good grief and not-so-good grief: countertransference in bereavement therapy
TRANSCRIPT

Good Grief and Not-So-Good Grief:Countertransference in Bereavement Therapy
�
Jeffrey A. Hayes, Yun-Jy Yeh, and Alanna Eisenberg
Pennsylvania State University
This study examined the relationship between therapists’ grief related tothe death of a loved one and clients’ perceptions of the process of bereave-ment therapy. Mail survey data were obtained from 69 client–therapistdyads. Results indicated that the extent to which therapists missed deceasedloved ones was inversely related to client perceptions of therapist empa-thy, but not to client ratings of the alliance, session depth, or therapistcredibility. Therapist acceptance of the death of a loved one was unrelatedto any of the dependent measures. Results are discussed in terms of coun-tertransference and its management. © 2007 Wiley Periodicals, Inc. J ClinPsychol 63: 345–355, 2007.
Keywords: grief; bereavement therapy; countertransference
The effects of the therapist’s well-being on the quality of therapy have long been recog-nized. Freud (1910/1959) wrote that “every analyst’s achievement is limited by what hisown complexes and resistances permit” (pp. 144–145) Theorists from humanistic (Rogers,2000), feminist (Brown, 2001), and existential (May, 1939/1989) camps have expressedsimilar sentiments about the importance of the therapist’s mental health. Even cognitive-behavioral theorists, who tend to emphasize technical factors in therapy, increasinglyrecognize the importance of the person of the therapist in treatment (e.g., Ellis, 2001,2003). Thus, theorists from a variety of theoretical persuasions acknowledge the impor-tant role that the therapist’s personal history and welfare can play in therapy.
Research is beginning to provide empirical foundations for what theorists and clini-cians have known in this area. For example, a meta-analysis conducted by Ahn andWampold (2001) concluded that therapist variables contribute more variability to out-come than do treatment-specific components; however, note that there is not universal
This study was supported by a Research Initiation Grant from the College of Education at Pennsylvania StateUniversity. Correspondence regarding this article may be addressed to: Jeffrey A. Hayes, 312 Cedar Building,Pennsylvania State University, University Park, PA 16802; e-mail: [email protected]
JOURNAL OF CLINICAL PSYCHOLOGY, Vol. 63(4), 345–355 (2007) © 2007 Wiley Periodicals, Inc.
Published online in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/jclp.20353
agreement on the relative importance of therapist and intervention-related variables (e.g.,Elkin, Falconnier, Martinovich, & Mahoney, 2006). While debate exists about the impor-tance of therapist effects, little empirical work is being devoted to therapist variables of apersonal nature that affect the process and outcome of therapy. In fact, Beutler et al.’s(2004) review of therapist variables noted the dearth of studies on the nature of thetherapist, despite a call a decade earlier for research on topics including the effects of“emotional problems on the part of the therapist” (Beutler, Machado, & Neufeldt, 1994,p. 238).
The therapist’s emotional problems fell under the realm of what Freud (1910/1959)referred to as “countertransference.” He used the term to refer specifically to the therapist’sunconscious defensive reactions to transference. Although countertransference has beendefined subsequently in a number of ways, most definitions acknowledge, to varyingdegrees, that therapists’ reactions to clients may be adversely influenced by therapists’unresolved personal conflicts. Research has demonstrated, for instance, that when ther-apists’ unresolved issues are provoked, they may display avoidance behavior, engage inreactive as opposed to reflective thinking, feel anxious, and be prone to distorted percep-tions of clients (Cutler, 1958; Hayes & Gelso, 1991, 1993; Latts & Gelso, 1995; McClure& Hodge, 1987; Normandin & Bouchard, 1993; Rosenberger & Hayes, 2002). Clients, inturn, may develop weaker alliances with therapists and perceive them to be less empathicwhen therapists display countertransference behavior (Ligiero & Gelso, 2002; Peabody& Gelso, 1982). Much of the research on countertransference, however, has been con-ducted in artificial laboratory settings using analogue designs with therapist trainees andsimulated clients. Whereas these studies have put a premium on internal validity bymaximizing control over independent variables, they have done so at the expense ofexternal validity. Thus, in the present study, we sought to obtain data from experiencedtherapists and real clients in actual field settings.
