guideline for interpretation of microbiology lab results · rod clostridium tetani salmonella typhi...
TRANSCRIPT

Guideline for interpretation of
Microbiology Lab Results
Lim Kruy, MD (SHCH)
Erika Vlieghe, MD (ITM)
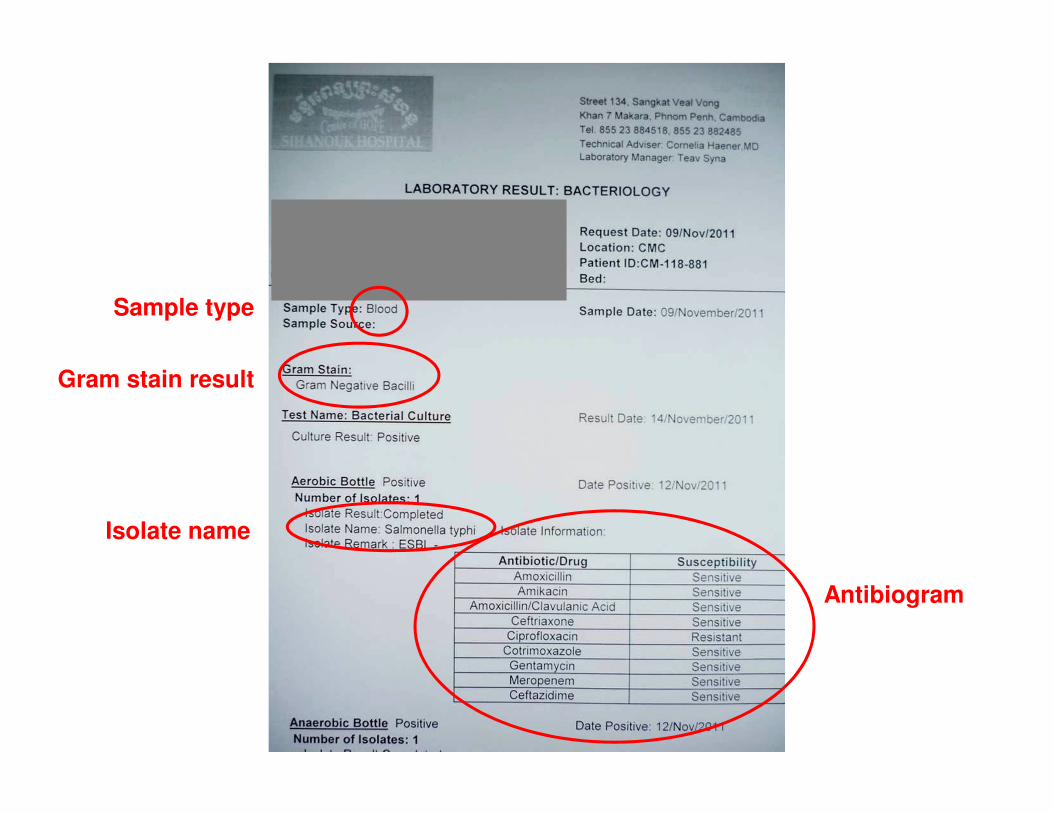
Sample type
Gram stain result
Isolate name
Antibiogram

Gram stain results
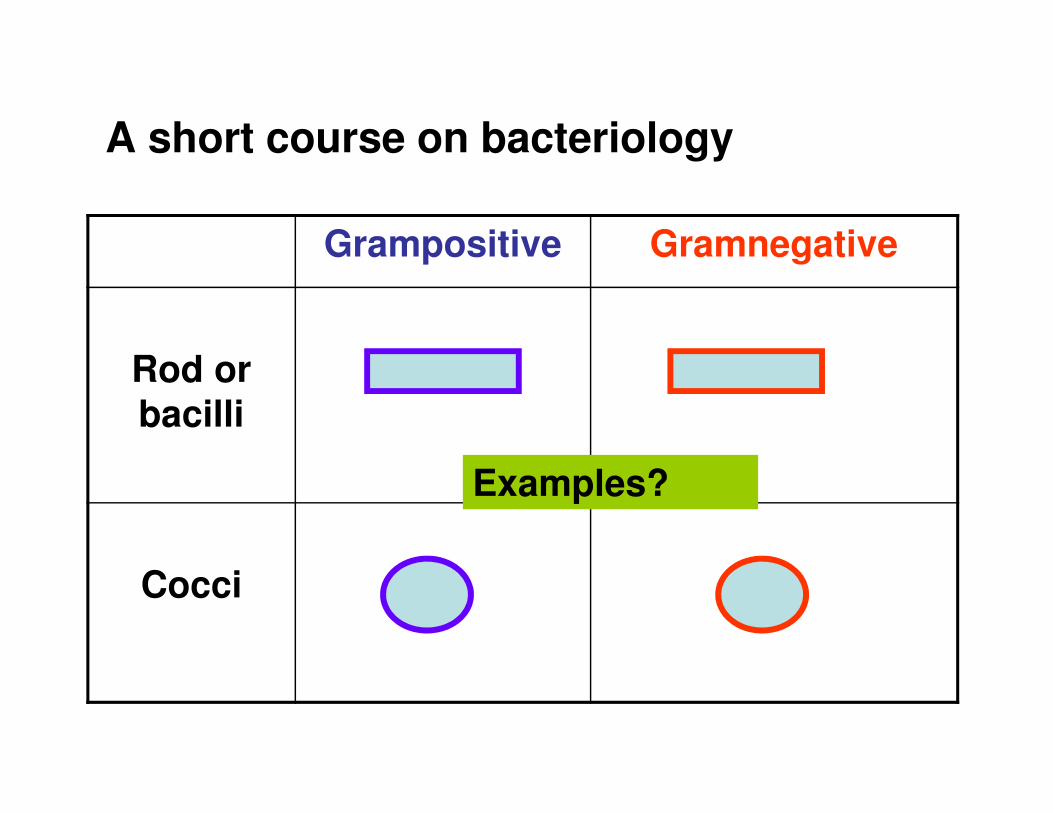
A short course on bacteriology
Grampositive Gramnegative
Rod or bacilli
Cocci
Examples?

