functional health literacy, medication-taking self-efficacy and adherence to antiretroviral therapy
TRANSCRIPT

ORIGINAL RESEARCH
Functional health literacy, medication-taking self-efficacy and
adherence to antiretroviral therapy
Alison M. Colbert, Susan M. Sereika & Judith A. Erlen
Accepted for publication 10 March 2012
Correspondence to A.M. Colbert:
e-mail: [email protected]
Alison M. Colbert PhD RN
Assistant Professor
School of Nursing, Duquesne University,
Pittsburgh, Pennsylvania, USA
Susan M. Sereika PhD
Assistant Professor
School of Nursing, University of Pittsburgh,
Pennsylvania, USA
Judith A. Erlen PhD RN
Professor and Department Chair, Health and
Community Systems
School of Nursing, University of Pittsburgh,
Pennsylvania, USA
COLBERT A.M., SEREIKA S.M. & ERLEN J.A. (2012)COLBERT A.M. , SEREIKA S.M. & ERLEN J.A. (2012) Functional health literacy,
medication-taking self-efficacy and adherence to antiretroviral therapy. Journal of
Advanced Nursing 00(0), 000–000. doi: 10.1111/j.1365-2648.2012.06007.x
AbstractAims. To report a study of the relationship between functional health literacy and
medication adherence, as mediated by medication-taking self-efficacy, while con-
trolling for the effect of key demographic variables (such as race, income and level of
education).
Background. Medication adherence is critical to successful HIV/AIDS self-man-
agement. Despite simplified regimens and the availability of tools to assist with
medication-taking, adherence remains a challenge for many people living with HIV/
AIDS.
Design. Cross-sectional, secondary analysis.
Methods. Data for this study of 302 adults living with HIV/AIDS who were taking
antiretroviral medications were collected from January 2004–December 2007.
Medication adherence was measured using electronic event monitors. Bivariate
analyses and stepwise regression were conducted to examine the associations among
functional health literacy, medication-taking self-efficacy and HIV medication
adherence.
Results. Overall, functional health literacy was much higher than expected; how-
ever, adherence in this sample was sub-optimal. Higher medication-taking self-
efficacy was associated with higher medication adherence; however, functional
health literacy was not significantly related to either medication adherence or self-
efficacy beliefs. Hence, medication-taking self-efficacy did not mediate the rela-
tionship between functional health literacy and medication adherence.
Conclusions. Medication adherence continues to be an issue for people living with
HIV/AIDS. Additional research is needed to understand the disparate findings
related to functional health literacy and medication adherence in this and other
studies examining this association.
Keywords: health literacy, HIV, medication adherence, nurses, nursing, self-efficacy
� 2012 Blackwell Publishing Ltd 1
J A N JOURNAL OF ADVANCED NURSING

Introduction
Successful self-management of HIV requires substantial effort
on the part of the individual because of the need for
consistent and effective medication taking behaviours.
Research has shown that viral suppression may require
nearly 100% adherence, but maintaining rates greater than
95% translates into less than one missed dose per week for a
patient on a twice-a-day pill regimen (Deeks et al. 1999,
Paterson et al. 2000). Effective management of HIV/AIDS is
a global issue, as there are approximately 33 million people
living with HIV/AIDS in the world today and 5 million are
currently receiving an HIV medication (Joint United Nations
Programme on HIV/AIDS 2010). Nurses are in an ideal
position to help patients to better manage their medication
regimen and this nursing role requires a solid understanding
of the various aspects of adherence. Functional health literacy
may be one of the many factors influencing the health
management behaviours of people living with HIV.
Background
Medication adherence is a critical issue in the management of
HIV/AIDS because poor rates of adherence can lead to
unsuccessful viral suppression, resistance to medication,
opportunistic infections, overall poor health, decreased
quality of life and potentially death (Bangsberg et al. 2001,
McNabb et al. 2003, Carballo et al. 2004). Therefore,
persons with HIV/AIDS who have inadequate functional
health literacy are even more vulnerable in accessing health
services and are at greater risk for poor health outcomes.
Even when they access health services and have discussions
with nurses about their medications, the person with lower
functional health literacy may not know what questions to
ask or may not fully comprehend what the nurses are
explaining to them. Researchers estimate the proportion of
people living with HIV/AIDS who demonstrate lower or
marginal functional health literacy level to be around 18–
20% (Kalichman & Rompa 2000, Golin et al. 2002, Drai-
noni et al. 2008, Kalichman et al. 2008).
Several published studies have directly examined the
association between functional health literacy and medica-
tion adherence in people living with HIV; however, the
results are inconsistent. Several authors showed that lower
functional health literacy is related to poorer adherence
(Kalichman et al. 2007, Osborn et al. 2007, Kalichman et al.
2008, Osborn et al. 2010). Conversely, others have found
that lower functional health literacy was not associated with
lower medication adherence (Golin et al. 2002, Wolf et al.
2004, Paasche-Orlow et al. 2006, Wolf et al. 2007, Murphy
et al. 2010). Among those, Paasche-Orlow et al. (2006)
found that low functional health literacy was not associated
with lower odds of adherence or viral suppression in a
population of 235 individuals who were HIV-positive and
had a history of alcohol problems. In fact, the authors
reported a non-significant trend that lower functional health
literacy might be associated with better adherence and
virological suppression.
The disparate findings may be attributable to issues of
measurement relative to the variables of interest. The
measurement of adherence is a complicated and controversial
issue. Individuals with lower functional health literacy may
have difficulty understanding what information is necessary
to report when asked about their adherence levels. In turn,
this may have an effect on studies investigating adherence. In
a qualitative study of 25 HIV-positive patients (75% with
lower functional health literacy as assessed by the Rapid
Estimate of Adult Literacy in Medicine), Wolf et al. (2005)
examined the association of health literacy with the partic-
ipants’ responses to HIV medication-adherence question-
naires. The authors’ analysis revealed several themes related
to format, administration and visual aids. The majority of
respondents thought that adherence measured as recall over
3 days was not accurate. In addition, most believed they
would require one-on-one assistance to complete a self-report
measure accurately (Wolf et al. 2005). These findings raise
issues about the validity of self-report as a measure of
adherence in people with lower functional health literacy.
