hac presentation (14)
TRANSCRIPT
HYPERADRENOCORTICISM
Jade Webster
Hyperadrenocorticism
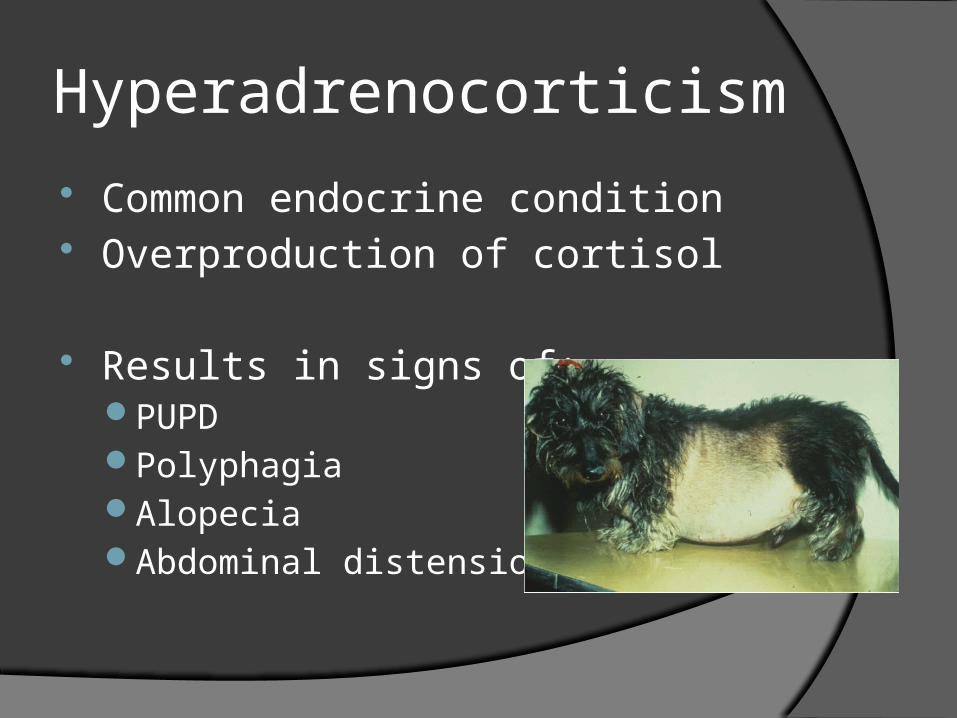
Common endocrine condition Overproduction of cortisol
Results in signs of:PUPD PolyphagiaAlopeciaAbdominal distension
Types
Categorised into 2 types:
Pituitary Dependent Adrenal Dependent
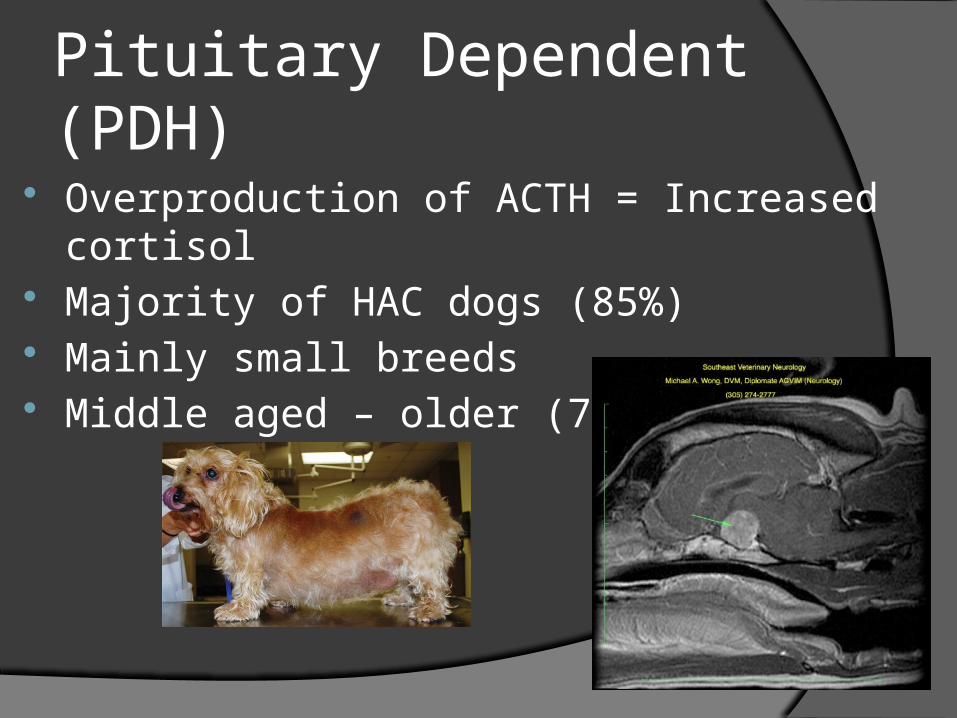
Pituitary Dependent (PDH)
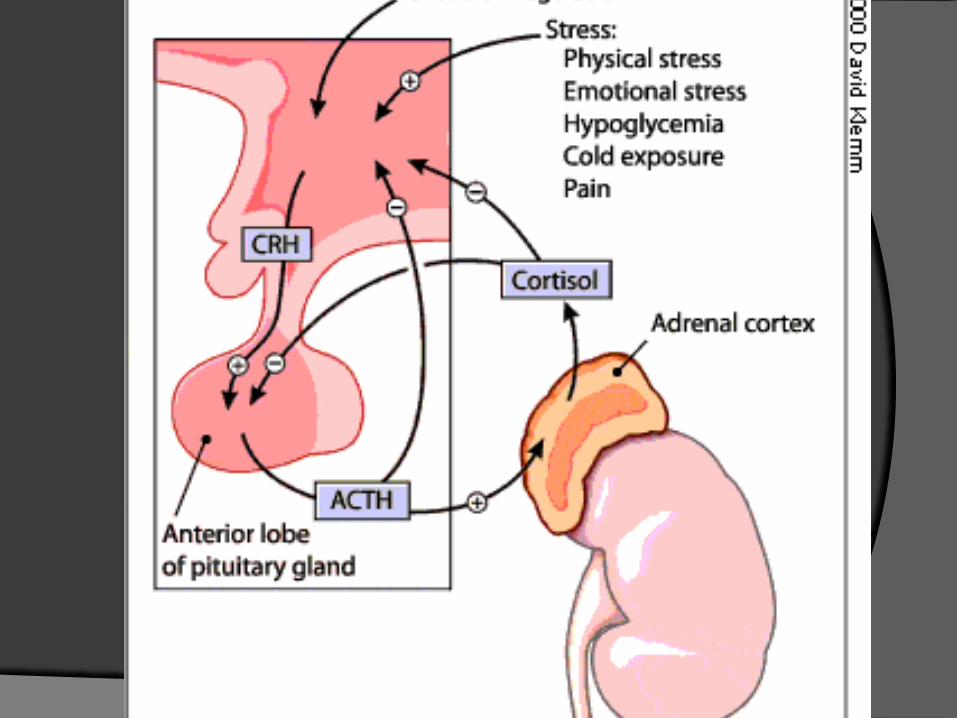
Overproduction of ACTH = Increased cortisol Majority of HAC dogs (85%) Mainly small breeds Middle aged – older (7-9yrs)
PDH
Radiotherapy Progression of disease : can form a
pituitary macroadenoma Neurological signs
Median survival time = 662-900 days (tx with trilostane)
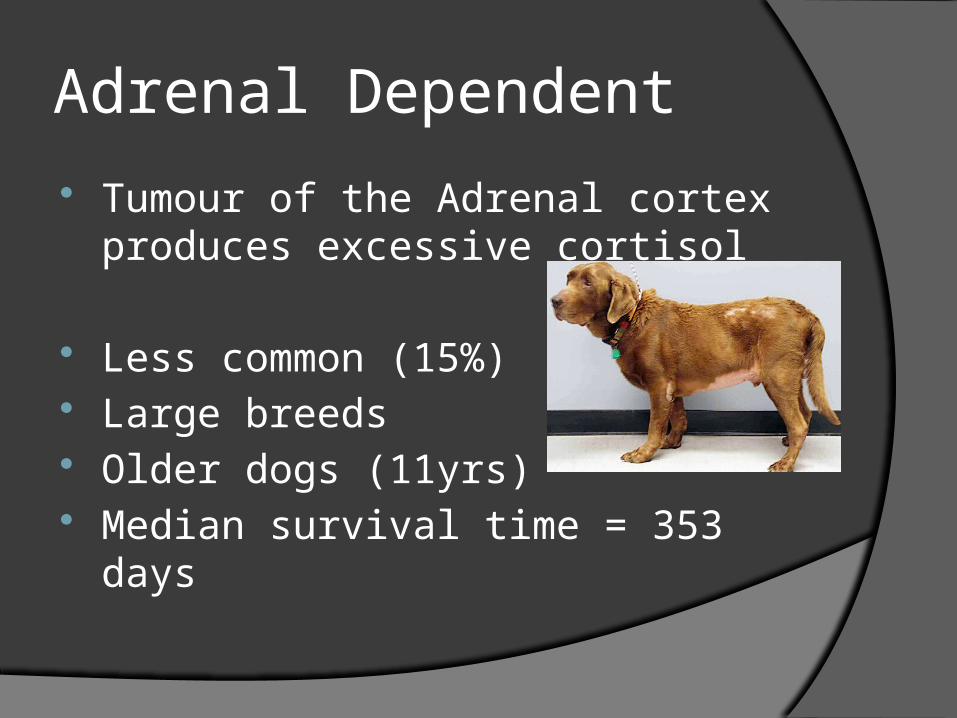
Adrenal Dependent
Tumour of the Adrenal cortex produces excessive cortisol
Less common (15%) Large breeds Older dogs (11yrs) Median survival time = 353 days
ADH
50% benign and 50% malignant
