gayle a. brazeau, ph.d. pain upon injection: … anatomy and physiology for pharmaceutical...
TRANSCRIPT

Gayle A. Brazeau, Ph.D.
Pain Upon Injection: Fundamentals of
Subcutaneous Anatomy and Physiology for
Pharmaceutical Scientists
Tuesday May 17, 2016 7:00 am
Three Key Considerations:
• Anatomy/Physiology Subcutaneous Tissues and
Adjacent Tissues
• Mechanisms Pain and Pain Pathways
• Optimizing Vehicles and Excipients for Parenteral
Formulations for Subcutaneous Injections.
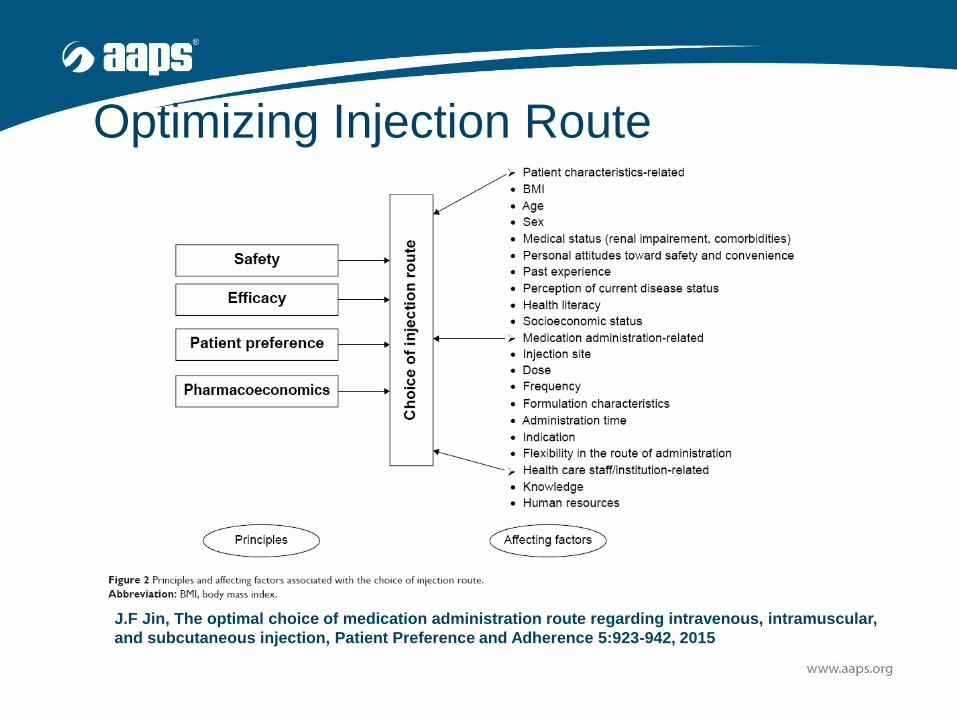
Optimizing Injection Route
J.F Jin, The optimal choice of medication administration route regarding intravenous, intramuscular,
and subcutaneous injection, Patient Preference and Adherence 5:923-942, 2015