Although all methods of measurement have their unique
problems, electronic event monitoring (EEM), a method for
indirectly monitoring mediation adherence, is believed to
offer more information over time than biological assays
(Turner 2002) and may be a more appropriate choice when
considering adherence in the context of health literacy. EEM
consists of a medication cap containing a micro-electronic
circuit that fits on a standard medication bottle and records
the time and date each time the bottle cap is opened.
However, most studies exploring adherence and health
literacy used self-report as the measure of adherence; those
that did not used pharmacy refills or pill counts (Graham
et al. 2007, Kalichman et al. 2007, 2008). Golin et al. (2002)
used a composite score that comprised of electronic moni-
toring, pill counts and self-report.
Measures of health literacy used among the published
studies also vary with the most commonly used measure
being the short version of the Test of Functional Health
Literacy in Adults (S-TOFHLA) and the Rapid Estimate of
Adult Literacy in Medicine (REALM). The S-TOFHLA,
described in greater detail below, measures the ability to
understand prose and to read and understand numerical
A.M. Colbert et al.
2 � 2012 Blackwell Publishing Ltd

information related to health management (Baker et al.
1999). The REALM is a 66-word recognition and pronun-
ciation test (Davis et al. 1993). In addition, the cut-off points
distinguishing higher and lower health literacy scores varied
across studies.
When considering the issue of HIV medication adherence,
researchers have explored how confidence in one’s ability to
take medication (self-efficacy) may be related to outcomes.
Results from several studies have supported the relationship
between higher self-efficacy and better HIV medication
adherence (Buchmann 1997, Catz et al. 2000, Simoni et al.
2002, Johnson et al. 2003, Cha et al. 2008) providing a
rationale for continued inquiry into the relationship between
self-efficacy and adherence and how other factors may be
influenced by self-efficacy. This association is supported
across diverse HIV-positive populations. Researchers found
that self-efficacy mediated the relationship between health
literacy and HIV medication adherence, as measured by self-
report (Wolf et al. 2007). An individual’s ability to read and
understand health directions may indeed be influenced by
their confidence in their abilities to take their medications
under different and changing circumstances.
Nurses working with people living with HIV/AIDS are in
an important position to assist with medication adherence
and to facilitate effective self-management strategies related
to medication taking. Orem’s self-care deficit nursing theory
posits that the nurse must comprehensively assess a patient
to identify key deficits related to self-care and that care
should then be provided according to the degree of the
deficit. Functional health literacy, medication-taking self-
efficacy and medication adherence are all potential areas for
deficits and research into how these issues are related may
give additional insight into how best to intervene (Orem
2001).
Bandura’s Social Cognitive Theory guided the selection of
variables of interest for this study; this framework focuses
heavily on the role of self-efficacy in behaviour. Bandura
(1997) asserts that self-efficacy is the self-assurance with
which individuals approach tasks to accomplish a specific
behaviour; self-efficacy determines whether or not people
make good use of their capabilities and can ultimately be
successful. Functional health literacy may play an important
role in an individual’s development of self-assurance in the
context of health.
Using the published literature and Bandura’s theory, we
hypothesized that (1) functional health literacy has a direct,
positive effect on medication-taking self-efficacy; and (2)
functional health literacy has an indirect, positive effect on
HIV medication adherence through medication-taking self-
efficacy.
The study
Aims
The article is a report of a study of the relationship between
functional health literacy and medication adherence, as
mediated by medication-taking self-efficacy, while control-
ling for the effects of key demographic variables (such as race,
income and level of education).
Design
This secondary analysis was a correlational study that used
de-identified baseline data obtained from the parent study,
‘Improving Adherence to Antiretroviral Therapy’ (2R01
NR04749, J. A. Erlen, PI), to address the aims of the study
and to test the hypotheses. The parent study’s project director
served as an honest broker, collecting and collating all
relevant data and replacing any identifiers with a code,
thereby making it impossible for the study investigators to
identify the participants. This process assured subject ano-
nymity. Data were collected from January 2004–December
2007. The parent study is a randomized clinical trial
comparing the efficacy of two nurse-delivered telephone
interventions (structured and individualized) on HIV medica-
tion adherence (Wickersham et al. 2011). The interventions,
focused on habit formation and problem solving, were based
on social cognitive and self-efficacy theory (Bandura 1997).
Sample/participants
Participants for the parent study were recruited from western
Pennsylvania and eastern Ohio via clinics and community
organizations serving people living with HIV/AIDS. All
participants from the parent study who completed the
functional health literacy assessment were included in this
analysis. To be eligible for the parent study, participants had
to be 18 years of age or older, able to speak and understand
English, free from HIV-related dementia as evidenced by
assessment using an HIV dementia tool (Power et al. 1995),
prescribed HIV medications, self administering the prescribed
HIV-antiretroviral medication and not living with a current
participant in the study.
A total of 354 participants were enrolled in the parent
study; of these 18 (5Æ1%) were excluded from this secondary
analysis because the functional health literacy assessment was
not completed. An additional three participants (0Æ8%) were
excluded due to a lack of electronic adherence data; all three
of these participants were classified as having adequate
functional health literacy. Finally, the secondary analysis
JAN: ORIGINAL RESEARCH Health literacy and HIV adherence
� 2012 Blackwell Publishing Ltd 3

included only those participants who self-reported as White
or African American, due to the very small number of people
not included in one of those two groups, their heterogeneity
(n = 31, 9Æ3% of those with adequate data, from eight
different ethnic groups) and the study aim of examining race
as a potential confounding variable. Therefore, the final
sample for this study included 302 participants.