Surgery: Adrenalectomy Progression of disease:
Malignancy is a possibility in 50% of these cases
Study
Involved 57 dogs from both first opinion (32 dogs) and referral hospitals (25 dogs)
All diagnosed with HAC Age Range = 4 – 17 years old Weight range = 2.3 - 38.5kg

Breeds involved Cross-breed (20) Jack Russell (7) Cocker Sp. (4) YRT (3) Shih-Tzu (3) WHWT (2) Springer Sp. (2) Bichon Frise (2) Schnauzer (2) Patterdale (1) Scottish Terrier (1)
Collie (2) SBT (1) Shetland Sheepdog (1) Affenpinscher (1) Beagle (1) Hungarian Viszla (1) CKCS (1) Flatcoat Ret. (1) Border Terrier (1) Red Setter (1) Shar Pei (1)
What tests were used to diagnose HAC?
Were the patients differentiated into PDH or ADH?
And if so, How were they differentiated?
Diagnostic tests
Cannot use basal cortisolNon-adrenal illness (NAI) can cause a high
circulating cortisol levelPulsatile action of ACTH
Therefore diagnosis of HAC based on other tests
Tests performed
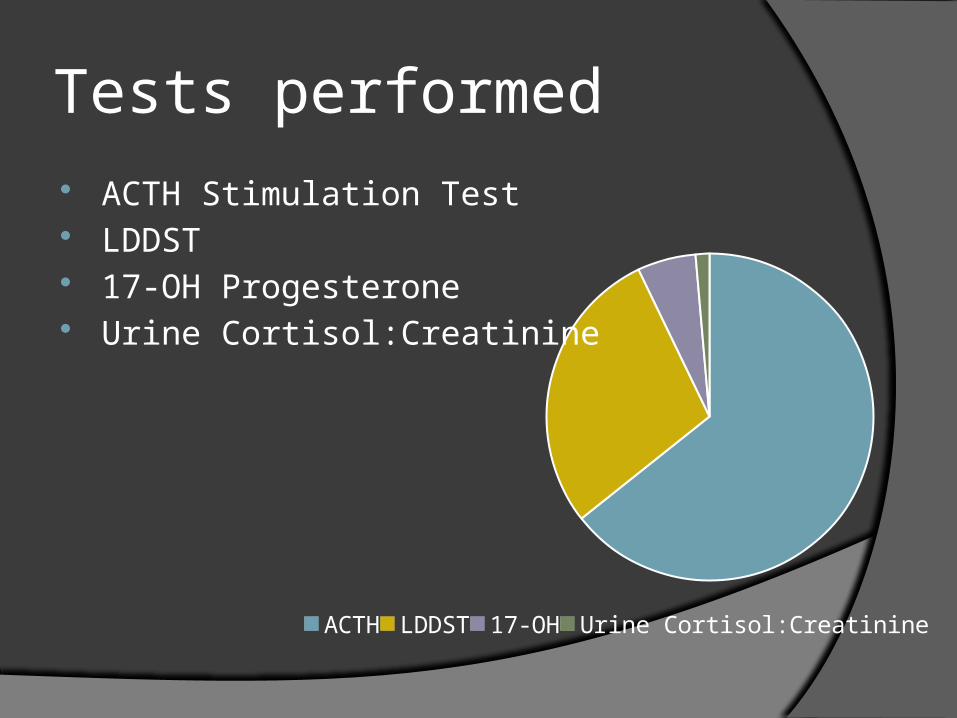
ACTH LDDST 17-OH Urine Cortisol:Creatinine
ACTH Stimulation Test LDDST 17-OH Progesterone Urine Cortisol:Creatinine
ACTH stimulation test
HAC = exaggerated responsePost ACTH cortisol >600nmol/l
Sensitivity = 57-83% Specificity = 59-93%
ACTH Stimulation Test
ACTH Stim was performed on 45 dogs in the study
31 recorded as a positive result Positive Post ACTH ranged from 618-
1443 (mean 926) Negative Post ACTH ranged from 218-
651 (median 427)
LDDST
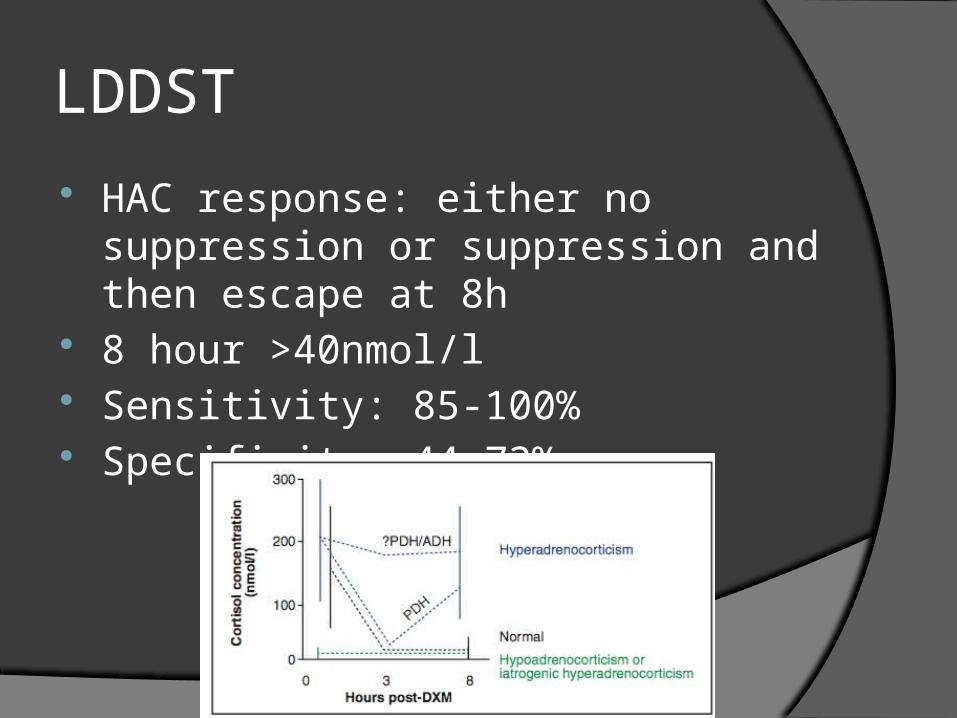
HAC response: either no suppression or suppression and then escape at 8h
8 hour >40nmol/l Sensitivity: 85-100% Specificity: 44-73%
LDDST performed in 20 dogs in study Of these 14 produced positive result
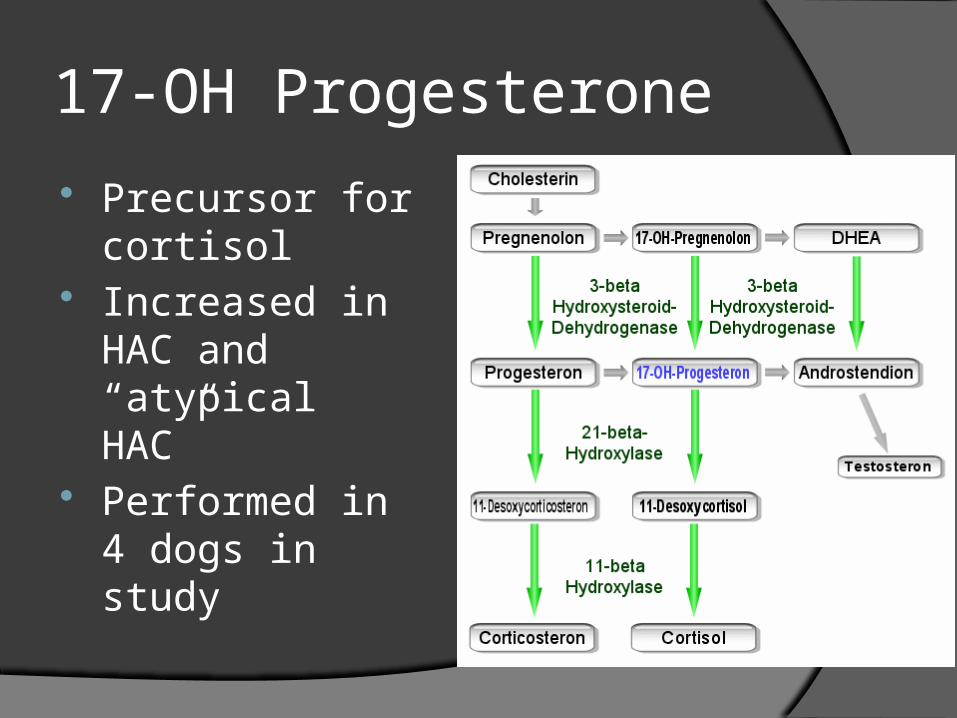
17-OH Progesterone
Precursor for cortisol
Increased in HAC and “atypical HAC”
Performed in 4 dogs in study
