from boys to men: nurturing your son with hemophilia
TRANSCRIPT
If you have a child with hemophilia, you may have been told toexpect the unexpected. “It was the Wednesday before thewedding,” recalls Mandy, mother of a son with hemophilia,telling a rueful tale of her son’s fall and subsequent bleed. “Itwas the day of the big dinner,” says Allie, who ended up in theER with her two sons. And Jane Smith, whose son fell in Juneand still had a black eye in October, laughs, “It was a no-brainerHalloween costume that year. He was a boxer—baggy shorts,boxing gloves, and a little white terrycloth robe with ‘KidBruiser’ written across the back.”
Bleeding disorders can stop a family in its tracks, scrappingdinner plans and Halloween costumes. More important, thesedisorders often change hopes and expectations for a child.Hemophilia, which affects almost exclusively boys, is notoriousfor overturning our basic concepts of maleness. For a child withhemophilia, masculinity is not just about muscles and tough-ness. Fathers can find this shift in expectations particularly hardto follow, as genetics play a nasty trick: a son with hemophiliais likely to have a father without it. Because of this, families andindividuals struggling with the diagnosis need to understandmaleness, while reassessing stereotypes of masculinity—whatmakes a boy a boy. And boys themselves need to know theyare understood and accepted. A reshaped understanding ofmaleness can fuel strong parental and community models,which will help our boys grow into the men they deserve to be.And while hemophilia may seem overwhelming at first glance,parenting a child with a bleeding disorder is actually quite sim-ple. As Jane’s story shows, sometimes all that’s needed is a ter-rycloth robe, plus the vision and adaptability to see what thatrobe (and the boy inside it) can become.
Being a GuySnips and snails and puppy-dog tails versus sugar and spice and every-thing nice. This childhood rhyme makes a point: Boys and girlsare different. Whether you base your understanding of genderon the rhyme, the playground, or what’s under the diaper, gen-der differences appear physically, emotionally and cognitively.Watch any group of children at play. Chances are, more boysare playing with trucks and trains, and more girls are playing
From Boys to Men:
Newsletter
November 2007 • Vo lume 17 • Issue 4
Parent Empowerment
LA Kelley Communications, Inc.
continued on page 11
inside
Nurturing Your Son with Hemophilia
3 As I See It: Dealing with a Rare Bleeding Disorder4 Inhibitor Insights: Therapies for Chronic Pain5 Project SHARE: A Different Kind of Lease6 Storm Watch: Bush Vetoes Children’s Health Expansion Bill7 Homefront: The Color of Boyhood8 Inspriation: A Real Guy’s View of Life with Hemophilia
10 Transitions: Do As I Say, Not As I Do11 Richard’s Review: The Curse of the Romanovs
BY ZIVA MANN

I CAN’T TELL YOU HOW MUCH I’VE LEARNED FROM PEN. IT’Sone thing to know and purchase the drugs. It’s a whole other ballgame to understand the families and patients. Thank you.
Christopher Lomax, Pharm DDirector, Pharmacy, Nutrition & Therapy ServicesChildren’s Hospital, Los Angeles, California
WHAT ARE THE PROS AND CONS OF USING A CRYO/CUFF®
versus using an ice pack or frozen peas to slow a bleed?Anonymous
Ed. note: In general, cold is a great way to alleviate pain and slow bleed-ing and swelling. Ice must be kept in a cloth to prevent damaging the skin.You can use ice chunks in a towel, a commercial ice pack, or even frozenpeas as you suggest. Benefits of ice include that it’s easy and cheap, andwhen in a towel or bag of peas, it’s somewhat malleable. A Cryo/Cuff is aspecially designed sleeve that allows ice water to flow into it from an elevatedcooler. The benefits are many. Pediatric and adult sizes are available.
Sleeves designed for the ankle, arm, shoulder and knee give the injuredbody part perfectly fitted cooling. Best of all, the Cryo/Cuff compresses theinjured site, which helps restrict further blood flow. Ice packs can’t dothat. Drawbacks? Cryo/Cuffs may or may not be covered by your insur-ance or home care company.
Project SHAREEd. note: Valentin and Stefan, two Romanian boys with hemophilia,attended hemophilia camp in Ireland this summer.
THANK YOU VERY MUCH FOR THE FACTOR VIII THAT YOU
have sent for me and Stefan Apetrei. Thanks to you, wewere able to fully enjoy all the activities, including archery,high ropes and horses. Probably without your support, wecouldn’t have been able to attend. Thank you very much!
Valentin BrabeteRomania
With school back in season, it’s amusingto picture a classroom full of boys,fresh from a summer at the beach or
camp, trying to settle down and focus for hoursa day. But it’s hard to be amused if you don’tunderstand what makes boys tick—and sometimeseven if you do. My mom had five brothers, andI have six; growing up, chaos was a way of lifefor me. Unruly was the rule. When I woke, itwas normal to find snakes in my bedroom, motor-cycle helmets on the kitchen table instead of
flowers, tools in the bathroom, and a half-assembled engine in thedriveway—for months. We never did anything halfheartedly. Weliked to compete, whether climbing a tree or arguing about whichcartoon on Saturday morning was the best. It was also the norm touse short sentences and direct communication (occasionally withfists), and to feel a blessed sense of forgiveness when it came to dis-agreements. But although I was surrounded by boys for my entirechildhood, and I loved to explore, copy and know their ways, Ialso knew instinctively that I was not at all like them—emotionally,socially or mentally. Boys are really different animals than girls.
And what happens when a boy has hemophilia? How does thediagnosis change our perceptions of what a boy is, how a boyacts, and how a boy thinks? What is a boy, anyway? What’s thestereotype, and is there a reason behind it? In this issue of PEN,Ziva Mann explores the nature and nurture of boys, and explainshow to better understand your boy with hemophilia.Understanding a boy’s chemical and physical makeup might justbe the clue to interpreting his emotional and mental makeup.
In Inhibitor Insights, we look at the challenge of chronic pain. And inStorm Watch, we focus on a new House bill that was intended to helppreserve healthcare coverage for millions of underprivilegedchildren. NHF has taken a firm stand on this matter. Have you?
Finally, read about hemophilia in another era. Despite hishemophilia and lack of treatment as a child, Pete Gladd enjoyedhis boyhood to the fullest and grew into a man with deep character.I think Pete’s parents understood well what makes boys tick.
Parent Empowerment Newsletter • November 2007 2
Sher
rell
Portr
ait D
esig
n
LA Kelley Communications
PARENT EMPOWERMENT NEWSLETTER NOVEMBER 2007EDITOR-IN-CHIEF Laureen A. Kelley
CONTRIBUTING WRITERS Paul ClementZiva MannRichard J. Atwood
EDITOR Sara P. EvangelosLAYOUT DESIGNER Tracy Brody
PROJECT SHARESM DIRECTOR Julia Q. LongEXECUTIVE ASSISTANT Zoraida Rosado
PEN is a newsletter for families affected by bleedingdisorders that is produced and edited by a parent of a childwith hemophilia. It is a forum that promotes an activeexchange of information and support among divergent groupsin the national and international hemophilia community.
PEN does not accept advertising and uses brandproduct names and company names pertaining only tonews and education.
All names, addresses, phone numbers and letters areconfidential and are seen only by the PEN editorial staff.PEN publishes information only with written consent. Fullnames will be used unless otherwise specified. PEN isprivately sponsored; sponsors have no rights to production,content or distribution, and no access to files. The viewsexpressed by various contributors to PEN do not necessarilyreflect those of the editor. PEN is in no way a substitute formedical care. Parents who question a particular symptomor treatment should contact a qualified medical specialist.
Articles may be reprinted from PEN only with expresswritten permission and with proper citation. PEN may notbe published, copied, placed on websites, or in any waydistributed without express written permission.
Funding provided through generous grants from our corporate sponsors (page 19)
LA Kelley Communications, Inc.68 East Main Street, Suite 102 • Georgetown, Massachusetts 01833 USA
978-352-7657 • 800-249-7977 • fax: [email protected] • www.kelleycom.com
welcome
inbox
On September 9, 2005, ourbeautiful daughter Emily Nellwas born, weighing eight
pounds, three ounces, and measuring20 inches long. Like most parents, weknew that our new baby would changeour lives; we just didn’t know how much.
On September 12, the joy of wel-coming Emily soon turned to fear andconfusion as she was admitted toSunrise Children’s Hospital, Las Vegas,Nevada, with uncontrolled bleedingfrom her umbilicus and heel-stick sites.A resident sat with me in the ER andsaid, “hemophilia.” I thought, “Thiscannot be happening.” The residentexplained the tests being done to deter-mine which clotting factor Emily wasmissing. We then met with a hematolo-gist, Dr. Jonathan Bernstein. As a phar-macist, I started thinking about factorreplacement products, home healthcare,home infusions—my head was spinning.Because hemophilia is rare in girls, Dr.Bernstein was surprised that Emily hadit. The first test results came back, butEmily did not have hemophilia A or B,which comprise about 95% of all factordeficiencies. Emily was still bleeding.First Dr. Bernstein tried prothrombinpowder—no luck. Then a dose of cryo-precipitate. If this stopped the bleeding,it would narrow the suspected factordeficiencies to von Willebrand factor,fibrinogen and factor XIII. Fortunately,after two doses the bleeding subsided,and our prayers were answered. Wetook Emily home and waited for thefinal test results.
The day of Emily’s diagnosis wassurreal. All I remember are Dr.Bernstein’s first four sentences: “Emilyhas factor I deficiency, afibrinogenemia.It is extremely rare. Probably less thantwenty people in the United States havethis disorder. There is no treatmentavailable right now.” I didn’t hear any-thing else he said that morning. Hiswords echoed in my head.
No treatment? What do we donow? How do we keep her safe? Isshe going to die? Why is this hap-pening? Everyone has these thoughtsand feelings when receiving unex-pected news, but with one difference:When we looked for someone elsewith factor I deficiency, someonewho has been through this, therewas no one. We realized that we werepart of a hemophilia community, butwe felt so totally alone. No factor, notreatment. It would have meant theworld to find someone who faced thesame challenges.