Data collection
All data were collected as part of the parent study. At the first
visit, participants were screened for inclusion and enrolled if
eligible. They were instructed in the use of the medication
diary and the electronic event monitor and asked to return
home and use the monitor for approximately 1 month with
one antiretroviral medication, randomly selected by project
staff. One month later participants were mailed a booklet of
questionnaires, allowing them to complete the self-adminis-
tered measures at home. The participants then returned for
the baseline data collection, at which time the data from the
electronic event monitors were downloaded, the functional
health literacy tool was administered and the remaining
questionnaires that required face-to-face format or that they
be timed were completed. These data were collected prior to
randomization in the parent study. The specific data used in
this study were obtained during the baseline data collection
session.
Functional health literacy was measured using the Short
Test for Functional Health Literacy (Baker et al. 1999). The
S-TOFHLA is a shorter version of the standard TOFHLA
which uses materials a patient may encounter in the context
of healthcare, such as patient instructions for surgery and a
prescription bottle. Functional health literacy was dichoto-
mized as inadequate/marginal (£ 75) or adequate (>75). The
S-TOFHLA demonstrated high internal consistency reliabil-
ity, with a Cronbach’s alpha of 0Æ953.
Adherence was objectively assessed using EEM, augmented
by daily diary self-report. EEM consists of a medication cap
containing a micro-electronic circuit that fits on a standard
medication bottle and records the time and date each time the
cap is opened. Participants were also asked to keep a daily
diary to track pocket dosing and refills of the medication
bottle. In these instances, the EEM data were augmented by
data from the medication-taking diary before summarizing
data to adherence indices.
For analysis, adherence was reported as both a continuous
variable (percentage of days with the correct intake or
percentage of number of prescribed administrations taken)
and a categorical variable based on the continuous variable
(<85% adherence, ‡ 85% adherence). This cut-off was
chosen because it reflects a moderate to high level of
adherence. Although the traditional cut-off point in HIV is
often 95–100%, the lower threshold for ‘higher’ adherence
may be more consistent with Bangsberg’s (2006) research
demonstrating effectiveness of medications at lower levels of
adherence. For the regression models, percentage of days
with correct intake was used as the dependent variable.
Self-efficacy was conceptualized as medication-taking self-
efficacy beliefs, or one’s belief in his/her ability to plan and
perform a desired behaviour. Self-efficacy was measured
using the Self-Efficacy Beliefs subscale of the HIV Self-
Efficacy Scale for Medication Taking (Erlen et al. 2010). The
content relates specifically to antiretroviral medication taking
and measures the level, generality and strength of medication-
taking self-efficacy. The total score for the self-efficacy beliefs
subscale ranges from 17–170. The subscale demonstrated
good internal consistency reliability with a Cronbach’s alpha
of 0Æ95.
Two investigator-developed tools, the Health Survey and
Medical Record Review were used to collect HIV-health
history information. To provide the most accurate data
possible, we first used available medical records to obtain
CD4 counts and detectable/undetectable viral load data.
When medical records were unavailable, we used self-report
as an additional data source. The Center for Research in
Chronic Disorders (CRCD) Socio-demographic Question-
naire was used to collected socio-demographic information.
Ethical considerations
Institutional Review Board (IRB) approval was obtained for
this secondary data analysis; the parent study had separate
IRB approval. In the parent study informed consent was
obtained from all participants prior to screening or the
collection of any baseline data.
Data analysis
Analysis was performed using SPSSSPSS (version 16.0; SPSS Inc.,
Chicago, IL, USA) and SASSAS (version 9.2; SAS Institute Inc.,
Cary, NC, USA). Measures of central tendency (means,
medians) and dispersion (standard deviations, ranges) were
used to summarize the continuous-type participant descrip-
tors, medication adherence and self-efficacy; frequency
counts and percentages were used to summarize categorical
descriptors. Bivariate analyses (t-tests, Mann–Whitney
U-test, Pearson correlation, Spearman correlation and chi-
square tests of independence, as appropriate) were conducted
to examine the unadjusted associations between dichotomized
functional health literacy and selected socio-demographic
A.M. Colbert et al.
4 � 2012 Blackwell Publishing Ltd
factors (as listed in Table 1) and HIV-health history infor-
mation (viral load, CD4 and number of medications) and
then the associations of those variables to medication
adherence.
To examine the relationship between functional health
literacy and medication adherence, stepwise multiple regres-
sion was performed treating medication adherence as the
outcome variable; included in the model were all variables
that met the screening criteria (P < 0Æ20) when examined
bivariately with adherence. The resultant models were
evaluated and modified to include only important correla-
tions and to identify the most parsimonious model. Signifi-
cance levels were set a priori at 0Æ05, except where indicated.
Due to the relatively small number of people with low health
literacy in this sample, we used bootstrapping to estimate
regression coefficient and confidence interval. A bootstrap
sample of 302 participants was generated by randomly
sampling with replacement from the original ‘real’ sample.
Since this new sample is drawn from the original sample via
sampling with replacement, the resulting bootstrap sample
would not be identical to the original sample. A multiple
regression was estimated on a bootstrap sample. Regression
coefficients were recorded. These steps were repeated 1000
times (i.e. 1000 bootstrap replication). An empirical sampling
distribution of a regression coefficient was estimated using
the results from the 1000 bootstrap replications. A 95%
confidence interval (CI) was computed for each regression
coefficient by computing the 2Æ5 and 97Æ5 percentile scores.
