fran lockie on kids: just little adults?
TRANSCRIPT

Kids: Just Little Adults?
Dr Fran Lockie MedSTAR
Paediatric Emergency, Women’s and Children’s
Bedside Critical Care, September 2013
Scope
• Case
• Why are we scared?
• Structured approach
– Airway,
– Breathing
– Circulation
• Can we do better?
15 month old male with fever
• NVD at term, BW 2.7kg
• Previously fit and well
• No meds, NKDA
• Immunisations UTD
• Family all coryzal
Country Hospital
• At triage (17:30)
– Alert and playful
– Temp 39, Hr 160, Rr 40
– Good central perfusion
– Mottled peripherally
18:45 Seen by RMO
• Given panadol with resolution of fever, HR never < 170 since triage
• Bloods
– VBG pH 7.15, BE -10, B/C 10, lact 5, CO2 25
– BSL 6
• Urine NAD
URTI focus for fever identified
• 2 small vomits in waiting room, then a small area of petechiae
21:00 Advice: O2, 20ml/kg Fluid bolus, Antibiotics, peripheral inotropes
22:00
• A Maintained, No O2
• B RR 60, marked increased resp effort
• C peripheral CRT: absent, central >5 secs
• D alert, talking to mum
• 24g PIV tissued, further attempts unsuccessful
Rapid deterioration
– AVPU
– Increasing respiratory distress
– HR >200, Only femoral pulse palpable
– IO sited
– Aggressive filling
– DA started
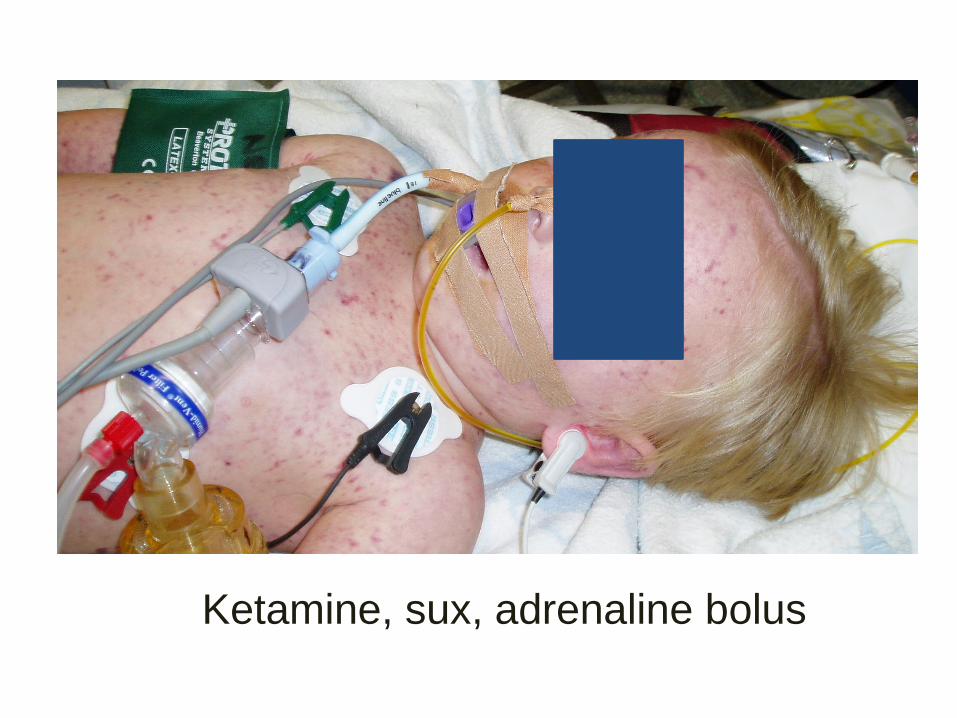
Ketamine, sux, adrenaline bolus
PEA Arrest
• Filling, filling, filling
• Dopamine started at 20mcg/kg/min
• Filling, filling, filling
– 4% albumin
– Blood products (packed cells, plts, FFP, cryo)
• Noradrenaline, Adrenaline, infusions commenced
• Stat dose hydrocortisone
6hrs later….still PEA / ROSC • Maximal inotropic / pressor support
• multiple dextrose, Ca, Mg boluses
• Total fluids 180ml/kg
• Sustained bradycardia, worsening acidosis
• Massive pulmonary haemorrhage
• Parents present throughout
• RIP, 03:00
We are scared of kids!
