hakim cme ortho_2
DESCRIPTION
orthoTRANSCRIPT
DEGENERATIVE
Disc DISEASE
Dr Muhammad Hakim UD41 Ortho HTAN
Anatomy
Pathophysiology
Classification
Clinical picture
Diagnosis
Treatment
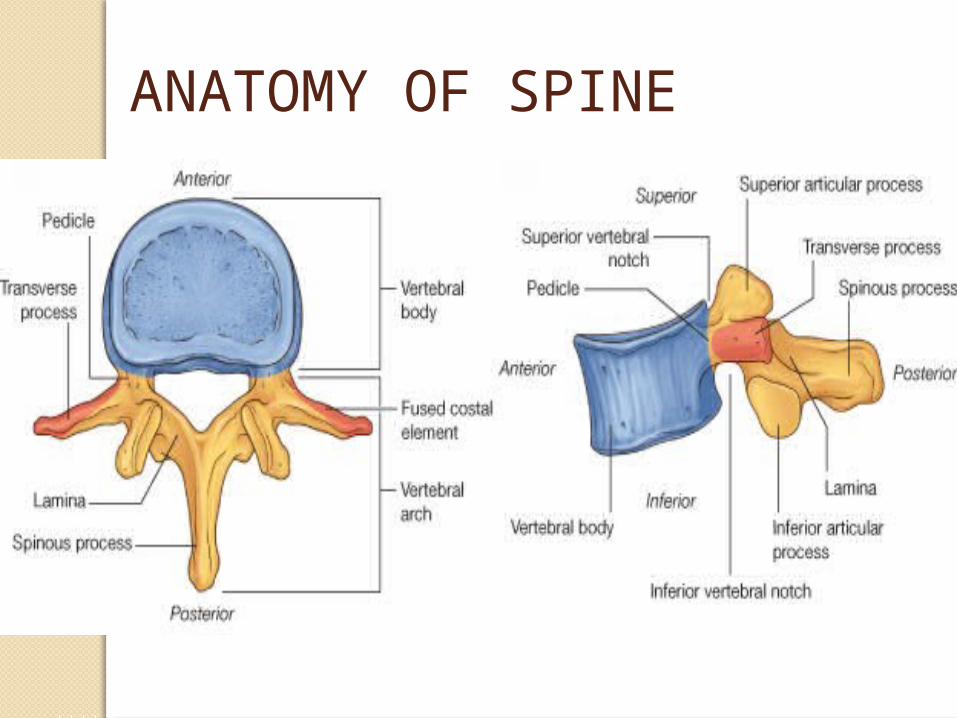
ANATOMY OF SPINE