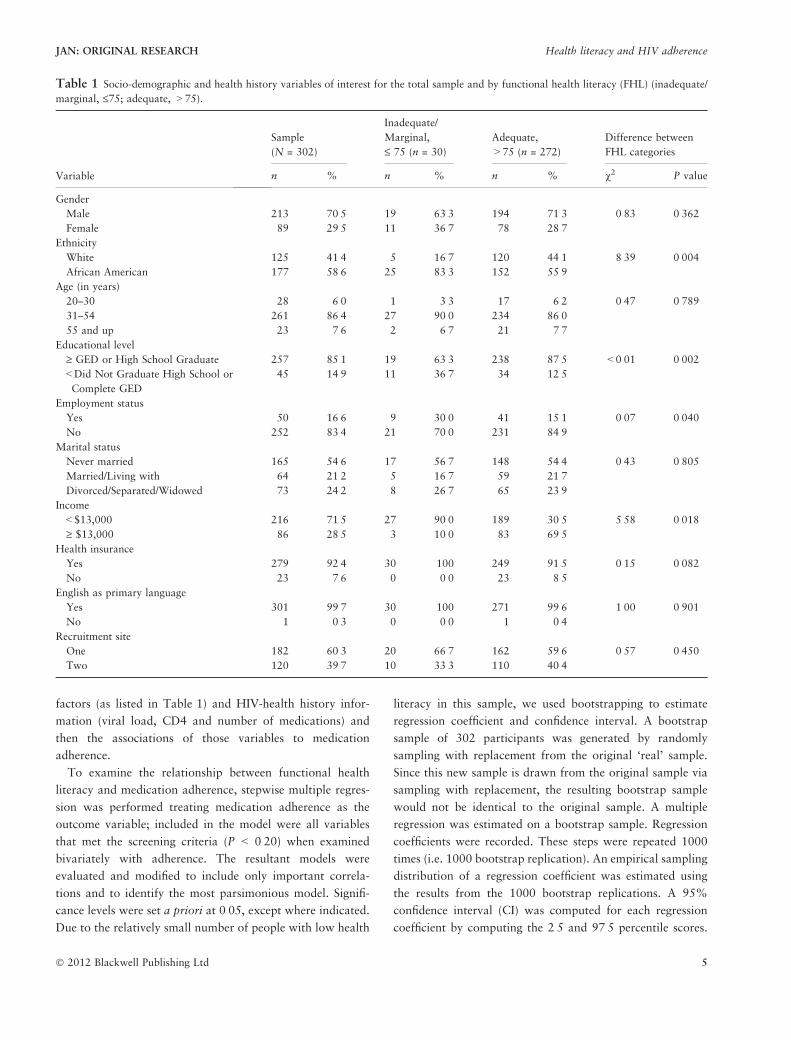
Table 1 Socio-demographic and health history variables of interest for the total sample and by functional health literacy (FHL) (inadequate/
marginal, £75; adequate, >75).
Variable
Sample
(N = 302)
Inadequate/
Marginal,
£ 75 (n = 30)
Adequate,
>75 (n = 272)
Difference between
FHL categories
n % n % n % v2 P value
Gender
Male 213 70Æ5 19 63Æ3 194 71Æ3 0Æ83 0Æ362
Female 89 29Æ5 11 36Æ7 78 28Æ7Ethnicity
White 125 41Æ4 5 16Æ7 120 44Æ1 8Æ39 0Æ004
African American 177 58Æ6 25 83Æ3 152 55Æ9Age (in years)
20–30 28 6Æ0 1 3Æ3 17 6Æ2 0Æ47 0Æ789
31–54 261 86Æ4 27 90Æ0 234 86Æ055 and up 23 7Æ6 2 6Æ7 21 7Æ7
Educational level
‡ GED or High School Graduate 257 85Æ1 19 63Æ3 238 87Æ5 <0Æ01 0Æ002
<Did Not Graduate High School or
Complete GED
45 14Æ9 11 36Æ7 34 12Æ5
Employment status
Yes 50 16Æ6 9 30Æ0 41 15Æ1 0Æ07 0Æ040
No 252 83Æ4 21 70Æ0 231 84Æ9Marital status
Never married 165 54Æ6 17 56Æ7 148 54Æ4 0Æ43 0Æ805
Married/Living with 64 21Æ2 5 16Æ7 59 21Æ7Divorced/Separated/Widowed 73 24Æ2 8 26Æ7 65 23Æ9
Income
<$13,000 216 71Æ5 27 90Æ0 189 30Æ5 5Æ58 0Æ018
‡ $13,000 86 28Æ5 3 10Æ0 83 69Æ5Health insurance
Yes 279 92Æ4 30 100 249 91Æ5 0Æ15 0Æ082
No 23 7Æ6 0 0Æ0 23 8Æ5English as primary language
Yes 301 99Æ7 30 100 271 99Æ6 1Æ00 0Æ901
No 1 0Æ3 0 0Æ0 1 0Æ4Recruitment site
One 182 60Æ3 20 66Æ7 162 59Æ6 0Æ57 0Æ450
Two 120 39Æ7 10 33Æ3 110 40Æ4
JAN: ORIGINAL RESEARCH Health literacy and HIV adherence
� 2012 Blackwell Publishing Ltd 5

With this approach, if the 95% CI of a regression coefficient
does not include 0, this is equivalent to P < 0Æ05. (Shrout &
Bolger 2002). The unstandardized regression coefficient and
95% CI are reported in the results. Mediation was also
analysed through bootstrapping, as it has been shown that
bootstrapping estimates the significance of mediation effect
accurately (Shrout & Bolger 2002). To evaluate the final
model, Cohen’s (1988) effect size values for regression was
used, which specifies an R2 of 0Æ02 to be small and 0Æ13 to be
medium.
Results
Participants
The sample comprised 302 participants. Primarily men
(70Æ5%) and African American (58Æ6%), the sample had a
mean age of 43Æ9 years (SDSD 7Æ94) and an average of 13Æ0 years
of education (SDSD 2Æ70). Over 70% of the sample (n = 216)
reported household incomes of less than $13,000 per year.
Table 1 provides additional socio-demographic information
about the participants.
