gestational hypertension
TRANSCRIPT
HYPERTENSION Gestational Hypertension
Mohammad Ilyas, M.D.
Assistant Clinical Professor
University of Florida / Health Sciences Center
Jacksonville, Florida USA
Outline
1. Definition, Regulation and Pathophysiology
2. Measurement of Blood Pressure, Staging of Hypertension and Ambulatory
Blood Pressure Monitoring
3. Evaluation of Primary Versus Secondary
4. Sequel of Hypertension and Hypertension Emergencies
5. Management of Hypertension (Non-Pharmacology versus Drug Therapy)
6. The Relation Between Hypertension: Obesity, Drugs, Stress and Sleep
Disorders.
7. Hypertension in Renal diseases and Pregnancies
8. Pediatric, Neonatal and Genetic Hypertension
Hypertension in Pregnancy
• Most common medical problem encountered during pregnancy
• 8% of pregnancies
• Third leading cause of maternal mortality, after
thromboembolism and non-obstetric injuries
• Maternal DBP > 110 is associated with ↑ risk of placental
abruption and fetal growth restriction
• Superimposed preeclampsia cause most of the
morbidity
Hypertension in Pregnancy
• 4 categories
1. Chronic Hypertension
2. Pregnancy Induced hypertension
3. Preeclampsia-eclampsia
4. Preeclampsia superimposed on chronic HTN
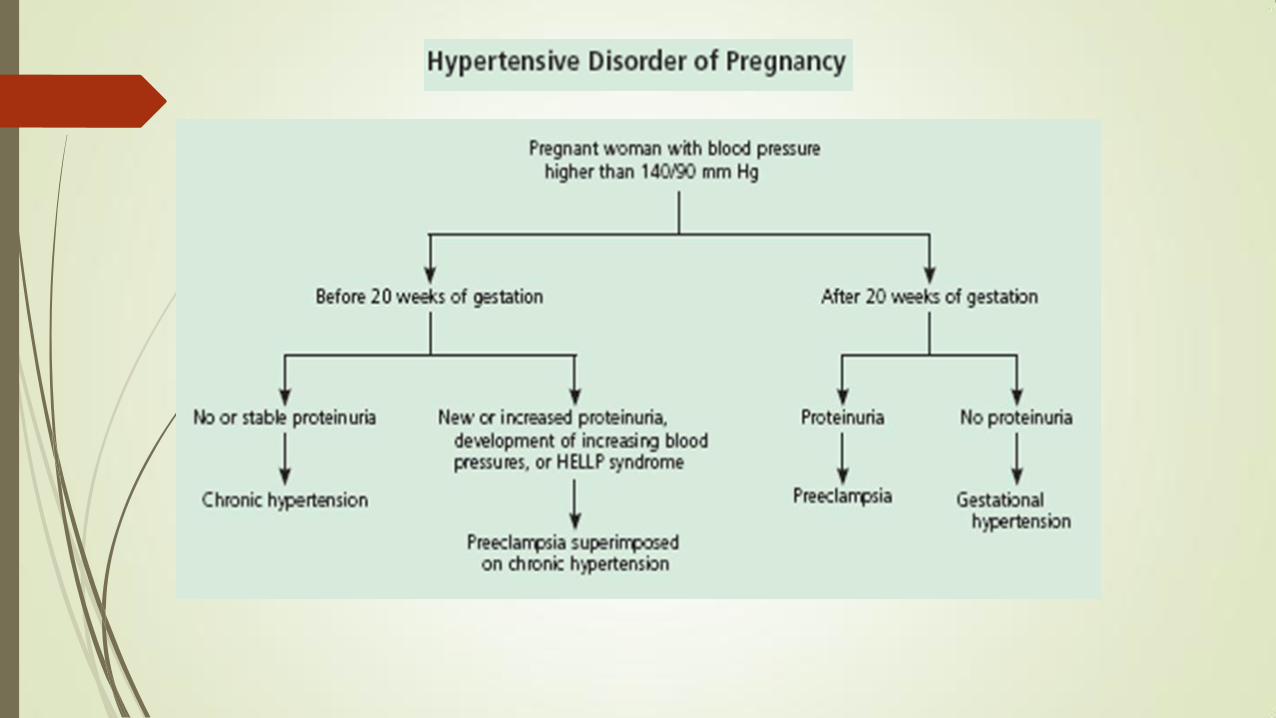
DEFINITION
Chronic hypertension, if blood pressure
elevation >140/90 before 20 weeks and persists
≥12 weeks postpartum
Gestational hypertension of pregnancy, if blood
pressure returns to normal by 12 weeks
postpartum
Chronic Hypertension
Treatment of mild to moderate chronic hypertension neither benefits the fetus nor prevents preeclampsia.