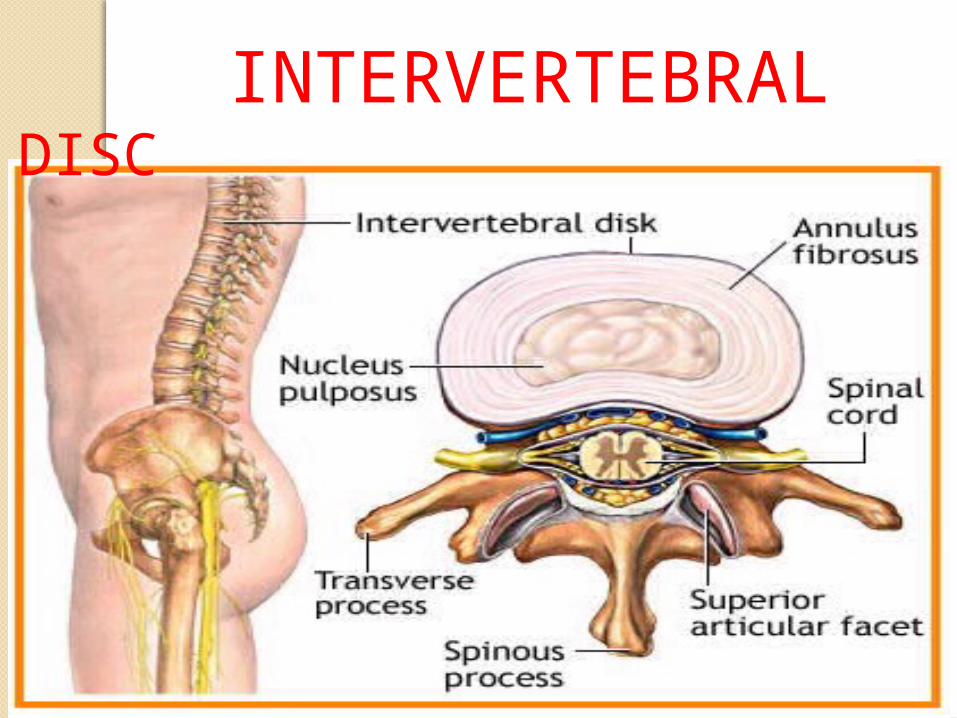
INTERVERTEBRAL DISC
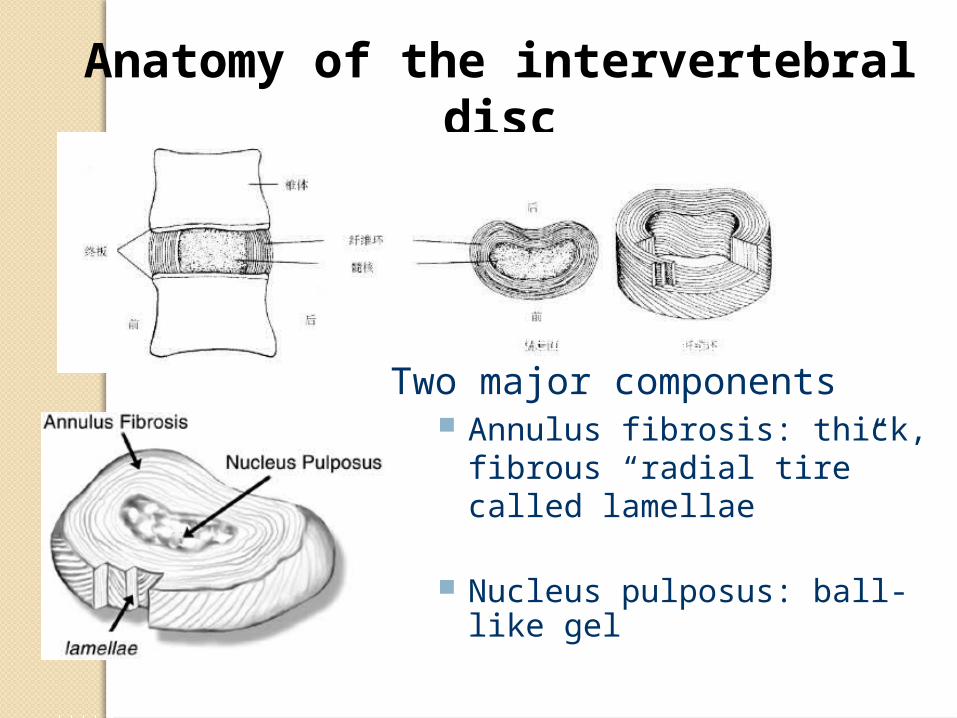
Anatomy of the intervertebral disc
The Intervertebral Disc
Two major components Annulus fibrosis: thick, fibrous
“radial tire” called lamellae
Nucleus pulposus: ball-like gel
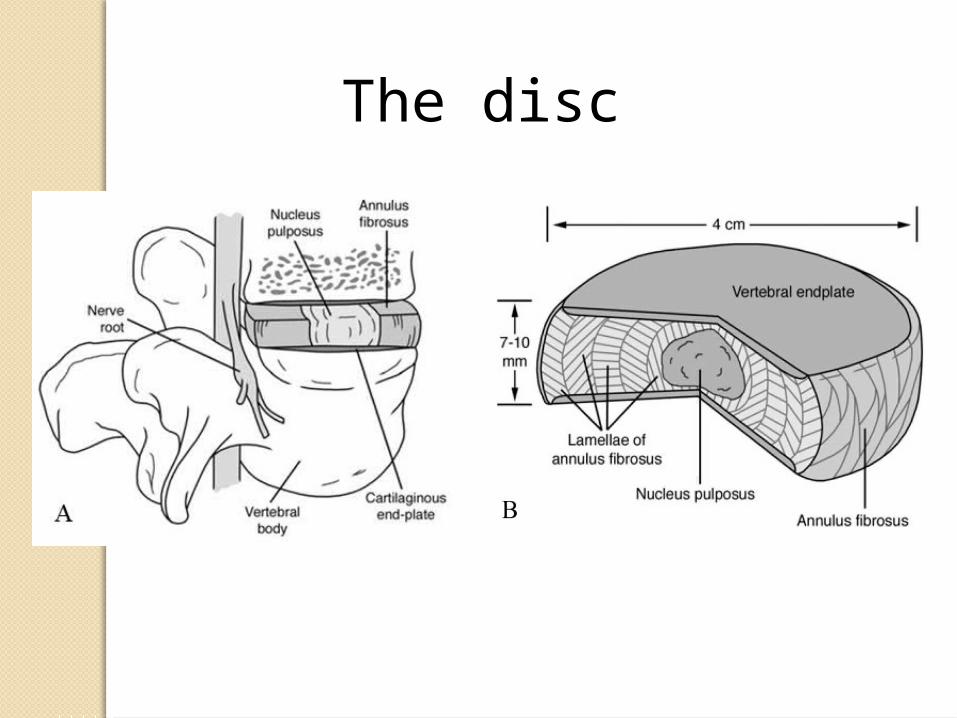
The disc
PathophysiologyDegenerative disc disease is a
general term used to describe changes that can occur along any area of the spine as you age but is most common in the lumbar area.
Its not actually a disease but rather a condition in which your disc “degenerate” or lose their flexibility and ability to cushion your spine.
Familial predisposition for degenerative for degenerative disc disease.Spine 21.1527-9.1996
The intervertebral disk undergoes the most serious age-related changes.
By the third decade of life, the nucleus pulposus becomes replaced with fibrocartilage, and the distinction between the nucleus and the annulus becomes blurred.
The proteoglycan, water, and noncollagenous protein concentrations decrease, while the collagen concentration increases.
The increase in collagen concentration is more pronounced in the nucleus and in the posterior quadrants of the disk.

