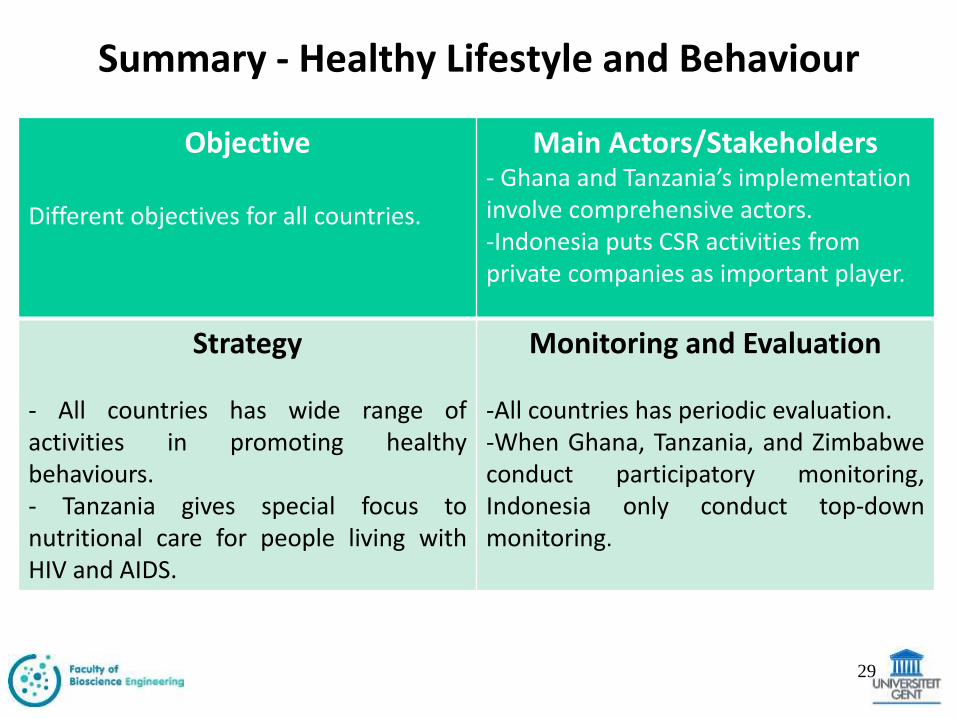
Summary - Healthy Lifestyle and Behaviour
Objective
Different objectives for all countries.
Main Actors/Stakeholders- Ghana and Tanzania’s implementation involve comprehensive actors.-Indonesia puts CSR activities from private companies as important player.
Strategy
- All countries has wide range ofactivities in promoting healthybehaviours.- Tanzania gives special focus tonutritional care for people living withHIV and AIDS.
Monitoring and Evaluation
-All countries has periodic evaluation.-When Ghana, Tanzania, and Zimbabweconduct participatory monitoring,Indonesia only conduct top-downmonitoring.
29

Summary - Food Safety and Quality
Objective
-All countries in Africa focus onlegislation, while Indonesia focus onimplementation.-Different target focus. Ghana targetswhole population, Zimbabwe targetsvulnerable family, Indonesia targetsschool community.
Strategy
Ghana and Tanzania focused indeveloping and enforcingimplementation of legislation. WhileIndonesia focuses in awareness andcapacity increment.
Main Stakeholder
All countries involve governmentagencies that responsible in health,food, and drugs and private sector.
Monitoring and Evaluation
-All countries conduct yearly periodicevaluation to review target fulfillment.-Indonesia specifically conductssampling and laboratory checking forfood safety and quality.
30

COMPARISON OF POLICIES
31

Healthy Lifestyle and Behavior
Indonesia Ghana Tanzania Zimbabwe
Policy Status
On-going On-going On-going On-going
Target Productive couple, pregnant and breast-feeding mother, children, teenager, adult, elderly people, baby sitter
General population, with specific strategies targeting various sections of the population such as children, pregnant women etc.
General population but more attention to children and women
General population
Source of funding
Indonesian Government and Private Company
Ghana Government Tanzania Government, Development Partners, national and international NGOs, CBOs, FBOs
Zimbabwe Government
32

Food Safety and Quality
Indonesia Ghana Tanzania Zimbabwe
Policy Status
On-going On-going On-going On-going
Target Student, student’s parent, teachers, street food vendor, canteen staffs
General population
General population General population
Sourceof Funding
IndonesiaGovernment
Ghana Government
TanzaniaGovernment,Development Partnersnational and international NGOs, CBOs, FBOs
Zimbabwe Government
33

ASSESSMENT OF POLICIES
34

Healthy Lifestyle and Behaviour
Indonesia Ghana Tanzania Zimbabwe
Clear objectives Clearly stated Clearly stated Clearly stated Clearly stated
Quantifiable indicators Present Absent Present Absent
Orderly, well-defined
processes
Yes Yes Yes Yes
Sufficient funding to
implement
Insufficient Sufficient Insufficient Insufficient
Stakeholder
Recognition and
cooperation
Defined expectations
Yes
Not well defined
Yes
Well defined
Yes
Well defined
Yes
Not well defined
Monitoring and
Evaluation Process
Yes for periodical
monitoring
Yes, evaluation
planned but not yet
carried out
Yes, on-going Yes, on-going
35

Food Safety and Food Quality
Indonesia Ghana Tanzania Zimbabwe
Clear objectives Clearly stated Clearly stated Clearly stated Clearly stated
Quantifiable indicators
Present Absent Present Absent
Orderly, well defined processes
Yes Yes Yes Yes
Sufficient funding to implement
Insufficient Sufficient Insufficient Insufficient
Stakeholder Recognition and cooperation Defined expectations
Yes
Not well defined
Yes
Well defined
Yes
Well defined
Yes
Not well defined
Monitoring and Evaluation process
Yes for periodical
monitoring
Yes, evaluation
planned but not
yet carried out
Yes-ongoing Yes –ongoing
36

IndonesiaWeaknesses
• Low number of medical assistant in remote areas.
• Limitation of clean water and proper sanitation in remote areas.
• Limited area coverage for policy implementation
• Limited number of school canteens available
• Low enforcement of food safety laws with regard to vendors
37
Strengths
• Well-planned policy.
• Practicing participatory process that involves target group directly.