Research indicates that therapists’ unresolved issues may be stimulated by a numberof factors. For example, the content of a client’s verbalizations can trigger countertrans-ference, as can aspects of the client that remind the therapist of significant people in thetherapist’s life, including him- or herself (Hayes et al., 1998; McClure & Hodge, 1987;Sharkin & Gelso, 1993). In other words, when the client discusses problems that arerelated to the therapist’s issues, countertransference reactions may be provoked. In thepresent study, we were interested in investigating this phenomenon in the context ofbereavement therapy. We chose to study bereavement therapy because of the near uni-versality of grief and because an instrument existed to measure therapist conflict resolu-tion in this area.
In particular, this study examined clients’ perceptions of the process of bereavementtherapy as a function of therapists’ grief related to the death of a loved one. We chose toexamine four indicators of therapy process: therapist empathy, therapist credibility, theworking alliance, and session depth. The choice of these variables was guided by severalfactors. First, we believed that these four variables are germane to effective bereavementtherapy across therapist theoretical orientations. Second, previous research has used thissame set of indicators in studying the quality of therapy process (e.g., Li & Kim, 2004).Finally and most importantly, in the context of bereavement therapy, each variable theo-retically is affected by the extent to which therapists have resolved their own grief. Forexample, the more that therapists are grieving the death of someone close to them, themore focused on themselves they might be and the less attention they might have avail-able to empathize with clients. Alternatively, having experienced the death of a loved oneand resolved one’s grief sufficiently, a therapist may be especially able to empathize witha client’s loss. Similarly, therapists who have experienced and worked through the death
346 Journal of Clinical Psychology, April 2007
Journal of Clinical Psychology DOI 10.1002/jclp

of someone close to them may be seen as particularly credible by grieving clients. Theycan reflect on their own experiences to inform treatment decisions, make judicious self-disclosures, and offer genuine hope borne of their own pain. On the other hand, therapistswho are still immersed in their own grief may function at a less than optimal level pro-fessionally and therefore be perceived by clients as generally less expert and credible.Along similar lines, because therapists can feel anxious and behave avoidantly whenclients discuss issues related to therapists’ unresolved conflicts, therapists who are strug-gling with grief may have difficulty staying connected to and on topic with grievingclients, thus undermining the working alliance and limiting session depth. On the whole,then, we hypothesized that therapists’ grief resolution would be directly related to clients’positive perceptions of the process of bereavement therapy along each of these fourdimensions.
Method
Participants
Participants were 69 therapists who had experienced the death of a loved one (71%women; 89% White), and 69 of their clients. Therapists ranged in age from 32 to 83 years(M � 53.5, SD � 8.6), and their mean level of therapy experience was 15.8 years (SD �9.1). Sixty-nine percent of therapists possessed master’s degrees, and 29% had doctoraldegrees. Ninety-one percent worked primarily in private practice settings. Approximatelyhalf (48%) of the therapists described their theoretical orientation as eclectic, 22% ascognitive-behavioral, 8% as systems oriented, 7% as humanistic, 7% as psychodynamic/psychoanalytic, and 8% as other. On average, therapists had experienced their most sig-nificant loss due to the death of a loved one 15.3 years prior to data collection (SD �12.5,range � 1–52 years).
Of the 69 clients in this study, 90% were women and 92% were White. Their meanage was 46.5 years (SD �12.8). Fifteen percent of clients had experienced the death of aloved one within the previous 3 months, 15% 3 to 6 months prior to data collection, 19%6 to 9 months previously, and 52% more than 9 months previously. Clients had been intherapy with their current therapist for an average of 24.0 sessions (SD � 36.8).
Measures
Barrett-Lennard Relationship Inventory-Form OS-40, Empathy (BLRI-E; Barrett-Lennard, 1962). The BLRI-E was used to measure client perceptions of therapist empa-thy. Although the BLRI contains multiple subscales, only the Empathy subscale was usedin the present study. This subscale contains 10 items that are rated from �3 (strongly nottrue) to �3 (strongly true). Higher scores reflect greater empathy. Examples of items are“My counselor usually understands the whole of what I mean” and “My counselor appre-ciates exactly how the things I experience feel to me.” The BLRI has demonstratedconsistently strong psychometric properties throughout its history (Barrett-Lennard, 1986).In the present study, Cronbach’s alpha was .82.
Counselor Effectiveness Rating Scale (CERS; Atkinson & Carskaddon, 1975). TheCERS assesses client perceptions of therapist credibility. The CERS is a 10-item seman-tic differential questionnaire that measures therapist expertness, attractiveness, and trust-worthiness. Higher scores indicate greater perceived therapist credibility. Internalconsistency estimates for the CERS tend to exceed .80 (Atkinson & Wampold, 1982).
