guidance of post myocardial infarction ventricular septal defect and pseudoaneurysm closure
TRANSCRIPT
ECHOCARDIOGRAPHY (RM LANG, SECTION EDITOR)
Guidance of Post Myocardial Infarction Ventricular Septal Defectand Pseudoaneurysm Closure
Itzhak Kronzon & Carlos E. Ruiz & Gila Perk
Published online: 29 January 2014# Springer Science+Business Media New York 2014
Abstract Left ventricular pseudoaneurysm and ventricularseptal defect are rare but devastating complications of myo-cardial infarction. With medical treatment alone, the majorityof patients will die from these complications. Until recently,the recommended treatment was surgical closure. These sur-geries carried extreme risk due to abnormal hemodynamics,necrotic substrates and the comorbidities of these patients.Recently, trans-catheter closure was shown to be an acceptablealternative to open surgical intervention. 3D echocardiogra-phy identifies the location, size, and shape of the defect andcan assess, guide, and follow up the closure procedure.
Keywords Left ventricular pseudoaneurysm . Ventricularseptal defect . 3-dimensional echocardiography .
Trans-catheter repair . Post myocardial infarction .
Pseudoaneurysm closure
Introduction
This chapter discusses the use of transcatheter procedures inthe treatment of two important complications of acute myo-cardial infarction; left ventricular pseudoaneurysm and ven-tricular septal defect.
Medical treatment of these patients carries very pooroutcomes with very high mortality rates. Surgery to closethe defects (frequently with coronary artery bypass as well)has better results, but still involves high mortality rates.
Transcatheter closure of these conditions is feasible and maybe an alternative therapy in these patients with hemodynamicinstability and other comorbidities. Real time 3D echocardiog-raphy is an important imaging modality in the diagnosis and theassessment of these structural heart diseases and has a significantrole in guiding and monitoring the interventional procedures.
Transcatheter Closure of Left VentricularPseudoaneurysm
Left ventricular free wall rupture is the most common acutetear of the left ventricle in patients with acute myocardialinfarction. Unfortunately, in most patients acute free wall tearleads to severe intra-pericardial bleeding which rapidly resultsin cardiac tamponade and death. Therefore, although free-walltear accounts for 14-20 % of all myocardial infarction relateddeaths, it is seen in only 7 % of in-hospital myocardialinfarction related deaths [1]. In other words, most cases ofdeath from acute free wall rupture occur before arrival in thehospital.
On rare occasions, the rupture is contained by pericardialand fibrous tissue, creating a left ventricular pseudoaneurysm.Characteristically, the orifice of the pseudoaneurysm is nar-row, with a characteristic to and fro blood flow; from the leftventricle into the pseudoaneurysm during systole, and fromthe pseudoaneurysm into the left ventricle during diastole. Thepseudoaneurysm wall is made of adherent pericardial or fi-brous tissue, without any myocardial or endocardial layers.Thus, this wall is thin and may easily rupture and causebleeding into the chest cavity and death. A meta-analysisreviewed the charts and reports of 290 patients with leftventricular pseudoaneurysm [2]. It demonstrated that approx-imately two thirds of all left ventricular pseudoaneurysmsoccur after myocardial infarction. Pseudoaneurysms are morecommon in men (75%), in Caucasians (75%) and the averageage of these patients is 60 years. The presenting symptoms in
This article is part of the Topical Collection on Echocardiography
I. Kronzon :G. Perk (*)Non Invasive Cardiology, Lenox Hill Hospital,100 E 77th St. 2E, New York, NY 10075, USAe-mail: [email protected]
C. E. RuizCardiac Imaging Laboratory, Lenox Hill Hospital,100 E 77th St. 2E, New York, NY 10075, USA
Curr Cardiol Rep (2014) 16:456DOI 10.1007/s11886-013-0456-1

infarct-related pseudoaneurysm include congestive heart fail-ure in 36 %, chest pain in 30 %, shortness of breath in 25 %,and sudden death in 3 %. Twelve percent are asymptomatic atthe time of presentation.
Imaging
Echocardiography suggests or establishes the diagnosis inmost cases. It shows a loculated echo-free space which com-municates with the left ventricle via a narrow neck, or tract;the ratio between the neck (communication) diameter and themaximal pseudoaneurysm diameter is less than 0.5. [3].