Ghana Strengths
• Demonstration of political will by allocating specific budget for implementation of policy.
• Involvement of main actors and stakeholders from planning until implementation and evaluation stages.
• Environmental modifications included to support behaviour change
• Use of multifaceted strategies which shows the complexity of nutrition problems
Weaknesses• No quantifiable indicators
stated.
• No review and update of policy during implementation
• Capacity to evaluate may be limited
• Impact may be difficult to determine since lifestyle changes may take long periods to manifest
38

Tanzania Strengths
• Clearly stated objectives.
• Quantifiable indicators stated
• Involvement of multiple stakeholders in the implementation of nutrition activities in the country, including the public sector
Weaknesses• Limited financial resources
for nutrition from government and development partners
• Few health facilities provide the full set of nutrition interventions
• Inadequate linkages between health facilities, communitiesand referral systems
• Policies, standards and guidelines in nutrition not fully used at implementation level 39
Zimbabwe
Strengths
• High literacy level which makes it easy to educate the population about the policies.
• Good infrastructure.
Weaknesses• Political instability
• Inadequate budgetary support especially without donor funding.
40

RECOMMENDATIONS • Policies should be based on local context and evidence.
• Policy planning should be participatory and involve stakeholders to ensure effectiveness.
• Policy makers and governments should be committed to policy implementation.
• In order ensure sustainability, policies should be more focused on improving individual self-efficacy for healthy lifestyles.
• Local funding should be sourced in order to ensure implementation of locally relevant policies.
• Improvement in general infrastructure to support policy implementation.
• Evaluation should play a critical role in policy development and implementation to ensure the creation of more effective policies in the future
• Importance to bridge the gap between the research community and policymakers.
41

REFERENCESJOURNAL/ BOOK
• FAO. (2001). Assuring Food Safety And Quality. http://www.who.int/foodsafety/publications/capacity/en/Englsih_Guidelines_Food_control.pdf
• D S Gochman (Ed), (1997). Handbook of Health Behavior Research New York, Vols. 1–4: Plenum.
GHANA
• Ghana National Health Policy- Creating Wealth through Health
• Ghana Ministry of Health: http://www.moh-ghana.org/
• Ghana Health Service : http://www.ghanahealthservice.org/
42

INDONESIA
• Food and Nutrition National Action Plan Year 2011-2015
• Strategic Plan of Ministry of Health Year 2009-2014
• Strategic Plan of National Agency of Food and Drug Control Year 2009-2014
• Government Institution Performance Accountability Report of National Agency of Food and Drug Control Year 2013
• Guideline of Assessment and Development of Healthy and Clean Behaviour in Household
• Yearly Report of National Agency of Food and Drug Control Year 2013
• Indonesia Health Profile Year 2012
43
REFERENCES
TANZANIA
• Nutrition Country Paper – The United Republic of Tanzania (Draft) The National Road Map Strategic Plan to Accelerate Reduction of Maternal, Newborn and Child Deaths in Tanzania 2008 - 2015
• The United Republic of Tanzania: National Nutrition Social and Behaviour Change Communication Strategy July 2013 – June 2018
• The United Republic of Tanzania: National Nutrition Strategy JULY 2011/12 –JUNE 2015/16
ZIMBABWE
• Zimbabwe Vulnerability assessment Committee (ZIMVAC) 2013, http://reliefweb.int/sites/reliefweb.int/files/resources/2013%20ZimVAC%20DRAFT%20REPORT.pdf accessed on 05 October 2014
• Zimbabwe Food Security Issues Paper for Forum for Food Security in Southern Africa, http://www.odi.org/sites/odi.org.uk/files/odi-assets/publications-opinion-files/5613.pdf accessed on 11 October 2014
44
REFERENCES

• Ms K. Mukudoka (2013) Intersectoral Coordination for Scaling Up Nutrition in Zimbabwe- The Food and Nutrition Security Policy in the context of Economic Growth and Development http://www.fao.org/fileadmin/user_upload/wa_workshop/PPT_SA/DAY3_SUNZimbabwe.pdf accessed on 23 October 2014
• Zimbabwe: Achieving Household and National Food Security, http://siteresources.worldbank.org/EXTMULTIDONOR/Resources/Findings2-Food-security.pdf accessed on 23 October 2014
• Ministry of Health and Child Welfare (2014), The National health Strategy for Zimbabwe (2009-2013): Equity and Quality in Health, A people’s right http://www.zadhr.org/national-documents/53-zim-health-policy.html accessed on 25 October 2014.
• Zimbabwe National Nutrition Survey 2010, http://www.zadhr.org/national-documents/103-zimbabwe-national-nutrition-survey-2010.html accessed on 25 October 2014
45
REFERENCES

46