hand and upper extremity trauma common - ucsf cme .pdf · 3/21/2009 1 hand trauma scott l. hansen,...
TRANSCRIPT
3/21/2009
1
Hand TraumaHand Trauma
Scott L. Hansen, M.D.Chief, Hand and Microvascular SurgeryUniversity of California, San Francisco
OverviewOverview• Hand and upper extremity trauma common
– MVA’s, PVA
– GSW’s– Work related
• Table saw• Knife• Crush
Hansen 2009
OverviewOverview
• Hand Injuries– Fingertip and Nail bed injuries
– Soft-tissue reconstruction– Tendon injuries
– Fractures and dislocations
– Amputations and replantation
Hansen 2009

3/21/2009
2
Evaluation: HistoryEvaluation: History• Age, handedness,
occupation• Past medical history• History/Mechanism of
Injury• History of previous
injuries/treatment• Tetanus vaccination
status
Hansen 2009
Evaluation: Physical examEvaluation: Physical exam
• Skin/Nail bed integrity• Neurologic evaluation
– Light touch, 2-point discrimination
• Capillary refill, pulse• Flexor, extensor tendon function
– ROM
• Ligaments (laxity)• Hand/Forearm compartment evaluation
Hansen 2009
Defect AssessmentDefect Assessment• Soft-tissue
– Skin and subcutaneous tissue
• Tendon• Ligaments
• Nerve• Vascular
• Bone
Hansen 2009