A short course on bacteriology
Grampositive Gramnegative
Rod Clostridium tetani Salmonella typhi
Coccus Staphylococcus aureus
Meningococcus
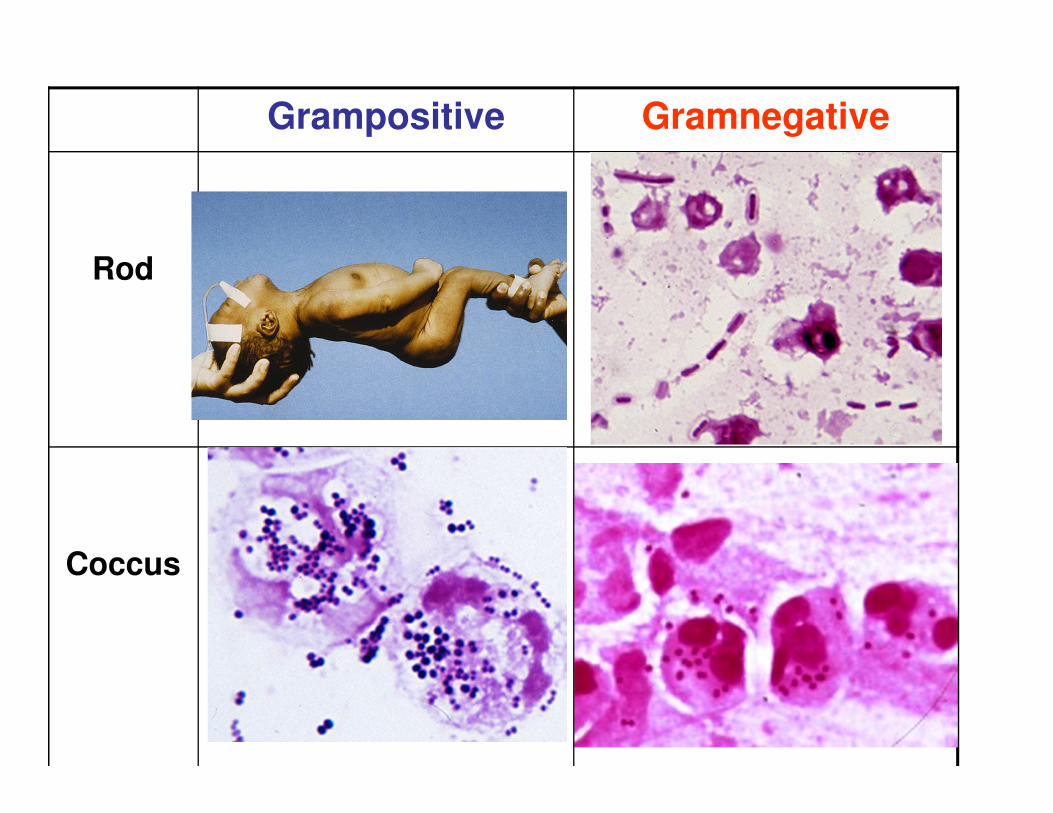
Grampositive Gramnegative
Rod
Coccus
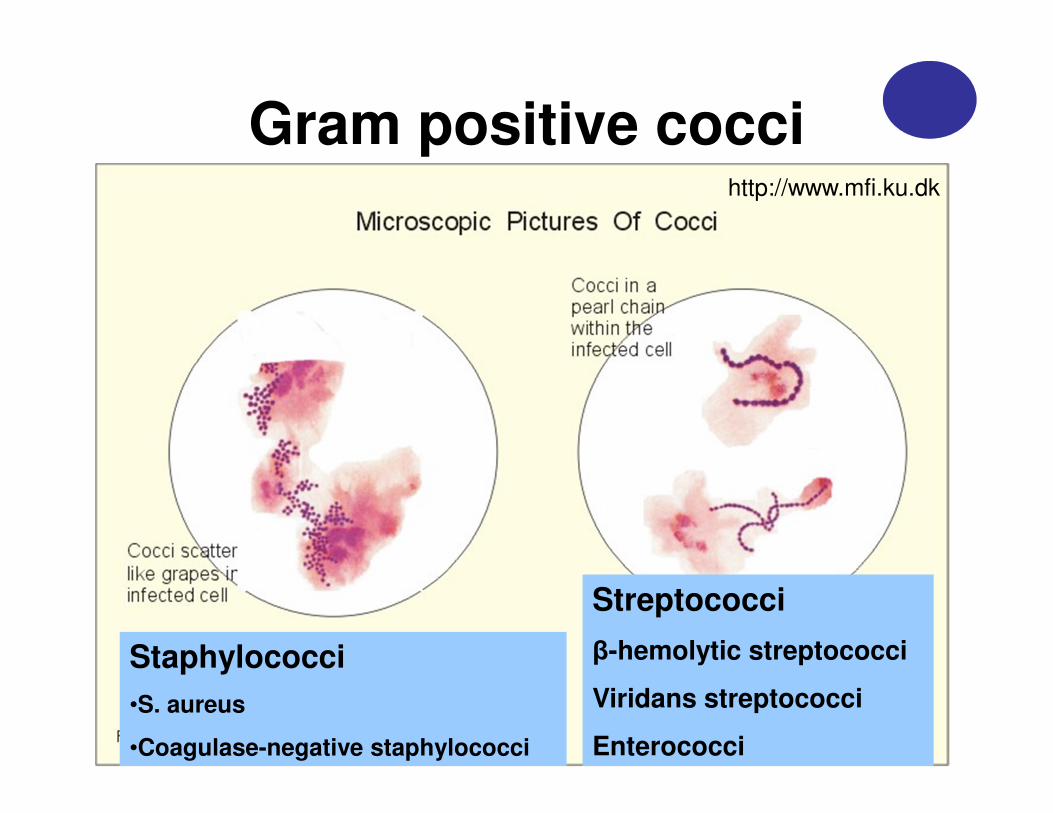
Gram positive coccihttp://www.mfi.ku.dk
Staphylococci
•S. aureus
•Coagulase-negative staphylococci
Streptococci
β-hemolytic streptococci
Viridans streptococci
Enterococci
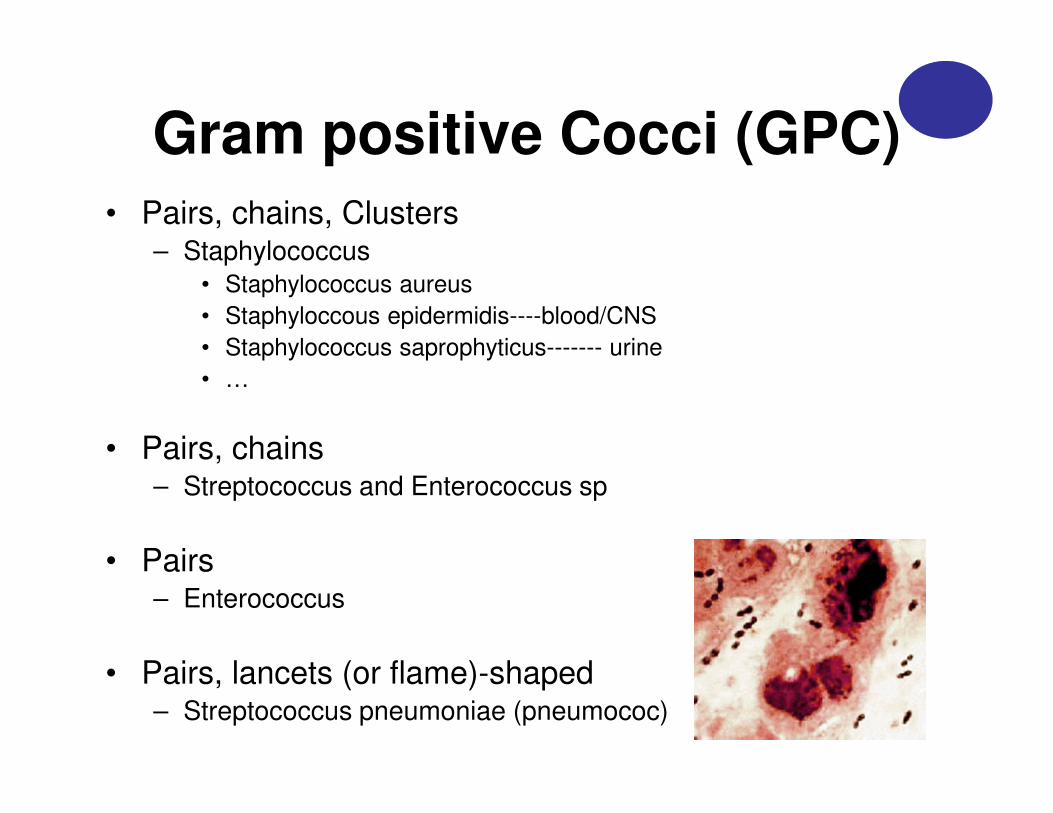
Gram positive Cocci (GPC)• Pairs, chains, Clusters
– Staphylococcus
• Staphylococcus aureus
• Staphyloccous epidermidis----blood/CNS
• Staphylococcus saprophyticus------- urine
• …
• Pairs, chains– Streptococcus and Enterococcus sp