Bereavement Therapy 347
Journal of Clinical Psychology DOI 10.1002/jclp

Cronbach’s alpha was .86 in the present study. Evidence of concurrent validity has beenfound through a correlation of .80 between the Therapist Rating Form (Barak & LaCrosse,1975) and the CERS (Atkinson & Wampold, 1982).
Working Alliance Inventory-Short Version (WAI-S; Tracey & Kokotovic, 1989). TheWAI-S is a 12-item self-report measure that was used to assess client perceptions of thestrength of the working relationship between therapist and client. Each item is rated on aLikert scale of 1 (never) to 7 (always). Higher scores indicate a stronger working alli-ance. Sample items include “My counselor and I are working toward mutually agreedupon goals” and “I believe my counselor likes me.” The WAI-S was developed from theoriginal WAI (Horvath & Greenberg, 1989) through confirmatory factor analysis thatsupported the validity of Bordin’s (1979) tri-partite theoretical model (agreement abouttasks, agreement about goals, and development of bonds). In the present study, only thetotal score was used. Internal consistency estimates range from .90 to .94 (Dunkle &Friedlander, 1996; Tracey & Kokotovic, 1989). Cronbach’s alpha was .88 in the presentstudy. Evidence for the validity of the WAI-S has been found through its positive rela-tionship to therapy outcome (Martin, Garske, & Davis, 2000).
Session Evaluation Questionnaire-Depth (SEQ-D; Stiles & Snow, 1984). The SEQ-Dwas used to measure client perceptions of session depth. The SEQ consists of 24 bipolaradjectives (e.g., “deep–shallow”) that are scored from 1 to 7. Subscales assess sessiondepth and smoothness, postsession mood, and arousal. In this study, only the five-itemDepth subscale was used. Higher scores reflect greater perceived session depth. Factoranalyses have supported the structural validity of the Depth scale, and the scale hasdemonstrated sensitivity to change across time in therapy (Stiles, Shapiro, & Firth-Cozens, 1988; Stiles & Snow, 1984). Internal consistency estimates among therapist,client, and observer ratings for Depth scores tend to range from .80 to .90 (Stiles et al.,1988). Cronbach’s alpha in the present study was .86.
Texas Revised Inventory of Grief (TRIG; Faschingbauer, Zisook, & DeVaul,1987). The TRIG was used to assess therapists’ grief resolution. The TRIG contains twosubscales: Past Behavior and Present Feelings. In this study, only the 13-item PresentFeelings subscale was used because we believed that therapists’ current emotional func-tioning would be more strongly related to their effectiveness in therapy than would theirbehaviors at the time they experienced a loss. Participants were instructed to completeitems with regard to the most significant loss they had experienced due to the death of aloved one. These directions were designed to prevent confounds due to other types of loss(e.g., divorce). Examples of items include “I still cry when I think of the person whodied” and “I am unable to accept the death of the person who died.” Each item is rated ona Likert scale of 1 (completely true) to 5 (completely false), and higher scores indicategreater grief resolution. Faschingbauer et al. (1987) reported an internal consistencyestimate of .86 and a split-half reliability of .88 for the Present Feelings scale, and in astudy of counselors’ reactions to termination, Boyer and Hoffman (1993) estimated inter-nal consistency to be .82. Despite these satisfactory internal consistency values, the scale’sauthors noted that there is relatively low shared variance among items and that items onthe Present Feelings subscale “are measuring grief from several different angles. . . .[including] thoughts, feelings, memories, opinions, and attitudes” (Faschingbauer et al.,1987, p. 120). It could be, then, that Present Feelings is a multidimensional scale, and thispossibility was investigated.
348 Journal of Clinical Psychology, April 2007
Journal of Clinical Psychology DOI 10.1002/jclp
First, it was determined that the correlation matrix among Present Feelings itemsfrom all 128 therapist respondents (discussed later) was factorable. Kaiser’s measure ofsampling adequacy was .83, above the desired level of .60, and Bartlett’s test of spheric-ity was statistically significant, x2 � 803.9, p � .01. A principal axis factor analysis wasthen conducted. Two factors were extracted based on a scree plot and the results ofparallel analysis (Lautenschlager, 1989). Parallel analysis is a method for determining thenumber of factors to retain based on the size of obtained eigenvalues relative to thoseexpected by chance. Critical eigenvalues, which are of a magnitude that would be expectedbased on chance given a particular sample size and a specific number of items on aninstrument, are extrapolated from tables. Then the magnitude of eigenvalues obtainedfrom one’s factor analysis is compared to these critical eigenvalues, and factors are retainedif obtained eigenvalues exceed critical eigenvalues. Parallel analysis yields more stablefactor solutions than simply retaining factors with eigenvalues greater than 1 (Zwick &Velicer, 1986).