Excessively lowering blood pressure may result in decreased placental perfusion and adverse perinatal outcomes.
When BP is 150 to 180/100 to 110 mm Hg, pharmacologic treatment is needed to prevent maternal end-organ damage.
Treatment of Chronic Hypertension
Methyldopa , labetalol, and nifedipine most common
oral agents.
AVOID: ACEI and ARBs, atenolol, thiazide diuretics
Women in active labor with uncontrolled severe chronic
hypertension require treatment with intravenous
labetalol or hydralazine.
Pregnancy Induced Hypertension
(Gestational)
• Usually mild and later in pregnancy
• BP ≥140/90 mmHg (severe when ≥160/≥110 mmHg)
• Previously normotensive
• ≥20 weeks of gestation
• No renal or other systemic involvement
• No proteinuria or new signs of end-organ dysfunction
• Resolves 12 weeks postpartum
• May become preeclampsia
Gestational Hypertension to Preeclampsia
The pathophysiology of gestational hypertension is unknown.
Different diseases with a similar phenotype (hypertension)
Primiparity is a strong risk factor for preeclampsia, but not for GH
The recurrence risk for gestational hypertension is ~40% (for PE 5%)
Total blood and plasma volumes are significantly lower in women
with preeclampsia (mean 2660 mL/m2 and 1790 mL/m2,
respectively) than in women with gestational hypertension (3139
mL/m2 and 2132 mL/m2, respectively)
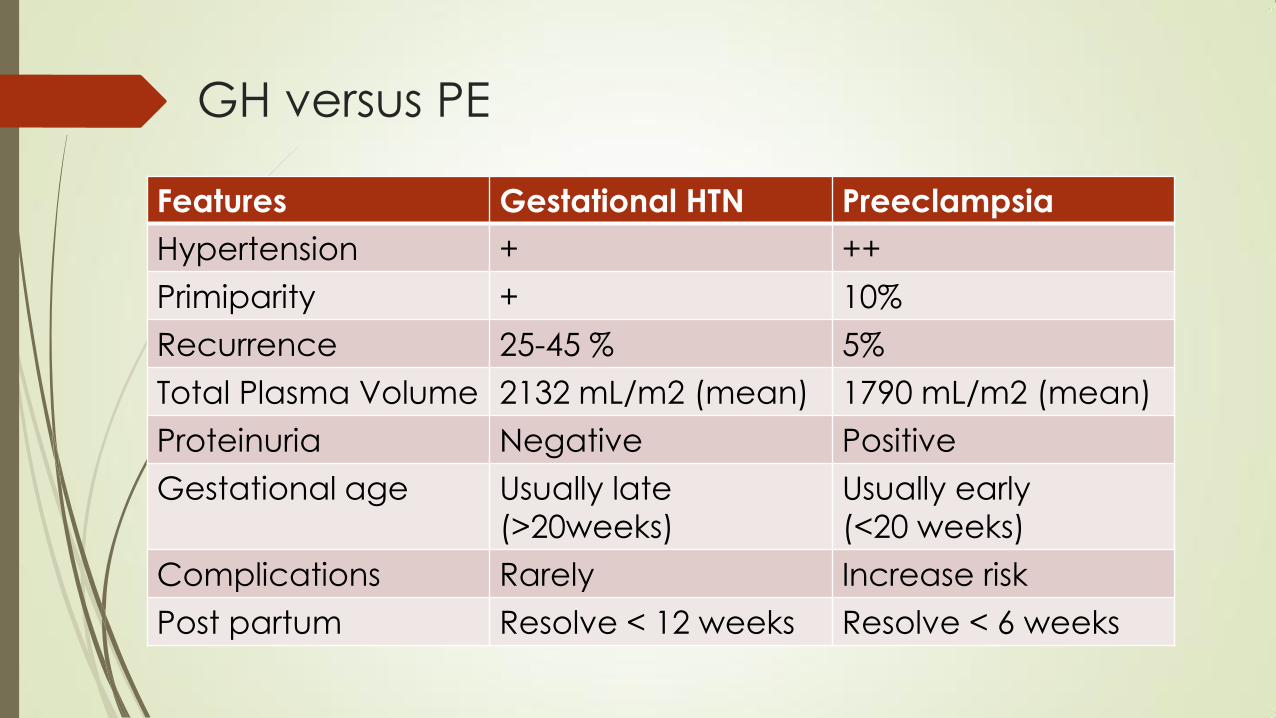
GH versus PE
Features Gestational HTN Preeclampsia
Hypertension + ++
Primiparity + 10%
Recurrence 25-45 % 5%
Total Plasma Volume 2132 mL/m2 (mean) 1790 mL/m2 (mean)
Proteinuria Negative Positive
Gestational age Usually late
(>20weeks)
Usually early
(<20 weeks)
Complications Rarely Increase risk
Post partum Resolve < 12 weeks Resolve < 6 weeks
RISK OF PROGRESSION TO PREECLAMPSIA
Preeclampsia develops in 15 to 25 % of women with initial GH,
Early onset of GH are more likely to progress to preeclampsia
(33 versus 37 weeks)
40 to 50 % of women with GH presenting at ≤30 weeks
developed preeclampsia as compared with about 10 % of
those who developed gestational hypertension at ≥36 weeks
Women who go on to develop preeclampsia have higher total
vascular resistance at presentation than women with
uncomplicated GH
PERINATAL OUTCOME
Pregnancy outcomes of patients with non-severe gestational
hypertension are generally favorable.