• Pairs– Enterococcus
• Pairs, lancets (or flame)-shaped– Streptococcus pneumoniae (pneumococ)
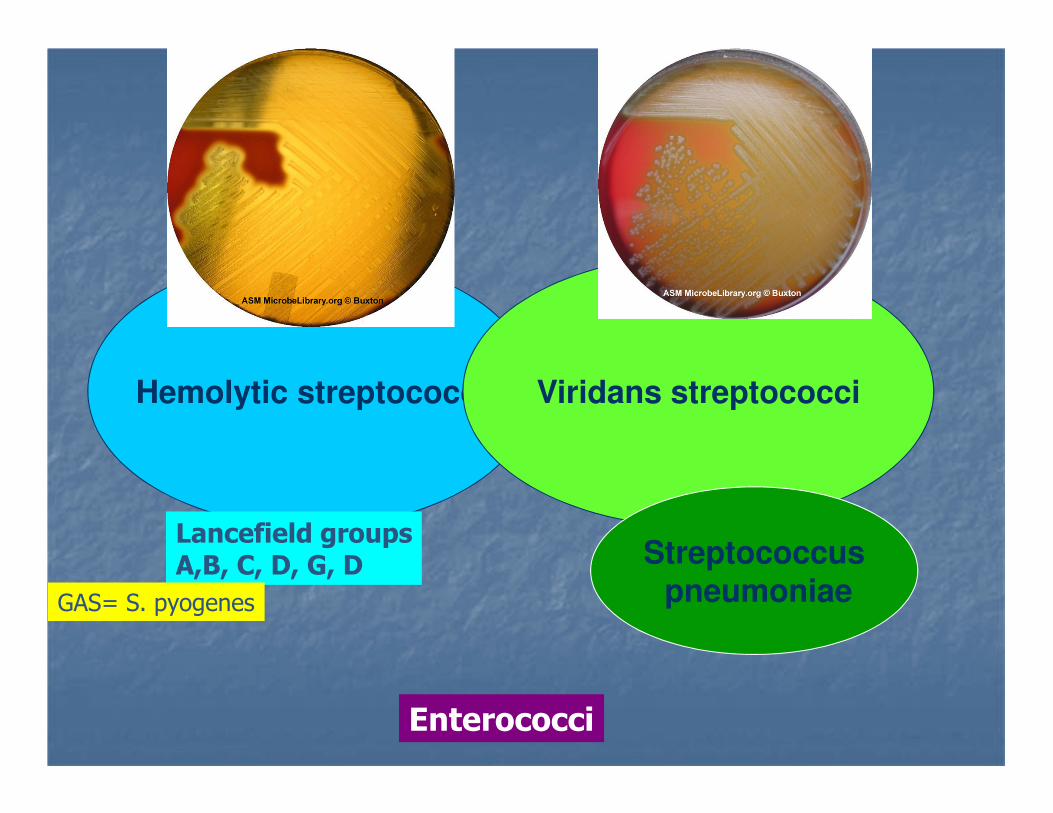
Hemolytic streptococci Viridans streptococci
Streptococcuspneumoniae
Lancefield groupsA,B, C, D, G, D
GAS= S. pyogenes
Enterococci

Gram Negative Cocci ( GNC)
• Diplococci (pairs, like beans): • Neisseria meningitidis
• Neisseria gonorrhea
• Moraxella catarralis

Gram Positive Bacilli (GPB)
• Diphtheroids– Small, pleomorphic
• Corynebacterium, Propionibacterium
– Large with spores• Clostridium sp• Bacillus sp
– Others: • Listeria sp ( Blood and CSF)
• Lactobacillus sp (vaginal/blood)
– Branching, beaded, rods:• Nocardia sp• Actinomyces sp
Mostly contaminants!