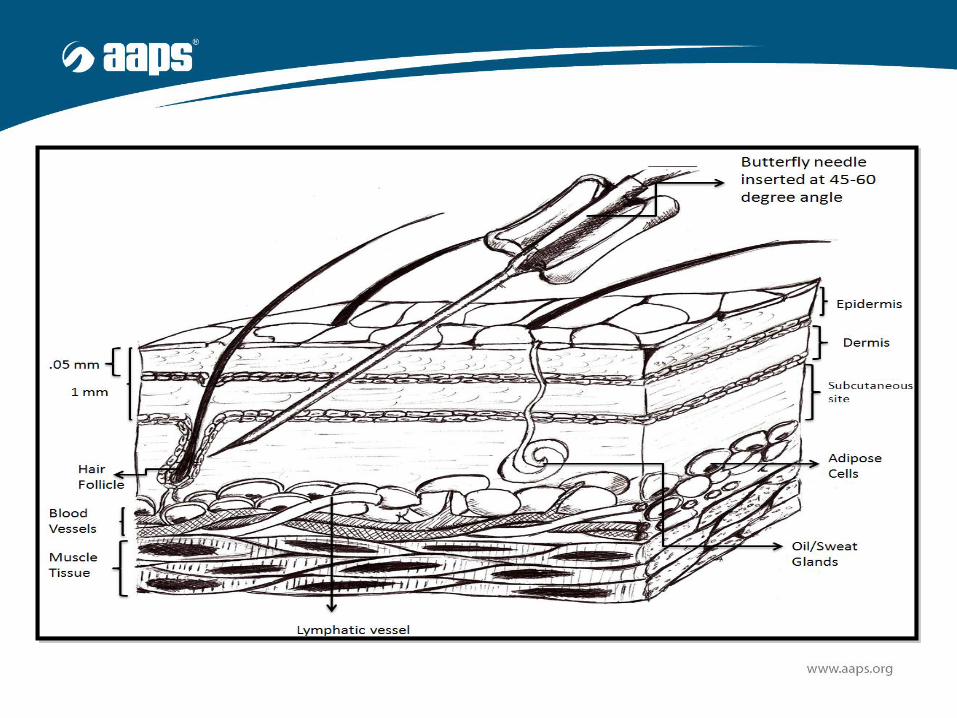
Subcutaneous Tissue
https://en.wikipedia.org/wiki/Subcutaneous_tissue#/me
dia/File:Skin.png
• Space beneath the
epidermis/dermis and
skeletal muscle
• Also called hypodermis
• Lowermost layer of the
integumentary system
• Composed of fibroblasts,
adipose cells and
microphages
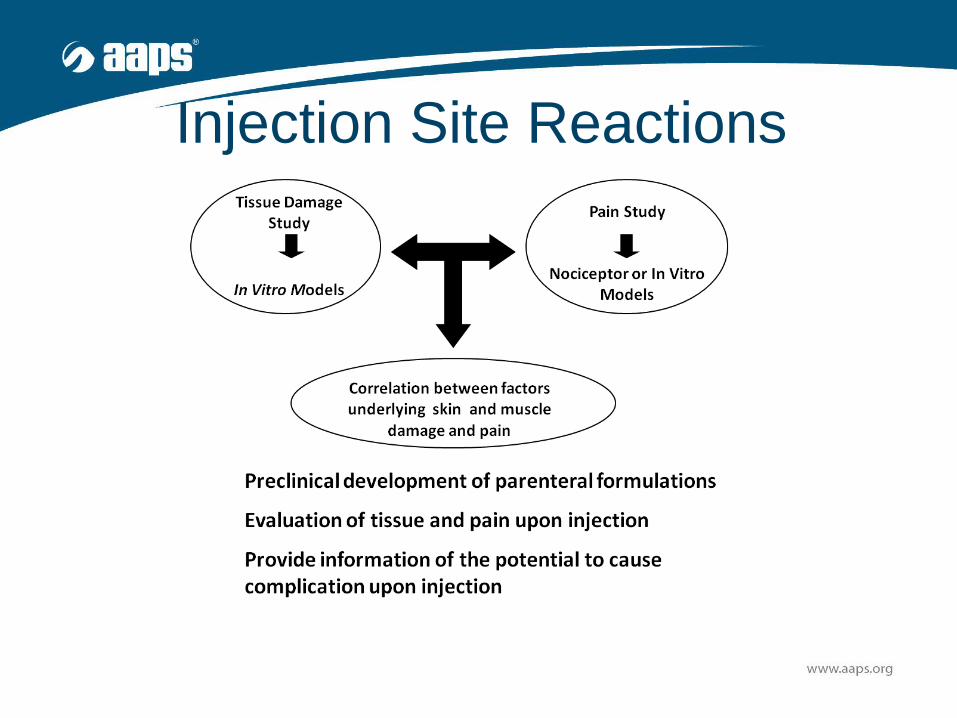
Injection Site Reactions
Key Questions
• What is the physiology associated
with pain upon injection?
• What are the mechanisms
associated with tissue damage?
• What is the role of inflammation and
swelling/edema?
Pain and Injections
http://classroomclipart.com/clipart-view/Clipart/Medical/nurse-giving-patient-injection_jpg.htm
Oh No,
Not Again!