Urine cortisol:creatinine
Cortisol excreted in urine – reflection of cortisol release
Very sensitive (92%) Non-specific (21%)
Used in one case in the study as ACTH, LDDST and 17-OH were all negative but clinical signs strongly suggested HAC.
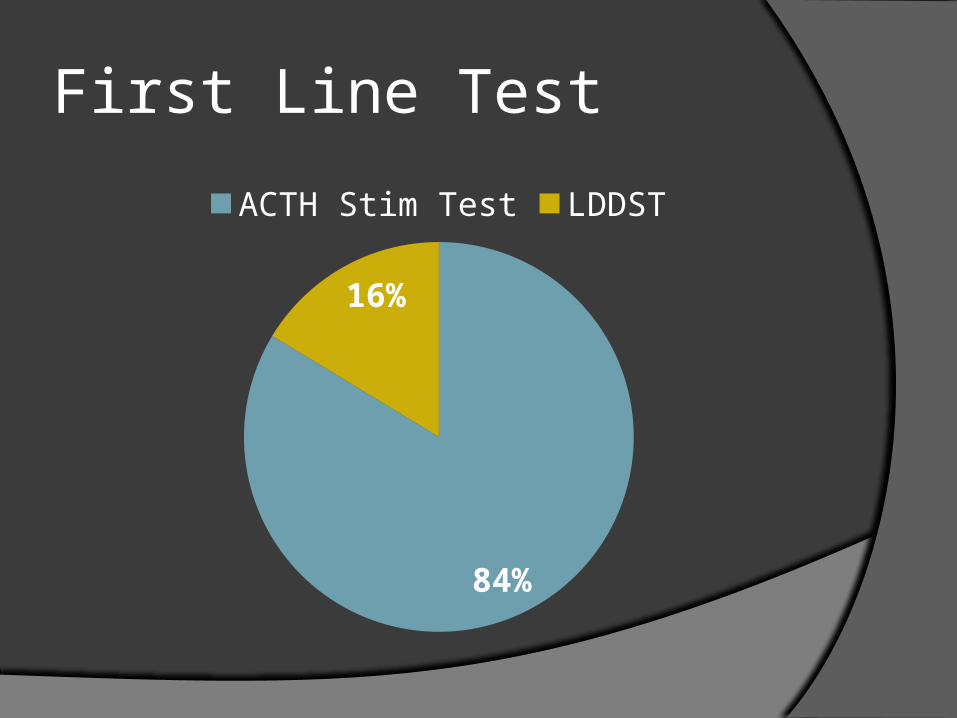
First Line Test
84%
16%
ACTH Stim Test LDDST
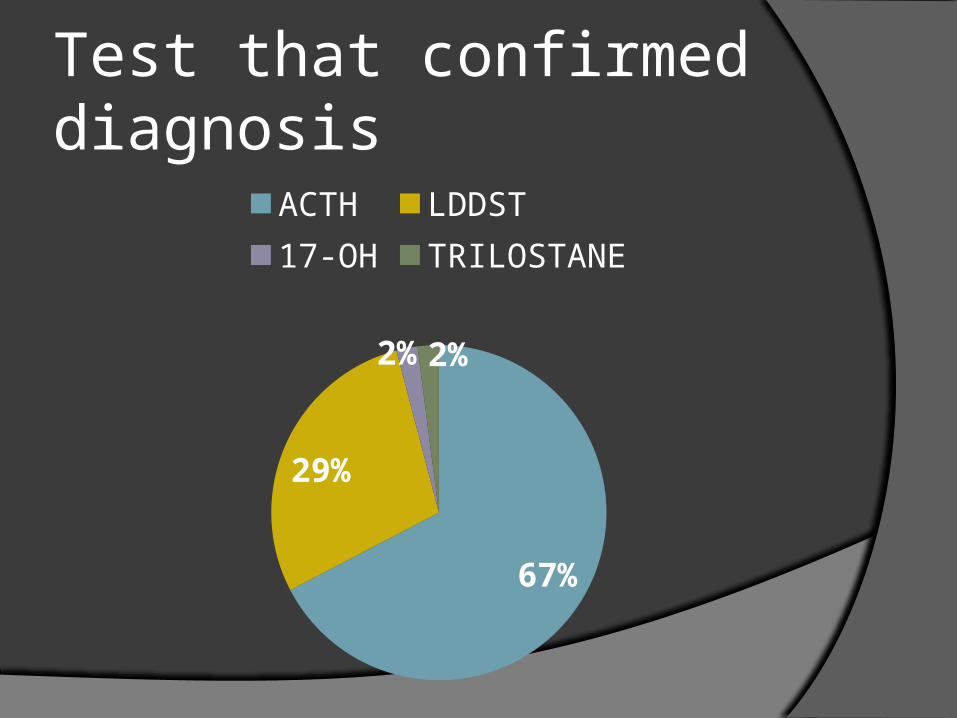
Test that confirmed diagnosis
67%
29%
2% 2%
ACTH LDDST17-OH TRILOSTANE
Differentiation
Ultrasound Endogenous ACTH LDDST
Differentiated
54% were differentiatedPDH = 25 cases (89%)ADH = 3 cases (11%)
29% cases in 1st opinion practice 90% cases in referral hospital
Ultrasound
PDH = Bilateral adrenomegaly ADH = Mass on adrenal gland
Ultrasound of adrenals performed in 24/53 dogs in study
95% of referral cases had adrenal ultrasound
15% of first opinion cases
Endogenous ACTH PDH = high ACTH (>28pg/ml) ADH = low ACTH (<5pg/ml) Used in 5 cases