Biochemically Aging increases the ratio of keratin sulfate to
chondroitin sulfate, and it also changes the proportion of chondroitin-4-sulfate to chondroitin-6-sulfate, with a parallel decrease in water content.
Proteoglycan synthesis decreases, which decreases the osmotic swelling and the traffic of oxygen and nutrients to the disk. Because of this decreased traffic, breakdown products of link and noncollagenous proteins stagnate in the disk.
Nonenzymatic glycosylation of these breakdown products accounts for the brown discoloration of the aging connective tissues
Eyre DR, Matsui Y, Wu JJ. Collagen polymorphisms of the intervertebral disc. Biochem Soc Trans 2002;30:844-8
Age related changes :Disc dry out and shrink-The disc made about 80 percent of water, as we age they slowly lose water. -This loss of flexibility puts more stress on the annulus.Small tears occur in the annulus-When there are tear in the wall, some gel like material will come out and touches the nerves.-This material has many inflammatory proteins that can inflame the nerves and cause pain.
Disc space get smaller-due to the loss of water in the disc, the distance between vertebrae begin to collapse, which is why we get shorter as we ageBone spurs grow-without the disc holding apart the vertebrae, they can rub on each other and cause abnormal bone growth.Spinal canal narrows-The stresses of all the above changes causes the
ligament and facet joint to be hyperthrophy. -This overgrowth causes the spinal canal to narrow
which can compress the spinal cord and nerve which result
in pain.