Health literacy
Overall, 9Æ9% (n = 30) of the participants were classified as
having inadequate/marginal functional health literacy (95%
CI = 7Æ05%, 13Æ83%). Total scores on the S-TOFHLA
ranged from 7–100 and, as expected, were heavily negatively
skewed, with a mean score of 90Æ09 (SDSD = 12Æ84, 95%
CI = 88Æ63, 91Æ54), median of 94 and mode of 98. A total of
53 participants (17Æ5%) scored 100 and 68Æ9% scored 90 or
above. Table 1 displays the difference in selected character-
istics between the two functional health literacy levels,
inadequate/marginal (£75) and adequate (>75).
HIV medication adherence, functional health literacy and
medication-taking self-efficacy
The mean adherence based on EEM for the sample was
67Æ71% (SDSD 32Æ91) for the average per cent of days with the
correct number of doses taken (95% CI = 63Æ98, 71Æ44).
There was no important difference in adherence levels
between patients having the inadequate/marginal and ade-
quate functional health literacy (U = 3845Æ50, Z = �0Æ521,
P = 0Æ602). Over three fourths of this sample (78Æ1%) had
adherence levels less than 95% and about half of the sample
(52%) had adherence levels less than 85%. In contrast to the
functional health literacy scores, adherence levels in the
sample were highly variable.
The mean self-efficacy beliefs score was 139Æ54 (SDSD 29Æ48),
with scores ranging from 17–170, suggesting a moderately
high level of self-efficacy beliefs. Self-efficacy belief scores did
not differ between inadequate/marginal and adequate func-
tional health literacy levels (U = �3997Æ00, Z = �0Æ183,
P = 0Æ855).
Stepwise multiple linear regression with the continuous
measure of medication adherence level as the outcome and
those variables that met selection criteria (self-efficacy beliefs,
health literacy, race, gender, age, education, employment
status, viral load and number of medications), showed
medication adherence to be significantly related to race,
self-efficacy beliefs, viral load and number of medications,
R2 = 0Æ089 (95% CI = 0Æ026, 0Æ169). African Americans had
significantly lower medication adherence than Whites,
b = �8Æ23 (95% CI = �15Æ25, �0Æ57). Greater medication
adherence was associated with higher self-efficacy beliefs,
b = 0Æ21 (95% CI = 0Æ08, 0Æ35). The participants with a
detectable viral load had significantly lower medication
adherence than the participants with an undetectable viral
load, b = �8Æ34 (95% CI = �15Æ93, �0Æ63). The participants
taking 2–3 medications had significantly higher medication
adherence than the participants only taking 1 medication,
b = 22Æ01 (95% CI = 2Æ43, 42Æ40). There was no important
difference in medication adherence between participants
taking 1 medication and those taking 4–5 medications,
b = 17Æ05 (95% CI = �3Æ86, 39Æ62). These results led to the
decision to reject both hypotheses; functional health literacy
did not have any important effect on medication-taking self-
efficacy; and functional health literacy did not have an
indirect, positive effect on HIV medication adherence,
mediated by medication-taking self-efficacy.
Discussion
The findings from this study indicate that there is no
statistically significant association between HIV medication
adherence and functional health literacy, as measured using
the S-TOFHLA. This is one of only a few published
investigations to examine functional health literacy and
medication adherence using electronic monitoring in people
living with HIV/AIDS.
These results are contrary to both our original hypotheses.
Functional health literacy was not related to medication-
taking self-efficacy. The non-significant correlation between
functional health literacy and medication adherence leads to
the rejection of our second hypothesis; medication-taking
self-efficacy did not mediate the association between func-
tional health literacy and HIV medication adherence. The
results do support one of the primary tenets in Bandura’s
A.M. Colbert et al.
6 � 2012 Blackwell Publishing Ltd

theory; specifically, the critical role of self-efficacy in
projecting expected behaviour.
Our results support the work of Golin et al. (2002), Wolf
et al. (2004) and Paasche-Orlow et al. (2006), which all
reported no important correlationship between HIV medica-
tion adherence and functional health literacy. However, our
findings contradict separate research studies that did find an
important association. This discrepancy may be attributable
to the various methods for assessing functional health literacy
and adherence. Several of the studies measured adherence
using self-report which has potential problems with memory
and recall bias (Turner 2002). However, Golin et al. (2002),
the study with the most comprehensive assessment of
adherence, reported a mean adherence rate similar to ours
at 71Æ3%.
These findings specific to health literacy rates were quite
different than expected; based on previously published work
in this area, we anticipated that 18–20% of this sample
would have lower functional health literacy. Also of note is
that what is considered the definition for ‘higher’ and ‘lower’
health literacy is also highly variable across studies. For
example, Kalichman et al. (1999) used an amended version
of the S-TOFHLA that included an HIV-specific reading
comprehension section along with two of the standard
reading sections and the numeracy items. The authors
considered those with greater than 85% of the items as
correct to have higher functional health literacy and those
with 85% or less to have lower functional health literacy. In a
different study assessing HIV-knowledge, Kalichman and
Rompa (2000) used a cut-off of 80% as the distinction
between higher and lower functional health literacy. Golin
et al. (2002), conversely, used the S-TOFHLA reading
comprehension section as a continuous variable in model
testing. The most recent study, Paasche-Orlow et al. (2006)
and Wolf et al. (2007) both used the REALM, with grade
level cut-off points (less than sixth grade as inadequate,
seventh–eighth grade as marginal and ninth grade and higher
as adequate). Studies using the S-TOFHLA in other popula-
tions have used cut-off points varying from 67–75% for
inadequate/marginal. Most recently, Osborn et al. (2010)
introduced an HIV-specific test of health literacy called the
Brief Estimate of Health Knowledge and Action (BEHKA)
and found that when using this instrument to measure health
literacy, lower scores in health literacy were associated with
poorer adherence. To move research in health literacy and
medication adherence forwards, researchers will need to
come to a consensus about measurement.