The mean birth weight and rates of fetal growth restriction,
preterm birth, abruption, and perinatal death are similar to those
in the general obstetrical population.
Severe gestational hypertension appear to be at increased risk of
maternal and perinatal morbidity
These pregnancies have significantly higher rates of preterm
delivery, small for gestational age infants, and abruptio placentae
MANAGEMENT
Non-severe gestational hypertension, monitoring blood
pressure once or twice weekly and weekly assessment of
proteinuria, platelet count, and liver enzymes
Patient education and counseling
Fetal assessment, monitor fetal movement daily
No antihypertensive therapy — unless hypertension is
severe (≥160 mmHg systolic or ≥110 mmHg diastolic)
No antenatal glucocorticoids
Timing of delivery at 370/7ths to 386/7ths weeks
Intrapartum management
administer magnesium sulfate for seizure prophylaxis
Preeclampsia • New onset HTN
• After 20 weeks of gestation, or
• Early post-partum, previously normotensive
• Resolves within 48 hrs postpartum
• With the following (Renal or other systemic)
• Proteinuria > 300 mg/24hr
• Oliguria or Serum-plasma creatinine ratio > 0.09 mmol/L
• Headaches with hyperreflexia, eclampsia, clonus or visual disturbances
• ↑ LFTs, glutathione-S-Transferase alpha 1-1, alanine aminotransferase or
right abdominal pain
• Thrombocytopenia, ↑ LDH, hemolysis, DIC
• 10% in primigravid
• 20-25% with history of chronic HTN
Diagnostic Criteria for Preeclampsia
1. SBP of 140 mm Hg or more or a DBP of 90 mm Hg or more on two occasions at least six hours apart after 20 weeks of gestation AND
2. Proteinuria – 300 mg in a 24-hour urine specimen or 1+ or greater on urine dipstick testing of two random urine samples collected at least four hours apart.
A random urine protein/creatinine ratio < 0.21 indicates that significant proteinuria is unlikely with a NPV of 83%.