• Evaluation: X-ray – 3 views of the hand and wrist– Fracture pattern– Fracture alignment

3/21/2009
3
Fingertip and Nail Bed InjuriesFingertip and Nail Bed Injuries
• 6 Million ER visits
• 12 million office visits
• 90 million days restricted activity
• 16 million days lost
• 10 billion dollars
American Association for Hand Surgery
Hansen 2009
Healing / Secondary IntentionHealing / Secondary Intention• Advantage
– Pulls innervated pulp into wound
• Disadvantage– Duration of healing
• Consider for small wounds <1cm, – Distal, volar, without bone
Hansen 2009
Superficial Pulp InjuriesSuperficial Pulp Injuries
• Skin graft– Full thickness = less contraction, increased sensibility
Hansen 2009
Fingertip Injuries: Goals Fingertip Injuries: Goals
• Preserve sensation• Maximum functional length• Prevent joint contractures• Soft-tissue coverage• Bony fixation• Satisfactory appearance
Hansen 2009
3/21/2009
4
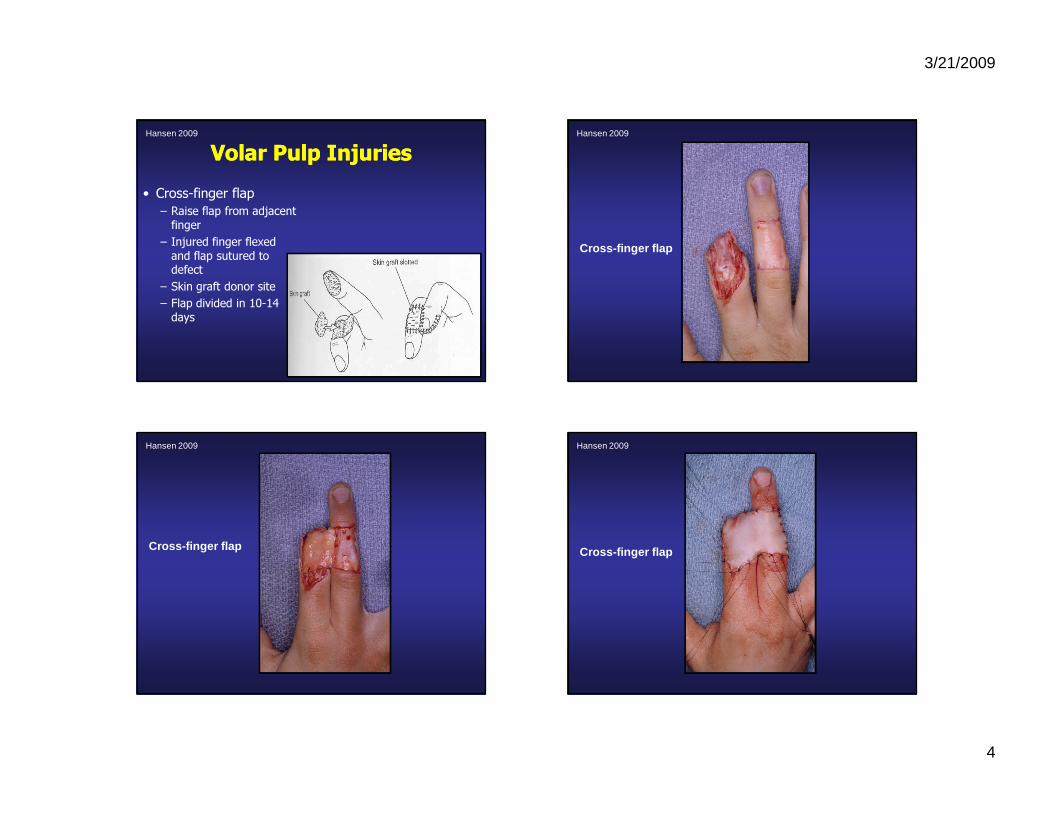
Volar Pulp InjuriesVolar Pulp Injuries• Cross-finger flap
– Raise flap from adjacent finger
– Injured finger flexed and flap sutured to defect
– Skin graft donor site– Flap divided in 10-14 days
Hansen 2009
Cross-finger flap
Hansen 2009
Cross-finger flap
Hansen 2009