These changes are more likely to occur in people who smoke cigarettes and those who do heavy physical work (such as repeated heavy lifting).
People who are obese are also more likely to have symptoms of degenerative disc disease.
A sudden (acute) injury leading to a herniated disc (such as a fall) may also begin the degeneration process.
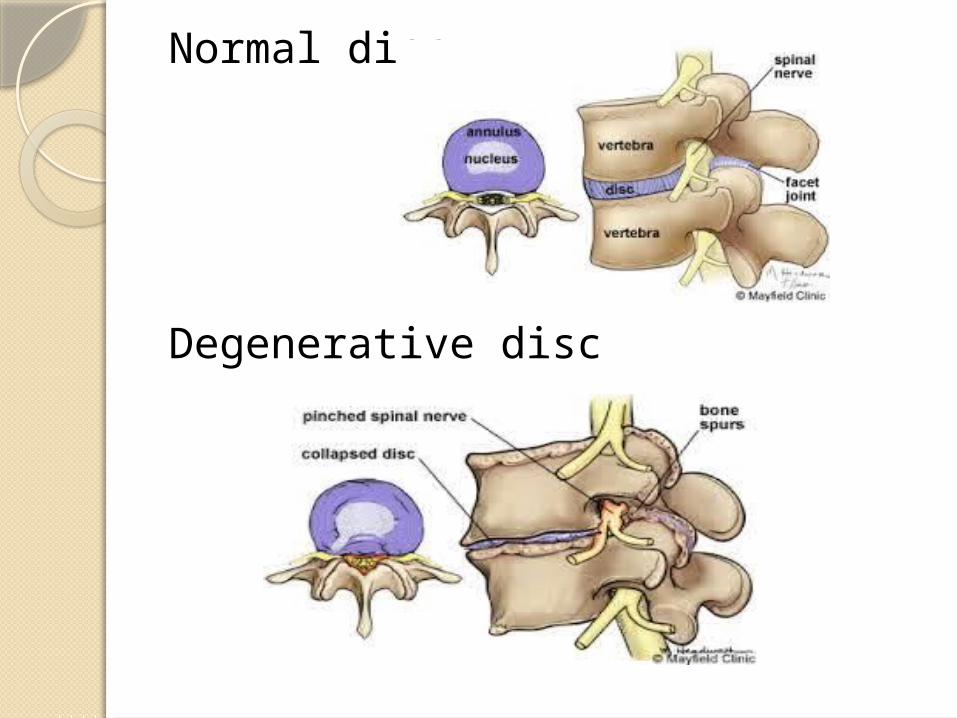
Normal disc
Degenerative disc
Degenerative Changes of the intervertebral disc
A. ) - DISC BULGE B. ) - ANNULAR TEARC. ) - HERNIATION
A ) DISC BULGE Generalized or circumferential disc displacement (involving 50% to 100% of the disc circumference) is known as “bulging”, and is not considered a form of herniation.
Bulging can be symmetrical (displacement of disc material is equal in all directions) or asymmetrical (frequently associated with scoliosis)
(Fardon and Milette 2001).
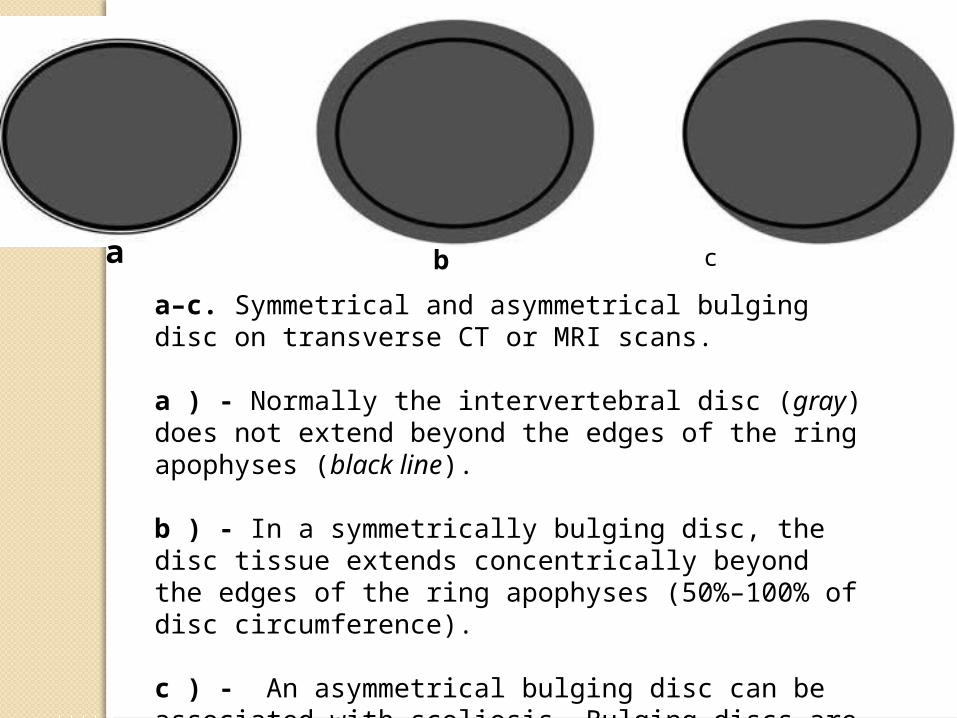
a–c. Symmetrical and asymmetrical bulging disc on transverse CT or MRI scans.
a ) - Normally the intervertebral disc (gray) does not extend beyond the edges of the ring apophyses (black line).
b ) - In a symmetrically bulging disc, the disc tissue extends concentrically beyond the edges of the ring apophyses (50%–100% of disc circumference).
c ) - An asymmetrical bulging disc can be associated with scoliosis. Bulging discs are not considered a form of herniation
a b c