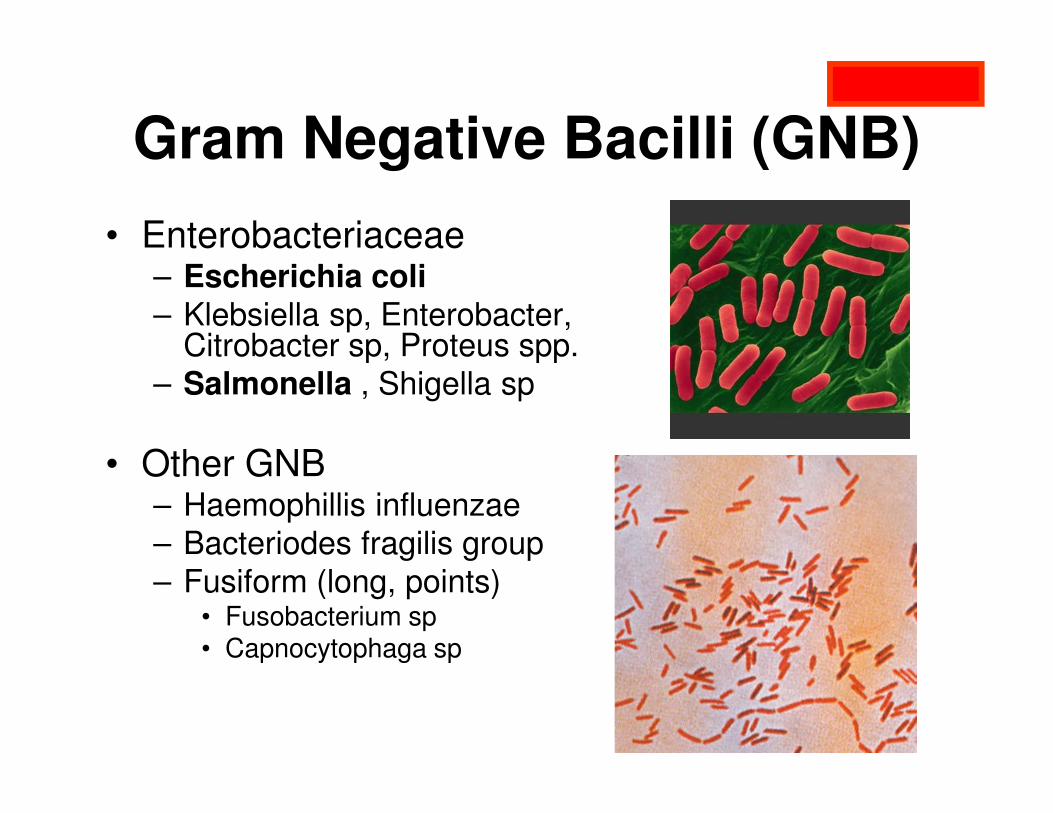
Gram Negative Bacilli (GNB)
• Enterobacteriaceae– Escherichia coli– Klebsiella sp, Enterobacter,
Citrobacter sp, Proteus spp.