Cross-finger flap
Hansen 2009
3/21/2009
5
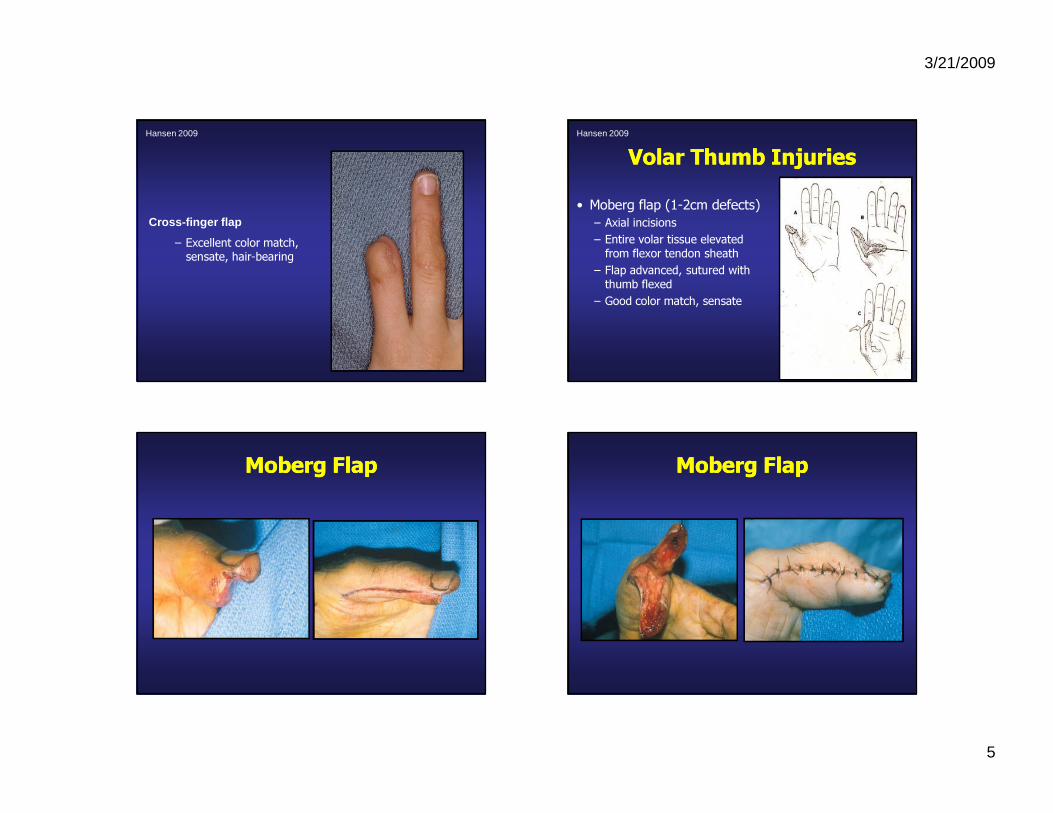
Cross-finger flap
– Excellent color match, sensate, hair-bearing
Hansen 2009
Volar Thumb InjuriesVolar Thumb Injuries• Moberg flap (1-2cm defects)
– Axial incisions – Entire volar tissue elevated from flexor tendon sheath
– Flap advanced, sutured with thumb flexed
– Good color match, sensate
Hansen 2009
Moberg FlapMoberg Flap Moberg FlapMoberg Flap

3/21/2009
6
SoftSoft--Tissue ReconstructionTissue Reconstruction
• Local Finger Flaps• Local Hand Flaps• Regional flaps
– Radial forearm flap
• Distant Flaps– Microvascular free tissue transfer
– Toe Transfer
Hansen 2009
Methods of CoverageMethods of CoverageHansen 2009
Hansen 2009
Large Thumb Large Thumb DefectsDefects
Hansen 2009
3/21/2009
7
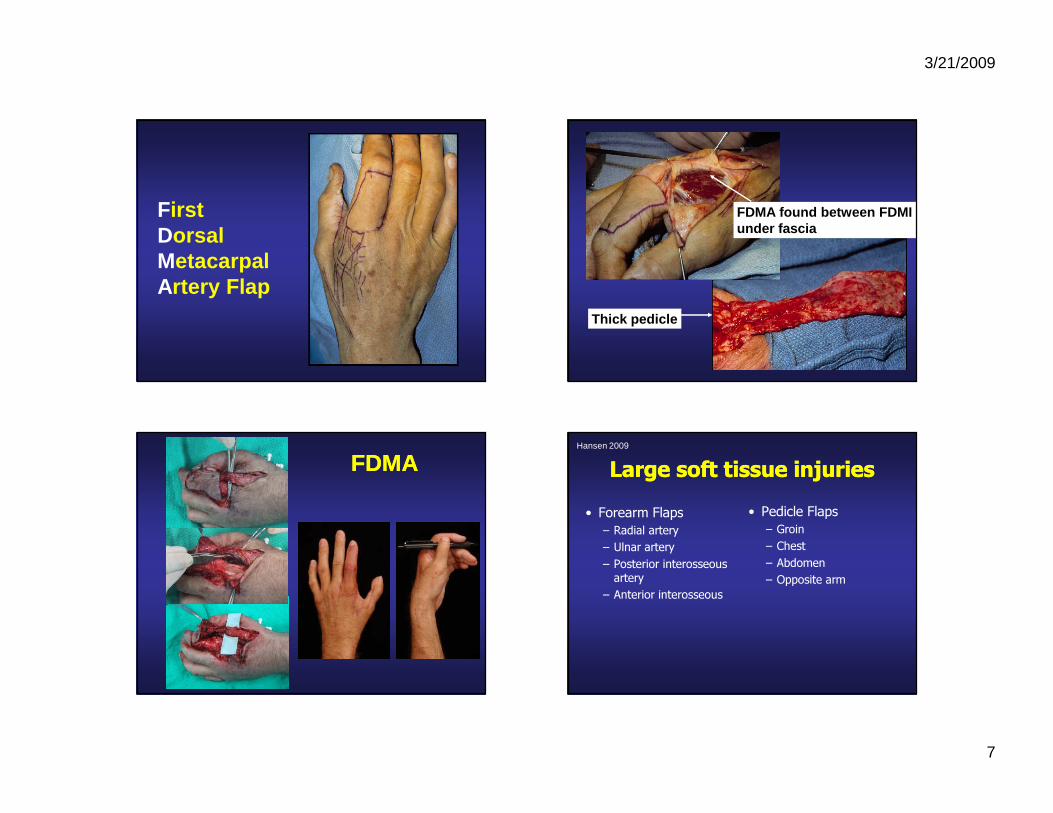
First Dorsal Metacarpal Artery Flap
FDMA found between FDMIunder fascia
Thick pedicle
FDMAFDMA Large soft tissue injuriesLarge soft tissue injuries• Forearm Flaps
– Radial artery – Ulnar artery– Posterior interosseous artery
– Anterior interosseous
• Pedicle Flaps– Groin– Chest– Abdomen– Opposite arm
Hansen 2009

3/21/2009
8
Radial Forearm FlapRadial Forearm Flap- “Workhorse” for hand injuries