Nociceptors – General Overview
• Sensory Receptors – free (bare) nerve endings
that detect signals from damaged tissue and
indirectly respond to chemicals released from
damaged tissue and or inflammation
• C-Fiber Classes and A Fiber Classes
• Categories
– Mechanical
– Thermal
– Chemical stimulation
http://neuroscience.uth.tmc.edu/s2/chapter06.htm
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2964977/
Nociceptor - Types
• Mechanonociceptors – respond to pinching,
cutting or stretching
• Thermal nociceptors – respond to the above
stimuli and thermal stimuli
• Chemical nociceptors - respond only to
chemical substances
• Polymodal nociceptors - respond to high
intensity stimuli such as mechanical, thermal
and to chemical substances
http://neuroscience.uth.tmc.edu/s2/chapter06.htm
Tissue Damage and Injections
Factors Affecting Tissue Damage
• Lipophilicity vehicle/drug
• Concentration
• Osmolarity
• pH (SC Avoid below 3 and above 9)
• Particle Size
• Solubility and Precipitation
• Biochemical Mechanisms
* Wu et al., JPP 62: 873, 2010
Biochemical Mechanisms:
Tissue Site Reactions
• Disruption sarcolemma membrane
• Alteration in cellular homeostasis
–Calcium release and transport
–Cellular energetics
• Free Radical Damage
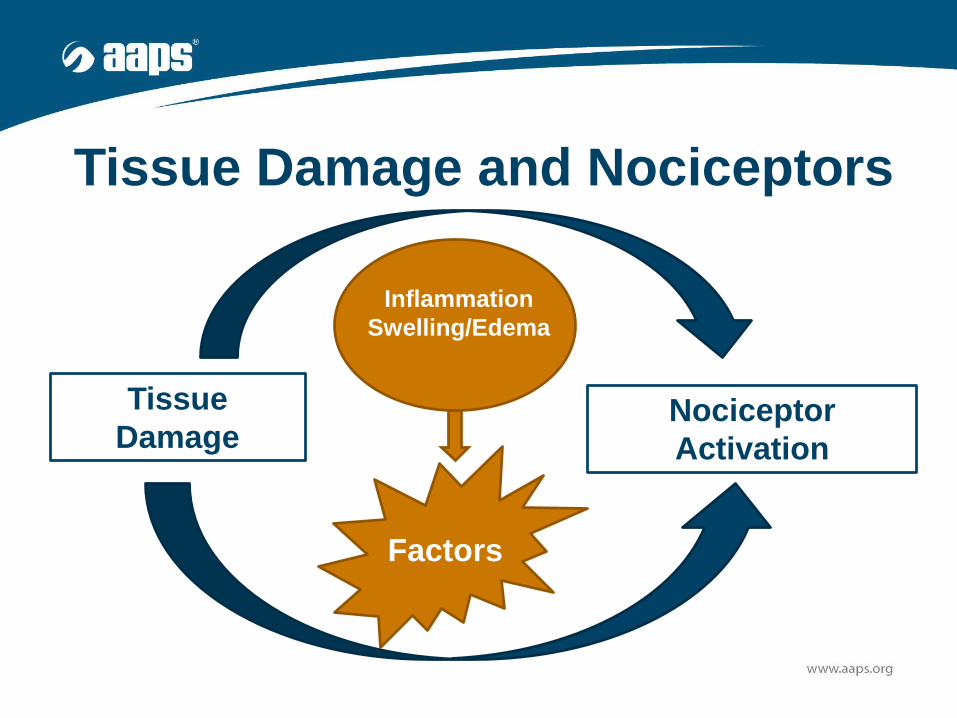
Tissue Damage and Nociceptors
Tissue
DamageNociceptor
Activation
Factors
Inflammation
Swelling/Edema

Tissue Damage - Factors Activating Nociceptors• Globulin and protein kinases
• Arachidonic acid
• Histamine
• Nerve growth factor (NGF)
• Substance P (SP) and calcitonin gene-related peptide
(CGRP)
• Potassium - K+
• Serotonin (5-HT)
• Acetylcholine (ACh)
• Low pH (acidic) solution
• ATP
• Lactic acidhttp://neuroscience.uth.tmc.edu/s2/chapter06.htm

Formulation Considerations: Tissue
Damage and Pain
W. Wang, Tolerability of hypertonic injectables, International Journal of
Pharmaceutics 490 (2015) 308–315
Important Considerations• Avoid drugs or formulations which are irritating
at the injection site