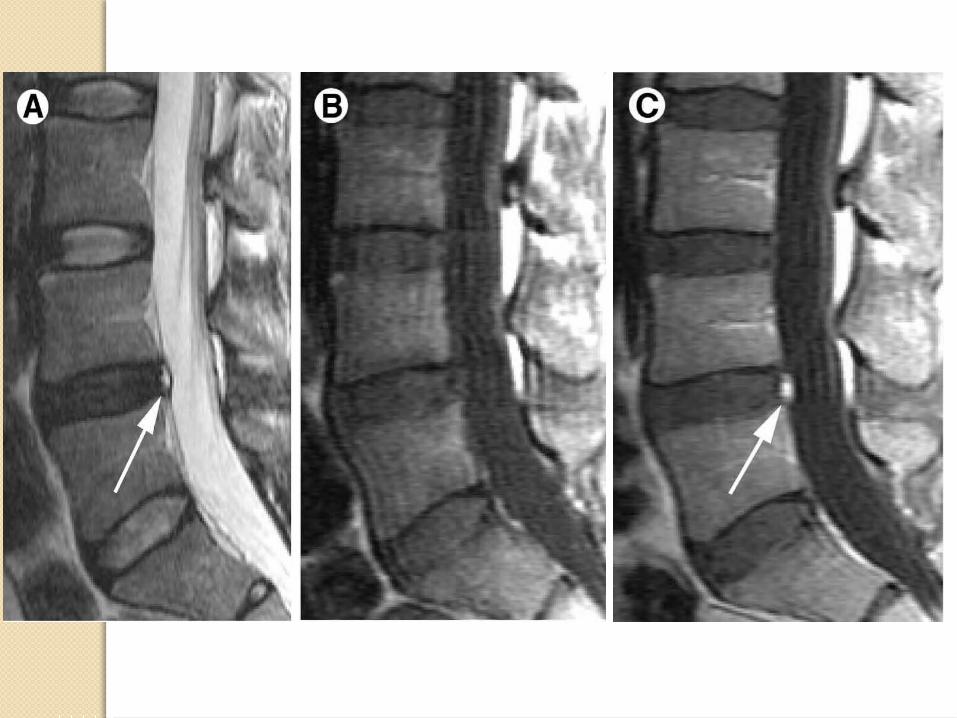
B ). ANNULAR TEAR
Disruption of concentric collagenous fibers comprising the anulus fibrosus
MRI Findings• Contrast-enhancing nidus in disc margin• High signal zone at edge of disc which has low intrinsic signal