The first factor that was extracted had an eigenvalue of 5.15 and accounted for 40%of the variance in the factor solution. The second factor had an eigenvalue of 2.02 andexplained 16% of the variance. The third factor had an eigenvalue of 1.01, smaller thanwhat would be expected based on chance alone, and was not retained. Items with load-ings greater than or equal to .45 and that loaded at least .10 higher on one factor than onthe other were used to interpret factors. Using this decision rule, 12 items loaded on eitherof the two factors. Oblique rotation resulted in two factors that were named “Acceptance”and “Missing” and that correlated .25. Acceptance consisted of 8 items such as “I cannotaccept this person’s death,” “I hide my tears when I think about the person who died,” and“I feel it’s unfair that this person died.” Missing comprised 4 items, including “Some-times I very much miss the person who died,” “Things and people around me still remindme of the person who died,” and “No one will ever take the place in my life of the personwho died.” Cronbach’s alpha was .87 for Acceptance and .63 for Missing.
Procedure
A sample of 500 therapists was identified from various online databases of therapists whodesignated bereavement therapy as one of their specialty areas. A prenotification letterwas mailed to these potential participants that described the study and invited their par-ticipation. Of the 500 potential participants, 31 were not eligible because they were notworking with a client on issues related to the death of a loved one, and 87 letters werereturned due to undeliverable addresses. Of the remaining 382 potential participants, 139completed and returned surveys, representing a 36% response rate. Eleven of these ther-apists indicated that they had never experienced the death of a loved one, and they wereremoved from the sample. Of the remaining 128 therapists, 69 had clients who returnedsurveys. These dyads constituted the final sample. Acceptance scores were similar fortherapists whose clients did and did not return surveys (M � 4.02 and 4.09, respectively),as were Missing scores (M � 2.61 and 2.55, respectively).
Therapists completed demographic questions and the TRIG, and mailed them back ina postage-paid return envelope. Therapists were asked to give a packet to the next clientwith whom they were addressing grief issues due to the death of a loved one. Clientscompleted the WAI, the CERS, the BLRI, and the SEQ in random order. Clients wereinstructed to complete all measures according to how they tended to view therapy or theirtherapist (as opposed to their last session). Clients mailed instruments back in a postage-paid return envelope separately from their therapists to assure confidentiality. A reminder
Bereavement Therapy 349
Journal of Clinical Psychology DOI 10.1002/jclp
letter was sent to therapist nonrespondents 3 weeks after the first mailing. Five weeksfollowing the first mailing, therapists who had not yet responded were sent a new coverletter and the same instruments that were contained in the initial mailing. All cover lettersto therapists were personally addressed and hand signed.
Results
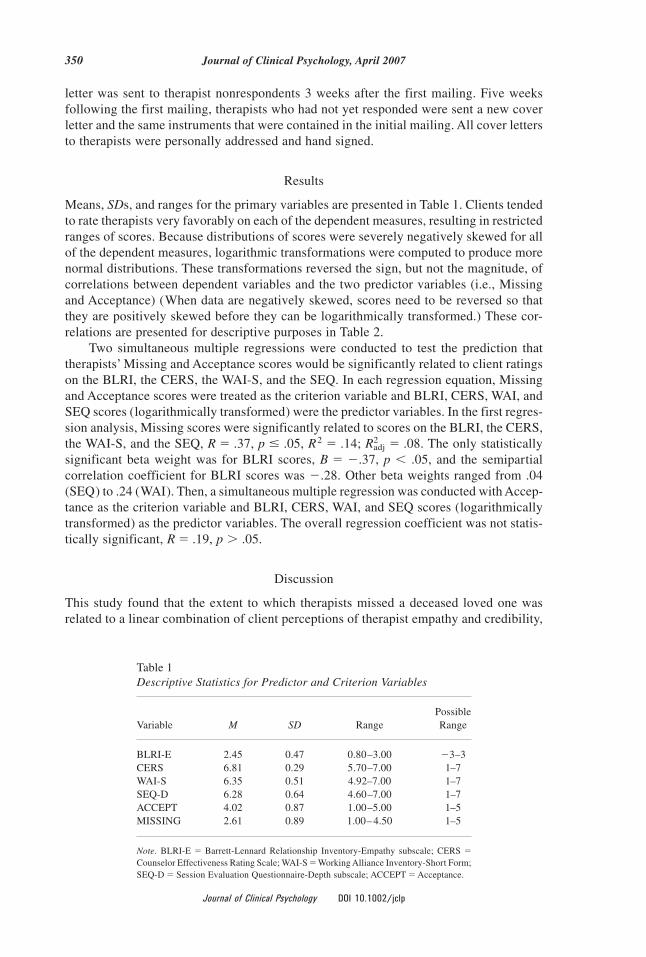
Means, SDs, and ranges for the primary variables are presented in Table 1. Clients tendedto rate therapists very favorably on each of the dependent measures, resulting in restrictedranges of scores. Because distributions of scores were severely negatively skewed for allof the dependent measures, logarithmic transformations were computed to produce morenormal distributions. These transformations reversed the sign, but not the magnitude, ofcorrelations between dependent variables and the two predictor variables (i.e., Missingand Acceptance) (When data are negatively skewed, scores need to be reversed so thatthey are positively skewed before they can be logarithmically transformed.) These cor-relations are presented for descriptive purposes in Table 2.