Factor I, also known as fibrinogen,helps platelets stick together. Peoplewith fibrinogen deficiency have a two-foldproblem: both clotting and plateletresponse can be abnormal. Newbornsusually begin bleeding after circumcisions,during head bleeds, or at the umbilicalsite. Soft tissue, mouth or nose bleedsmay happen, as well as easy bruising.
Through experience, we learnedhow to adjust regular activities to pre-vent injury, bruising and bleeds becauseany bruise, cut or scrape can mean acall to or visit to the doctor. Emily canbruise from the slightest touch or fromany repetitive movement.
When Emily was learning to crawl,her knees, shins and wrists were con-stantly black and blue; she adjusted hercrawling style to stay all fours like a catso her knees wouldn’t touch theground. When she started walking, thesoles of her feet bruised and became sopainful that she stopped. With the helpof a physical therapist, we found shock-absorbing foam for her shoes and mole-skin to prevent rubbing so she couldwalk. Sometimes the bruising andswelling in her feet and legs are so badthat when rest, ice and compressiondon’t work, her hematologist prescribespain medication. Emily gets “handprint” bruises under her arms and on herback when she is picked up repeatedly.
She also gets a bruise line on her trunkand hips from the five-point harness ofcar seatbelts. When the bruising is par-ticularly bad, we stay close to home. Wecarry doctor’s letters to explain anybruise or injury. But our bigger worry isthe possible hidden injury missed dur-ing the day when we are trying to letEmily be a normal toddler. I say thesame prayer in my head every night as Ilay her down to sleep: “Please God, lether sleep peacefully and wake up to usin the morning.”
There is hope on the horizon. CSLBehring has begun a study in the UnitedStates with its fibrinogen concentrate,Haemocomplettan P, and althoughEmily is too young to participate, theFDA has granted her special approvalto receive this concentrate as treatment.
As we celebrate Emily’s secondbirthday, we are grateful for every dayand hope for an active, wonderfulfuture. We have met so many coura-geous families in the bleeding disordercommunity, and we’re thankful for theirsupport and friendship. We have yet tomeet anyone with factor I deficiencyand look forward to sharing our storyand experiences.
Alison and her husband John live inLas Vegas, Nevada, where John worksas a registered pharmacist. Alison, alsoa pharmacist, stays at home with theirtwo daughters, Abigail, age four, andEmily, age two. Please feel free tocontact them at [email protected].
Parent Empowerment Newsletter • August 20023 Parent Empowerment Newsletter • November 2007
BY ALISON BARTKO
as I see it
Dealing with a RareBleeding Disorder
Emily Nell Bartko
Bartk
o fa
mily
Chronic pain—lasting sixmonths or longer—is a signifi-cant concern for people with
hemophilia and inhibitors. Clottingfactor concentrates used to treatinhibitors are less effective than thepure factor concentrates that stopbleeds in people without inhibitors. Sofor people with inhibitors, bleeding isprolonged. Prolonged or frequentbleeding into joints causes joint dam-age, ravaging the cartilage. Cartilagedamage may progress until the jointbecomes arthritic. Once arthritis ispresent, pain becomes chronic.Chronic pain often begins as mild,intermittent pain, progressing over theyears to severe, sometimes constantpain. Unfortunately, many youngadults with hemophilia incorrectlybelieve that their chronic pain is dueto an active bleed, so they try repeat-edly and unsuccessfully to treat thepain with factor infusions rather thanpain medication.1
Because chronic pain doesn’trespond to typical over-the-counter(OTC) medications for acute pain,patients need their HTC’s help.Although prescription-only, higher-dose formulations of OTC pain med-ications may control some chronicpain, they have their risks.Acetaminophen (like Tylenol®) and allNSAIDs2 (non-steroidal anti-inflamma-tory drugs like aspirin, ibuprofen andMotrin®) have a dose ceiling. Taking anamount above the dose ceiling signifi-cantly increases the risk of serious side
effects. For example, high doses orlong-term use of acetaminophen maycause liver damage. And long-term useof NSAIDs may cause kidney failureor gastrointestinal bleeding, which canbe life-threatening.
Yet people with hemophilia andinhibitors desperately need pain con-trol. If OTC medications may not con-trol the pain and prescription-strengthNSAIDs carry significant risks, howcan people manage moderate to severechronic pain?
Multi-ModalityMedication TreatmentChronic pain is best managed with acombination of treatments—a “multi-modality” or “multi-disciplinary”approach. Treatments include painmedication, exercise, stress reduction,and a host of other therapies. Varioussurgical interventions can also reduceor eliminate chronic pain.
Medications to treat pain are divid-ed into three groups: (1) non-opioids(NSAIDs and acetaminophen); (2)opioids (narcotics like hydrocodone andmorphine); and (3) adjuvant analgesics(antidepressants and anticonvulsants).In overall pain management, drugswith no direct pain-relieving propertiesmay be used to treat insomnia, anxi-ety, depression and muscle spasms.
Unfortunately, many physicianshave outdated or inaccurate ideasabout opioids and their risks, and may
be afraid to prescribe them to managesevere chronic pain even though theyare highly effective. Media coverage ofnarcotic use and drug addiction canscare people into believing they’llbecome drug addicts if they take opi-oids. Both physicians and patients maymisunderstand the terms tolerance, physi-cal dependence and addiction.
Tolerance means that a drugbecomes less effective the longer youuse it. But if you become tolerized toan opioid, your dose can be increasedto maintain effectiveness. This caneven be repeated several times becauseopioids don’t have a ceiling dose.However, high doses of opioidsincrease the risk of side effects such asconstipation, nausea, drowsiness, andrespiratory depression.
Physical dependence means thatsuddenly stopping or lowering adrug’s dose will cause symptoms ofwithdrawal: sweating, rapid heartrate, nausea, diarrhea, goose bumpsand anxiety. Physical dependencedoesn’t mean the person is addicted;it’s considered a normal reaction toopioids as well as to many otherdrugs. Anyone who takes opioids formore than several days is usually con-sidered dependent. To safely stop anopioid and avoid withdrawal symp-toms, the dosage must be decreasedslowly. When a person is dependenton a drug, suddenly stopping the med-ication can be life-threatening. Alwaysconsult your healthcare professionalbefore stopping any opioid.
BY PAUL CLEMENT
Parent Empowerment Newsletter • November 2007 4
inhibitor insights
continued on page 17
1 Sponsored by Novo Nordisk Inc. and four HTCs, a collaborative study was conducted by Munson Medical Center in Traverse City, Michigan, and Henry Ford Health System in Detroit.Witkop, M; Lambing, A, “Pain Assessment,” Hemaware, May/June 2007; 12 91. To join in a pain study currently underway, results to be published in December 2007, visithttp://www.henryford.com/painstudy 2 NSAIDs should not be taken when a bleed is in progress because they temporarily inhibit platelet adhesion and the formation of a platelet plug(the first step in forming a clot). They may also irritate the stomach lining and cause gastrointestinal bleeding. No one with a bleeding disorder should ever take aspirin for pain relief.
Easing the Pain of Inhibitors:
Therapies for Chronic Pain
second in a two-part series
Inhibitor Insights is a PENcolumn sponsored by
Novo Nordisk, Inc.
Parent Empowerment Newsletter • August 2003Parent Empowerment Newsletter • November 20075
a Project SHARE story
A Different Kind of Lease
BY JULIA QUIGLEY LONG
On October 19, 2006, BeverlyParkinson of Jamaica tele-phoned our office moments
before it closed for the day. She hadjust learned about Project SHAREfrom a friend, and she wanted towaste no time. Her son Kurt neededhelp urgently. Following our instruc-tions, sixteen hours later Kurt’s doctorsent us a fax:
Mr. Parkinson has severe haemophiliaA. He is currently hospitalized at theCornwall Regional Hospital, withsevere intra-abdominal bleeding. Tosuccessfully treat Mr. Parkinson, andtherefore increase his chances of survival,he needs factor VIII concentrates urgently.Currently there is no factor VIIIavailable on the island.
That same day, we shipped morethan 80,000 units of factor VIII toKurt’s doctor. In the days and weeksthat followed, Kurt’s life slowlyreturned to normal.
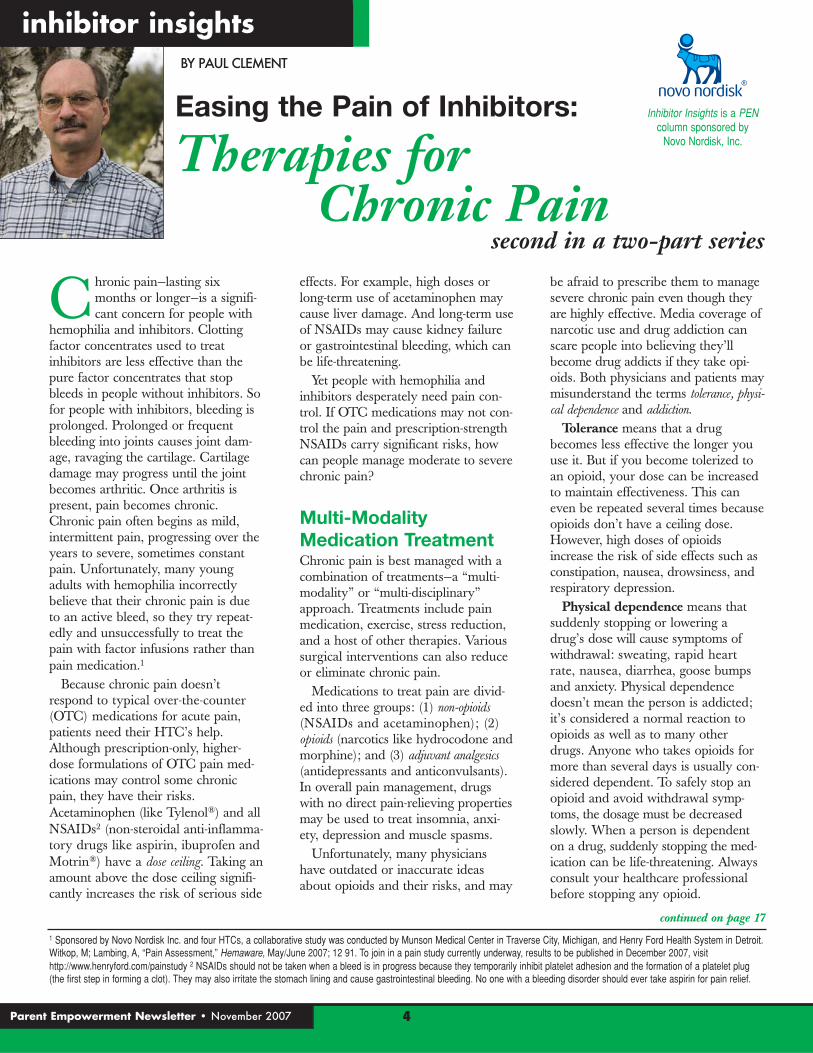
Kurt is a 26-year-old teacher. Histwo brothers, ages 18 and 16, also havehemophilia. Although a mostly inde-pendent young man, Kurt credits hismother for stepping in when he needshelp to ease the pain of a bleed, sched-ule a doctor’s appointment, or arrangeimmediate transport to the hospital.