– Salmonella , Shigella sp
• Other GNB– Haemophillis influenzae
– Bacteriodes fragilis group
– Fusiform (long, points)• Fusobacterium sp• Capnocytophaga sp
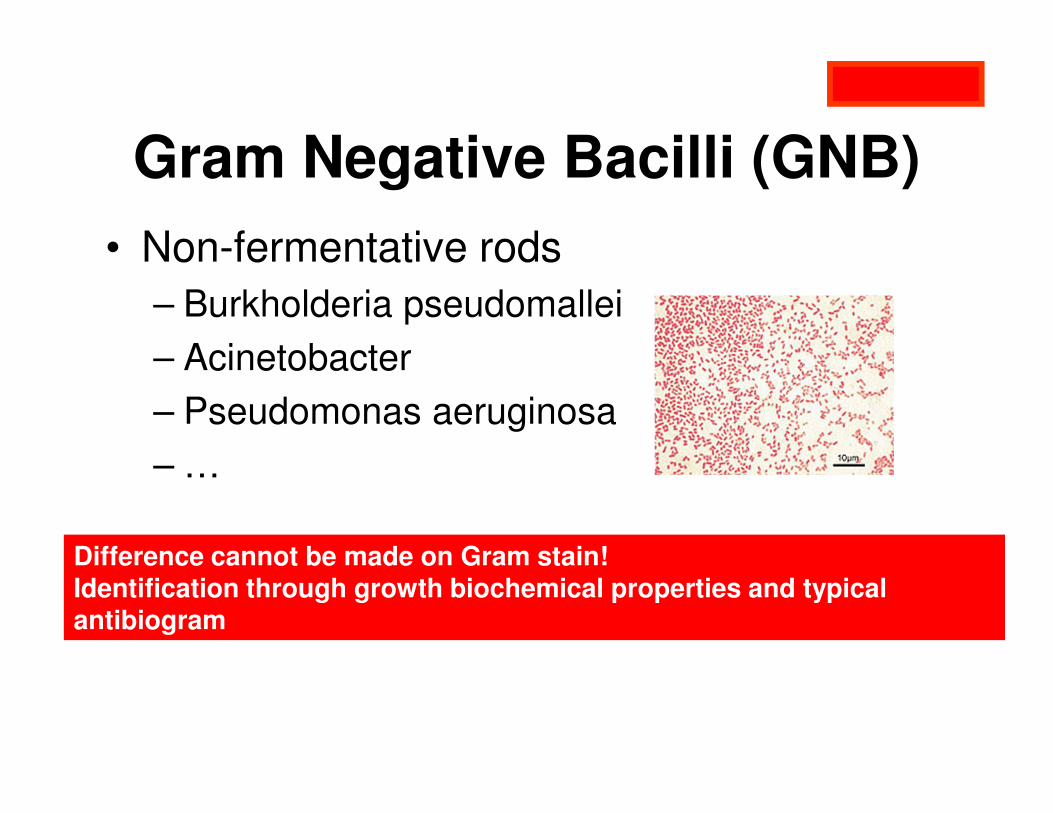
• Non-fermentative rods
– Burkholderia pseudomallei
– Acinetobacter
– Pseudomonas aeruginosa
– …
Difference cannot be made on Gram stain!Identification through growth biochemical properties and typical antibiogram
Gram Negative Bacilli (GNB)
Antibiogram interpretation
1. Look for the name of the bacteria
• Is this a ‘true’ pathogen (causing the disease) e.g.– Staphylococcus aureus
– E coli and other Gram negative bacilli
• Or is this more likely a contaminant e.g.– Coagulase negative Staphylococci
– Bacillus
– Corynebacterium
Choose antibiotics!
No antibiotics needed!!
• if you think your patient needs antibiotics…

2. Look for the first choice antibiotic
• Each bacterium has ‘first choice’ antibiotics
• Best activity, smallest spectrum,…
• Should be written in treatment guideline
• Staphylococcus aureus � cloxacillin
• Pneumococ � penicillin G
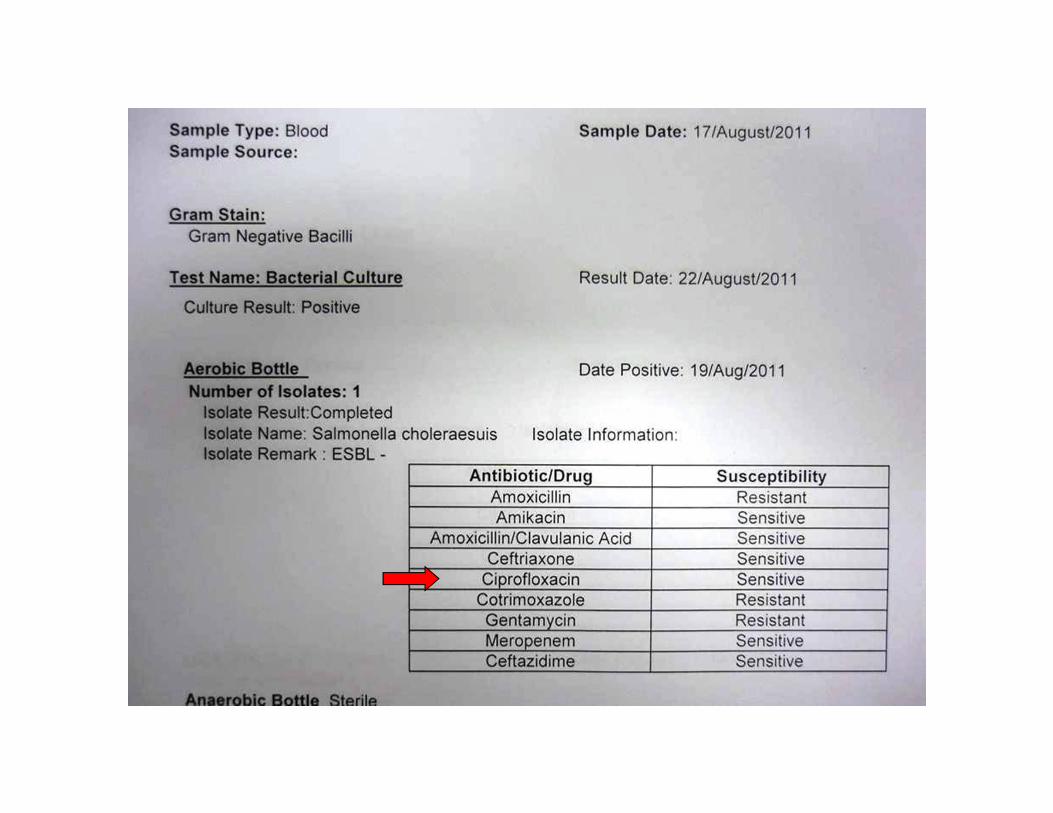