Two simultaneous multiple regressions were conducted to test the prediction thattherapists’ Missing and Acceptance scores would be significantly related to client ratingson the BLRI, the CERS, the WAI-S, and the SEQ. In each regression equation, Missingand Acceptance scores were treated as the criterion variable and BLRI, CERS, WAI, andSEQ scores (logarithmically transformed) were the predictor variables. In the first regres-sion analysis, Missing scores were significantly related to scores on the BLRI, the CERS,the WAI-S, and the SEQ, R � .37, p � .05, R2 � .14; Radj
2 � .08. The only statisticallysignificant beta weight was for BLRI scores, B � �.37, p � .05, and the semipartialcorrelation coefficient for BLRI scores was �.28. Other beta weights ranged from .04(SEQ) to .24 (WAI). Then, a simultaneous multiple regression was conducted with Accep-tance as the criterion variable and BLRI, CERS, WAI, and SEQ scores (logarithmicallytransformed) as the predictor variables. The overall regression coefficient was not statis-tically significant, R � .19, p � .05.
Discussion
This study found that the extent to which therapists missed a deceased loved one wasrelated to a linear combination of client perceptions of therapist empathy and credibility,
Table 1Descriptive Statistics for Predictor and Criterion Variables
Variable M SD RangePossibleRange
BLRI-E 2.45 0.47 0.80–3.00 �3–3CERS 6.81 0.29 5.70–7.00 1–7WAI-S 6.35 0.51 4.92–7.00 1–7SEQ-D 6.28 0.64 4.60–7.00 1–7ACCEPT 4.02 0.87 1.00–5.00 1–5MISSING 2.61 0.89 1.00– 4.50 1–5
Note. BLRI-E � Barrett-Lennard Relationship Inventory-Empathy subscale; CERS �Counselor Effectiveness Rating Scale; WAI-S � Working Alliance Inventory-Short Form;SEQ-D � Session Evaluation Questionnaire-Depth subscale; ACCEPT � Acceptance.
350 Journal of Clinical Psychology, April 2007
Journal of Clinical Psychology DOI 10.1002/jclp

the working alliance, and session depth. When these variables were examined individu-ally, empathy was the only variable that was associated with therapists’ missing theirdeceased loved ones. In particular, the more grief that therapists had about missing aloved one who had died, the less empathic clients perceived them to be. This finding fitswith previous research on countertransference that has demonstrated that therapists’unresolved conflicts can contribute negatively to the process of therapy (Ligiero & Gelso,2002; Rosenberger & Hayes, 2002). More specifically, the data from the present studysupport the notion that when therapists’ emotional energy is tied up in an unresolvedpersonal issue such as grief, clients may perceive therapists to be less available and lessunderstanding.