– Essential to initially screen for irritation
• Cell culture, isolated tissues (muscle, skin)
• Avoid drugs which may case vasoconstriction
• Avoid viscous suspensions
All can lead to induration, sloughing, abscess
formation or even necrosis
General Considerations SQ
• Sites
– Upper Arm
– Anterior Thigh Surface
– Lower Portion of Abdomen
– Upper Back
• Injection Volume 2-5 ml
• Needles 3/8 – 1 inch, 24-27 Gauge

Drug Release Factors
• Function of drug solubility
• Type of formulation – solution
versus suspension
• Formulation viscosity
• Particle size
• Changes in blood flow (minor)
Formulation Factors - Tolerability
• Specific Agent/Concentration
• Formulation Excipients and pH
• Formulation Tonicity
• Formulation Osmolarity
• Injection Speed
• Injection Volume
• Injection Site
• Particle Size
• Injection Frequency
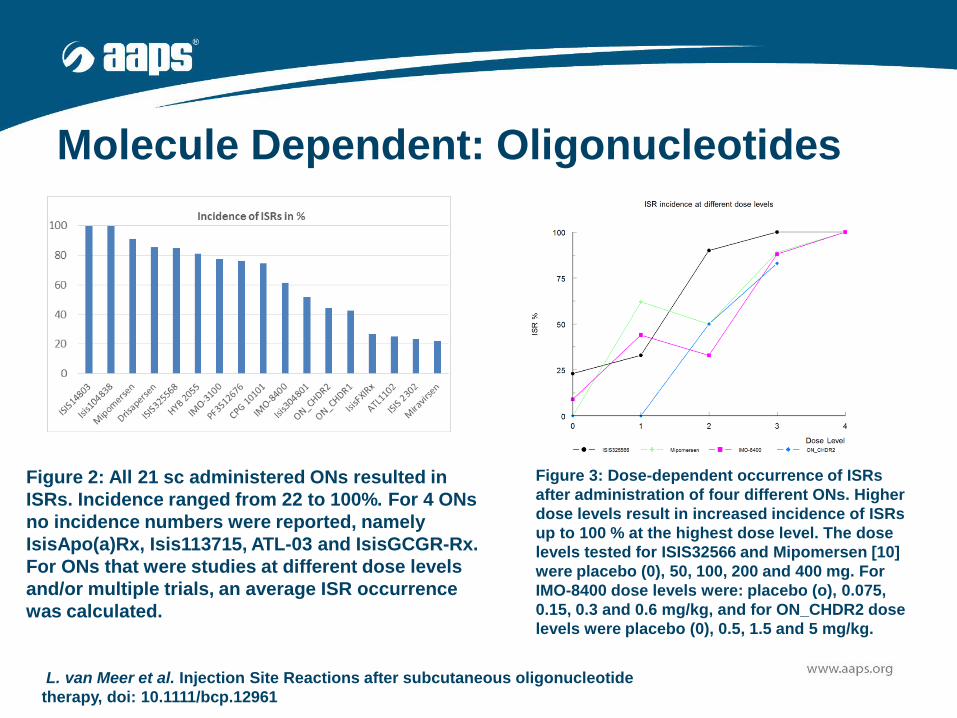
Molecule Dependent: Oligonucleotides
Figure 2: All 21 sc administered ONs resulted in
ISRs. Incidence ranged from 22 to 100%. For 4 ONs
no incidence numbers were reported, namely
IsisApo(a)Rx, Isis113715, ATL-03 and IsisGCGR-Rx.
For ONs that were studies at different dose levels
and/or multiple trials, an average ISR occurrence
was calculated.
Figure 3: Dose-dependent occurrence of ISRs
after administration of four different ONs. Higher
dose levels result in increased incidence of ISRs
up to 100 % at the highest dose level. The dose
levels tested for ISIS32566 and Mipomersen [10]
were placebo (0), 50, 100, 200 and 400 mg. For
IMO-8400 dose levels were: placebo (o), 0.075,
0.15, 0.3 and 0.6 mg/kg, and for ON_CHDR2 dose
levels were placebo (0), 0.5, 1.5 and 5 mg/kg.
L. van Meer et al. Injection Site Reactions after subcutaneous oligonucleotide
therapy, doi: 10.1111/bcp.12961

pH Effects
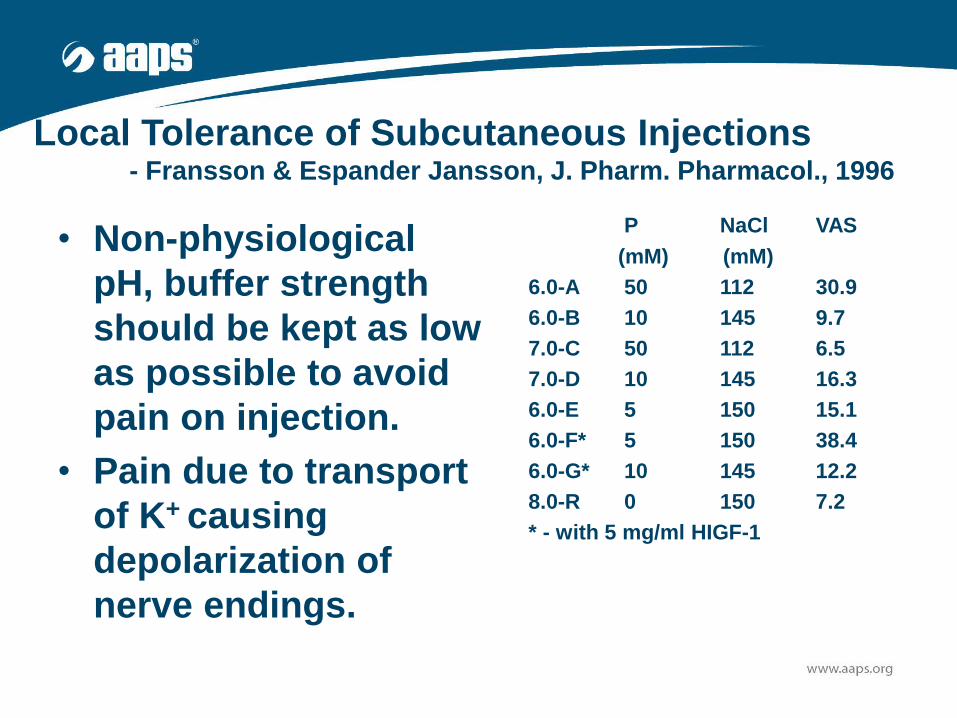
Local Tolerance of Subcutaneous Injections- Fransson & Espander Jansson, J. Pharm. Pharmacol., 1996
• Non-physiological
pH, buffer strength
should be kept as low
as possible to avoid
pain on injection.