Without factor, life can be unbearable.“It’s when I am feeling the worst painthat I have suicidal thoughts,” admitsKurt. Before finding Project SHARE,Kurt received factor only once, nineyears ago. A surgeon attempted torelieve pressure from an elbow bleedby cutting into it and “squeezing outthe blood,” without first raising Kurt’sfactor level. This caused additionaldamage and great pain. The next day,another surgeon at another hospitalhad to perform emergency surgery tocorrect the problem—but this time withfactor. The medical bill astoundedKurt and his parents, and it took themmonths to pay.
Kurt raves about Jamaica as “one ofthe best places to live,” with its perfectclimate, diverse geography, and eclec-tic food and culture. With help fromProject SHARE, Kurt’s focus is nowshifting toward his future. He is con-templating important life decisions:When to ask his girlfriend to marry
him? A dedicated teacher, Kurt alsoappreciates the ability to spend moretime in the classroom with his stu-dents. Project SHARE has shippedtwo donations of factor to Kurt andhis brothers since his abdominal bleedlast October, and will try to help thefamily as much as possible.
Beverly thanks and praisesAmericans who donate unused andunwanted factor to Project SHARE.“There is a special blessing stored upfor you somewhere,” she says. “Youhave practically given our sons a newlease on life.”
A future to plan:Kurt Parkinson of Jamaica
New lease on life: Kurt and his mother, Beverly
phot
os: P
arki
nson
fam
ily
To learn more about Project SHARE, please visit www.kelleycom.com/projshare.html
To make a donation of factor or funding to Project SHARE, contact Julia Long, director, at [email protected]
or call (800) 249-7977
Parent Empowerment Newsletter • November 2007 6
storm watch
On October 3, President Bush signed his fourth veto inseven years in office. The veto targeted an expansionof medical coverage under the State Children’s
Health Insurance Program (SCHIP). Both NHF and HFAhad sought to prevent this veto, which can negatively impactfamilies with chronic disorders. In early September, NHFsent an urgent email appeal to all its constituents, asking themto email the White House and persuade Bush to support TheChildren’s Health and Medicare Protection Act (CHAMP, H.R.3162), an expansion of SCHIP. SCHIP is a state/federally fund-ed program that subsidizes healthcare coverage for low-incomefamilies (including 6.7 million children) who earn too much toqualify for Medicaid, but who cannot afford private insurance.The Census Bureau estimates that about 8 million children inthe US lack health insurance.
NHF’s email, titled “Bush Administration Blocks ExpandedHealthcare Coverage for Children: Take Action Now,”1 states:
Prior to going into month-long recesses, both the House andSenate approved bills reauthorizing…SCHIP, and allowing morestates to expand eligibility for the program to more children infamilies above the federal poverty level. However, the BushAdministration, through the federal Center for Medicaid and StateOperations [CMS], has instituted new policies that would severelyrestrict the ability of states to expand the SCHIP program, coveringmore children. In addition, these new restrictions may threatenthe existing coverage that children in many states are alreadyreceiving. NHF has drafted a sample letter to President Bushexpressing disagreement with this action and asking him to rescindit. You can help make a difference by personalizing the letter belowwith your own story and sending it to President Bush today.
NHF states that the Bush administration opposes a SCHIP
expansion “to prevent the SCHIP program from being used as asubstitute for private insurance.” Why did Bush veto H.R. 3162?Is he callous toward the needs of children with health problems,as some have suggested, or is there more to it? Is the expansionbill dead, or is there still hope of resurrecting it? Beyond NHF’swell-intentioned call to action, consumers should know that in-depth reasons exist for the Bush veto; consumers should alsounderstand the in-depth reasons that so many advocacy groupsopposed his veto. This is information that consumers andpatients need to know before they take further action.
Why Bush is Opposed to H.R. 3162The battle is at once about money and ideology. The expan-sion bill would add $35 billion to the SCHIP program overfive years, adding about 5 million people to the 6.6 millionalready registered. Current allocations of federal funds forSCHIP, at $5 billion a year, are not enough for states tomaintain their current programs. According to the Center onBudget and Policy Priorities, unless Congress acts when itreturns from recess, 17 states will have a total of nearly $890million less in federal SCHIP funds than they need in fiscalyear 2007 to maintain their existing SCHIP enrollment.2This means these 17 states will not be able to help all thechildren who need insurance. The expansion bill would seemto help secure funds for a program that is already inadequate-ly funded, according to the bill’s supporters.
Ideologically, President Bush denounces H.R. 3162 as astep toward “the goal of government-run healthcare for everyAmerican.”3 Expansion, he feels, would encourage families toabandon private insurance in favor of state or federally fund-ed insurance, putting more strain on federal budgets andencouraging socialized medicine.
Cheryl Smith and Robert E. Moffit, PhD, of conservativethink tank The Heritage Foundation, agree with Bush. Theybelieve that H.R. 3162 greatly expands millions of Americans’dependency on government healthcare, undermines privatehealth plans, reduces choice for Medicare beneficiaries, andsaddles taxpayers with a permanent new entitlement. Accordingto the Congressional Budget Office (CBO), the bill wouldmove nearly 1.9 million people off private insurance andonto taxpayer-supported healthcare.
1 http://gomembers-ecommunicator.com/campaign/ProtectSCHIP 2 The 17 states anticipating FY 2007 funding shortfalls: Alaska, Georgia, Illinois, Iowa, Louisiana, Maine, Maryland,Massachusetts, Minnesota, Mississippi, Missouri, Nebraska, New Jersey, North Carolina, North Dakota, Rhode Island, South Dakota, and tentatively Wisconsin. 3 Pear, Robert and Hulse,Carl, “Congress Set for Veto Fight on Child.” New York Times, September 25, 2007.
BY LAURIE KELLEY Bush Vetoes Children’s Health Expansion Bill: NHF and HFA RequestAction From You Now
continued on page 18

Recently I had my fourth pedicure. Ever. Delighted, Ispent way too much time admiring my toes, andeventually Shai noticed. “Mum,” he said, “your feet
are beautiful.” I looked at my awestruck son, and smiled.“Thanks, hon.” He looked up at me, his eyes wide with anidea. “Could you make my feet beautiful, too?”
One of the challenges of living with hemophilia is definingwhat it means to be male, and responding to the equationthat male = tough. This is the right challenge for Shai’sgeneration, as concepts of manhood are reshaping themselvesfrom physical toughness into a sense of responsibility, familialinvolvement, and advocacy for the child, the family, the indi-vidual. Recently I came across a magazine photo of actorKevin Sorbo being tackled by one of his sons. In a late 1990sTV show, Sorbo played Hercules, the strongest man in theworld; but this photo didn’t show the tough-guy look.Muscles felled by love? Or muscles reprioritized? Physicalstrength made secondary to love, family and home? It’s aromantic picture, and a romantic thought.
It seems that while the boundary between guy stuff andgirl stuff is glaringly obvious to grownups, the distinction isless clear to children. One day I arrived at Shai’s classroom tofind him playing “Fireman Rescue” with three of the moreboisterous boys. They had commandeered the top of theclassroom climbing structure as their firehouse, and set look-outs to spot imaginary fires. Then, they’d rush out and putout the flames.
In between emergencies, the boys lined up to show metheir gear. They had a motley collection of helmets and con-
trived hoses. Best of all, each boysported a pair of evening gloves and ahandbag. “These are our fire helmets,”they explained, “our fire hoses andour fire gloves.” “And the bags?” I asked. “Those are for car-rying the things we need,” they said, “so that we can be pre-pared.” A bag-wearer myself, I could only agree.
It is my fiercely held opinion that gender is what youmake of it. Sure, more often boys tend to be rough-and-tum-ble—mine does!—and more often girls pretend to be princess-es. But that doesn’t mean that a rough-and-tumble boy can’talso be caring and sensitive to the needs of others. Our Xand Y chromosomes don’t lock us into simple, gender-basedroles. Biology determines some of what we are; but our envi-ronment, our brains, our hearts and our choices determinethe rest.
Any mother who has advocated for her child knows thatfemininity doesn’t have to be weak or yielding, or imitate adoormat. And masculinity doesn’t have to be muscular,uncaring and steely. Hemophilia forces us to rethink thesestereotypes. It requires our boys to look for manhood insomething other than a football field. Hemophilia teachesparents to express compassion and advocacy in a way thatcrosses princess and fireman gender roles. Mama bear canroar, and papa bear can offer a hug.
So what about those so-beautiful toes? I was prepared toteach Shai that as a boy—as a human—he can be anything hewants, with or without beautiful toes. And I trusted my hus-band to model compassion and offer non-macho images of aman worthy of respect. As usual, I had a plan. And, as usual,I probably didn’t need it. Right now, the shaping of genderidentity is a non-issue, even unimportant. According to Shai,a pair of evening gloves can be princess-delicate on one set ofhands, and fireproof on a different set of hands. When I askedabout this, Shai shrugged. “They’re just gloves,” he said.
I chewed this over for a while. Then one day, when I cameto pick up Shai, I saw one of the former firemen wearing aBoston Red Sox shirt. Well, we live in Red Sox Nation, so nosurprise there. The shirt, however, was pink. I couldn’t helpmyself, and I asked the kid about it.
“I like the Red Sox,” he informed me. (Stupid adult.) Thestupid adult nodded and asked, “What about the color?” Thekid looked down. Then, scornfully, he said, “Well, it’s pretty.”Ah. Well, and so it is.