On the other hand, it also was true that the more that therapists had resolved theirgrief about missing a loved one who had died, the more empathic clients perceived themto be. This is consistent with the notion of the wounded healer. Wounded healers areindividuals, according to Jackson (2001),
whose personal experiences . . . have left lingering effects on them—in the form oflessons learned that later serve constructive purposes, in the form of attitudes and sensi-tivities that recurrently serve them in ministering to those whom they treat, or in the formof symptoms or characteristics that stay with them and usefully influence their therapeu-tic endeavors. (p. 2)In the realm of bereavement therapy, therapists can function as wounded healers in thatlosing a loved one and working through the emotional pain of missing that person canserve as a basis for enhanced empathy with clients who are also dealing with the death ofa loved one. In the words of the 14th-century Italian poet Petrarca, “No one’s solacepenetrates a saddened mind more than that of a fellow sufferer, and therefore the mosteffective words to strengthen the spirits of the bystanders are those which emerge fromthe actual torments” (as cited in Jackson, 2001, p. 8). That is, by reflecting upon one’sown experience, a therapist may better understand what a client is feeling, althoughtherapists must be tentative when doing so. One must be careful not to overgeneralizefrom personal experience and blur important distinctions between one’s own feelings andthose of the client. To intentionally draw from one’s suffering and use it in the service ofthe client requires the therapist’s awareness of and continual attention to his or her ownwounds (Hayes, 2004; Hayes & Gelso, 2001). In the words of Nouwen (1972),
A deep understanding of one’s own pain makes it possible to convert weakness into strengthand to offer one’s own experience as a source of healing to those who are often lost in thedarkness of their own misunderstood sufferings. (p. 87)
Table 2Correlations Among Predictor and Criterion Variables
CERS WAI-S SEQ-D ACCEPT MISSING
BLRI-E .51 .60 .29 .05 �.09CERS .65 .59 �.02 .22WAI-S .62 �.11 .20SEQ-D �.05 �.20ACCEPT .28
Note. BLRI-E � Barrett-Lennard Relationship Inventory-Empathy subscale; CERS �Counselor Effectiveness Rating Scale; WAI-S � Working Alliance Inventory-Short Form;SEQ-D � Session Evaluation Questionnaire-Depth subscale; ACCEPT � Acceptance.
Bereavement Therapy 351
Journal of Clinical Psychology DOI 10.1002/jclp
The concept of the wounded healer was expressed succinctly by Jung (1963) whenhe wrote that “Only the wounded physician heals” (p. 134). Jung elaborated on thisidea: “The patient’s treatment begins with the doctor, so to speak. Only if the doctorknows how to cope with himself and his own problems will he be able to teach thepatient to do the same” (p. 132). Jung’s statement raises the question of how therapistscan teach or otherwise help clients to cope with their grief. Most germane to the studyat hand is the issue of whether therapists should self-disclose personal experiences ofloss, and what the effects are of such disclosures. Although we did not observe thera-pists’ actual in-session behavior, a recent study suggests that the effects of therapists’countertransference disclosures can be quite positive, but only when the client per-ceives the working alliance to be strong (Myers & Hayes, 2006). In particular, when thealliance was perceived as strong, sessions were rated as deeper, and therapists wereperceived as more expert when therapists made countertransference disclosures thanwhen they made no disclosures; however, when the alliance was perceived as weak, theopposite effects were found.
Returning to the present study, we expected, but did not find, a relationship betweentherapists’ acceptance of the death of a loved one and client perceptions of the quality ofbereavement therapy. One reason why this relationship did not emerge may be that ther-apists were fairly resolved about accepting the death of someone close to them. AverageAcceptance scores were 4.02 on a scale of 1 to 5, indicating high resolution. Notably,average Missing scores were only 2.61 on the same scale of 1 to 5, suggesting lessresolution in this area. Still another possible reason clients’ perceptions of therapy werenot related to therapists’ Acceptance scores was because clients tended to perceive theirtherapists very positively, as evidenced by clients’ consistently high ratings on the BLRI,the WAI-S, the CERS, and the SEQ. The restricted range of scores on these instruments,combined with the ceiling effect for Acceptance scores, makes it difficult to detect sta-tistically significant relationships.
Why were client ratings on the dependent measures so positive? It could be, and onewould hope, that clients were receiving good therapy. Another explanation is that scoreswere a function of the mail-survey methods that were employed. Even though therapistswere instructed to give packets to the next client with whom they were working on griefissues, therapists may have given the measures to clients with whom they had betterrelationships. Alternatively, it may be that therapists followed the study’s instructions,and only those clients who had good relationships with their therapists completed theinstruments. In either case, the small variability in scores on the dependent measures,while clinically encouraging, was empirically limiting.
From a methodological perspective, it is clear that future studies in this area need togather data with less range restriction on the dependent measures. It also seems wise tocollect effectiveness data from therapists’ vantage points. In the present study, 128 ther-apists returned surveys, but data were provided by only 69 of their clients. Gathering datafrom all of the therapists would have yielded a larger sample size for some analyses,enhancing statistical power and thus increasing the probability of detecting potentialeffects. Furthermore, the fact that nearly two thirds of potential therapist participants didnot return surveys places limitations on the external validity of findings from the study.One potential reason for the low response rate may have been the relatively intrusivenature of the study. Several therapists wrote to us and indicated that they were not com-fortable asking their clients to participate in the study, and other therapists may have beenuncomfortable disclosing personal information about their grief. Finally, because Accep-tance and Missing scores resulted from a factor analysis of the TRIG that has yet to bereplicated with other samples, results should be interpreted with caution.