- Pedicle or free flap- Antegrade/retrograde flow
- Fasciocutaneous, also tendons, bone, nerves, fascia alone
- Not bulky, reliable- Defect requires STSG
Hansen 2009
Radial Forearm FlapRadial Forearm FlapHansen 2009
Radial Forearm FlapRadial Forearm FlapHansen 2009
Radial Forearm FlapRadial Forearm Flap

3/21/2009
9
Distant Flap: Groin FlapDistant Flap: Groin Flap Distant Flap: Groin FlapDistant Flap: Groin Flap
Groin FlapGroin FlapHansen 2009
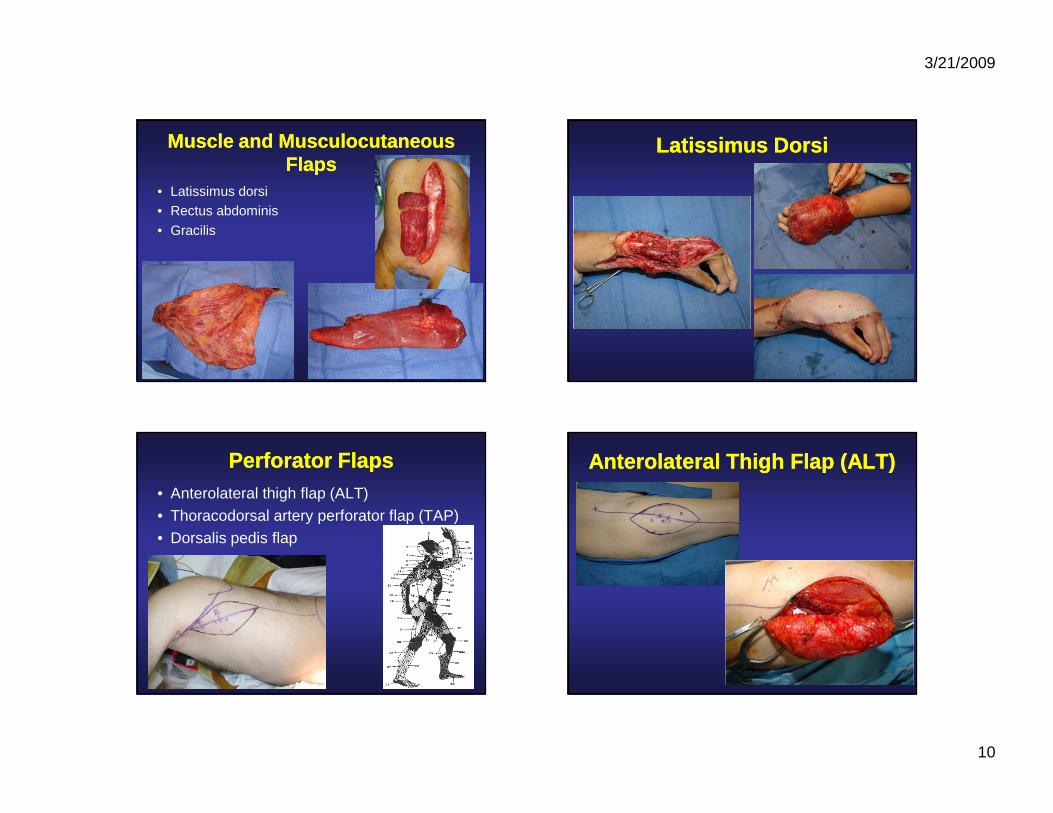
Microvascular Free Tissue TransferMicrovascular Free Tissue Transfer
• Muscle flaps• Musculocutaneous flaps• Perforator flaps• Toe transfer
– Great toe– Second Toe
3/21/2009
10
Muscle and Musculocutaneous Muscle and Musculocutaneous FlapsFlaps
• Latissimus dorsi• Rectus abdominis
• Gracilis
Latissimus DorsiLatissimus Dorsi
Perforator FlapsPerforator Flaps• Anterolateral thigh flap (ALT)• Thoracodorsal artery perforator flap (TAP)• Dorsalis pedis flap
Anterolateral Thigh Flap (ALT)Anterolateral Thigh Flap (ALT)

3/21/2009
11
3/21/2009
12
3/21/2009
13
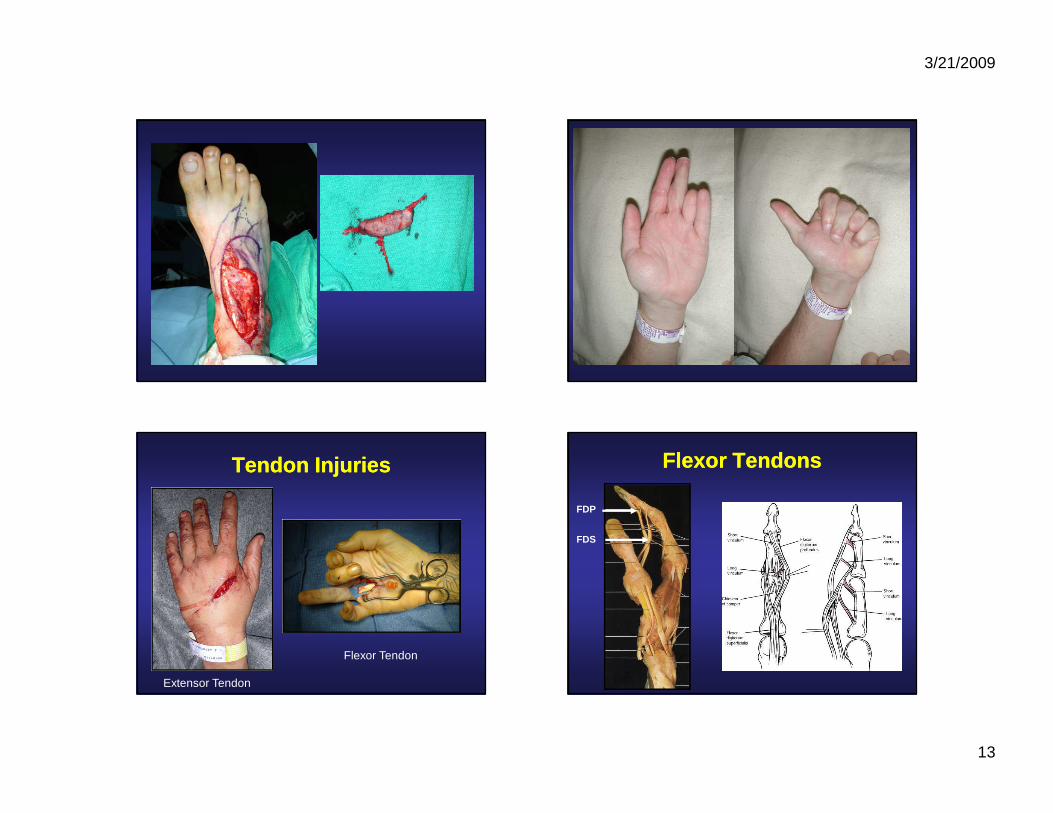
Tendon InjuriesTendon Injuries
Extensor Tendon
Flexor Tendon
Flexor TendonsFlexor Tendons
FDP