The Color ofBoyhood
BY ZIVA MANN
7 Parent Empowerment Newsletter • November 2007
homefront
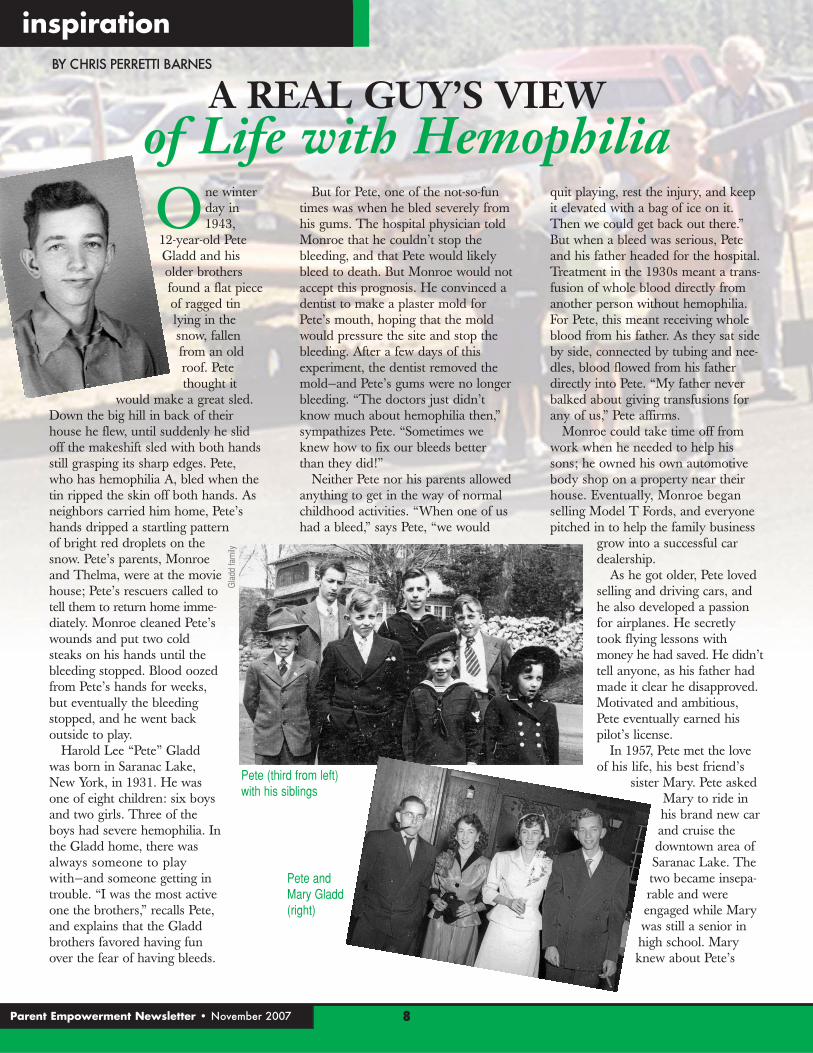
One winterday in1943,
12-year-old PeteGladd and hisolder brothersfound a flat pieceof ragged tinlying in thesnow, fallenfrom an oldroof. Petethought it
would make a great sled.Down the big hill in back of theirhouse he flew, until suddenly he slidoff the makeshift sled with both handsstill grasping its sharp edges. Pete,who has hemophilia A, bled when thetin ripped the skin off both hands. Asneighbors carried him home, Pete’shands dripped a startling pattern of bright red droplets on thesnow. Pete’s parents, Monroeand Thelma, were at the moviehouse; Pete’s rescuers called totell them to return home imme-diately. Monroe cleaned Pete’swounds and put two coldsteaks on his hands until thebleeding stopped. Blood oozedfrom Pete’s hands for weeks,but eventually the bleedingstopped, and he went back outside to play.
Harold Lee “Pete” Gladdwas born in Saranac Lake,New York, in 1931. He wasone of eight children: six boysand two girls. Three of theboys had severe hemophilia. Inthe Gladd home, there wasalways someone to playwith—and someone getting introuble. “I was the most activeone the brothers,” recalls Pete,and explains that the Gladdbrothers favored having fun over the fear of having bleeds.
But for Pete, one of the not-so-funtimes was when he bled severely fromhis gums. The hospital physician toldMonroe that he couldn’t stop thebleeding, and that Pete would likelybleed to death. But Monroe would notaccept this prognosis. He convinced adentist to make a plaster mold forPete’s mouth, hoping that the moldwould pressure the site and stop thebleeding. After a few days of thisexperiment, the dentist removed themold—and Pete’s gums were no longerbleeding. “The doctors just didn’tknow much about hemophilia then,”sympathizes Pete. “Sometimes weknew how to fix our bleeds betterthan they did!”
Neither Pete nor his parents allowedanything to get in the way of normalchildhood activities. “When one of ushad a bleed,” says Pete, “we would
quit playing, rest the injury, and keepit elevated with a bag of ice on it.Then we could get back out there.”But when a bleed was serious, Peteand his father headed for the hospital.Treatment in the 1930s meant a trans-fusion of whole blood directly fromanother person without hemophilia.For Pete, this meant receiving wholeblood from his father. As they sat sideby side, connected by tubing and nee-dles, blood flowed from his fatherdirectly into Pete. “My father neverbalked about giving transfusions forany of us,” Pete affirms.
Monroe could take time off fromwork when he needed to help hissons; he owned his own automotivebody shop on a property near theirhouse. Eventually, Monroe beganselling Model T Fords, and everyonepitched in to help the family business
grow into a successful cardealership.
As he got older, Pete lovedselling and driving cars, andhe also developed a passionfor airplanes. He secretlytook flying lessons withmoney he had saved. He didn’ttell anyone, as his father hadmade it clear he disapproved.Motivated and ambitious,Pete eventually earned hispilot’s license.
In 1957, Pete met the loveof his life, his best friend’s
sister Mary. Pete askedMary to ride inhis brand new carand cruise thedowntown area ofSaranac Lake. Thetwo became insepa-rable and wereengaged while Marywas still a senior inhigh school. Maryknew about Pete’s
8Parent Empowerment Newsletter • November 2007
inspirationBY CHRIS PERRETTI BARNES
Gla
dd fa
mily
A REAL GUY’S VIEWof Life with Hemophilia
Pete (third from left)with his siblings
Pete and Mary Gladd (right)

bleeding disorder before they gotmarried, and she knew Pete’s routinefor treating a bleed. Pete recalls,“Mary got used to me icing my bodyparts. I always worked hard andsometimes had bleeding from thelong hours. But I was the breadwinnerand had responsibilities.”
The newlyweds, just 27 and 17, weresoon thrown into a challenging situa-tion. Pete was struck by polio, whichseverely damaged his right leg. Hespent eight months bedridden, with nofamily income. This was devastatingto a proud, active young man. Peteasked a doctor to fashion a brace sohe could go out and find work.Although the doctor advised using thebrace only sparingly, Pete went out jobhunting the very next day.
Pete became a successful car sales-man. With his savings and the help ofa loan, he bought six cars and openedhis own showroom. Pete purposelysold cars to people who desperately
needed them. He thoughtthat even an underdog, whohad difficulty obtaining aloan, deserved to have a car.“I was always an honestbusinessman and believedeveryone deserved a breaknow and then.”
When Pete and Marystarted their own family, theyknew that any daughterswould be carriers of hemo-philia. Their first child andonly son, Peter, was born in1959. The next three chil-dren were daughters Shellie,Lisa and Velvet. Each daugh-ter eventually gave birth to aboy with hemophilia:
Shellie’s second child; both of Lisa’ssons; and Velvet’s only son. Despite acarrier’s 50% chance of having a boywithout hemophilia, says Pete, “In thisfamily [those odds] went right downthe tubes!” He smiles and adds, “Ah,they’ll be okay…Treating hemophiliais much better now than when I wasgrowing up. They’re all healthy andstrong and really good kids.”
With a mischievous gleam in hiseye, Pete continues, “These boys aremy flesh and blood. I wish they didn’thave hemophilia like me, but I have alot to teach them about being whothey are, who they are meant to be,and having fun.” He appreciates thattoday, his grandsons have excellenttreatment for their hemophilia. And itappears that the boys inherited notonly a hemophilia gene, but an“adventure” gene. Each grandsonseems to want have as much fun aspossible, to constantly be aroundPapa, and to fly in his airplane. Velvetsays of her son, Nick, “You just can’t
separate them. They love beingtogether, and Nick acts just like myfather. It’s scary sometimes!”
Now 76, Pete remains spry andactive. He flies his own Forney F1Aircoupe. He bought his first planewhen he was 36 and has been flyingfor 50 years. Pete’s words sum up hisperspective on life with hemophilia: “Inever let my bleeding disorder get inmy way of working hard and havingfun.”
When asked for his advice to youngparents raising children with hemo-philia, Pete answers adamantly, “Don’tkeep ‘em in a bubble. They’ll learn ontheir own, through difficult experi-ences, making mistakes, and learningfrom them. You just have to trust ‘em.My parents let me be me with all myexperiences, both good and bad, andboy, I had a lot of fun in my life…awhole lot of fun!”
Chris Perretti Barnes is the mother of Casey, age seven, and Bennett, age five, who has severe hemophilia A.She is the director of PatientEducation for BioRx, a home healthcare company. She is theauthor of the children’s book The Great Inhibinator. Chris lives with her sons and husband, Matt, in Chapel Hill, North Carolina.
To learn more about life withhemophilia in the mid-twentieth
century, readLegacy: TheHemophilia ofYesterday. Told mainly through period diary entries, Matthew DeanBarkdull’s biography of
his grandfather, Ralph Dean Rytting, is the inspirational account of a teenagergrowing up with hemophilia duringWorld War II. To order your copy,contact LA Kelley Communications at www.kelleycom.com.
Pete and Mary (far left and right) with their grown children: Peter, Shellie, Lisa and Velvet.
At 76, Pete still enjoystaking his grandchildrenflying in his ForneyAircoupe.
9 Parent Empowerment Newsletter • November 2007

Even when we have the best inten-tions, as mothers, our hearts some-times lead us to act differently than
our minds tell us. I have a son with hemo-philia. He is 23 years old now, and we arestill having a hard time with transitioning.We both know that he should be independ-ent and not need me anymore, but ourhearts are having trouble letting go of ourold patterns. Why? Looking back, I recog-
nize the steps I needed to take—but didn’t—to encourage myson to grow into a healthy, independent young man.