Generalized edema (affecting the face and hands) is often present in patients with preeclampsia but is not a diagnostic criterion.
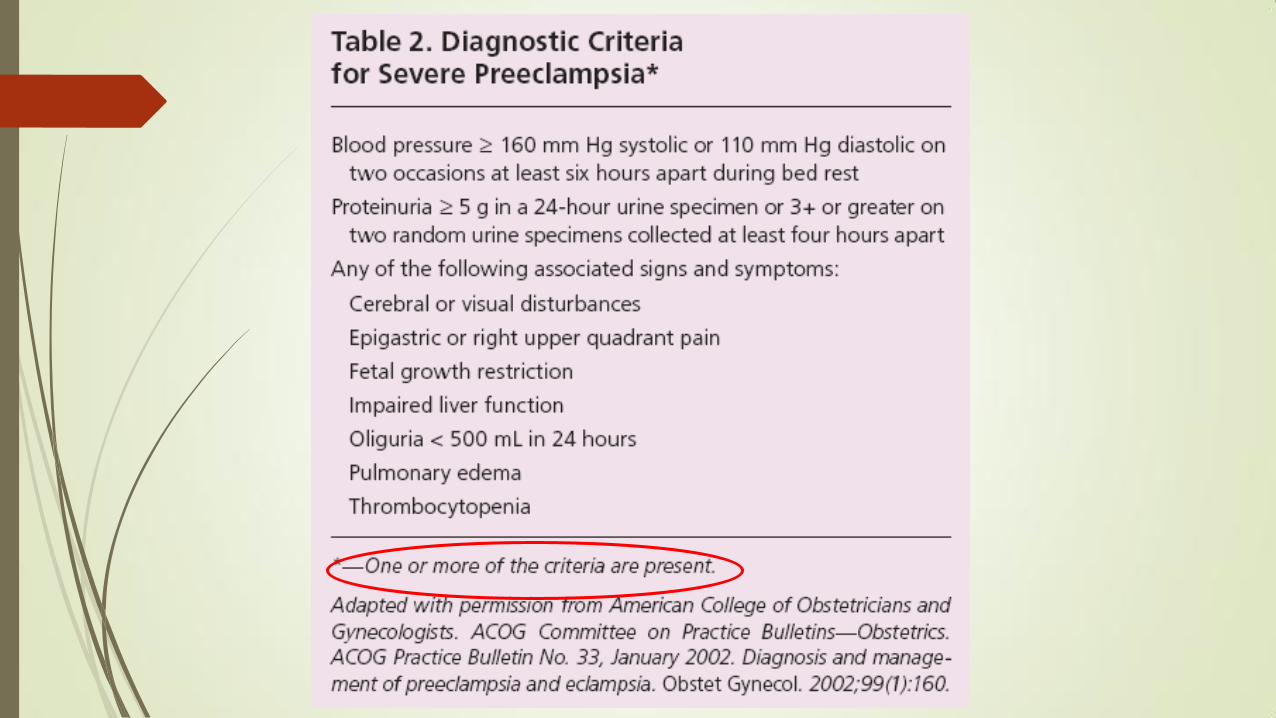
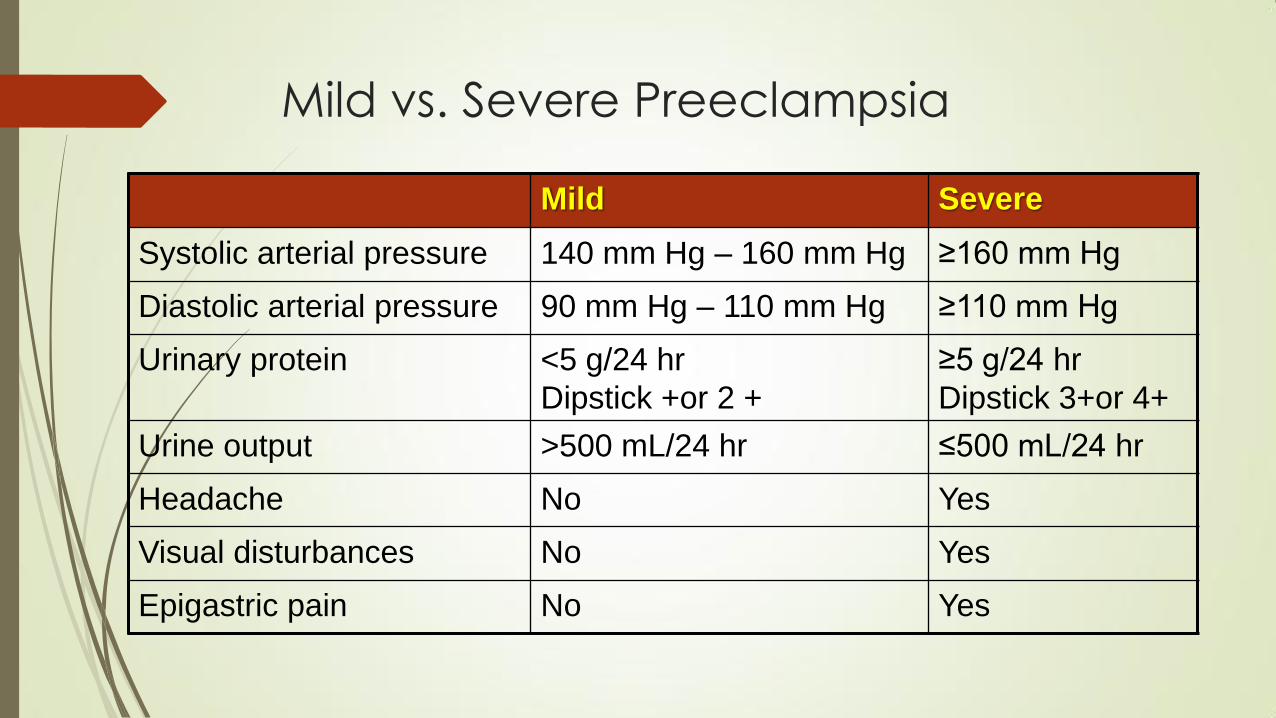
Mild vs. Severe Preeclampsia
Mild Severe
Systolic arterial pressure 140 mm Hg – 160 mm Hg ≥160 mm Hg
Diastolic arterial pressure 90 mm Hg – 110 mm Hg ≥110 mm Hg
Urinary protein <5 g/24 hr
Dipstick +or 2 +
≥5 g/24 hr
Dipstick 3+or 4+
Urine output >500 mL/24 hr ≤500 mL/24 hr
Headache No Yes
Visual disturbances No Yes
Epigastric pain No Yes
Maternal Risk Factors
• First pregnancy
• Age younger than 18 or older than 35
• Prior h/o preeclampsia
• Black race
• Medical risk factors for preeclampsia - chronic HTN,
renal disease, diabetes, anti-phospholipid syndrome
• Twins
• Family history
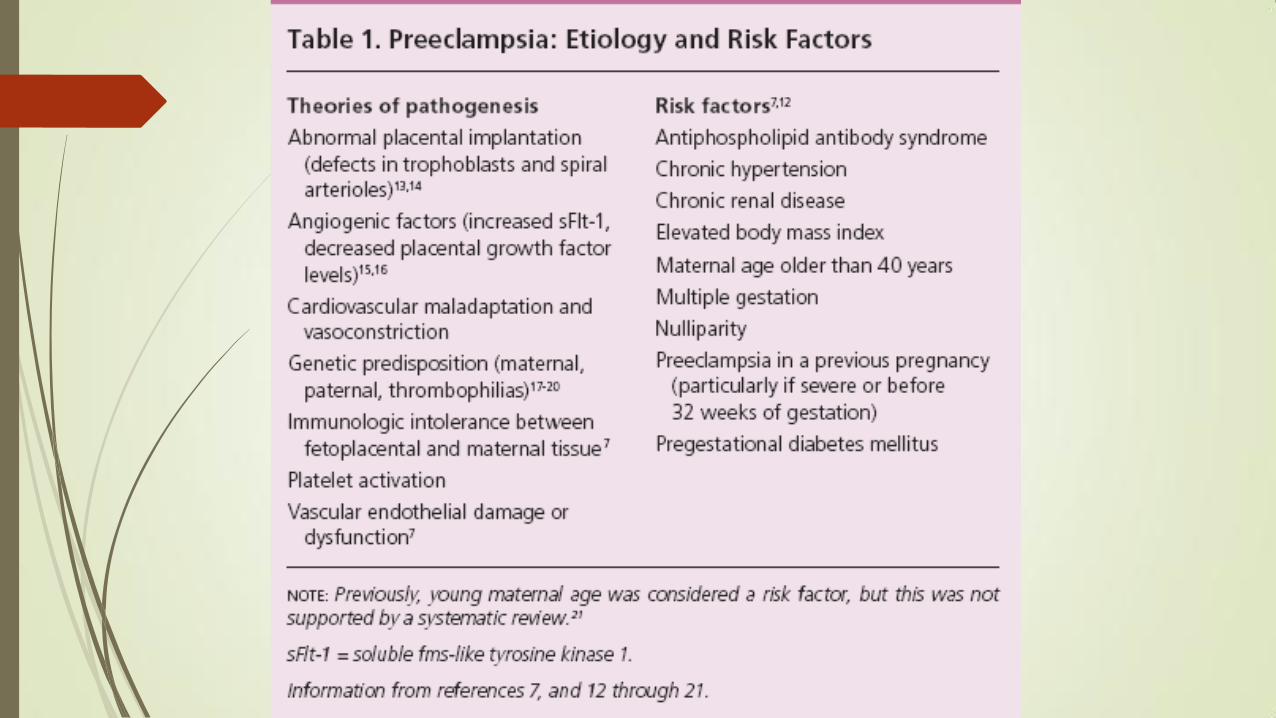
Etiology
Exact mechanism not known
• Immunologic
• Genetic
• Placental ischemia
• Endothelial cell dysfunction
• Vasospasm
• Hyper-responsive response to vasoactive hormones (e.g.