FDS
3/21/2009
14
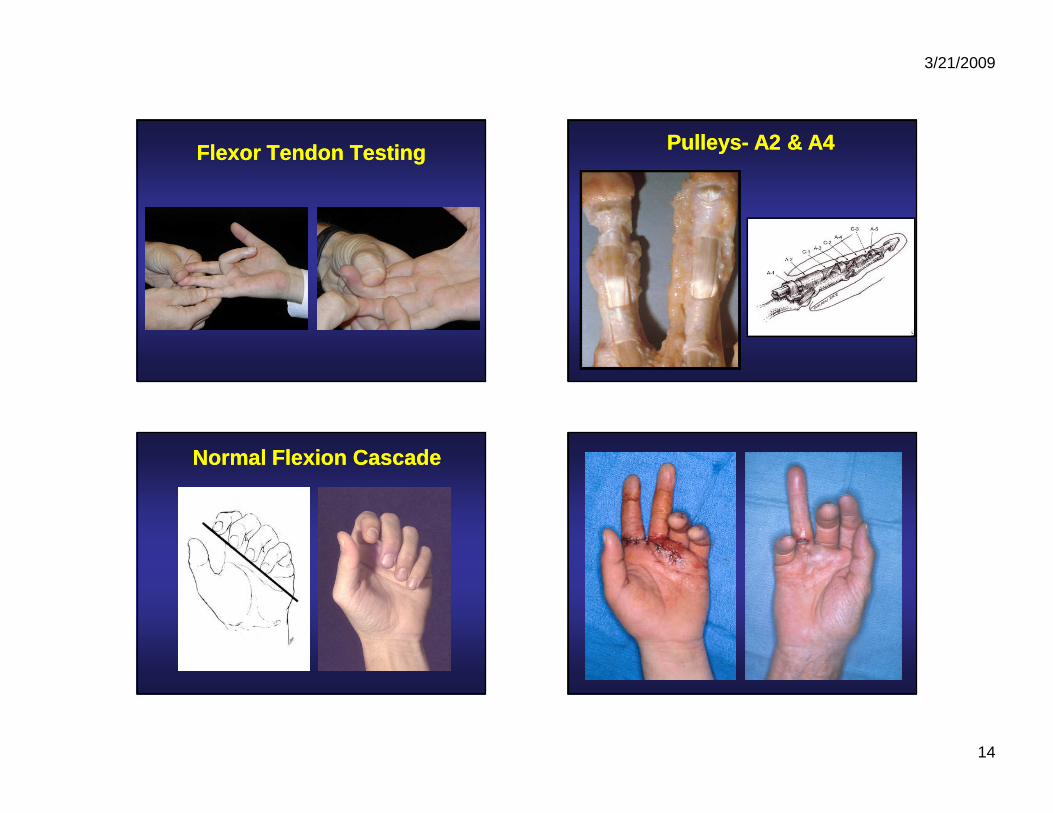
Flexor Tendon TestingFlexor Tendon Testing PulleysPulleys-- A2 & A4A2 & A4
Normal Flexion CascadeNormal Flexion Cascade

3/21/2009
15
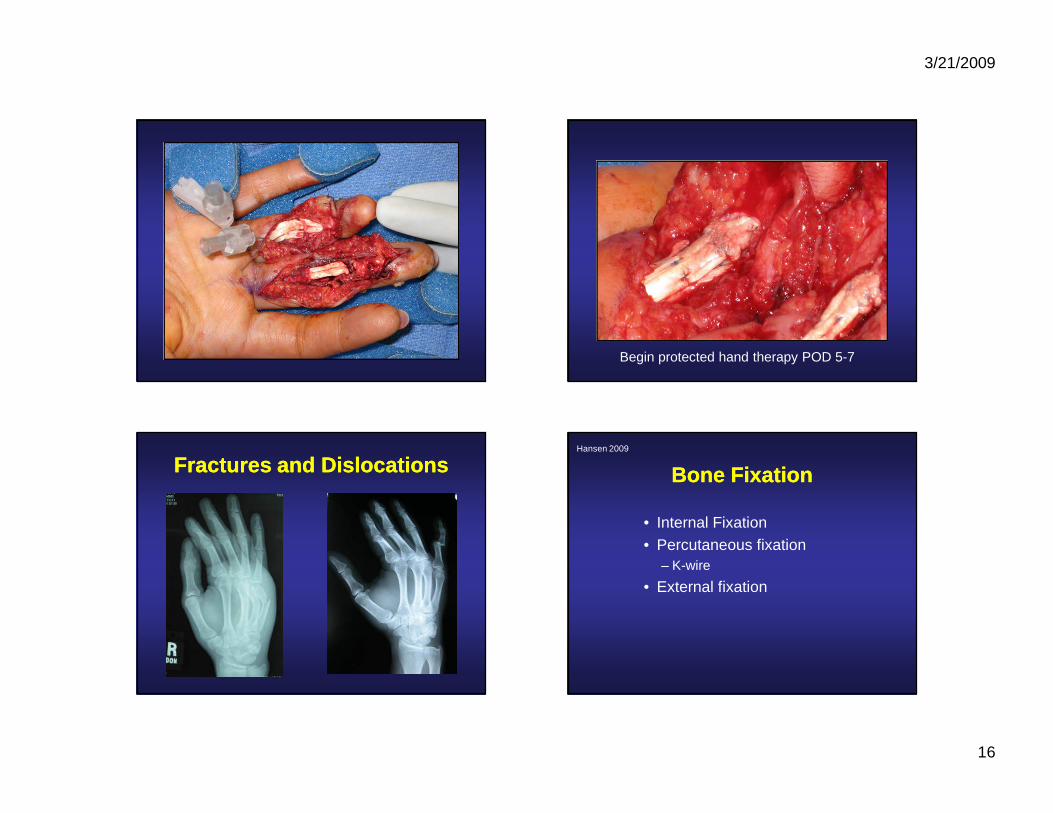
Flexor Tendon InjuriesFlexor Tendon Injuries
• Timing of repair– Primary repair: within 24 hours of injury
– Delayed primary repair: 24 hrs to 2 wks– Similar results for primary and delayed
primary
• Splint to prevent proximal retraction
3/21/2009
16
Begin protected hand therapy POD 5-7
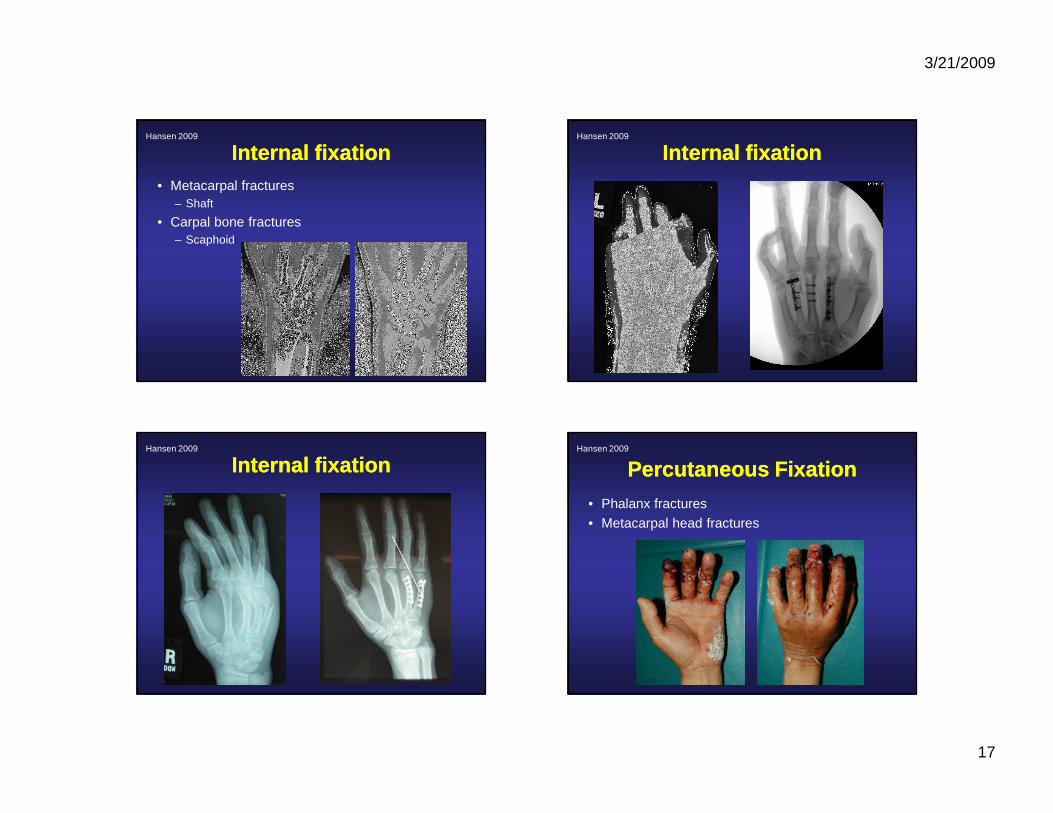
Fractures and DislocationsFractures and Dislocations Bone FixationBone Fixation
• Internal Fixation• Percutaneous fixation
– K-wire
• External fixation
Hansen 2009
3/21/2009
17
Internal fixationInternal fixation• Metacarpal fractures
– Shaft
• Carpal bone fractures– Scaphoid
Hansen 2009
Internal fixationInternal fixationHansen 2009
Internal fixationInternal fixationHansen 2009
Percutaneous FixationPercutaneous Fixation• Phalanx fractures• Metacarpal head fractures
Hansen 2009

3/21/2009
18
Percutaneous FixationPercutaneous FixationHansen 2009
External FixationExternal Fixation
• Comminuted bone fractures• Poor soft-tissue envelope