Concentric tears are circumferential lesions which are found in the outer layers of the annular wall (Martin et al. 2002). They represent splitting between adjacent lamellae of the annulus, like onion rings. Concentric tears are most commonly encountered in the outer annulus fibrosus, and are believed to be of traumatic origin especially from torsion overload injuries.
Radial tears are characterized by an annular tear which permeates from the deep central part of the disc (nucleus pulposus) and extends outward toward the annulus, in either a transverse or cranial-caudal plane.
Transverse tears, also known as “peripheral tears” or “rim lesions,” are horizontal ruptures of fibers, near the insertion in the bony ring apophyses. Their clinical significance remains unclear. Transverse tears are believed to be traumatically induced and are often associated with small osteophytes.
TYPES
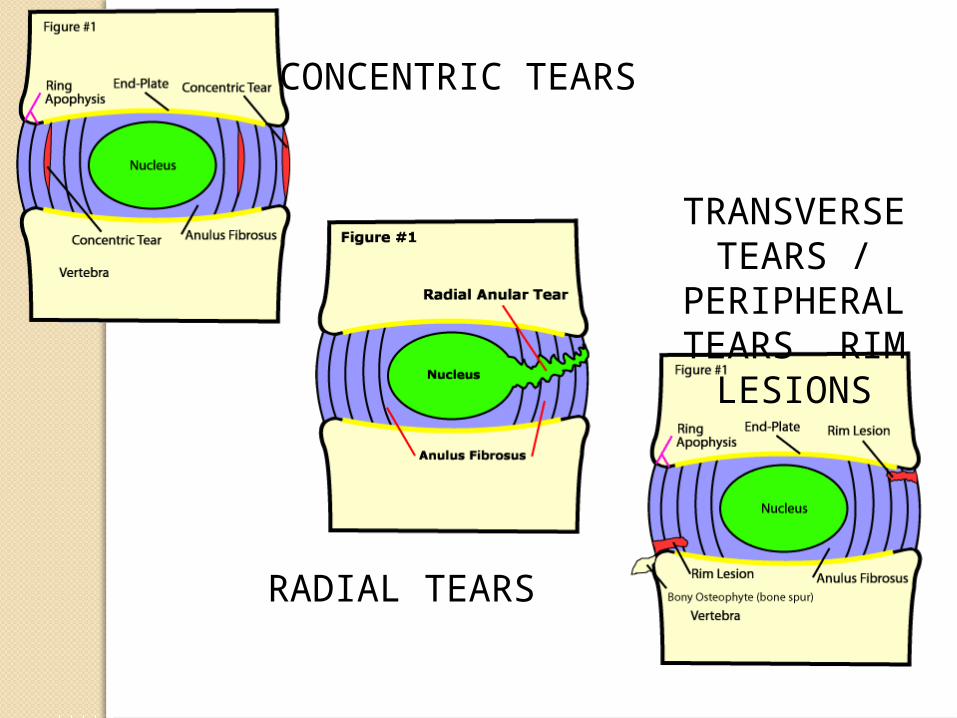
CONCENTRIC TEARS
TRANSVERSE TEARS /
PERIPHERAL TEARS RIM
LESIONS
RADIAL TEARS
C). DISC HERNIATION
Herniation is defined as a localized displacement of disc material (nucleus, cartilage, fragmented apophyseal bone, fragmented annular tissue) beyond the limits of the intervertebral disc space.
(Fardon and Milette 2001).
Herniated discs in the cranio-caudal (vertical) direction through a break in one or both of the vertebral body endplates are referred to as “intravertebral herniations” (also known as Schmorl’s nodes). They are often surrounded by reactive bone marrow changes. Nutrient vascular canals may leave scars in the endplates, which are weak spots representing a route for the early formation of intravertebral body nuclear herniations
(Chandraraj et al. 1998).