We have no history of hemophilia in our family, so whenmy son was diagnosed, my husband read everything aboutthe disorder. One thing stuck in my mind: Hemophilia isgenetic, passed from mother to son. Oh great, this was my fault,I thought. While my husband read and reported to me all thefacts about hemophilia, I sat next to my baby and apologizedfor giving him hemophilia. After several months and our firstvisit to the hemophilia treatment center, I made a pact withmyself that I would do everything in my power to keep mybaby from getting hurt. It didn’t take me long to realize thatthis wasn’t going to happen.
No matter how hard I tried, injuries happened, and I couldn’tmake them better. That is, until home infusion entered ourlives. Finally, I could do something. I had the power to makehis injuries better. I could help my son.
As he got older and went off to camp, he learned to self-infuse. He received awards for successful infusions andreturned home proud of his newfound independence. Yetwithin a couple of weeks, we would be right back in ourroutine: I did his infusions. Prior to his high school overnighttrips, I made him self-infuse a couple of times to ensure thathe could do it, and then I let him go. After the trips? Rightback to our routine.
Why was this so hard? Why couldn’t my son just continueself-infusing without my interference? He certainly was nolonger a child.
I had become the mother that I swore I never would be.When my son was ten, I heard other moms talking aboutordering factor for their 30-year-old sons and still infusingthem. Not me. I was never going to be that mom. I was goingto be like the moms of those 12-year-old boys I’d met whoalways infused themselves once they’d learned. Where did Ifall short? Did I not want to let go—or did my son not want tobecome independent?
What we developed is called “enmeshment” in family-dynamicterms; both my son and I gained some pleasure from ourmutually dependent relationship. My son sensed the comfort itgave me to be able to care for him. He wanted me to feelneeded. I am a caretaker by nature, and I felt I was caring for
my “sick” son. But my son wasn’t sick. And evidently, he isalso a caretaker by nature. To this day, he calls to tell mewhen he’s having a bleed because he thinks I will be upset if Idon’t know.
My son never wanted to exclude me from his life. We werevery close, and we remain so. This could be due in part to agedifferences in our family. Although he has two older siblings, myson was like an only child growing up, since his closest siblingis 11 years older. I took my young son everywhere with me.
He also remained my dependent child, and this is emotion-ally unhealthy for a young man embarking in the world. I did-n’t allow him to transition; I didn’t suppress my maternalinstinct to take care of him. I didn’t work through my ownguilt about “giving” this disorder to him. I could have, andshould have, fostered his independence little by little by turninghis care over to him beginning at an early age. Transitioningshould begin as soon as a child is capable of handling smalltasks. Let him wipe his skin with alcohol swabs, and let himchoose a bandage. Allow him to push the factor in throughthe syringe. When he’s 11 or 12 and has been taught toinfuse, don’t infuse him when he asks, even late at night orearly in the morning. Teach him that it’s his body, his life.
Now I am trying to foster my son’s independence. I tell himit’s okay if he doesn’t call me when he has a bleed, unless it issomething very serious. I try not to ask him about bleeds orinfusions whenever I call him. We are working very hard togetheron this. And I think we’re getting healthier all the time.
transitionsBY NANCY PHELPS
10Parent Empowerment Newsletter • November 2007
Do As I Say, Not As I Do
Phelps family

with dolls. What makes boys tend to focus on physics(all things that go zoom) while girls focus on the socialsciences?
To explain this, Michael Gurian, author of Boys andGirls Learn Differently! offers an array of charts and listsof sex-based differences. These boil down to two facts:(1) If you look at the anatomy and chemistry of thebrain and body, you’ll see that boys and girls are builtdifferently. (2) Boys and girls develop differently. As aresult, their brains and bodies are geared toward differ-ing innate strengths and weaknesses. Girls tend tospeak and read earlier than boys, and girls maturefaster emotionally. By contrast, boys are slower todevelop as communicators but are more prepared tolearn through physical activity and risk-taking—as inthe physics play. As girls develop faster both sociallyand linguistically, they are pulled to explore the worldof those skills. So it’s biology that leads the boys totrucks and trains and the girls to social play, right?
Well, maybe. Gurian’s charts show an impressivelist of differences, and seem to imply that biologicalgender difference is inarguable. Boys must be differentfrom girls—biology says so. But even biology canchange. Specialists who work with people with dyslex-ia, learning disabilities, and strokes emphasize that thebrain can usually figure out an alternative neurologicalpathway to its goal. It can adapt. This means that boyscan learn to be social, and girls can choose to go zoom.
A study of workplace environment conducted byRobin J. Ely, a professor at Harvard University,shows how the toughest of males can adapt. Menworking on an oil rig talked openly about their feel-ings and admitted uncertainty or anxiety about theirwork.1 Until recently, these guys had been thetoughest of the tough, the super-macho. Why thechange? Their company had encouraged emotionalopenness as a way of recognizing and resolvingpotential safety issues. And it worked well. The meneven talked about problems they were having at home,saying, “If you would please keep me focused andunderstand if I’m a little distracted, I’d appreciate it.”
From Boys to Men... continued from cover
1 Harvard Magazine, September-October 2007.
11 Parent Empowerment Newsletter • November 2007
BY RICHARD J. ATWOOD
richard’s review
The Curse of the Romanovs
Staton Rabin, 2007New York, NY: Margaret K. McElderry BooksJuvenile fiction, 273 pages
From 1912 until 1918, the young Russian prince AlexeiNikolaevich Romanov writes a diary about his struggleswith hemophilia, while his royal family struggles withinternational war and domestic revolution. The Curse ofthe Romanovs, a novel for ages 12 and older by StatonRabin, concerns Alexei’s fictional diary, which he hidesfor his tutor to find and save for posterity.
Brought in to treat the bleeding, Father GrigoryRasputin can reportedly stop hemorrhages and painwith his eyes and by laying on his hands—or by hypno-tism, prayer, or séances—and his power is considereddangerous. Alexei participates in a failed assassinationattempt on Rasputin in 1916, and must escape to savehis own life. Using the mental visualization techniquesRasputin taught him, 12-year-old Alexei time-travelsalong a river of blood to New York City in the year2010. Here, Alexei is saved by Varda Ethel Rosenberg,his 15-year-old distant Jewish cousin and the daughter ofa man with hemophilia who died of AIDS. To avoid thewrath of Rasputin, who has also conveniently traveledto New York, the cousins return on the river of blood to1918 St. Petersburg, knowing that the Bolsheviks plan toassassinate the royal family.
This story of Alexei and his hemophilia hardlyrequires a wildly fictional account of time travel tomake it interesting, because the true story is captivatingenough. Rabin does include some accurate information.Besides Rasputin’s mystical treatments, for example,Alexei receives mud baths for a hip bleed; rags and icefollowed by cauterization for a nose bleed; and an infu-sion of factor VIII concentrate for a knee bleed whenhe is in the future New York City. Alexei’s dog “Joy” isaccurately mentioned.
Possibly anticipating criticism of her distortions ofhemophilia history, Rabin wisely includes an explana-tion of how she altered the biographies of the realRomanov family for this work of fiction. She thanksNeil Frick and Dr. Ann-Marie Nazzaro, both currentemployees of National Hemophilia Foundation, for theirassistance. And fortunately, Rabin also includes a seriesof notes on hemophilia history and facts, including thehelpful title “Historical Notes (What’s True, What’sNot).” While these 24 pages of notes are worth reading,the rest of the book can be easily avoided.
Novelist Staton Rabin, who is also a screenwriter, lives inIrvington, New York.
Astonished, Ely asked her colleagues, “Where’s the mas-culinity?” Maybe a better question would be, “How didmacho evolve?”
Starting Over: How to Be a Guy Who Bleeds In the case of Ely’s oil riggers, opportunity combined with aneed for safety to effect change. Similarly, for families dealingwith hemophilia, the diagnosis provides both opportunityand the need for change. Parents find themselves rethinkingtheir ideas about who and what their boy with hemophiliawill be. In doing so, they have to reconsider what they valuein a man or boy. Can you be proud of a boy who doesn’tplay football? What if he’s a swimmer instead? Or plays cut-ting-edge guitar? This is the challenge for new parents of achild with a bleeding disorder: to learn about hemophilia,adapt their expectations, and still find pride in the midst ofall the newness. Simply put, parents must learn to let theirboy be a normal boy—on his own terms. But how?
The first and sim-plest step is to offer arole model. DanKindlon,Massachusetts psy-chologist and authorspecializing in boys,notes that boys lookto their fathers fortheir core ideas ofmasculinity andcodes of behavior. Inresponse, manyfathers try to be theUltimate Guy: neverwrong, always strongand capable, protect-ing the family fromharm. This super-hero-style parentingcan be a reflex in
fathers confronted with a major medical diagnosis. They justwant to fix it and make things right. They are responding totheir sons’ challenges, offering safety and absolute paternalcertainty. It’s a well-meaning gesture, but a flawed one. Theproblem with the super-dad model, observes Kindlon and co-author Michael Thompson2, is that it’s unattainable. It’s animpossible model for any father to maintain, and an impossiblemodel for any son (with or without hemophilia) to live up to.
“Men are afraid,” explains Kindlon, “and they can’t admitthey’re afraid…Men still feel like they have to be invulnera-ble, know everything, be good at everything.”3 This façade ofinvulnerability protects them emotionally, pushing awaydoubts and fears. But when confronted with a major diagno-sis and no real understanding of the implications for theirchild, it’s easy for fathers to get overwhelmed, even step
away from their sons. Frustrated mothers may push fathersto change; but, warns Kindlon, “You can’t push too hard orthey’ll get defensive and run away.” Instead, fathers can bewon over by the promise of what Laurie Kelley calls a tribe,or a community.4
In the bleeding disorder community, both fathers andsons have the opportunity to feel normal, or average, and totalk comfortably with people who share their experiences.Some fathers in the Boston area, for example, go out togetherfor an informal dads’ night out, while others attend father-sonevents like Dads in Action.5 Still others meet at family campsand NHF or HFA events, where dads swap war stories—aboutadvocacy in the ER, completing factor logs, identifying bleedingpatterns—while the boys learn coping skills and build friendships.The tribe offers a chance for fathers to compare notes andwatch more experienced dads handle parenting their children.Sons can watch other boys with bleeding disorders, develop-ing a network of “blood brothers.” The tribe builds slowly,
2 Dan Kinlon and Michael Thompson, Raising Cain. Ballantine Books. 3 Personal communication, Sept. 11, 2007. 4 Laureen Kelley, Raising a Child With Hemophilia. Centeon, LLC. 5 For more information, contact Hemophilia Federation of America, www.hemophiliafed.org
12Parent Empowerment Newsletter • November 2007
Knights and Superheroes: Ten-year-old Alex Mueller’s supercharged view of battling hemophilia.