Hansen 2009
External FixationExternal FixationHansen 2009
External FixationExternal Fixation

3/21/2009
19
DislocationDislocation
• 29 year old male s/p MCA presents to ER with R hand pain
ReplantationReplantation
Hansen 2009
3/21/2009
20
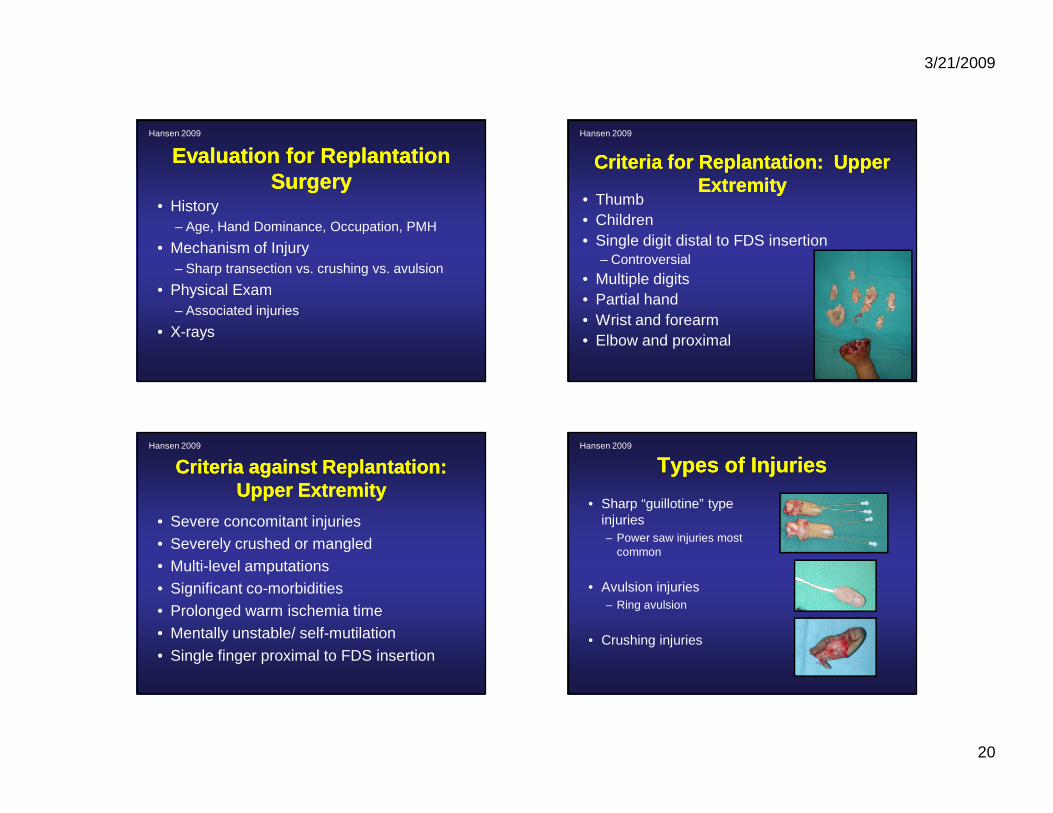
Evaluation for Replantation Evaluation for Replantation SurgerySurgery
• History– Age, Hand Dominance, Occupation, PMH
• Mechanism of Injury– Sharp transection vs. crushing vs. avulsion
• Physical Exam– Associated injuries
• X-rays
Hansen 2009
Criteria Criteria forfor Replantation: Upper Replantation: Upper ExtremityExtremity
• Thumb• Children• Single digit distal to FDS insertion
– Controversial
• Multiple digits• Partial hand• Wrist and forearm• Elbow and proximal
Hansen 2009
Criteria Criteria againstagainst Replantation: Replantation: Upper ExtremityUpper Extremity
• Severe concomitant injuries• Severely crushed or mangled• Multi-level amputations• Significant co-morbidities• Prolonged warm ischemia time• Mentally unstable/ self-mutilation
• Single finger proximal to FDS insertion
Hansen 2009
Types of InjuriesTypes of Injuries
• Sharp “guillotine” type injuries– Power saw injuries most
common