Degenerative Changes of the
Posterior ElementsMost commonly affected are:1.Facet Joints 2.Ligamentum
Flavum
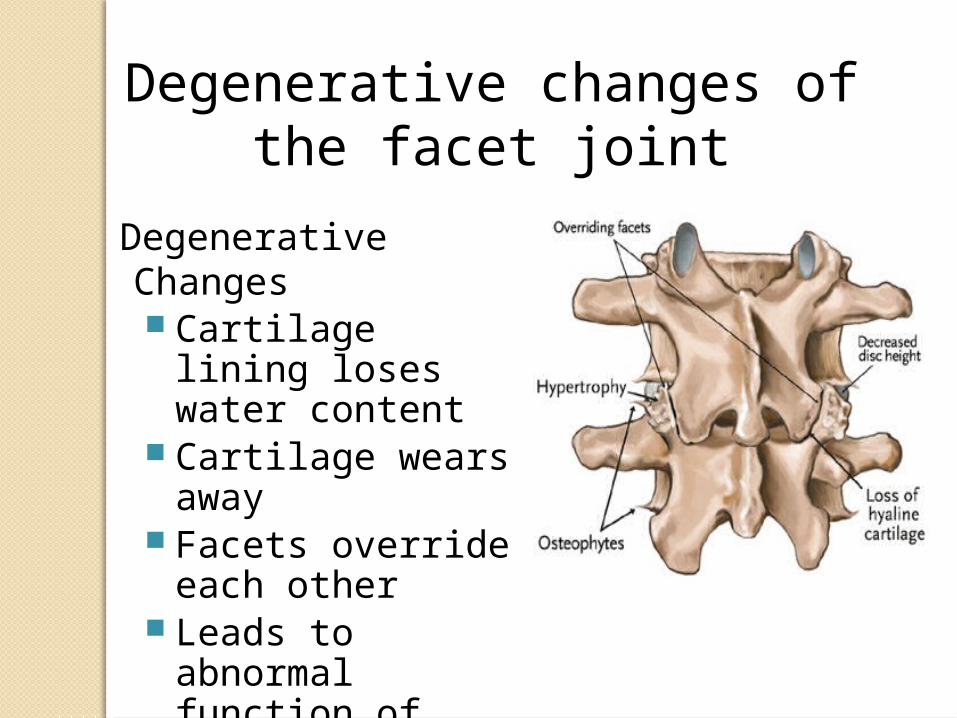
Degenerative changes of the facet joint
Degenerative Changes Cartilage lining loses
water content Cartilage wears
away Facets override
each other Leads to abnormal
function of motion segment


2). LIGAMENTUM FLAVUM

Degenerative Changes
Partial ruptures, necrosis
and calcifications
Negatively impact function
of motion segment and can
cause spinal stenosis

MRI of spinal stenosis: arrow points to the moderately stenotic spinal canal caused by hypertrophic facets and ligament flavum

Clinical pictureAt least 30% of people aged 30-50 years old will
have some degree of disc space degeneration, although not all will have pain or ever receive a formal diagnosis.
In fact, after a patient reaches 60, some level of disc degeneration is a normal finding.
History of recurring or persistent back painOccasional buttock pain and referred pain radiating
down the posterior thigh with no radiculopathyPain:deep,dull ache in the lower lumbar region Increased pain with rotation,flexion and side
bending,prolonged sitting/standing/walkingRelief of pain with rest,lateral recumbent positionLeg pain develop as late findingSLR causes back pain only

Initially a physical exam consisting of range of motion, check nerve-related changes, and look for fractures or infection
Diagnostic test
-Laboratory studies
-Imaging studies
-diagnostic procedure
Diagnostic Tests

Laboratory Studies
Inflammatory causes of low back pain can be ruled out with tests for acute phase reactants such as the erythrocyte sedimentation rate (ESR) and C- reactive protein level. A complete blood count should be obtained, including a platelet count.
Rheumatoid factor testing and antinuclear antibody testing are good screening tools for autoimmune disorders.