• Pain due to transport
of K+ causing
depolarization of
nerve endings.
pH P NaCl VAS
(mM) (mM)
6.0-A 50 112 30.9
6.0-B 10 145 9.7
7.0-C 50 112 6.5
7.0-D 10 145 16.3
6.0-E 5 150 15.1
6.0-F* 5 150 38.4
6.0-G* 10 145 12.2
8.0-R 0 150 7.2
* - with 5 mg/ml HIGF-1
Excipients: Buffers• Goal Physiological pH (better to err on the more
basic versus acidic)
• Most common:
– Citrate (5-15 mM), Higher concentration 50 mM
can case pain (chelation of calcium)
– Acetates – Lower pH (concern with
lyophilization)
– Phosphates – need to be cautious complexation
• Alternatives: lactate and tartrate
Y. Mehmood, U. Farooq, Excipients Use in Parenteral and Lyophilized Formulation Development, Open
Science Journal of Pharmacy and Pharmacology 3(3): 19-27, 2015

An In Vitro Muscle Model
An isolated rodent extensor digitorum longus or soleus muscle
Carbogenated 37oC BSS
Creatine kinase activity is
measured with
spectrophotometric kinetic
assay at 340 nm
15 ml Test
Solution
Injected into
the muscle
or muscle
incubated in
the presence
of the test
compound

pH and Buffers*
• Carboxylic Buffers
– Acetate
– Succinate
– Citrate
• Type of Buffer
• pH Effect
– pH 2, 4, 6
• Buffer Capacity
– 0.1, 0.01, 0.001
*Napaporn et al., PDT, 2000
1. Buffer solutions with low concentrations should be
made isotonic.
2. For acetate buffer, formulate a solution at low buffer
capacity and near physiological pH. Although the
myotoxicity of acetate buffers is not significantly
different from normal saline, a trend towards
increased myotoxicity was evident at higher buffer
capacity and lower pH.
3. For succinate and citrate buffers, formulate near
physiological muscle pH as the myotoxicity is
minimized in this range.
General Formulation Considerations
Tonicity/OsmolarityConsequences: Enhanced tissue site irritation and
pain, tissue permeability and possible damage
• For intradermal, subcutaneous, and intramuscular
injections
– Ideally – around 300 30 mOsm/kg
– Preferably < 600 mOsm/kg
• Mitigation
– Avoid extreme pH and high buffer concentration
– Reduce injection volume
– Use anesthetic agentW. Wang, Tolerability of hypertonic injectables, International Journal of Pharmaceutics 490
(2015) 308–315
Injection Speed/Volume• 82 Individuals Type 1 or 2 Diabetes, 39% Females
• SC injections in the abdomen or thigh of 0.9% sodium chloride
• Injection speeds: 150, 300 and 450 µl/s
• Volumes: 400, 800, 1200 and 1600 µl
• Pain; Visual Analogue scale (VAS)
• Results:
– Lower end of the VAS scale
– Speed of injection was not significant
– Larger injection volumes (1200 and 1600 µl) were associated
with greater pain
– More pain associated with injections into thigh versus
abdomenHeise et al., Impact of injection speed and volume on perceived pain during subcutaneous injections
into the abdomen and thigh: a single-centre, randomized controlled trial, Diabetes, Obesity and
Metabolism 16: 971–976, 2014
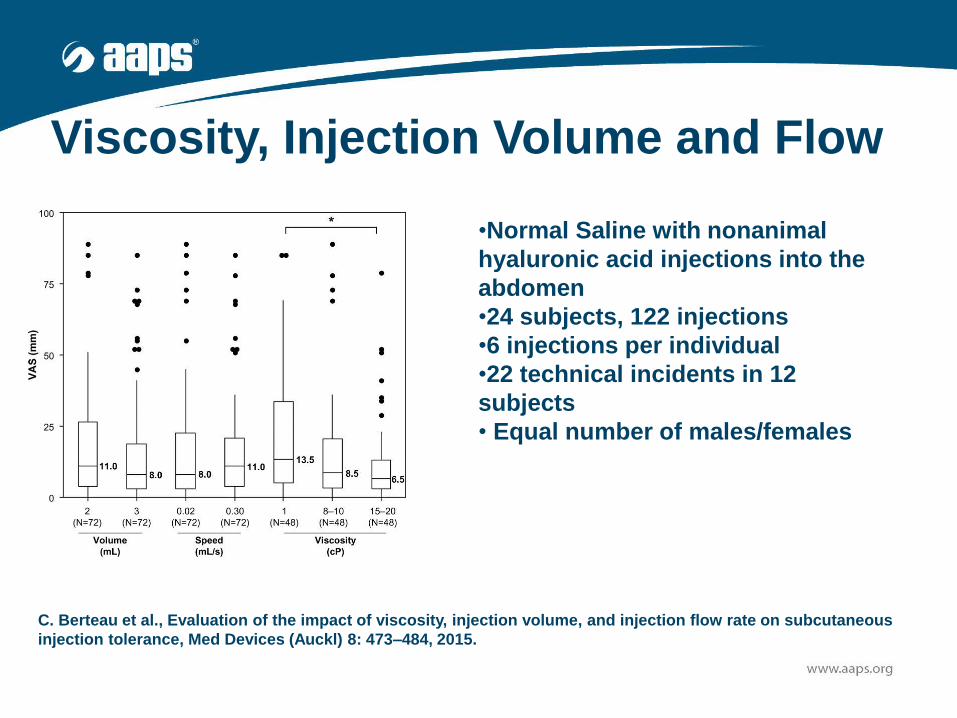
Viscosity, Injection Volume and Flow
C. Berteau et al., Evaluation of the impact of viscosity, injection volume, and injection flow rate on subcutaneous
injection tolerance, Med Devices (Auckl) 8: 473–484, 2015.