352 Journal of Clinical Psychology, April 2007
Journal of Clinical Psychology DOI 10.1002/jclp
In any event, data from the present study suggest that the extent to which thera-pists miss a deceased loved one is directly related to clients’ perceptions of therapists’empathy in bereavement therapy. This finding underscores the importance of thera-pists’ attending to and working to resolve personal issues that may affect their work withclients, especially when the client’s concerns mirror the therapist’s. A therapist’s unresolvedissues can interfere with critical therapeutic processes such as empathy whereas greaterresolution of such issues may serve to deepen the therapist’s empathic capacity.
References
Ahn, H., & Wampold, B. E. (2001). Where oh where are the specific ingredients? A meta-analysisof component studies in counseling and psychotherapy. Journal of Counseling Psychology, 48,251–257.
Atkinson, D. R., & Carskaddon, G. (1975). A prestigious introduction, psychological jargon, andperceived counselor credibility. Journal of Counseling Psychology, 22, 180–186.
Atkinson, D. R., & Wampold, B. E. (1982). A comparison of the Counselor Rating Form and theCounselor Effectiveness Rating Scale. Counselor Education and Supervision, 22, 25–36.
Barak, A., & LaCrosse, M. B. (1975). Multidimensional perception of counselor behavior. Journalof Counseling Psychology, 22, 471– 476.
Barrett-Lennard, G. T. (1962). Dimension of therapist responses as causal factors in therapeuticchange. Psychological Monographs, 76(43, Whole No. 562).
Barrett-Lennard, G. T. (1986). The Relationship Inventory now: Issues and advances in theory,method, and use. In L. Greenberg & W. Pinsoff (Eds.), The psychotherapeutic process: Aresearch handbook (pp. 439– 476). New York: Guilford Press.
Beutler, L., Machado, P. P., & Neufeldt, S. A. (1994). Therapist variables. In A. E. Bergin & S. L.Garfield (Eds.), Handbook of psychotherapy and behavior change (3rd ed., pp. 229–269).New York: Wiley.
Beutler, L. E., Malik, M., Alimohamed, S., Harwood, T. M., Talebi, H., Noble, S., & Wong, E.(2004). Therapist variables. In M. J. Lambert (Ed.), Bergin and Garfield’s handbook of psy-chotherapy and behavior change (5th ed., pp. 227–306). New York: Wiley.
Bordin, E. S. (1979). The generalizability of the psychoanalytic concept of the working alliance.Psychotherapy, 16, 252–260.
Boyer, S. P., & Hoffman, M. A. (1993). Counselor affective reactions to termination: Impact ofcounselor loss history and perceived client sensitivity to loss. Journal of Counseling Psychol-ogy, 40, 271–277.
Brown, L. S. (2001). Feelings in context: Countertransference and the real world in feminist ther-apy. Journal of Clinical Psychology/In Session, 57, 1005–1012.
Cutler, R. L. (1958). Countertransference effects in psychotherapy. Journal of Consulting Psychol-ogy, 22, 349–356.
Dunkle, J. H., & Friedlander, M. L. (1996). Contribution of counselor experience and personalcharacteristics to the working alliance. Journal of Counseling Psychology, 43, 456– 460.
Elkin, I., Falconnier, L., Martinovich, Z., & Mahoney, C. (2006). Therapist effects in the NationalInstitute of Mental Health Treatment of Depression Collaborative Research Program. Psycho-therapy Research, 16, 144–160.
Ellis, A. (2001). Rational and irrational aspects of countertransference. Journal of Clinical Psychology/In Session, 57, 999–1004.
Ellis, A. (2003). How to deal with your most difficult client—You. Journal of Rational-Emotiveand Cognitive-Behavior Therapy, 21, 203–213.
Faschingbauer, T. R., Zisook, S., & DeVaul, R. A. (1987). The Texas Revised Inventory of Grief. InS. Zisook (Ed.), Biopsychosocial aspects of bereavement (pp. 109–124). Washington, DC:American Psychiatric Press.
Bereavement Therapy 353
Journal of Clinical Psychology DOI 10.1002/jclp
Freud, S. (1959). Future prospects of psychoanalytic psychotherapy. In J. Strachey (Ed. & Trans.),The standard edition of the complete psychological works of Sigmund Freud (Vol. 11, pp. 139–151). London: Hogarth Press. (Original work published in 1910)
Hayes, J. A. (2004). The inner world of the psychotherapist: A program of research on counter-transference. Psychotherapy Research, 14, 21–36.