• Avulsion injuries– Ring avulsion
• Crushing injuries
Hansen 2009
3/21/2009
21
Hansen 2009
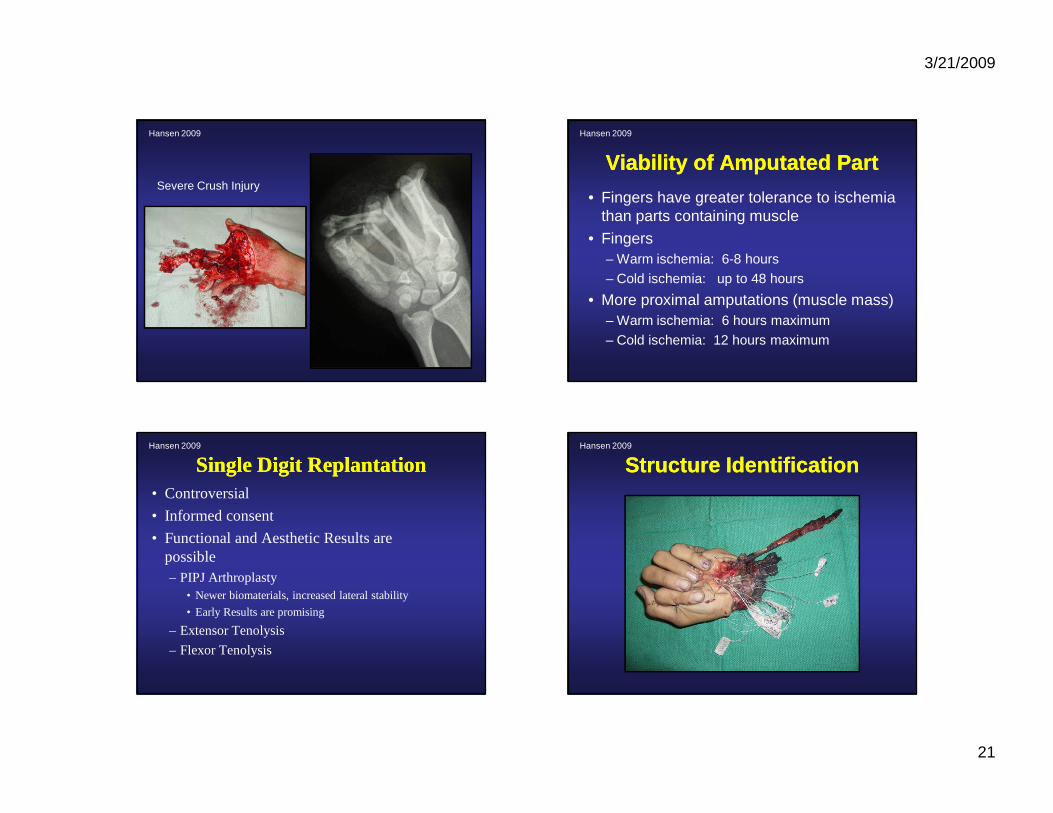
Severe Crush Injury
Viability of Amputated PartViability of Amputated Part
• Fingers have greater tolerance to ischemia than parts containing muscle
• Fingers– Warm ischemia: 6-8 hours
– Cold ischemia: up to 48 hours
• More proximal amputations (muscle mass)– Warm ischemia: 6 hours maximum
– Cold ischemia: 12 hours maximum
Hansen 2009
Single Digit ReplantationSingle Digit Replantation• Controversial
• Informed consent
• Functional and Aesthetic Results are possible– PIPJ Arthroplasty
• Newer biomaterials, increased lateral stability
• Early Results are promising
– Extensor Tenolysis
– Flexor Tenolysis
Hansen 2009
Structure IdentificationStructure IdentificationHansen 2009

3/21/2009
22
Osseous fixationOsseous fixation
• Bone shortening essential to provide tension-free vascular anastomoses– Preferentially from detached part to preserve
option on the proximal side
Hansen 2009
Vascular AnastomosisVascular Anastomosis
• Arterial anastomosis - 8-0 to 11-0 nylon
• Debride to undamaged artery
• If there is tension, further bone shortening or vein graft (distal forearm, dorsal foot, spare parts)