Our results contradict the work of Wolf et al. (2007), who
found a statistically significant association between func-
tional health literacy and medication adherence that was
mediated by self-efficacy. Our findings may be the result of
differences in the measurement strategy or the limited
variability of functional health literacy in our sample. Wolf
et al. used a 4-day recall self-report to measure adherence and
dichotomized results as 100% or less than 100%; they also
used the REALM to measure functional health literacy. Our
results do support, however, the broad body of research that
has found self-efficacy to be associated with adherence.
Adherence, in contrast to functional health literacy, was
quite variable in the sample. This finding supports the reports
of sub-optimal adherence to HIV medication, such as Mills
et al. (2006) meta-analysis that showed average HIV medi-
cation adherence to be approximately 55%. Although there
may be variation in the adherence levels required for viral
suppression, Bangsberg (2006) noted that the probability of
viral suppression, reduced disease progression and reduced
mortality are increased with greater adherence levels, thereby
supporting continued efforts to maximize adherence in
people living with HIV/AIDS.
No matter what the reason for the less than optimal
adherence (barring, perhaps, personal choice), poorer adher-
ence alone suggests that patients with HIV have at least some
degree of difficulty with managing their health. Although the
S-TOFHLA may be able to measure part of the functional
health literacy construct – specifically reading comprehension
– it may not be able to measure all of the components
adequately. This is consistent with continued calls from
researchers for different and more comprehensive ways to
measure functional health literacy, including tools that are
disease specific, such as the newly developed BEHKA
(Osborn et al. 2010).
Limitations
Several limitations to this study must be noted. First, the
relatively small number of people exhibiting lower health
literacy limits the extent of the examination between the
associations (potentially due to factors such as the high
educational level of the sample or a selection bias). Although
EEM is considered reliable for measuring adherence, EEM is
not infallible. Turner and Hecht (2001) point out that EEM
assessment does not demonstrate definitively that pills were
actually taken by the participant. In addition, participants
may refuse to participate in studies using EEM because they
may need to discontinue use of medication reminder systems,
resulting in a selection bias (Turner & Hecht 2001).
However, despite these limitations, EEM assessment can
provide valuable insight into the individual’s capacity to
create and maintain a consistent medication-taking behav-
iour. The parent study attempted to manage this weakness by
JAN: ORIGINAL RESEARCH Health literacy and HIV adherence
� 2012 Blackwell Publishing Ltd 7

asking participants to complete a daily medication-taking
journal, as described in the methods section.
Timing of the study and the rapid changes in medication
regimens for the treatment of HIV/AIDS may also be a
limitation, since the data collection began in 2004 and
regimens have been simplified over the years to allow for
fewer pills in a day. To address this, we examined the
association between both functional health literacy and
medication adherence with number of medications. The
number of HIV/AIDS medications that participants were
prescribed ranged from 1–5; this is similar to what is seen in
clinical practice today.
Finally, the study may also be limited because it is a
secondary data analysis; therefore the methodology and
measurement tools were selected to address other primary
research questions. However, the instruments and method-
ology addressed gaps in the literature and were appropriate
to the framework and the research question.
Conclusions
These findings have several important clinical implications
for nurses. First, adherence to medication for people living
with HIV continues to be an issue that warrants on-going
examination, with an understanding that there is no single
solution to this multi-factorial problem. The lack of an
important relationship between health literacy and medica-
tion adherence reinforces the idea that just because a patient
is able to easily read and understand a prescription does not
necessarily mean the patient is taking the medication as
prescribed. The results also suggest that African American
patients may be at higher risk for lower adherence rates.
Clinicians working with people living with HIV need to
assess adherence regularly with their patients; self-efficacy
may be another avenue to explore during the standard clinic
visit. Nurses need to ask patients about their self-confidence
in their ability to take their medications in their normal
schedule and when that schedule is disrupted; responses to
these questions may provide insight into individual medica-
tion taking behaviours.
These results identify several areas for additional
research. For example, researchers could design a study
to address specifically some of the limitations that may
have served as a deterrent to those with limited functional
health literacy, such as reading demands on recruitment
and data collection materials. Also, additional research
specifically targeted to individuals with lower functional
health literacy may contribute to a better understanding of
medication adherence in that particular population. The
racial differences that were identified warrant additional
exploration into how race, health literacy and medication
adherence may be related, and identify some potential bias
in the measurement strategy. Findings from Osborn et al.
(2007), where health literacy mediated the association
between race and HIV medication adherence support this
line of inquiry (Osborn et al. 2007). Interventions to help
patients more effectively manage their medication taking
are also clearly needed and incorporating strategies specif-
ically designed to improve self-efficacy should be consid-
ered. Finally, these results highlight the need for expanded
attention to how the functional health literacy construct is
being defined and measured to understand the role of
health literacy in self-management for chronic conditions
more fully.
What is already known about this topic
• Adherence is a critical component of HIV/AIDS
management; however, rates of medication adherence
are suboptimal.
• Health literacy has recently emerged as a potential
variable linked to chronic disease management,
although results have been contradictory.
• Self-efficacy has been shown to be related to medication
adherence in multiple populations, including those with
HIV/AIDS.
What this paper adds
• Health literacy assessed by the Short Test of Functional
Health Literacy in Adults may not be related to
medication adherence assessed using electronic
monitoring for adherence in a population actively
engaged in care.
• The connection between self-efficacy and HIV
medication adherence is further supported.
• African Americans were shown to be both more likely
to have inadequate health literacy and lower medication
adherence.
Implications for practice and/or policy
• Continued attention to medication adherence in the
clinical setting is critical.
• Helping people increase their self-efficacy around
medication taking may improve their adherence.
• Standardizing the way researchers, clinicians and policy
makers define and measure health literacy needs to
occur to better understand the problem and to improve
patient outcomes.
A.M. Colbert et al.