•Normal Saline with nonanimal
hyaluronic acid injections into the
abdomen
•24 subjects, 122 injections
•6 injections per individual
•22 technical incidents in 12
subjects
• Equal number of males/females
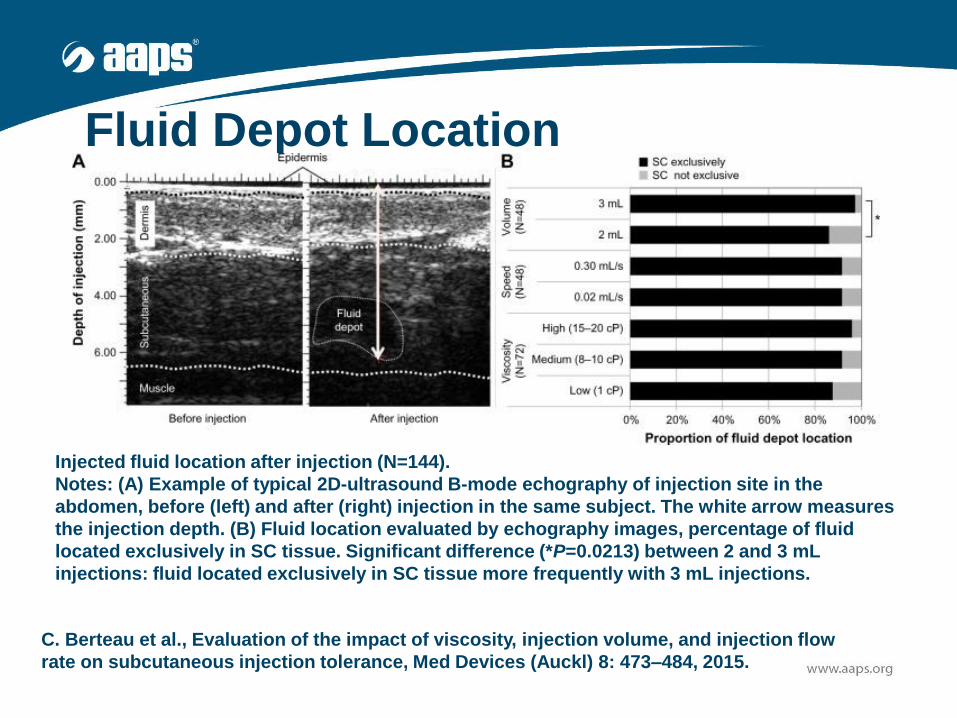
Fluid Depot Location
Injected fluid location after injection (N=144).
Notes: (A) Example of typical 2D-ultrasound B-mode echography of injection site in the
abdomen, before (left) and after (right) injection in the same subject. The white arrow measures
the injection depth. (B) Fluid location evaluated by echography images, percentage of fluid
located exclusively in SC tissue. Significant difference (*P=0.0213) between 2 and 3 mL
injections: fluid located exclusively in SC tissue more frequently with 3 mL injections.
C. Berteau et al., Evaluation of the impact of viscosity, injection volume, and injection flow
rate on subcutaneous injection tolerance, Med Devices (Auckl) 8: 473–484, 2015.