angiotensin II & epinephrine)
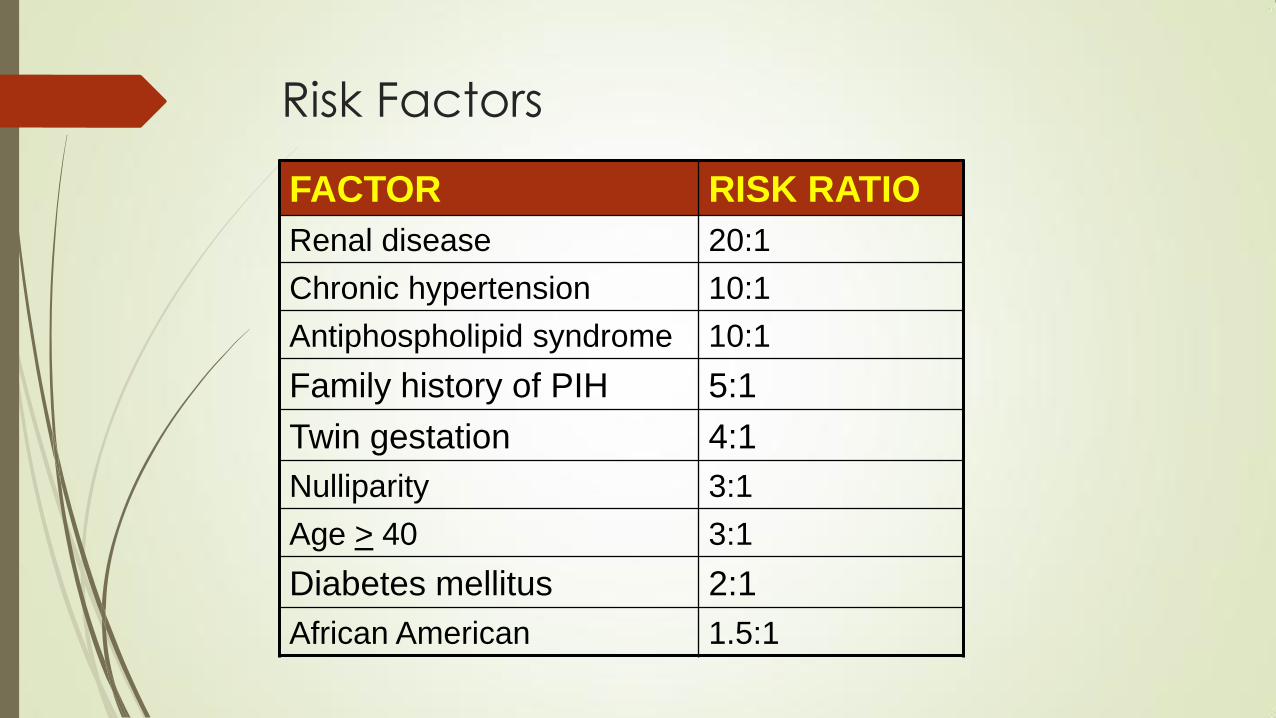
Risk Factors
FACTOR RISK RATIO
Renal disease 20:1
Chronic hypertension 10:1
Antiphospholipid syndrome 10:1
Family history of PIH 5:1
Twin gestation 4:1
Nulliparity 3:1
Age > 40 3:1
Diabetes mellitus 2:1
African American 1.5:1
Symptoms of preeclampsia
• Visual disturbances
• Headache
• Epigastric pain
• Rapidly increasing or nondependent edema - may
be a signal of developing preeclampsia
• Rapid weight gain - result of edema due to
capillary leak as well as renal Na and fluid retention
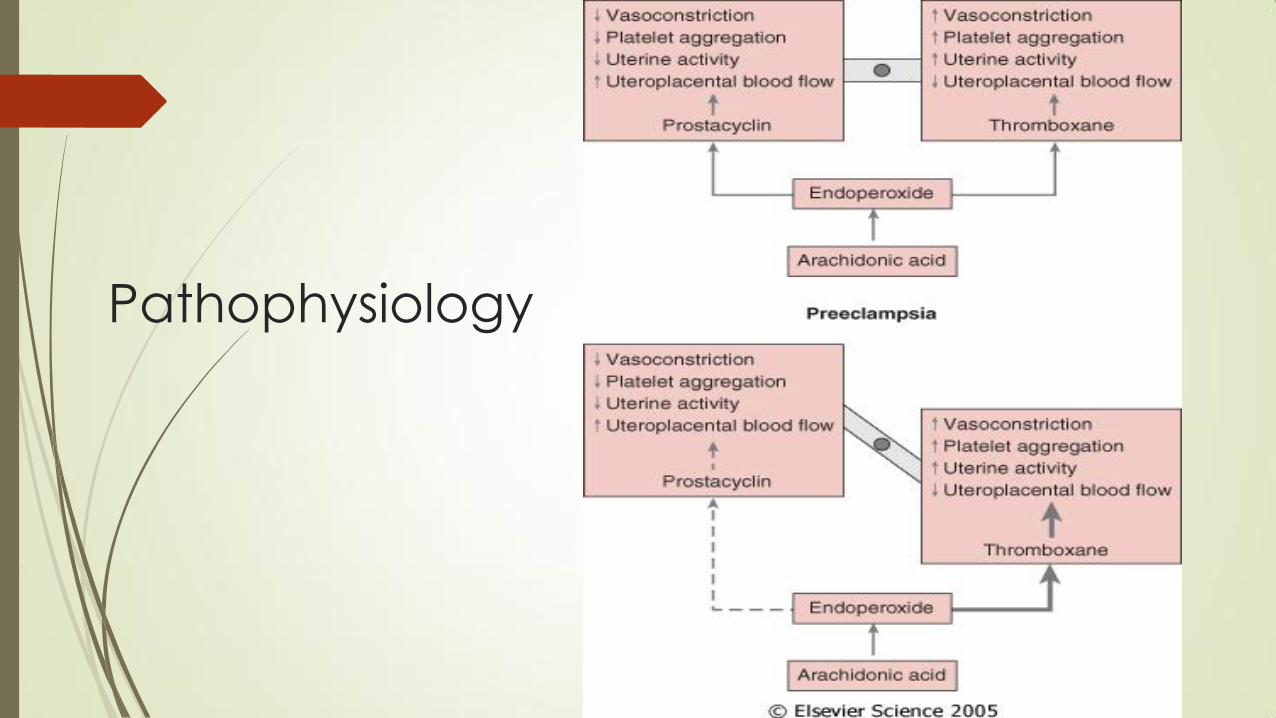
Pathophysiology
Organ involvement
• Airway edema
• Cardiac
• Renal
• Hepatic
• Uterine
Upper airway edema
• Upper airway edema
• Laryngeal edema
• Airway obstruction
• Potential for airway compromise or difficulty in intubation
Cardiac/Pulmonary
• Increased CO & SVR
• CVP normal or slightly increased
• Plasma volume reduced
• Pulmonary edema
• Decrease oncotic/colloid pressure
• Capillary/endothelial damage leak
• Vasoconstriction
• increase PWP and CVP
• Occurs 3 % of preeclamptic patients

Hepatic
• Usually mild
• Severe PIH or preeclampsia complicated by HELLP
periportal hemorrhages
ischemic lesion
generalized swelling
hepatic swelling
epigastric pain
Renal
• Adversely affected proteinuria
• GFR and CrCl decrease
• BUN increase, may correlate w/ severity
• RBF compromised
• ARF w/ oliguria – PIH, esp. w/ abruption, DIC, HELLP
*Oliguria + renal failure may occur in the absence of hypovolemia. Be careful w/ hydration pulmonary edema*
Uterine
• Activity increased