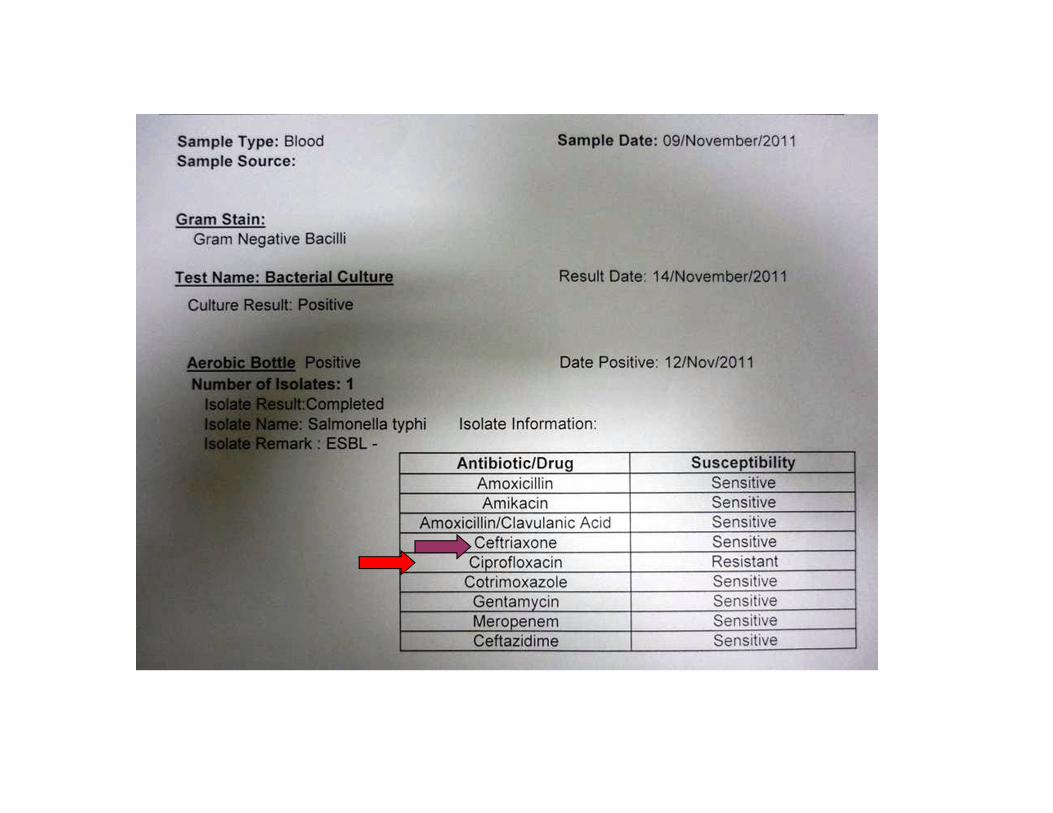
• Salmonella species � ciprofloxacin
• E. coli � ciprofloxacin, ampicillin, Augmentin

3. If the first choice AB shows ‘S’
• Then you prescribe the first choice AB!
– According to your local guidelines & availability
– With the smallest spectrum possible
– Dose according to the disease severity e.g.
• S aureus causing skin infection
» Cloxacillin PO 500 mg q6
• S aureus causing blood stream infection/sepsis
» Cloxacillin IV 1-2 g q4-6
4. If the first choice shows ‘R’
• Use the ‘second choice’ antibiotic
– As listed in guidelines
– Or: with known good activity against this bacterium
– AND with the smallest spectrum possible
Example1: Staphylococcus aureus
• Cloxacillin R (MRSA)
– Serious infection� use vancomycin if possible
– Mild infection� use cotrimoxazole (or lincomycin) if ‘S’


Example 2: E. coli
• Ampicillin R � use Augmentin or ciprofloxacin
• Ciprofloxacin R � use Augmentin (if S) or Ceftriaxone
• Augmentin R � check if also Ceftriaxone R (likely ESBL+)
• � use ciprofloxacin, cotrimoxazole (if S)
• � if all other AB R: use meropenem (if available)