8 � 2012 Blackwell Publishing Ltd

Acknowledgements
The authors appreciate the contributions of the staff of the
Managing Medications Project at the University of Pittsburgh
School of Nursing, and the assistance of Dr. Kevin Kim. The
authors also wish to thank the study volunteers for their
participation.
Funding
This study was funded by National Institute for Nursing
Research (NINR) of the National Institute of Health (R01
NR04749 and 2R01 NR04749) and a Clinical & Transla-
tional Science Institute Fellowship (Colbert).
Conflict of interest
No conflict of interest has been declared by the authors.
Author contributions
All authors meet at least one of the following criteria
(recommended by the ICMJE: http://www.icmje.org/
ethical_1author.html) and have agreed on the final version:
• substantial contributions to conception and design,
acquisition of data, or analysis and interpretation of data;
• drafting the article or revising it critically for important
intellectual content.
References
Baker D.W., Williams M.V., Parker R.M., Gazmararian J.A. &
Nurss J. (1999) Development of a brief test to measure functional
health literacy. Patient Education & Counseling 38(1), 33–42.
Bandura A. (1997) Self-Efficacy: The Exercise of Control. W.H.
Fressman and Co., New York, NY.
Bangsberg D.R. (2006) Less than 95% adherence to nonnucleoside
reverse-transcriptase inhibitor therapy can lead to viral suppres-
sion. Clinical Infectious Diseases 43(7), 939–941.
Bangsberg D.R., Perry S., Charlebois E., Clark R., Robertson M.D.,
Zolopa A. & Moss A. (2001) Non-adherence to highly active
antiretroviral therapy predicts progression to AIDS. AIDS 15(9),
1181–1183.
Buchmann W.F. (1997) Adherence: a matter of self-efficacy and
power. Journal of Advanced Nursing 26(1), 132–137.
Carballo E., Cadarso-Suarez C., Carrera I., Fraga J., de la Fuente J.,
Ocampo A., Ojea R. & Prieto A. (2004) Assessing relationships
between health-related quality of life and adherence to antiretro-
viral therapy. Quality of Life Research 13, 587–599.
Catz S.L., Kelly J.A., Bogart L.M., Benotsch E.G. & McAuliffe T.L.
(2000) Patterns, correlates and barriers to medication adherence
among persons prescribed new treatments for HIV disease. Health
Psychology 19(2), 124–133.
Cha E., Erlen J.A., Kim K.H., Sereika S.M. & Caruthers D. (2008)
Mediating roles of medication-taking self-efficacy and depressive
symptoms on self-reported medication adherence in person with
HIV: a questionnaire survey. International Journal of Nursing
Studies 45, 1175.
Cohen J. (1988) Statistical Power Analysis for the Behavioral Sci-
ences, 2nd edn. Erlbaum Associate, Hillsdale, NJ.
Davis T.C., Long S.W., Jackson R.H., Mayeaux E.J., George R.B.,
Murphy P.W. & Crouch M.A. (1993) Rapid estimate of adult
literacy in medicine: a shortened screening instrument. Family
Medicine 25(6), 391–395.
Deeks S.G., Hecht F.M., Swanson M., Elbeik T., Loftus R., Cohen
P.T. & Grant R.M. (1999) HIV RNA and CD4 cell count response
to protease inhibitor therapy in an urban AIDS clinic: response to
initial and salvage therapy. AIDS 13, F35–F43.
Drainoni M.L., Rajabiun S., Rumptz M., Welles S.L., Relf M.,
Rebholz C., Holmes L., Dyl A., Lovejoy T., Dekker D. & Frye A.
(2008) Health literacy of HIV-positive individuals enrolled in an
outreach intervention: results of a cross-site analysis. Journal of
Health Communication 13(3), 287–302.
Erlen J.A., Cha E., Kim K.H. & Sereika S.M. (2010) The HIV
medication taking self-efficacy scale: psychometric evaluation.
Journal of Advanced Nursing 66(11), 2560.
Golin C.E., Liu H., Hays R.D., Miller L.G., Beck C.K., Ickovics J.,
Kaplan A.H. & Wenger N.S. (2002) A prospective study
of predictors of adherence to combination antiretroviral
medication. Journal of General Internal Medicine 17(10), 756–
765.
Graham J., Bennett I.M., Holmes W.C. & Gross R. (2007) Medi-
cation beliefs as mediators of the health literacy-antiretroviral
adherence relationship in HIV-infected individuals. AIDS &
Behavior 11(3), 385–392.
Johnson M.O., Catz S.L., Remien R.H., Rotheram-Borus M.J.,
Morin S.F., Charlebois E., Gore-Felton C., Goldsten R.B., Wolfe
H., Lightfoot M., Chesney M.A. & Team N.H.L.P. (2003) Theory-
guided, empirically supported avenues for intervention on HIV
medication nonadherence: findings from the healthy living project.
AIDS Patient Care STDS 17(12), 645–656.
Joint United Nations Programme on HIV/AIDS (UNAIDS) (2010)
Global Report: UNAIDS Report on the Global AIDS Epidemic
2010 (Publication UNAIDS/10.11E/JC1958E). Retrieved from
http://www.unaids.org/documents/20101123_GlobalReport_em.pdf
on February 1, 2012.
Kalichman S.C. & Rompa D. (2000) Functional health literacy is
associated with health status and health-related knowledge in
people living with HIV-AIDS. Journal of Acquired Immune Defi-
ciency Syndromes 25(4), 337–344.
Kalichman S.C., Catz S. & Ramachandran B. (1999) Barriers to HIV/
AIDS treatment and treatment adherence among African-American
adults with disadvantaged education. Journal of the National
Medical Association 91(8), 439–446.
Kalichman S.C., Amaral C.M., Stearns H., White D., Flanagan J.,
Pope H., Cherry C., Cain D., Eaton L. & Kalichman M.O. (2007)
Adherence to antiretroviral therapy assessed by unannounced pill
counts conducted by telephone. Journal of General Internal Med-
icine 22(7), 1003–1006.