Alex
Mue
ller
Psychologist Dan Kindlon advises fathersto be Real Guys, not super-dads.
Dan
Kin
dlon

13 Parent Empowerment Newsletter • November 2007
based on friendship and a shared issue; and with it comes adifferent kind of model than the macho tough guy. Instead, itoffers something quieter, less dramatic, closer to…normal.
Boys in Motion: The Need to WiggleWhen you form a tribe, you give each boy access to aworld where he is the norm. He joins his blood brotherslearning to infuse at camp. He celebrates his bleeding disor-der milestones with boys who understand their significance.At home, he watches his parents advocate for him, and hesees his father learn to relate to him on his terms. It’sheady, wonderful stuff—and it has to be. This sense ofpride, confidence and normalcy is challenged when a boyleaves the tribe and family to attend school—a place with itsown hurdles to jump.
Many schools are badly built for boys. Or perhaps boysaren’t well designed for the traditional school. “Being aroundboys is like observing a miniature tornado,” writes authorRobin Bradford. “Their bodies and minds are forces of ener-gy taking in information, spinning it into something new, andspitting it back out before roaring on.”6 A wiggling, restlessboy may be trying to learn, process stress, or deal with emo-tion. You might even say that he has to wiggle. “Engaging thewhole body in the task of emotional processing seems toenhance neurotransmission to limbic (emotional) and left-brain (verbal) areas,” Gurian theorizes.7 This means that aboy wiggling in his seat may be learning, or he may be wor-rying about a bleed or perhaps thinking about an argumenthe had with someone. To sort it all out, he might need towalk up and down, squeeze a stress ball to help him think, orbe sent on an errand by the teacher. But if the classroomcan’t find a way to channel his functional energy, the wrig-gling boy will become disruptive and unhappy.
It’s a warning echoed by Kindlon and Thompson, whonote that schools designed to accommodate boys’ energy andlearning style see happier, better-adjusted and higher-achiev-ing boys, along with less violence and behavior problems.But this kind of accommodation requires big adjustments inteaching style to accept boyish bounce. Such adjustments arecrucial in the early years of formal education, according toKindlon and Thompson, as boys are less developmentallyprepared than girls for the classroom. Neurologically, girlsare more prepared to read in kindergarten and first grade,and better able to sit quietly and focus during the early yearsof school. Boys are slower to make the transition from thehigh-energy, loosely-structured world of preschool andkindergarten. A teacher struggling with boyish energy maynot be able to teach a boy to read, but unfortunately, mayteach him that he’s failed to learn. The risks are obvious. Ifboys are less prepared to learn than girls, they may learnone, clear lesson: that their role is to be disruptive ratherthan to learn.
School, with its structure and demand for conformity (orat least cooperation), can hit hard at the positive models aboy with hemophilia finds in the bleeding disorder communi-ty. While he may be a hero for self-infusing in his tribe, inhis classroom he might be the kid who never gets the mathproblem right, or the one who always wiggles. So along withhis community, he’s going to need resilience.
Outside of School: Stress and ResilienceThe current generation of children, experts say, is over-programmed. Recess time is disappearing, and after-schoolactivities are increasing. Rates of attention deficit disorders(ADD/ADHD) are soaring, as are learning disorders. Bothare signs of stressed brains, says Gurian, with boys morelikely than girls to be diagnosed with these conditions. Andchildren with hemophilia are showing signs of stress morefrequently than their peers. One study8 showed that the
6 Andrea Buchanan, ed., It’s a Boy: Women Writers on Raising Sons. Seal Press. 7 Michael Gurian, Boys and Girls Learn Differently! Jossey-Bass. 8 Mayes, Handford, Schaefer, Scogno,Neagley, Michael-Good and Pelco, Journal of Genetic Psychology, 1996 June; 157(2):137-51.
14Parent Empowerment Newsletter • November 2007
rates of boys with hemophiliadiagnosed with ADD/ADHDare higher than those of theirclotting peers. Higher, too, thanin the general population arethe rates of gifted childrenwith hemophilia. Stress pusheschildren hard, and the resultsare mixed.
Unfortunately, in additionto feeling increased stress, thecurrent generation of children isalso considered less resilientthan previous generations.Experts say that our kids are less inclined to think ofthemselves as problem solvers.Causes for this are many.Modern toys, for example,invite passivity and push-buttons. Instead of figuringout what he can do with a toy,a child is now likely to askwhat the toy can do for him. Aset of plain blocks, on the otherhand, doesn’t entertain him,but challenges him to be imag-inative and creative, to figureout what works—and to rethinkhis construction when the towercomes tumbling down. Thefalling tower of blocks takes onnew significance when youimagine it as your child’s body,stopped in its tracks by a bleed.Or as a teenager on prophylax-is, casually aware of his diagno-sis until a nasty bleed provesthat he is vulnerable. Reality hits hard,and it demands resilience. Achild with a chronic conditionwho cannot regroup and tryagain, who accepts his failureas final, is a child in trouble. For children with bleeding disorders, resilience is not an option. It’s a necessity.
You can approach resiliencein two ways. Either it’s the innate, instinctive quality of a toddler who falls down, gets up, and keeps figuring out howto walk. Or it’s something that children need to learn. Intruth, both innate and learned resilience are essential. Partof resilience is problem solving and practice: learning tolook for alternative ways to build that tower of blocks;learning to think about your resources and figure outwhich friends will help you with your crutches. And part of
resilience is trusting your innate ability to find a solution to aproblem: believing that there’s something you can do when asituation seems overwhelming.
Children with a sense of their own inner resources, andwith faith in their ability to solve problems, says Kindlon, aremore likely to be resilient in the face of adversity. And thatresilience is even more crucial in a chronic condition withphysical and social implications. How do you handle going toschool with crutches for the first time? Will you stay at homeon Halloween, or will you learn to make a joke out of thatblack eye? Both parent and child may need to express angeror frustration over the situation, but they also need to be ableto figure out what to do to move forward.
Mapping the New EmotionalLandscape Most people approach problem solving rationally, by definingthe problem, then setting goals and developing a strategy toachieve them. This works fine when you’re dealing with atower of blocks, but when emotions are the problem, boysespecially can run into trouble. Do they even recognize whatthey are feeling?
If your idea of masculinity isn’t a guy who admits he’sworried or scared, then you’ll be as puzzled as Robin Ely wasover her emotionally honest oil riggers. But if your child has ableeding disorder and you’re rethinking your ideas of male-ness, those oil riggers can be fantastic role models. Probablymore than other children, boys with bleeding disorders needto understand their feelings, with so much emotional inputcoming straight at them—more highs (that first self-infusion!)and more lows (that big bleed). More than their peers, theseboys need to push away the kind of cultural training that pro-duces the classic, insensitive guy. With help from parents andthe tribe, and with role models that balance masculinity with

15 Parent Empowerment Newsletter • November 2007
emotional literacy, boys can learn to understand their feelingsand discover what to do about them. For example, a boycould punch something when he’s angry. Or he could learn torecognize and name the anger, and then work it off, finding asolution to the problem. Boys can learn what to do with theiranger, frustration and sadness, but it may go against the grainfor some parents to teach boys this skill.
Parents may hesitate because they know something theirboys don’t: Learning emotional skills is only the start. It’sjust as important to learn to use these new skills in a culturethat’s more comfortable with the tough, unemotional guythan the thinking, feeling guy. Being aware of feelings, andunderstanding the inner emotional landscape, is anotherthing that can make our boys different—and it’s hard, hard,hard to be different. But being different is not a choice thatboys with hemophilia get to make. Their choice is how theywant to handle their differences, and how to find the strengthand skills to make difference into a good thing.
Again, parents play a crucial role. Parents of children witha bleeding disorder may not share the condition, but theyhave their own challenges. It helps immensely to show chil-dren our challenges as parents, and let them see how the bigguys—and gals—do it. A child might hear his parents calmlydiscussing tough issues. He might see a man communicatewith a woman, showing her respect. In even the smallest con-versations, parents can offer an example of men and womentalking, expressing feelings and concerns, and workingtogether toward goals and solutions. Watching their parentswork through difficulties, children learn how it’s done; and
they feel less alone, less unique in their challenges.But children want to do more than just copy mom or dad.
They want to understand their parents’ choices and and val-ues, and learn how to apply them in the world. Boys look totheir parents for examples of how to behave and how differentthey can afford to be outside of the tribe, but they must alsolook to themselves. Can they pull off being different? Yes,but they’ll need to figure out how. Given the opportunity,children will bring their problems to people they trust, andbegin to talk through their concerns and hopes. By offeringchildren chances to talk, parents forge lines of communica-tion that start by educating and end by supporting.
“Develop rituals,” Kindlon advises. “Figure out somethingyou [and the child] both have fun doing—whether it’s pingpong, video games—find it and do it once a week.”9 Ritualsbecome the opportunity for parent and child to connect; theycreate comfortable, relaxed environments where the parentisn’t doing dishes or folding laundry or paying bills. Onemother describes a regular spa night, when she and herdaughter paint their nails and talk quietly—sometimes aboutskin creams, sometimes about life.10 Or the ritual might be afather and son playing a Sunday morning ping-pong game.Now, mix it up: a mom playing catch with her son, a daugh-ter visiting the museum with her dad. In choosing a ritual, ithelps to remember that many boys communicate betterthrough shared experiences and often prefer to talk side-by-side with another person. It’s really the first lesson of hemo-philia: Adapt to your child’s need, not to your preference.
One day, says Kindlon, that ping-pong game will turn intoa long conversation about hopes for the future or worriesabout the school bully. With luck, the son will see his parentas an honest, trustworthy person who helps and listens. Witheven more luck, he will ask for guidance—and trust himself tocome up with the ultimate answer.