Hayes, J. A., & Gelso, C. J. (1991). Effects of therapist-trainees’ anxiety and empathy on counter-transference behavior. Journal of Clinical Psychology, 47, 284–290.
Hayes, J. A., & Gelso, C. J. (1993). Male counselors’ discomfort with gay and HIV-infected clients.Journal of Counseling Psychology, 40, 86–93.
Hayes, J. A., & Gelso, C. J. (2001). Clinical implications of research on countertransference: Sci-ence informing practice. Journal of Clinical Psychology/In Session, 57, 1041–1052.
Hayes, J. A., McCracken, J. E., McClanahan, M. K., Hill, C. E., Harp, J. S., & Carozzoni, P. (1998).Therapist perspectives on countertransference: Qualitative data in search of a theory. Journalof Counseling Psychology, 45, 468– 482.
Horvath, A. O., & Greenberg, L. (1989). Development and validation of the Working AllianceInventory. Journal of Counseling Psychology, 36, 223–232.
Jackson, S. W. (2001). Presidential Address: The wounded healer. Bulletin of the History of Med-icine, 75, 1–36.
Jung, C. G. (1963). Memories, dreams, reflections. New York: Vintage.
Latts, M. G., & Gelso, C. J. (1995). Countertransference behavior and management with survivorsof sexual assault. Psychotherapy, 32, 405– 415.
Lautenschlager, G. J. (1989). A comparison of alternatives to conducting Monte Carlo analyses fordetermining parallel analysis criteria. Multivariate Behavioral Research, 24, 365–395.
Li, L. C., & Kim, B. S. K. (2004). Effects of counseling style and client adherence to Asian culturalvalues on counseling process with Asian American college students. Journal of CounselingPsychology, 51, 158–167.
Ligiero, D. P., & Gelso, C. J. (2002). Countertransference, attachment, and the working alliance:The therapist’s contributions. Psychotherapy, 39, 3–11.
Martin, D. J., Garske, J. P., & Davis, M. K. (2000). Relation of the therapeutic alliance with out-come and other variables: A meta-analytic review. Journal of Consulting and Clinical Psychol-ogy, 68, 438– 450.
May, R. (1989). The art of counseling. New York: Gardner. (Original work published 1939)
McClure, B. A., & Hodge, R. W. (1987). Measuring countertransference and attitude in therapeuticrelationships. Psychotherapy, 24, 325–335.
Myers, D., & Hayes, J. A. (2006). Effects of therapist general self-disclosure and countertransfer-ence disclosure on ratings of the therapist and session. Psychotherapy, 43, 173–185.
Normandin, L., & Bouchard, M. A. (1993). The effects of theoretical orientation and experience onrational, reactive, and reflective countertransference. Psychotherapy Research, 3, 77–94.
Nouwen, H. (1972). The wounded healer. Garden City, NY: Image.
Peabody, S. A., & Gelso, C. J. (1982). Countertransference and empathy: The complex relationshipbetween two divergent concepts in counseling. Journal of Counseling Psychology, 29, 240–245.
Rogers, C. (2000). Interview with Carl Rogers on the use of self in therapy. In M. Baldwin (Ed.),The use of self in therapy (pp. 29–38). Binghamton, NY: Haworth.
Rosenberger, E. W., & Hayes, J. A. (2002). Origins, consequences, and management of counter-transference: A case study. Journal of Counseling Psychology, 49, 221–232.
Sharkin, B., & Gelso, C. J. (1993). The influence of counselor-trainee anger proneness on reactionsto an angry client. Journal of Counseling and Development, 71, 483– 487.
Stiles, W. B., Shapiro, D. A., & Firth-Cozens, J. A. (1988). Do sessions of different treatments havedifferent impacts? Journal of Counseling Psychology, 35, 391–396.
354 Journal of Clinical Psychology, April 2007
Journal of Clinical Psychology DOI 10.1002/jclp

Stiles, W. B., & Snow, J. S. (1984). Counseling session impact as viewed by novice counselors andtheir clients. Journal of Counseling Psychology, 31, 3–12.
Tracey, T. J., & Kokotovic, A. M. (1989). Factor structure of the Working Alliance Inventory.Psychological Assessment, 1, 207–210.
Zwick, W. R., & Velicer, W. F. (1986). Comparison of five rules for determining the number ofcomponents to retain. Psychological Bulletin, 99, 432– 442.
Bereavement Therapy 355
Journal of Clinical Psychology DOI 10.1002/jclp