Particle Size – Tissue DamageDrug
Suspension Concentration
(%w/v)
Suspension Size
Classification pka Solubility Log P or cLogP
Bupivacaine5%
SmallMediumLarge
Local Anesthetic 8.05 Free Base Solubility:0.7 mg/mlat pH 7.4HCl Salt:40 mg/ml
3.41
Phenytoin10%
0.2 m1.2 m4 m6 m
Anticonvulsant 8.3 0.032 mg/mL 2.52
Diazepam10%
0.4 m1.7 m2.1 m
Anticonvulsant, sedative, and
muscle relaxant
3.4 Free Base: 0.06 mg/mL13
3.86
0
500
1000
1500
2000
Norm
al S
alin
e
Bupiv
acai
ne (s
mal
l)
Bupiv
acai
ne (m
ediu
m)
Bupiv
acai
ne ( l
arge)
Dia
zepam
(0.4
µm
)
Dia
zepam
(1.7
µm
)
Dia
zepam
(2.1
µm
)
Phenyt
oin (0
.2 µ
m)
Phenyt
oin (1
.2 µ
m)
Phenyt
oin (4
.0 µ
m)
Phenyt
oin (6
.0 µ
m)
Cu
mu
lati
ve C
K
(Mean
+ S
EM
)
* *
*
**
**
*
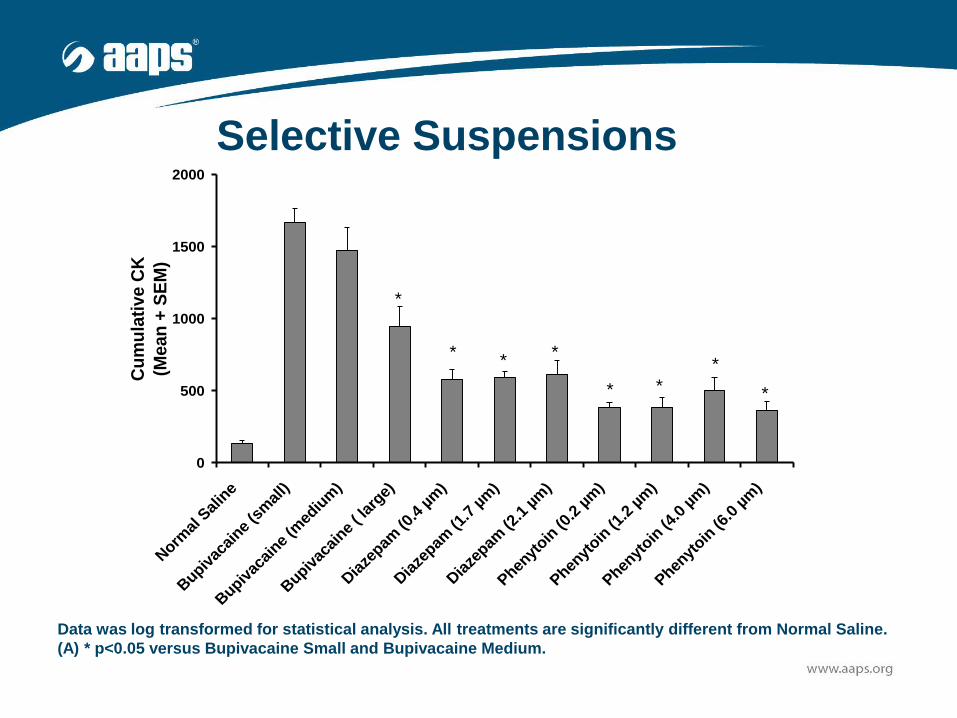
Data was log transformed for statistical analysis. All treatments are significantly different from Normal Saline.
(A) * p<0.05 versus Bupivacaine Small and Bupivacaine Medium.