The Good EggsSo boys will be boys. Some boys will be the kinds of boys wenever expected: non-clotting, needle-using, active and won-derful. Some will be classic rough-and-tumble boys, alwaysmuddy and loud. Some will be both. Inevitably, boys withbleeding disorders, like other boys, will confound the stereo-types of what is male. They will change our ideas aboutwhat’s normal, what’s good, strong or healthy. By being dif-ferent, bleeding disorder boys shake up our preconceptionsof boyhood, making us rethink.
In her book on the nature of women, Natalie Angierwrites poetically about apoptosis, or the cellular suicide of theimperfect egg-sperm combination. If a bad egg meets a badsperm, they do not create a fetus and are triggered to simplydie. It’s a rather vicious but practical bit of natural engineer-ing, and it’s all the more compelling in the bleeding disordercommunity of the imperfect, the nearly average, the almostnormal. Are our non-clotting boys bad eggs or good ones?“Through cell suicide,” Angier writes, “we at last get to yes—arare word. We are all yeses. We are worthy enough, we passinspection, we survived. We are good eggs, every one ofus.”11 It’s something worth thinking about. Our boys, with
9 Personal communication, September 11, 2007. 10 Mothering, September-October 2007. 11 Natalie Angier, Woman: An Intimate Geography. Anchor Books.
16Parent Empowerment Newsletter • November 2007
• Create rituals that presentopportunities for open lines ofcommunication, especially one-on-one. Boys prefer side-by-sideinteraction and activity, so look fora task you can accomplish jointlyor an experience you can share.
• Offer models that your child canrealistically live up to. Let him seeyou struggle, tackle and solveproblems. Let him see you admitto mistakes. Openly recognizepositive and negative emotions.Show him that masculinity isn’tabout being tough as nails oralways having the right answer.
• Show your child that you valuehim, and not because he is perfector excels at something. Showyour support for the person he is.
• Volunteer at your child’s school.Show him you are investing yourtime, and that school is importantto you. Use your involvement toevaluate the school: Is the artsprogram failing? Do they need aparent to coach the baseballteam? Step up or find a volunteer.
Work with the administration andparent-teacher organization tosolve problems and keep theschool strong.
• Help your child identify his feelings. Boys especially needhelp naming their emotions. Askquestions: “You look nervous about the soccer game today. Do you want to talk about it?”Then explore his answers.
• Teach empathy. Play a gamecalled “Trading Shoes” to teachempathy and understanding. Have your child switch shoes with someone in an argument. He can wear the shoes—andargue the case—of the other person.12
• Help your child recognize stressand its effects, and model pacingyourself. Teach him to evaluate hiscapacity for projects or work, andto recognize his limits: “You looktired this semester. Why do youthink that is? Did somethingchange?”
• Teach your child to think criticallyand evaluate the role modelsoffered by TV, movies and othermedia: “Is that the kind of personyou want to be? Why or why not?”
• Encourage your child to askquestions about everything.Answer respectfully, and admitwhen you don’t know the answers.Invite him to figure out answerswith you: “What do you thinkabout that?”
• Value downtime—relaxed, non-electronic time. Encourage him toplay pickup basketball, work on apuzzle, pretend to be a pirate. Lethim relax, interact casually withother children, and learn to rely onhis internal resources.
• Admit your limits as a parent. Ifyour child needs help and youcan’t provide it, seek professionalhelp. Some psychologists andpsychiatrists specialize in childrenwith chronic conditions—your HTCmay be able to offer a reference.
Ziva Mann earned her MA in medieval literature from Harvard University. She lives in Massachusetts with her husband,Ezra, and sons Shai and Akiva. PEN readers know Ziva from her regular column, Homefront.
their mutated genes and inherited disor-ders, are not bad eggs; they are survivorsof nature’s screening process—and they’revaluable.
As valued good eggs, our different,idea-shaking boys deserve to be taken ontheir own terms. They deserve to havetheir energy accommodated, their emo-tions turned from liabilities into strengths,and their supports made strong. In theend, Kindlon says, that different boy canbe an extraordinary one. “He’s going togrow up faster, be more mature, havemore perspective, maybe be nicer to peo-ple.” In other words, if he receives help,consideration and opportunity, your soncan be better than normal. He can bewonderfully, proudly different. He can bea boy, a man…himself.
12 From Catherine Dooley, co-director of the Mother-Son Project at Wellesley College. Boston Globe, November 6, 1997.
Helping Boys Be Boys
Parent Empowerment Newsletter • August 2003Parent Empowerment Newsletter • November 200717
Addiction, according to theNational Institute on Drug Abuse, is acomplex but treatable brain diseasethat can include a variety of mostlynegative behaviors, including compul-sive drug craving, compulsive use, andcontinued drug use despite possiblesevere consequences. Physical depend-ence and addiction are not synony-mous. Most people who use opioidsare dependent on the drugs, but notaddicted. Yet fear of addiction promptsmany people to forego adequate paintreatment, although many studies con-clude that opioid addiction amongchronic pain sufferers is rare, at1%–2%.
Non-MedicationTherapiesThe goal of managing chronic pain isto take the lowest possible dose ofmedication to effectively reduce painand let you function normally. Lowerdoses mean fewer side effects. Tomaintain low dosing, you and yourHTC pain management team shoulduse additional or “adjunct” therapiesto reduce pain, help control bleedingand speed healing.
Exercise. Every pain managementplan should include some exercise,which may be part of occupationaltherapy to help your joints regainrange of motion. Exercise has manybenefits:
• strengthens muscles• increases flexibility and range of
motion (helping reduce frequencyof bleeds)
• protects heart and blood vessels• helps maintain healthy weight• improves mood• boosts energy level• improves sleep quality• releases natural painkillers
(endorphins) in the bodyHydrotherapy (aquatic or pool ther-
apy) using warm water is useful forpeople with hemophilia, easing stiffjoints and muscles. And the buoyancyprovided by water greatly reducesstress on joints, making it easier toperform range-of-motion exercises.
R.I.C.E. People with hemophilia aretaught early about the benefits of rest,ice, compression and elevation. Those withinhibitors and chronic joint painshould always rest a bleeding area, iceit every 20 minutes, compress the jointor muscle, and elevate it to relievepressure. This helps control bleeding,speeds healing and reduces pain.
CAM. The National Center forComplementary and AlternativeMedicine (NCCAM) is a part of theFederal National Institutes of Health.It defines CAM as a “group ofdiverse medical and health care sys-tems, practices, and products that arenot presently considered to be part ofconventional medicine.”3
Complementary medicine is usedalong with conventional medicine, asmassage therapy may be used to helpreduce pain. Alternative medicine isused in place of conventional medi-cine, as a particular diet or herb maybe used for pain control. NCCAMreports that most people dealing withchronic pain use some form of CAM,yet fewer than half tell their physicians.If you decide to use an alternativetherapy, tell your HTC pain manage-ment team since some therapies canincrease your risk of bleeding or seriousside effects.
Understanding CAMCAM includes many therapies to helpyou manage pain:
Relaxation Therapy. You learnhow to relax tense muscles, reduceanxiety, and alter your mental state.Mindfulness meditation is a concentra-tion exercise that helps you focusattention on something specific, likeyour breathing pattern. Guidedimagery is a conscious meditationtechnique involving relaxation andvisualization of a soothing mentalimage, like walking on a beach.
Biofeedback Training. Electronicequipment is used to monitor yourbrain activity, blood pressure, muscletension and heart rate. This informa-tion teaches you how to recognize andthen change your reactions to stressand pain.
Behavioral Modification. Youattempt to change the habits, behav-iors and attitudes that can developfrom living with chronic pain: depend-ency, anxiety, and remaining home-bound or bedridden.
Stress Management Training.Stress, anxiety and depression canincrease your pain level. You can oftenreduce pain by learning to control orlessen your stress and anxiety throughactivities like exercise or physical ther-apy, and learning “self talk” to keep apositive outlook.
Hypnotherapy. Therapeutic ormedical hypnosis directs your focusinward, aiming at relaxation andreduced pain or anxiety. After trainingwith a hypnotherapist, you can learnself-hypnosis.
Counseling. Individual, family orgroup counseling, with a professionalexperienced in pain management, canhelp the whole family cope with aloved one’s persistent pain.Counseling provides valuable emo-tional support and guidance.
Dozens of other therapies may beuseful in pain management: acupunctureor acupressure, massage or chiropracticmanipulation, and electric stimulationto interfere with pain transmission.
The hallmark of effective pain man-agement is increased quality of life andincreased function—so you feel wellenough to go about your normal dailyactivities. Finding the right mix oftherapies may take time, but it willmake a critical difference in your life.
Pain management is an ongoingprocess. Your response to a medicationmay change over time; what works atone stage in your life may not worklater. Mapping your treatment planrequires the knowledge and expertiseof the medical team at your HTC.Regardless of how long it takes todevelop a successful pain managementplan, don’t resign yourself to “tough-ing it out” or attempting to live withchronic pain. With the myriad painmanagement options available today,no one needs to endure the cripplingeffects of unmanaged chronic pain.
Inhibitor Insights... continued from page 4
3 http://nccam.nih.gov/health/whatiscam/

18
Smith and Moffit further note that the bill’s sponsors makeit easier for applicants to be defined as low-income or as children.Low-income would now mean families with incomes up to400% above the current federal poverty level (FPL)—$82,600for a family of four. This level, according to Smith andMoffit, is “hardly considered low-income by any reasonablestandard.” Currently, 89% of all children between 300% and400% above the FPL are enrolled in private health insurance;and under the proposed legislation, people up to age 21would be recognized as “children.” Finally, unlike the originalSCHIP legislation, H.R. 3162 requires no future reauthoriza-tion, so it would become a permanent government programthat Smith and Moffit call a “full-blown entitlement.”
But Robert Greenstein, executive director of The Centeron Budget and Policy Analysis4, says that the proposed SCHIPbill would not offer or provide coverage to large numbers ofmiddle-class children who already have private coverage. Henotes that according to the CBO, H.R. 3162 would providecoverage to 5 million uninsured children by 2012. Some 4.6million (90%) of these children would have incomes belowcurrent eligibility limits. “Contrary to White House rhetoric,”writes Greenstein, “the bulk of the children who would gaincoverage are poor and near-poor children who are uninsured,not middle-income children with private coverage.”