• Hyperactive/hypersensitive to oxytocin
• Preterm labor – frequent
• Uterine/placental blood flow – decreased by 50-70%
• Abruption – incidence increased
Morbidity / Mortality
Maternal complications:
• Leading cause of maternal death in PIH is intracranial hemorrhage
• Seizures
• Pulmonary edema
• ARF
• Proteinuria
• Hepatic swelling with or without liver dysfunction
• DIC (usually associated with placental abruption and is uncommon
as a primary manifestation of preeclampsia)
Morbidity / Mortality
Fetal complications:
• Abruptio placentae
• IUGR
• Premature delivery
• Intrauterine fetal death
HELLP Syndrome
• Hemolysis
• Elevated Liver enzymes
• Low Platelets
• < 36 wks
• Malaise (90%), epigastric pain (90%), N/V (50%)
• Self-limiting
• Multi-system failure
Diagnosis Criteria for HELLP
HTN SPB is ≥160 mmHg or DPB is ≥110 mmHg
Proteinuria ≥0.3 grams in a 24-hour urine specimen or
protein (mg/dL)/creatinine (mg/dL) ratio ≥0.3
Platelet count <100,000/microliter
Serum creatinine >1.1 mg/dL or doubling of serum
creatinine in the absence of other renal disease
Liver transaminases at least twice the normal
concentrations
Pulmonary edema
Cerebral or visual symptoms
HELLP Syndrome
• Hemostasis is not problematic unless PLT < 40,000
• Rate of fall in PLT count is important
• Regional anesthesia - contraindicated fall is sudden
• PLT count normal within 72 hrs of delivery
• Thrombocytopenia may persist for longer periods.
• Definitive cure is delivery
Treatment
• Management of maternal hemodynamics & prevention
of eclampsia are key to a favorable outcome
• MgSO4 - Rx of choice for preeclampsia.