Doppler echocardiography demonstrates the characteristic toand fro flow in the communicating tract (from the LV to thepseudoaneurysm during systole, and from the pseudoaneurysmto the ventricle during diastole). Occasionally, when there is anecho free space near the left ventricle, but the communication isnot clearly seen, color Doppler and contrast echocardiographycan be used to demonstrate the abnormal communication [4].Real time 3D echocardiography can demonstrate the anatomyof the pseudoaneurysm and define the size and shape of thecommunication.
In the meta-analysis mentioned earlier, the maximal diam-eter of the pseudoaneurysm varied from 1.5 to 20 cm. Thepseudoaneurysm involved the posterior and lateral walls morecommonly than the anterior wall.
Other diagnostic imaging modalities include chest X ray,which demonstrates abnormal cardiac silhouette in 65 %,cardiac computed tomography, magnetic resonance imaging,radionuclide studies, and contrast left ventriculography [5].
Pseudoaneurysms can also occur after mitral valve replace-ment, with a rupture near the posterior aspect of the mitralring. Other conditions that may lead to LV pseudoaneurysmformation include aortic valve replacement, endocarditis withabscess formation, and cardiac trauma.
Clinical Course and Treatment Options
Infarction related pseudoaneurysm is an ominous complica-tion. Surgery is considered the treatment of choice, however itis frequently unsuccessful. Suturing into the necrotic myocar-dium may fall apart. The quoted surgical mortality is 23 %.Medical therapy has higher mortality (30-45 %) [2].
Transcatheter repair of pseudoaneurysm is now anothertreatment option. It is best done under fluoroscopic as wellas two dimensional (2D) and real time 3 dimensional (3D)TEE and TTE surveillance and guidance [6•]. The 3D imagecan be helpful in the selection of the closure device. Otherimaging modalities such as CT scan are frequently used aswell in preparation for surgical or trans-catheter procedure.
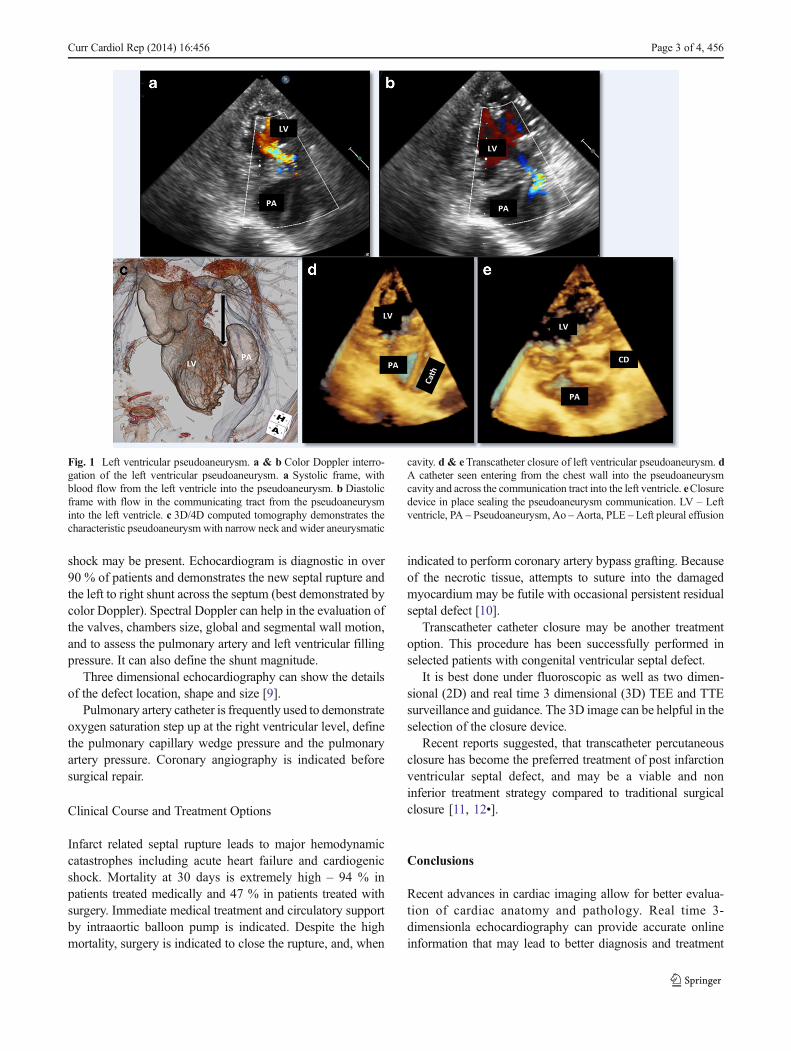
Figure 1 shows a case of an anterior wall infarct with alarge pseudoaneurysm.