Imaging studies X-rays would show the narrowing between the vertebral
bodies
CT scan shows how much space is available for the nerve roots to pass through
MRI tests are the most significant diagnostic imaging that shows disk herniation and compressed nerves

Diagnostic procedure
-Selective nerve root blocks Transforaminal selective nerve root blocks (SNRBs) have
been used as both subjective diagnostic tools and therapeutic interventions for lumbar spinal stenotic levels. When MRI shows evidence of multilevel degenerative disk disease, SNRBs can be used to determine whether a specific nerve root is affected. The procedure involves injection of anesthetic and contrast at the nerve root level of interest under fluoroscopic guidance. This creates an area of hypoesthesia in the respective dermatome.
Anderberg et al investigated the correlation of SNRBs with MRI findings and clinical symptoms in cervical spines with multilevel degenerative disk disease. The results showed a 60% correlation with the most severe areas of MRI degeneration. In areas of neurological deficit, dermatomal radicular pain showed a 28% correlation with SNRB results.1.Anderberg L, Annertz M, Brandt L, Saveland H. Selective diagnostic cervical nerve root block--correlation with clinical symptoms and MRI-pathology. Acta Neurochir (Wien). Jun 2004;146(6):559-65; discussion 565.

Conservative Modifying daily activities and physical therapy Chiropractor Analgesics, NSAIDs and oral steroids are prescribed
to reduce pain Epidural injections and selective nerve root blocks
are before surgery
Surgery is a last resort for treatment of DDD
Treatment

ExerciseDifferent types of exercises are prescribed,
depending on each patient's diagnosis. Floor exercises consist of abdominal bracing, modified sit-ups, double-knee-to-chest or low back stretches, seat lifts, mountain and sag exercises, knee-to-elbow exercises, hamstring stretches, extension exercises, and extension flexibility exercises. Swimming exercises are some of the best activities. Aerobic exercises improve endurance if performed regularly (ie, ≥ 3 times/wk). Relaxation exercises are good for relieving muscular tension that may aggravate back pain.

ChiropractorChiropractic manipulation or spinal
adjustment is done for patient with back or neck pain.The philosophy is to return the joints to more normal motion.Good joint motion is essential for the health and nutrition of the discs and joints because it permits the exchange of nutrient,fluids and waste.

MedicationNonsteroidal anti-inflammatory drugs-aspirin,ibuprofen,naproxen and celecoxib are examples of non steroidal anti-inflammatory drugs used to reduce inflammation and relieve pain.Analgesics-acetaminophen can relieve pain but don’t have the anti-inflammatory effect of NSAIDs.Steroids-can be used to reduced swelling and inflammation of the nerve.steroids have the advantage of providing almost immediate pain relief within a 24 hour period

Injections Epidural steroid injections are most commonly used for
therapeutic purposes. The type and dosage of steroid varies widely. Methylprednisolone (80-120 mg) mixed with normal saline to achieve a volume of 8-10 mL is an effective and safe dosage and volume. In some centers, 2-3 injections are given over a 1- to 2-week course, but long-term results do not appear to be any different from those achieved with a single injection.
The response to epidural injections is variable, and many authorities believe the injections are only of short-term value. Even if a favorable response occurs, no more than 4 injections should be given annually. Immediate pain relief may be achieved by adding 4-6 mg of preservative-free morphine to the epidural steroid injection.

Surgical theraphyDiskectomy





Take Home MessagesKnow the natural history of the
diseaseKnow your patientCorrelate clinical findings and
investigation if neededUntil definitive evidence
available, choose the most cost-effective available treatment option