• Does not significantly reduce systemic BP at the serum concentration that are efficacious in treating preeclampsia
• Goals
• Control BP
• Prevent seizures
• Deliver the fetus
Controlling the HTN
• Hydralazine
• Labetalol
• Nitroglycerin
• Nifedipine
• Esmolol
• Na Nitroprusside – risk of cyanide toxicity in the fetus
Preventing Seizures
• MgSO4 - Drug of choice. Narrow therapeutic index
• Reduce > 50% w/o any serious maternal morbidity
• 4g IV Bolus over 10 minutes, then infusion @ 1g/hr
• Renal failure - rate of infusion by serum Mg levels
• Plasma Level should be between 4-6 mmol/L
• Monitor clinical signs for toxicity
• Toxic: 10 ml of 10% Ca Gluconate IV slowly
MgSO4 Toxicity
• 5-10 mEq/L – Prolonged PR, widened QRS
• 11-14 mEq/L – Depressed tendon reflexes
• 15-24 mEq/L – SA, AV node block, respiratory paralysis
• >25 mEq/L - Cardiac arrest
Quiz
Quiz 1. Which of the following is NOT true
about Hypertension in Pregnancy ?
A. HTN is the Most common medical problem encountered during pregnancy
B. Majority of the of pregnancies complicate with HTN.
C. Third leading cause of maternal mortality, after
thromboembolism and non-obstetric injuries
D. Maternal DBP > 110 is associated with ↑ risk of placental
abruption and fetal growth restriction
E. Superimposed preeclampsia cause most of the morbidity
Quiz 1. Which of the following is NOT true
about Hypertension in Pregnancy ?
A. HTN is the Most common medical problem encountered during pregnancy
B. Majority of the of pregnancies complicate with HTN.
C. Third leading cause of maternal mortality, after
thromboembolism and non-obstetric injuries
D. Maternal DBP > 110 is associated with ↑ risk of placental
abruption and fetal growth restriction
E. Superimposed preeclampsia cause most of the morbidity
Quiz 2. Which of the following is the
RISK for progression to preeclampsia?
A. Gestational diabetes
B. Gestational hypertension
C. Late onset of GH are more likely to progress to
preeclampsia
D. Low total vascular resistance
Quiz 2. Which of the following is the
RISK for progression to preeclampsia?
A. Gestational diabetes
B. Gestational hypertension
C. Late onset of GH are more likely to progress to
preeclampsia
D. Low total vascular resistance
Quiz 3. Hypertension in Pregnancy can be
categorized in the following categories
EXCEPT?
A. Chronic Hypertension
B. Malignant hypertension
C. Pregnancy Induced hypertension
D. Preeclampsia-eclampsia
E. Preeclampsia superimposed on chronic HTN
Quiz 3. Hypertension in Pregnancy can be
categorized in the following categories
EXCEPT?
A. Chronic Hypertension
B. Malignant hypertension
C. Pregnancy Induced hypertension
D. Preeclampsia-eclampsia
E. Preeclampsia superimposed on chronic HTN
Quiz 4. Which of the following statement about
Gestational Hypertension is TRUE?
A. The pathophysiology of gestational hypertension is known.
B. GH and PE are same diseases with a different phenotype
(hypertension)
C. Primiparity is a weak risk factor for preeclampsia, but not
for GH
D. The recurrence risk for gestational hypertension is ~40%
(for PE 5%)
E. Total blood and plasma volumes are significantly higher in
preeclampsia than in women with gestational
hypertension
Quiz 4. Which of the following statement about
Gestational Hypertension is TRUE?
A. The pathophysiology of gestational hypertension is known.
B. GH and PE are same diseases with a different phenotype
(hypertension)
C. Primiparity is a weak risk factor for preeclampsia, but not
for GH
D. The recurrence risk for gestational hypertension is ~40%
(for PE 5%)
E. Total blood and plasma volumes are significantly higher in
preeclampsia than in women with gestational
hypertension
Quiz 5. All of the following are required for
management of GH, EXCEPT?
A. Monitoring blood pressure once or twice weekly
B. Weekly assessment of proteinuria, platelet count, and
liver enzymes
C. Patient education and counseling
D. No antihypertensive therapy — unless hypertension is
severe (≥160 mmHg systolic or ≥110 mmHg diastolic)
E. Antenatal glucocorticoids
Quiz 5. All of the following are required for
management of GH, EXCEPT?
A. Monitoring blood pressure once or twice weekly
B. Weekly assessment of proteinuria, platelet count, and
liver enzymes
C. Patient education and counseling
D. No antihypertensive therapy — unless hypertension is
severe (≥160 mmHg systolic or ≥110 mmHg diastolic)
E. Antenatal glucocorticoids