After establishing the diagnosis, a decision was made toclose the PAvia an apical approach. Using 3D real time TEE, adirect percutaneous needle puncture of the pseudoaneurysmwas performed, and a wire, and then a catheter were advancedfrom the puncture site through the communicating tract intothe LV cavity (Fig. 1). A closure device (Amplatzer) was thendeployed to close the communication. Upon withdrawal of allcatheters, another Amplatzer closure device was deployed atthe pseudoaneurysm puncture site. The patient recoveredwithout complications.
The aneurysmal cavity can be approached from the leftventricular cavity or by chest wall puncture, as in the casedescribed.
Smaller pseudoaneurysms can be closed by a coil, or evenby the combination of coil (to close the pseudoaneurysmcavity) and a closure device to close the communication.
Transcatheter Closure of Post Myocardial InfarctionRuptured Interventricular Septum
Rupture of the interventricular septum is one of the deadliestcomplications of acute myocardial infarction. The incidenceand the clinical course of the disorder had changed dramati-cally in the last few decades. The incidence prior to thethrombolytic era was 1-5 %. The incidence had declinedsignificantly to only 0.2 % in a large cohort of patients withacute myocardial infarction who underwent early reperfusiontherapy (GUSTO-1) [7]. Interestingly, the time interval fromthe index infarction to the diagnosis of septal rupture declinedconsiderably from 3 days in the pre-thrombolytic era to 1 dayin patients who underwent thrombolysis. While wall reperfu-sion may explain the decline in septal rupture, it was specu-lated that thrombolysis was responsible for peri-infarctionhemorrhage which resulted in earlier septal rupture.
Septal rupture is more common in older, hypertensivefemales. There are two anatomic variants of post infarctionseptal rupture. The first is the simple rupture of the apical andanterior septal wall, which opens to the right ventricle at thesame level. This rupture is associated with occlusion of the leftanterior descending coronary artery. The other type of septalrupture is the one seen with basal inferior infarction as a resultof right coronary artery occlusion. This septal rupture is oftena complex one which may be long and serpiginous and maystart at the base of the septum, and then open into the rightventricle at a different, more apical level [8].
Diagnostic Modalities and Imaging
Rupture of the septum is suspected in a patient with acutemyocardial infarctionwho suddenly deteriorates hemodynam-ically and develops a new harsh holosystolic murmur. Acuteheart failure, pulmonary edema, hypotension and cardiogenic
456, Page 2 of 4 Curr Cardiol Rep (2014) 16:456
shock may be present. Echocardiogram is diagnostic in over90 % of patients and demonstrates the new septal rupture andthe left to right shunt across the septum (best demonstrated bycolor Doppler). Spectral Doppler can help in the evaluation ofthe valves, chambers size, global and segmental wall motion,and to assess the pulmonary artery and left ventricular fillingpressure. It can also define the shunt magnitude.
Three dimensional echocardiography can show the detailsof the defect location, shape and size [9].
Pulmonary artery catheter is frequently used to demonstrateoxygen saturation step up at the right ventricular level, definethe pulmonary capillary wedge pressure and the pulmonaryartery pressure. Coronary angiography is indicated beforesurgical repair.
Clinical Course and Treatment Options
Infarct related septal rupture leads to major hemodynamiccatastrophes including acute heart failure and cardiogenicshock. Mortality at 30 days is extremely high – 94 % inpatients treated medically and 47 % in patients treated withsurgery. Immediate medical treatment and circulatory supportby intraaortic balloon pump is indicated. Despite the highmortality, surgery is indicated to close the rupture, and, when
indicated to perform coronary artery bypass grafting. Becauseof the necrotic tissue, attempts to suture into the damagedmyocardium may be futile with occasional persistent residualseptal defect [10].
Transcatheter catheter closure may be another treatmentoption. This procedure has been successfully performed inselected patients with congenital ventricular septal defect.
It is best done under fluoroscopic as well as two dimen-sional (2D) and real time 3 dimensional (3D) TEE and TTEsurveillance and guidance. The 3D image can be helpful in theselection of the closure device.
Recent reports suggested, that transcatheter percutaneousclosure has become the preferred treatment of post infarctionventricular septal defect, and may be a viable and noninferior treatment strategy compared to traditional surgicalclosure [11, 12•].