Kalichman S.C., Pope H., White D., Cherry C., Amaral C.M.,
Swetzes C., Flanagan J. & Kalichman M.O. (2008) Association
JAN: ORIGINAL RESEARCH Health literacy and HIV adherence
� 2012 Blackwell Publishing Ltd 9

between health literacy and HIV treatment adherence: further
evidence from objectively measured medication adherence. Journal
of the International Association of Physicians in AIDS Care 7(6),
317–323.
McNabb J.J., Nicolau D.P., Stoner J.A. & Ross J. (2003) Patterns of
adherence to antiretroviral therapy predicts biologic outcomes for
human immunodeficiency virus-infected persons in clinical trials.
Clinical Infectious Diseases 34(8), 1115–1121.
Mills E.J., Nachega J.B., Buchan I., Orbinski J., Attaran A., Singh S.,
Rachlis B., Wu P., Cooper C., Thabane L., Wilson K., Guyatt G.H.
& Bangsberg D.R. (2006) Adherence to antiretroviral therapy in
sub-Saharan Africa and North America: a meta-analysis. Journal of
the American Medical Association 296(6), 679–690.
Murphy D.A., Lam P., Naar-King S., Harris R., Parsons J.T. &
Muenz L.R. (2010) Health literacy and antiviral adherence among
HIV-infected adolescents. Patient Education and Counseling 79,
25.
Orem D.E. (2001) Nursing Concepts of Practice, 6th edn. Mosby, St
Louis, MO.
Osborn C.Y., Paasche-Orlow M.K., Davis T.C. & Wolf M.S. (2007)
Health literacy: an overlooked factor in understanding HIV health
disparities. American Journal of Preventive Medicine 33(5), 374–
378.
Osborn C.Y., Davis T.C., Bailey S.C. & Wolf M.S. (2010) Health
literacy in the context of HIV treatment: introducing the brief
estimate of health knowledge and action (BEHKA)-HIV version.
AIDS & Behavior 14(1), 181–188.
Paasche-Orlow M.K., Cheng D.M., Palepu A., Meli S., Faber V. &
Samet J.H. (2006) Health literacy, antiretroviral adherence and
HIV-RNA suppression: a longitudinal perspective. Journal of
General Internal Medicine 21(8), 835–840.
Paterson D.L., Swindells S., Mohr J., Brester M., Vergis E., Squier C.,
Wagener M. & Singh N. (2000) Adherence to protease inhibitor
therapy and outcomes in patients with HIV infection. Annals of
Internal Medicine 133(1), 21–30.
Power C., Selnes O., Grim J.A. & McArthur J. (1995) HIV dementia
scale: a rapid screening tool. Journal of Acquired Immune Defi-
ciency Syndromes 8(3), 273–278.
Shrout P.E. & Bolger N. (2002) Mediation in experimental and
nonexperimental studies: new procedures and recommendations.
Psychological Methods 7(4), 422.
Simoni J.M., Frick P.A., Lockhart D. & Liebovitz D. (2002) Medi-
ators of social support and antiretroviral adherence among an
indigent population in New York City. AIDS Patient Care STDS
16(9), 431–439.
Turner B.J. (2002) Adherence to antiretroviral therapy by human
immunodeficiency virus infected patients. Journal of Infectious
Diseases 185, 143–151.
Turner B.J. & Hecht F.M. (2001) Improving on a coin toss to predict
patient adherence to medication. Annals of Internal Medicine
134(10), 1004–1006.
Wickersham K., Colbert A., Caruthers D., Tamres L., Martino A. &
Erlen J.A. (2011) Assessing fidelity to an intervention in a
randomized controlled trial to improve medication adherence.
Nursing Research 60(4), 264–269.
Wolf M.S., Davis T.C., Cross J.T., Marin E., Green K.W. & Bennett
C. (2004) Health literacy and patient knowledge in a southern U.S.
health clinic. International Journal of STD & AIDS 15(11), 747–
752.
Wolf M.S., Davis T.C., Arozullah A.M., Penn R., Arnold C., Sugar
M. & Bennett C. (2005) Relation between health literacy and HIV
treatment knowledge among patients on HAART regimens. AIDS
Care 17(7), 863–873.
Wolf M.S., Davis T., Osborn C.Y., Skripkauskas S., Bennett C. &
Makoul G. (2007) Literacy, self-efficacy and HIV medication
adherence. Patient Education & Counseling 65, 253–260.
The Journal of Advanced Nursing (JAN) is an international, peer-reviewed, scientific journal. JAN contributes to the advancement of
evidence-based nursing, midwifery and health care by disseminating high quality research and scholarship of contemporary relevance
and with potential to advance knowledge for practice, education, management or policy. JAN publishes research reviews, original
research reports and methodological and theoretical papers.
For further information, please visit JAN on the Wiley Online Library website: www.wileyonlinelibrary.com/journal/jan
Reasons to publish your work in JAN:
• High-impact forum: the world’s most cited nursing journal and with an Impact Factor of 1Æ540 – ranked 9th of 85 in the 2010
Thomson Reuters Journal Citation Report (Social Science – Nursing). JAN has been in the top ten every year for a decade.
• Most read nursing journal in the world: over 3 million articles downloaded online per year and accessible in over 10,000 libraries
worldwide (including over 6,000 in developing countries with free or low cost access).
• Fast and easy online submission: online submission at http://mc.manuscriptcentral.com/jan.
• Positive publishing experience: rapid double-blind peer review with constructive feedback.
• Rapid online publication in five weeks: average time from final manuscript arriving in production to online publication.
• Online Open: the option to pay to make your article freely and openly accessible to non-subscribers upon publication on Wiley
Online Library, as well as the option to deposit the article in your own or your funding agency’s preferred archive (e.g. PubMed).
A.M. Colbert et al.
10 � 2012 Blackwell Publishing Ltd