All in referral centres Used alone in 2 of these
Rest were used in conjunction with ultrasound
LDDST
Suppression at 4hours and then escape suggest PDH
No suppression – either ADH or PDH Suggestive results were used to
differentiate alone in 7 cases6 in First opinion1 in Referral
Used in conjunction with ultrasound and endogenous ACTH
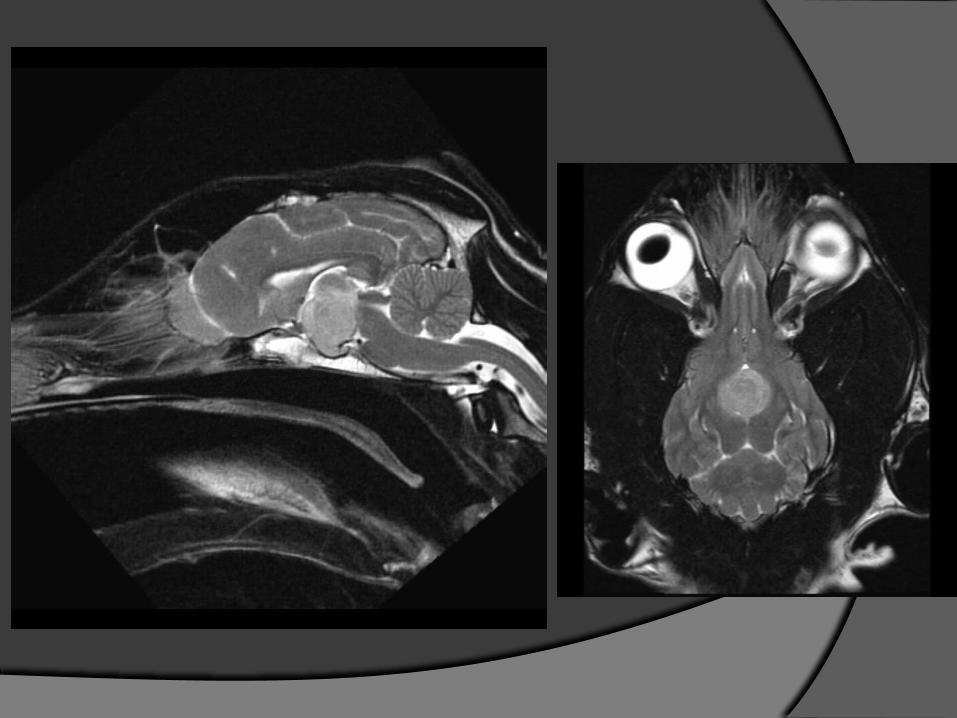
MRI
Used to diagnose PDH or following PDH diagnosis for planning of radiotherapy
Used in one case in the study as showed neuro signs and was diagnosed with a macroadenoma
Conclusions
ACTH was the most popular test of choice for diagnosing HAC
LDDST suggested as test of choiceHigher Sensitivity
Confusion over interpretation
UCCR
LDDST
17-OH
ACTH
Decreasing Sensitivity
Only 54% of dogs were differentiated
Simple test that can be performed in first opinion practice
Case Example - Sammy Diagnosed in first opinion practice with HAC