Hansen 2009
Multiple Finger ReplantationMultiple Finger Replantation
Hansen 2009
Multiple Finger ReplantationMultiple Finger ReplantationHansen 2009

3/21/2009
23
Multiple Finger ReplantationMultiple Finger ReplantationHansen 2009
Ring Avulsion InjuryRing Avulsion InjuryHansen 2009
Ring Avulsion InjuryRing Avulsion InjuryHansen 2009
Finger Tip ReplantationFinger Tip ReplantationHansen 2009

3/21/2009
24
Finger Tip ReplantationFinger Tip ReplantationHansen 2009
Finger Tip ReplantationFinger Tip ReplantationHansen 2009
Thumb AmputationsThumb Amputations
• 40% function of the hand• Requires
– Sensibility– Length for opposition to medial digits
• Even with poor motion and sensation, useful as a post for opposition
Hansen 2009
Thumb ReplantationThumb ReplantationHansen 2009
3/21/2009
25
Thumb ReplantationThumb ReplantationHansen 2009
Hand Trauma: SummaryHand Trauma: Summary• History and physical examination crucial• Address the soft tissue, tendon, nerve,
vasculature and bone individually• Reconstructive ladder for soft tissue
reconstruction• Immobilize for only as long as you need to• REHABILITATION is key to a successful
outcome
Hansen 2009
Thank YouThank You