Conclusions
Recent advances in cardiac imaging allow for better evalua-tion of cardiac anatomy and pathology. Real time 3-dimensionla echocardiography can provide accurate onlineinformation that may lead to better diagnosis and treatment
Fig. 1 Left ventricular pseudoaneurysm. a & b Color Doppler interro-gation of the left ventricular pseudoaneurysm. a Systolic frame, withblood flow from the left ventricle into the pseudoaneurysm. b Diastolicframe with flow in the communicating tract from the pseudoaneurysminto the left ventricle. c 3D/4D computed tomography demonstrates thecharacteristic pseudoaneurysm with narrow neck and wider aneurysmatic
cavity. d & eTranscatheter closure of left ventricular pseudoaneurysm. dA catheter seen entering from the chest wall into the pseudoaneurysmcavity and across the communication tract into the left ventricle. eClosuredevice in place sealing the pseudoaneurysm communication. LV – Leftventricle, PA – Pseudoaneurysm, Ao –Aorta, PLE – Left pleural effusion
Curr Cardiol Rep (2014) 16:456 Page 3 of 4, 456

of catastrophic complications of acute myocardial infarction,namely left ventricular pseudoaneurysm and ventricular septaldefect. It is hoped that the less invasive approach will lead tobetter results and improved survival of patients suffering fromthese complications.
Compliance with Ethics Guidelines
Conflict of Interest Itzhak Kronzon has been a consultant for St. JudeMedical and has received speaker honoraria from Philips Healthcare.
Carlos Ruiz declares that he has no conflict of interest.Gila Perk declares that she has no conflict of interest.
Human and Animal Rights and Informed Consent This article doesnot contain any studies with human or animal subjects performed by anyof the authors.
References
Papers of particular interest, published recently, have beenhighlighted as:• Of importance
1. Reddy SG, RobertsWC. Frequency of rupture of the left ventricularfree wall or ventricular septum among necropsy cases of fatal acutemyocardial infarction since the introduction of coronary care units.Am J Cardiol. 1989;63:906–11.
2. Frances C, Romero A, Grady D. Left ventricular pseudoaneurysm.J Am Coll Cardiol. 1998;32:557–61.
3. Gatewood RP, Nanda NC. Differentiation of left ventricularpseudoaneurysm from true aneurysm with two dimensional echo-cardiography. Am J Cardiol. 1980;46:869–78.
4. Tunick PA, Slater W, Kronzon I. The hemodynamics of left ven-tricular psudoaneurysm—color doppler echocardiographic study.Am Heart J. 1989;117:116–7.
5. Narayan RL, Vaishnava P, Goldman ME, et al. Percutaneous clo-sure of left ventricular pseudoaneurysm. Ann Thorac Surg.2012;94:e123–5.
6.• Dudiy Y, Jelnin V, Einhorn BN, Kronzon I, Cohen HA, Ruiz CE.Percutaneous closure of left ventricular pseudoaneurysm. CircCardiovasc Interv. 2011;4:322–6. This is a single institution ex-perience which describes in details the use of trans-catheterclosure of left ventricular pseudoaneurysm and the imagingmodalities used.
7. Crenshaw BS, Granger CB, Birnbaum Y, et al. Risk factors, angio-graphic patterns, and outcomes in patients with ventricular septaldefect complicating acute myocardial infarction GUSTO-1 trialinvestigators. Circulation. 2000;101:27–32.
8. Yip HK, Wu CJ, Chang HW, et al. Cardiac rupture complicatingacute myocardial infarction in the direct PCI reperfusion era. Chest.2003;124:565–71.
9. Halperin DG, Perk C, Ruiz CE, et al. Percutaneous closure of postmyocardial infaction ventricular septal defect guided by three di-mensional echocardiography. Eur J Echocardiogr. 2009;10:569–71.
10. Kulkarni M, Conte HA, Hut A, et al. Coronary artery disease, acutemyocardial infarction and newly developing ventricular septal de-fect: surgical repair or closure. J Cardiothorac Vasc Anesth.2011;25:1213–18.
11. Sathananthan J, Ruyarok P. Evolution in the management of postinfarct ventricular septal defects from surgical topercutaneous ap-proach: a single center experience. J Invasive Cardiol. 2013;25:339–43.
12.• Zhu XY, Qin YW, Han YL, et al. Long term efficiency of trans-catheter closure of ventricular septal defect in combination withpercutaneous coronary intervention in patients with ventricularseptal defect complicating acute myocardial infarction: a multicen-ter study. EuroIntervention. 2013;8:1270–6. A multicenter studythat shows that trans-catheter closure of ventricular septal defectis associated with significantly better outcomes.
456, Page 4 of 4 Curr Cardiol Rep (2014) 16:456