• Ceftriaxone R � serious infections: use meropenem (if available)
• � mild infections: use cotrimoxazole, ciprofloxacin (if S)
• � UTI: use nitrofurantoin (if S)
Use only meropenem if serious and if you have no other possibility
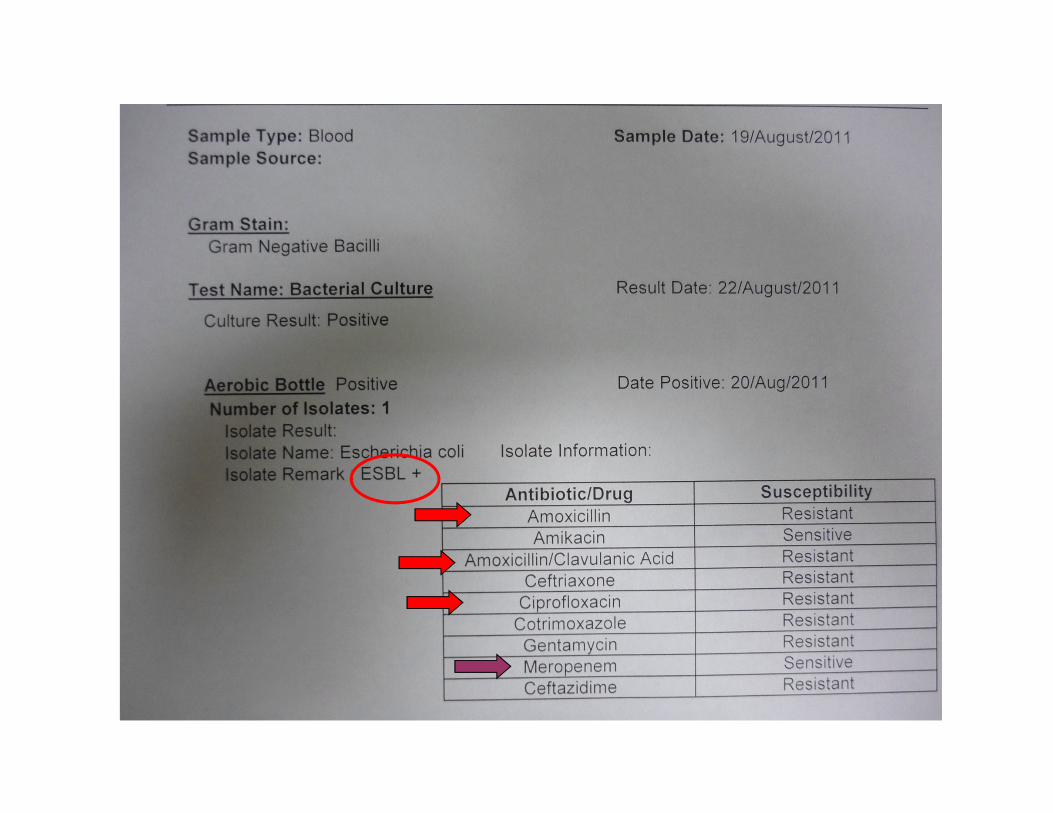

ESBL Extended Spectrum Beta-
Lactamase• Lives in bowel bacteria (E.coli, Klebsiella, …)
•Hydrolizes (destroys) all ‘beta-lactam antibiotics’–Penicillin, ampicillin, Augmentin
–Ceftriaxone, cefuroxime and other cephalosporins–Often co-resistant to ciprofloxacin, cotrimoxazole, gentamicin

ESBL• Extended spectrum beta-lactamase
• Treatment options:
– Severe disease:
• carbapenem( meropenem or imipenem)
• amikacin (use ALWAYS in combination)
– Moderate disease:
• Is treatment necessary, is I&D alone enough,…
• Check if you can use cotrimoxazole or ciprofloxacin
• Only if no other option use carbapenem
– UTI: nitrofurantoin (if ‘S’)
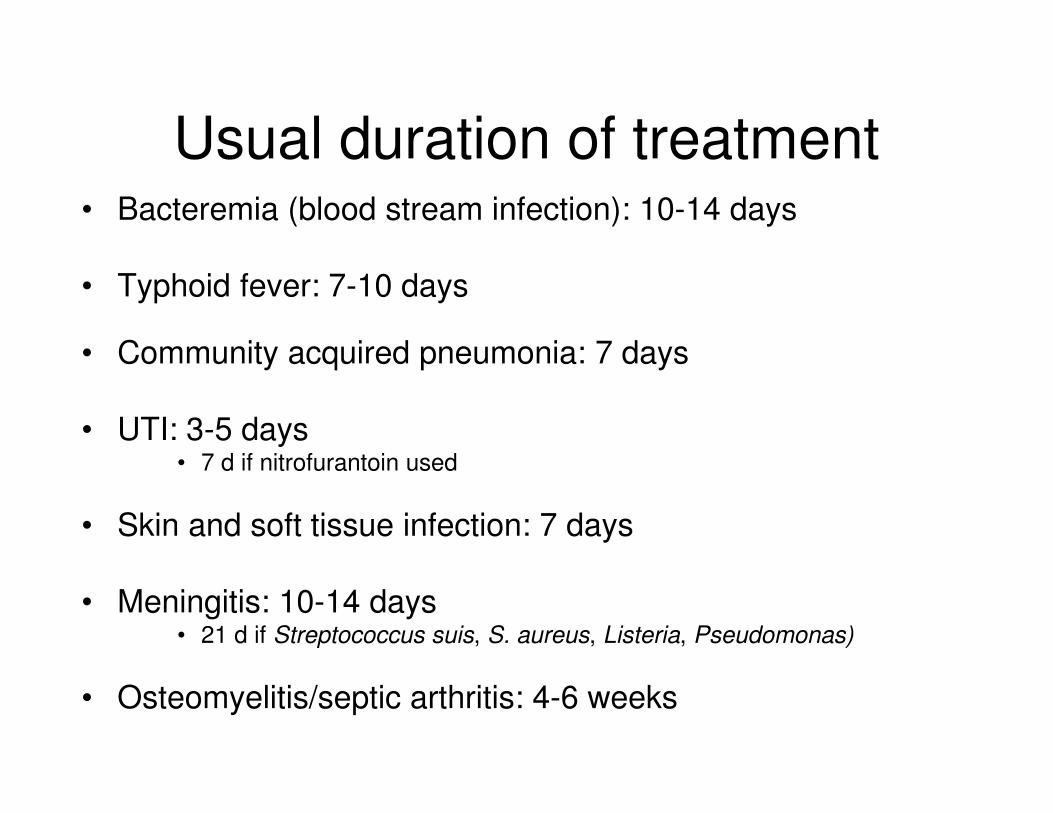
Usual duration of treatment• Bacteremia (blood stream infection): 10-14 days
• Typhoid fever: 7-10 days