and was not differentiated The year following diagnosis
More PUPD Dx: diabetes insipidus. Responded to tx
6 months later represented for PUPD, weight loss and lethargyBelieved to be due to an over suppression
(Addisons) therefore decreased dose of trilostane 2 months later – presented for lying in lateral
recumbency and head banging
Limitations of Study
Assumptions of correct diagnosis History availability Information on diagnosis Absent values for Post ACTH/8hr
LDDST Assumptions of ultrasound
measurements made by first opinion vets
Important to differentiate
Not being done as often in first opinion practice as in referral hospitals
Endogenous ACTH – very simple
References Gould S.M, Baines E.A, Mannion P.A, Evans H and Herrtage M.E. (2001) Use of
endogenous ACTH concentration and adrenal ultrasonography to distinguish the cause of canine hyperadreocorticism. Journal of Small Animal Practice 42, 113-121
Behrend et al. (2012) Diagnosis of Spontaneous Canine Hyperadrenocorticism:ACVIM Consensus Statement (Small Animal). J Vet Intern Med 2013;27:1292–1304
Mooney C.T, Peterson M.E (2012) BSAVA Manual of Canine and Feline Endocrinology 4th ed.
Helm et al. (2011) A Comparison of Factors that Influence Survival in Dogs with Adrenal-Dependent Hyperadrenocorticism Treated with Mitotane or Trilostane. J Vet Intern Med 2011;25:251–260.
Chapman, P.S. et al (2003) Evaluation of the basal and post adrenocorticotrophic hormone serum concentrations of 17-hydroxyprogesterone for the diagnosis of hyperadrenocorticism in dogs. Veterinary Record 153, 77-775
Smiley L.E, Peterson M.E (1993) Evaluation of a urine cortisol:creatinine ratio as a screening test for hyperadrenocorticism in dogs. JVIM 7, 163-8
Ramsey I, Ristic J (2007) Diagnosis of canine hyperadrenocorticism. In Practice 2007;29:446-454
Acknowledgements
Thanks to Laura Cosgrove

Questions?