Interested PartiesThe battle for this bill is not yet over. Many interested partieshave been vying to influence the SCHIP expansion bill’s pas-sage or veto, and will continue to fight. In fact, the bill hadan unusual amount of bipartisan support. But one group thatstrongly opposes it is the tobacco industry, which supportedthe veto. Why? A proposed increase of the cigarette tax wouldfund the expansion.5 Senator Elizabeth Dole (R-North Carolina)supports SCHIP, but feared that the expansion, supported bytobacco tax increases, would harm her state’s economy.
Yet Greenstein notes that the bill’s costs, at least over thenext five years, would be fully paid for. “This represents asharp change from earlier bills that the President enthusiasti-cally supported—from the 2003 Medicare prescription drugbill to his tax cuts—which were financed by massive amountsof deficit spending.”
The SCHIP expansion bill has fans and foes on all politicalsides. In his August 3 article, “Senate Passes Children’s HealthBill, 68-31,” Robert Pear of the New York Times offers a fascinatingreview of quotations by politicians concerning this bill. SenatorMax Baucus (D-Montana), chief sponsor of the bill, says,“Millions of American children have hope for a healthier futuretonight.” Senator Orrin Hatch (R-Utah), who helped createthe SCHIPS program ten years ago, agrees: “Covering thesechildren is worth every cent.” Says Senator Debbie Stabenow(D-Michigan), “As lawmakers, we have a moral obligation toprovide health care coverage for the millions of uninsuredchildren. Health care should be a right, not a privilege.”
But Senate Republican Whip Trent Lott (R-Mississippi)warns, “If you want to go to government-run, socialistic med-
icine, this is it, this is the way it’s going to happen.”
Do insurance companies support H.R. 3162? The bill wouldreduce federal subsidies paid to insurance companies offeringprivate health plans to Medicare beneficiaries. Robert Pearwrites, “Many Democrats say these plans, which serve nearlyone-fifth of the 43 million Medicare beneficiaries, are over-paid…Insurers say the private plans would disappear frommany parts of the country if Medicare payments were cut.”
Supporting the SCHIP expansion bill are manyDemocratic and Republican senators and representatives, andmany advocacy, civic and medical groups—about 270 in all,according to Speaker of the House Nancy Pelosi, “from theAARP to the YMCA.” Also supporting the bill, of course, aremany pharmacies and pharmaceutical companies, and theirpowerful lobbyists, who want to make sure coverage existsfor their products and services.
A Complex BillThe Bush administration rightly worries that media manipula-tion will portray this situation as a struggle between Bush andpoor children, rather than as a debate over the role of govern-ment in healthcare. Now that Bush has vetoed H.R. 3162, arethere alternatives to help uninsured children? Smith and Moffitof The Heritage Foundation recommend that Congress pro-vide direct tax relief to individuals and families—or refundabletax credit or vouchers to low-income families—enabling themto choose the type of coverage that best suits their needs.
Daniel E. Smith, vice president of the American CancerSociety, seems to suggest the answer is obvious: “The choiceis simple: Are you for kids? Are you for tobacco companies?Mr. President and Congress, we hope you side with thekids.” Sadly, the answer isn’t so simple.
In a letter to President Bush, Governors ArnoldSchwarzenegger (R-California) and Eliot Spitzer (D-NewYork) acknowledge common goals with Bush, but urgegreater cooperation toward finding a common answer: “Weagree with your administration’s goal of trying to deter fami-lies from dropping private coverage in favor of SCHIP…butthe rules proposed by CMS would install thresholds that areimpossible to meet for nearly every state and impose a one-size-fits-all solution to a dynamic and complex problem.”6
Although this is only Bush’s fourth veto since taking office, hehas clearly signaled that he wants to negotiate, to make healthcoverage for underprivileged children more effective. “Becausethe Congress has chosen to send me a bill that moves our healthcare system in the wrong direction, I must veto it,” Bush said inhis statement. He added that he hoped to work with Congress“to produce a good bill that puts poorer children first.”7
Like healthcare itself, H.R. 3162 is tremendously complex.Firing off an email to the president may feel like a decisiveact, but its echoes are meaningless unless grounded in well-thought-out beliefs and principles concerning how Americashould best allocate funding and most effectively structure itshealthcare system.
4 www.cbpp.org/9-21-07health-stmt.htm and www.cbpp.org/9-25-07health2.htm 5 Funding for the expansion would come from higher tobacco taxes. The federal excise tax on cigaretteswould rise to $1 a pack under the Senate bill and to 84 cents a pack under the House measure, up from 39 cents a pack. 6 Letter to President Bush, August 29, 2007, governors ArnoldSchwarzenegger and Eliot Spitzer: www.mrmib.ca.gov/mrmib/HFP/POTUS_SCHIP_letter_08-29-07.pdf 7 “Bush Vetoes Children’s Health Bill,” David Stout, New York Times, October 3, 2007.
Storm Watch... continued from page 6
Parent Empowerment Newsletter • November 2007

800-423-2862www.hemophiliagalaxy.com
Baxter’s website for hemophilia families
Customer Service 800-243-4153
Reimbursement HELPline800-288-8374
www.kogenatefs.com
PEN gratefullyacknowledges ourcorporate sponsors
Parent Empowerment Newsletter • August 2003Parent Empowerment Newsletter • November 200719
888-999-2349www.hemophiliavillage.com
888-508-6978 www.cslbehring.com
800-727-6500www.novonordisk-us.com/biopharm
Prophylaxis patients now have proof toshow healthcare insurers. The article“Prophylaxis versus Episodic Treatmentto Prevent Joint Disease in Boys withSevere Hemophilia” was published inThe New England Journal of Medicine,August 9, 2007. It describes a clinicalstudy by the principal investigator and
lead author of the resulting report,Marilyn J. Manco-Johnson, MD, profes-sor of pediatrics and associate professorof pathology, department of pediatrics,University of Colorado at Denver andHealth Science Center. The results ofthe study suggest that when it comes toreducing joint bleeds and life-threatening
bleeding in young boys with severehemophilia A, prophylactic therapy isbetter than on-demand treatment.
Source: AScribe Newswire, August 8, 2007
Proof That Prophylaxis Works
New preclinical data presented at theInternational Society of Thrombosis andHaemostasis (ISTH) in June demonstrates thatPEGylated forms of recombinant factor VIIIprolong bleeding protection. The data offershope for commercially available longer-actingfactor concentrates some day.
Source: Joseph M. Miller, managing supervisor,Fleishman-Hillard, (216) 928-3491
Bayer Reports PositivePreclinical Study Results on
Longer-Acting Recombinant Factor VIII
headlines
Baxter BioScience’s Advate is nowavailable in 250, 500, 1000, 1500,2000 and 3000 dosage strengths.The new 3000 IU strength is recon-stituted with 5 ml of sterile water,supplied with the BaxJect II needle-less transfer device. Decreasing thenumber of vials needed and reduc-ing total infusion volume makestreatment easier and faster for peo-ple who need higher doses.
Source: company press release
New 3000 IU Dosage for Advate
King Pharmaceuticals’ new FDA-approved bovine thrombin topical hemostatic product canhelp stop nosebleeds. The Thrombin-JMI Epistaxis Kit offers emergency department andtrauma center staff “a convenient new option to achieve fast, active hemostasis during epis-taxes,” reports a company official. The product will be available in the fourth quarter 2007.
Source: International Blood and Plasma News, August 2007
New Intranasal Spray Delivery Device
man
ufac
ture
r
The Taipei Times reported on August 30 thata man with hemophilia in Taiwan is await-ing sentencing for a number of crimes hedid not commit. The man appeared incourt at trials, in place of the real criminals,and served their prison sentences in return
for large sums of money. Apparently, hisscam worked. He knew he would bereleased early from his prison sentences as aresult of the high cost of his factor, whichthe prison could not afford.
Source: www.TaipeiTimes.com
Man with Hemophilia Jailed for Impersonating Crooks
wor
ld
Alan Kinniburgh, PhD, resigned in Augustas CEO of NHF for undisclosed reasons.Hired in January 2005, Kinniburghresigned after his three-year contract wasup. Effective immediately, NHF appointed
Howard A. Balsam, CPA, to the position ofinterim chief executive officer. HowardBalsam joined NHF in April 2005 as chiefoperating officer.
nonp
rofit
NHF CEO Resigns
factor deficiency type and severity
name and date of birth of child(ren) with hemophilia
daytime phone email address
city/state/zip/country
address
name
organization
the
&
patient parent medical treater educator hemophilia organization hemophilia company
email only (PDF file)post only (hard copy)both
maintains a special network of patients and parents to provide uswith information for upcoming articles and projects. We want to get yourideas, opinions and experiences periodically through telephone surveys,interviews, or written questionnaires. If you’d like to be on our elite team,check “Yes” in the box at left, and send or email this form to us.
Do you wantto join the
ResearchTeam?
Yes! Nocu t a long t he do t t ed l i ne
Join Our Research Team
sign up to receive
LA Kelley Communications
LA Kelley Communications, Inc.68 East Main Street, Suite 102Georgetown, Massachusetts 01833 USA
hemophilia newsletter by families
for families
ADDRESS SERVICE REQUESTED
PRST STD
US POSTAGEPAID
N. READING MA
PERMIT # 140
Check any that apply:
is available either in hard copy or electronically in PDF format.To receive PEN electronically in a PDF file, you must downloadAcrobat Reader (free through Adobe at www.adobe.com). PDF filessave us postage and arrive about two weeks before the hard copy.
is free to patients, families, hospitals, nonprofit organiza-tions and corporate partners of LA Kelley Communications. Otherinterested readers may subscribe for $24.95/year (mail/hard copy) or$14.95/year (email/PDF). To sign up, simply complete this form andreturn it to the address below with a check or money order madepayable to LA Kelley Communications, Inc.
LA Kelley Communications, Inc.68 East Main Street, Suite 102 Georgetown, MA 01833 USA
Or subscribe online at www.kelleycom.com
I would like to receive by:
Inside:
FROM BOYS TO M
EN: NURTURING
YOUR SON WITH HEM
OPHILIA