• Community acquired pneumonia: 7 days
• UTI: 3-5 days• 7 d if nitrofurantoin used
• Skin and soft tissue infection: 7 days
• Meningitis: 10-14 days• 21 d if Streptococcus suis, S. aureus, Listeria, Pseudomonas)
• Osteomyelitis/septic arthritis: 4-6 weeks
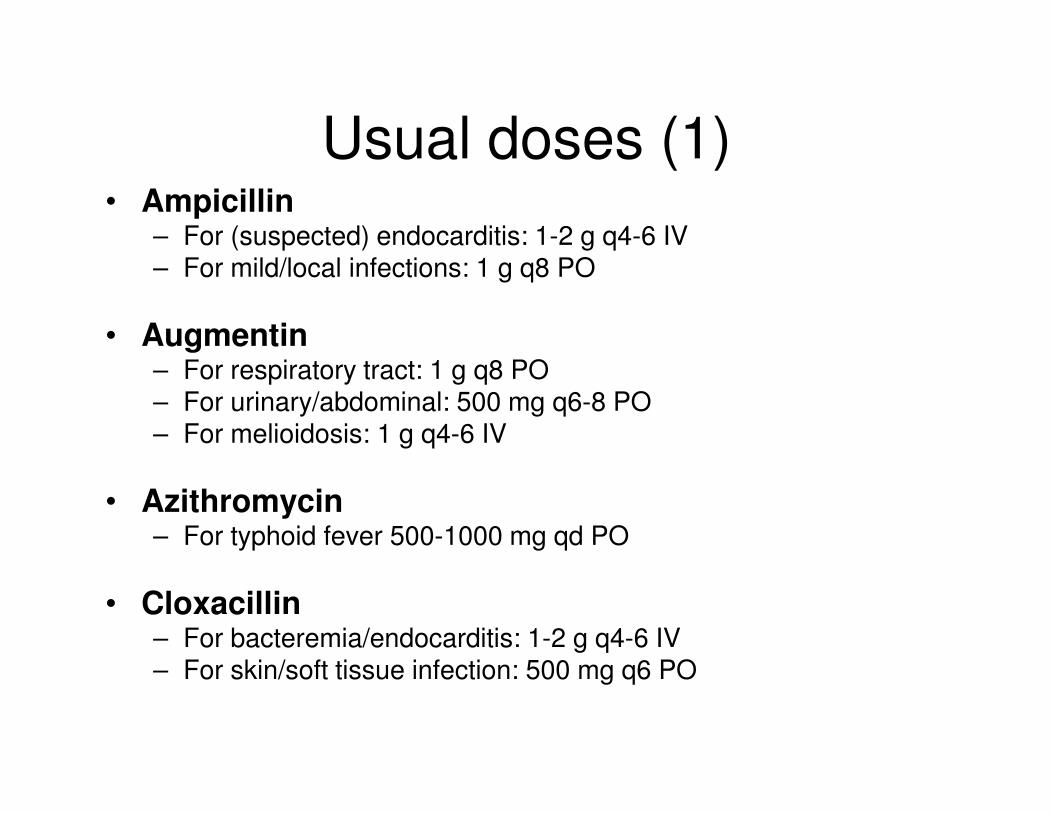
Usual doses (1)• Ampicillin
– For (suspected) endocarditis: 1-2 g q4-6 IV– For mild/local infections: 1 g q8 PO
• Augmentin– For respiratory tract: 1 g q8 PO– For urinary/abdominal: 500 mg q6-8 PO– For melioidosis: 1 g q4-6 IV
• Azithromycin– For typhoid fever 500-1000 mg qd PO
• Cloxacillin– For bacteremia/endocarditis: 1-2 g q4-6 IV– For skin/soft tissue infection: 500 mg q6 PO
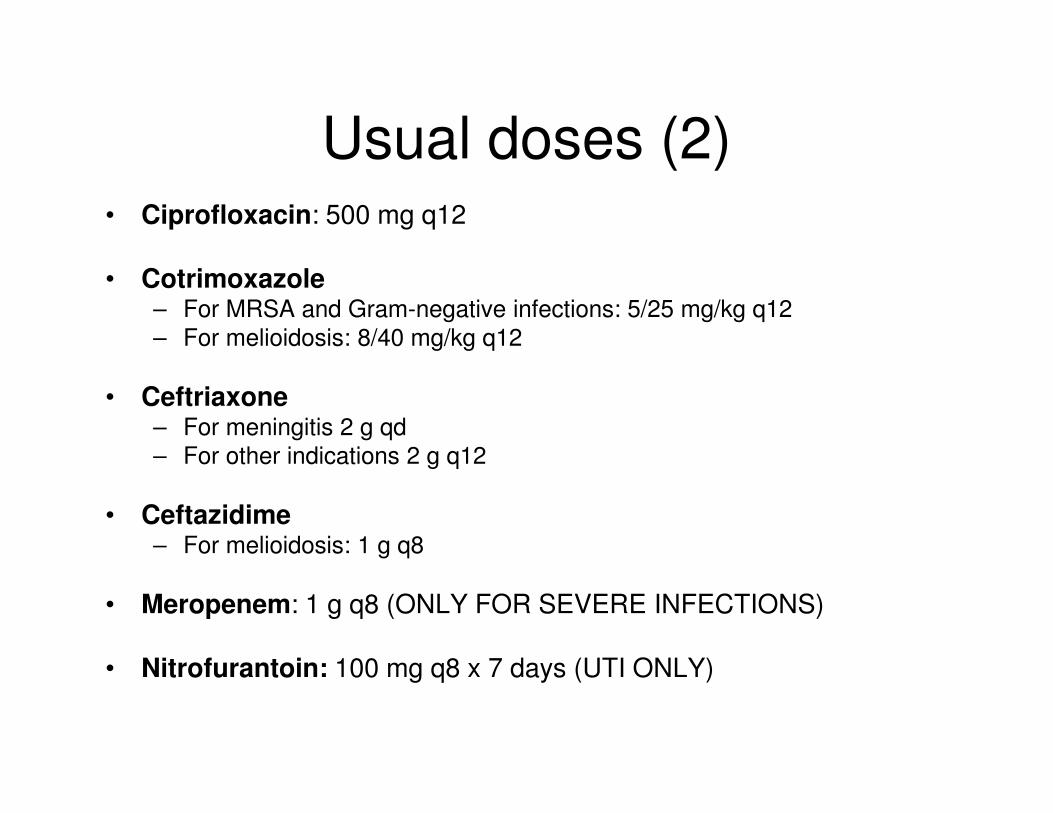
Usual doses (2)• Ciprofloxacin: 500 mg q12
• Cotrimoxazole– For MRSA and Gram-negative infections: 5/25 mg/kg q12
– For melioidosis: 8/40 mg/kg q12
• Ceftriaxone– For meningitis 2 g qd
– For other indications 2 g q12
• Ceftazidime– For melioidosis: 1 g q8
• Meropenem: 1 g q8 (ONLY FOR SEVERE INFECTIONS)
• Nitrofurantoin: 100 mg q8 x 7 days (UTI ONLY)

Thank you for your attention!