Selective Suspensions
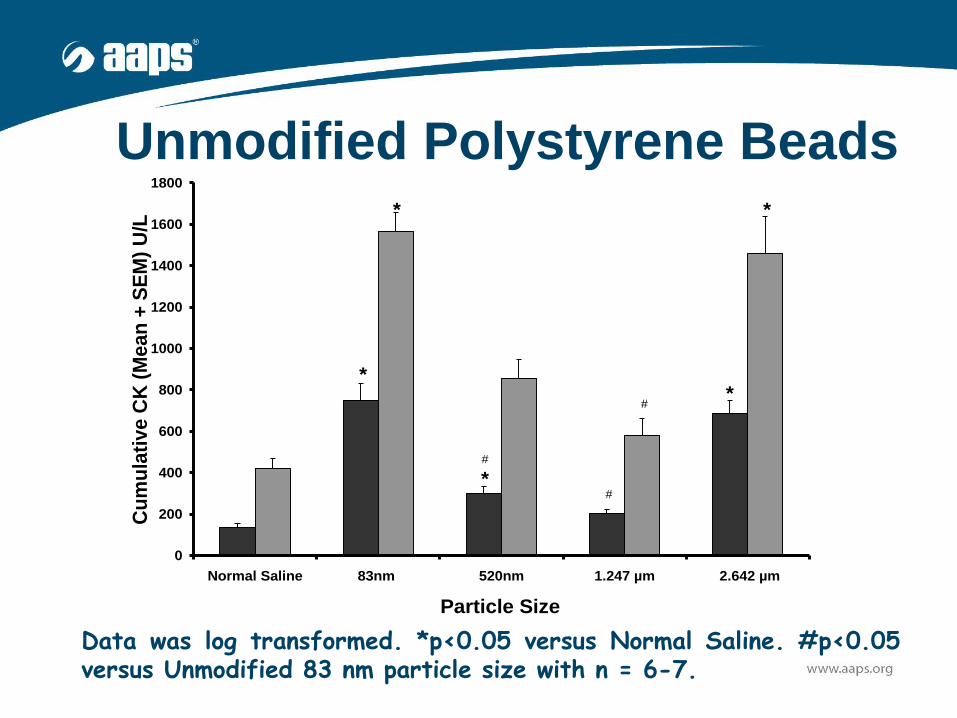
Unmodified Polystyrene Beads
0
200
400
600
800
1000
1200
1400
1600
1800
Normal Saline 83nm 520nm 1.247 µm 2.642 µm
Particle Size
Cu
mu
lati
ve C
K (
Mean
+ S
EM
) U
/L
* *
#
*#
#
**
Data was log transformed. *p<0.05 versus Normal Saline. #p<0.05versus Unmodified 83 nm particle size with n = 6-7.
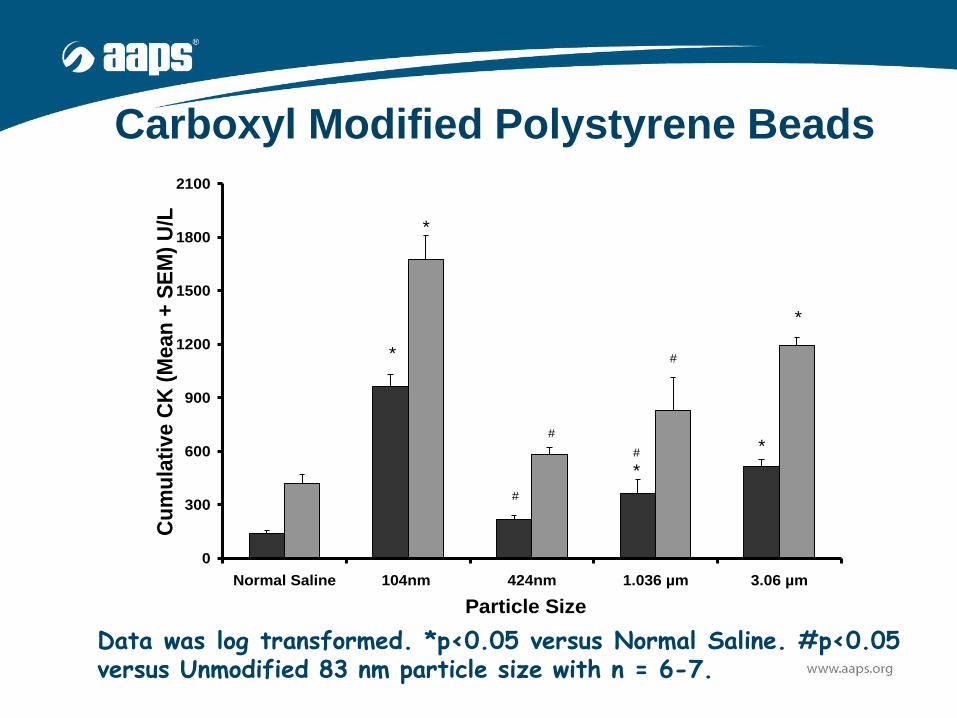
Carboxyl Modified Polystyrene Beads
0
300
600
900
1200
1500
1800
2100
Normal Saline 104nm 424nm 1.036 µm 3.06 µm
Particle Size
Cu
mu
lati
ve C
K (
Mean
+ S
EM
) U
/L *
*
#
#
#
#
*
*
*
Data was log transformed. *p<0.05 versus Normal Saline. #p<0.05versus Unmodified 83 nm particle size with n = 6-7.
Minimizing Injection Pain SQ Injections
• Medication should be at room
temperature
• Warm the injection solution
• Let alcohol dry before injection
• Optimize injection depth
• Injection sites should be rotated
• Message the site after injection

Conclusions – SQ Injection Formulations
• Complex site with potential for pain and/or tissue
damage
• Ideally goal is to minimize the concentration of API,
excipients, injection volume, pH, tonicity and
viscosity needed for formulation stability and release
• Look at the pharmacological properties of the API or
excipients which could cause pain or tissue damage
• Screen early in the development process for potential
pain or tissue damage.

Questions
Thank You!
Gayle Brazeau
University of New England
College of Pharmacy