• Kids need early aggressive treatment
• Failure to diagnose shock
• Failure to resuscitate
– Early access
– Early fluids
– Early Abx
– Early inotropes (peripheral is OK!)
– Early intubation
– Evaluate our actions: lactate and physiology
• Audit of 17 PICU’s
• 107 patients with septic shock
• 8% received care c/w ACCM guideline
– 21% not given >60ml/kg despite ongoing shock
– 15% not given dopa/ dobu despite fluid refractory shock
– 23% not given catechol for dopa/ dobu refractory shock
– 30% not given steroid despite catechol resistant shock
Arch Dis Child 2009
• FAILURE TO DIAGNOSE SHOCK
• 3 factors
– Not looked after by a paediatrician
– Lack of supervision
– Failure to administer inotropes
BMJ
2005
Pediatrics 2009;124;56
Early Resuscitation of Children with Moderate to severe TBI
• 299 kids with mod-severe TBI
• 39% became hypotensive
– Of these only 48% were treated
• 44% became hypoxic
– Of these 92% were treated
• ED staff
• Anaethetics
• Theatre staff
• Standardised scenarios
• Causes of error
Resuscitation, in Press 2013
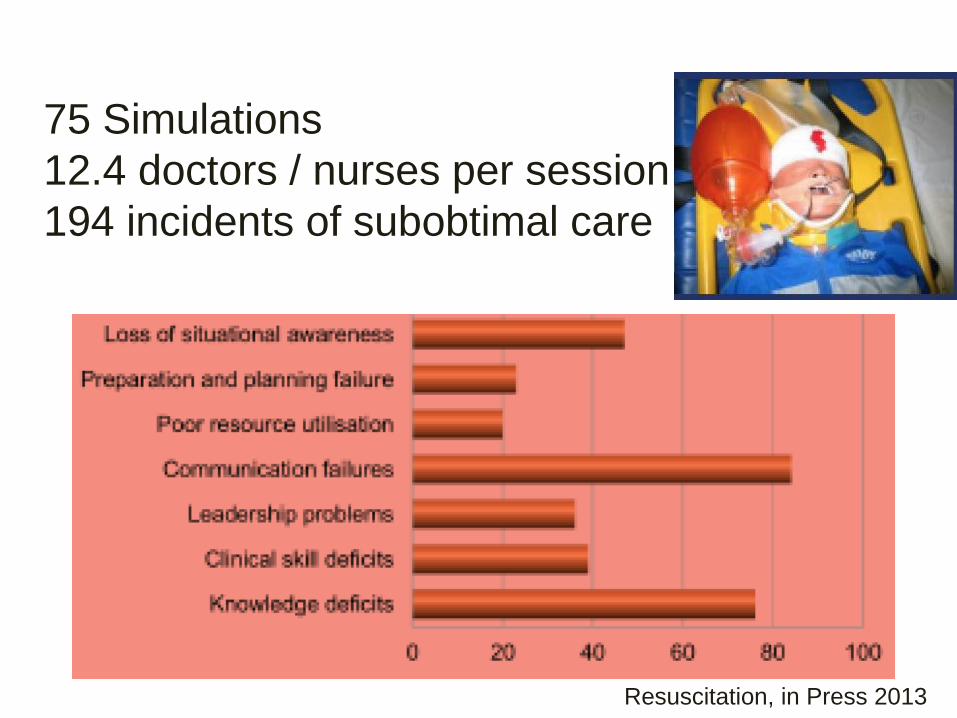
75 Simulations
12.4 doctors / nurses per session
194 incidents of subobtimal care
Resuscitation, in Press 2013
We are scared of kids! Solutions…
Train together!
• One Base
• Adult teams
– ED
– Intensivists
– Anaesthetists
• Paediatric and neonatal teams
• Special operations paramedics


• Teamwork
• Leadership
• Crew Resource Management
• Resus drills
• Intubation drills
• Competency frameworks

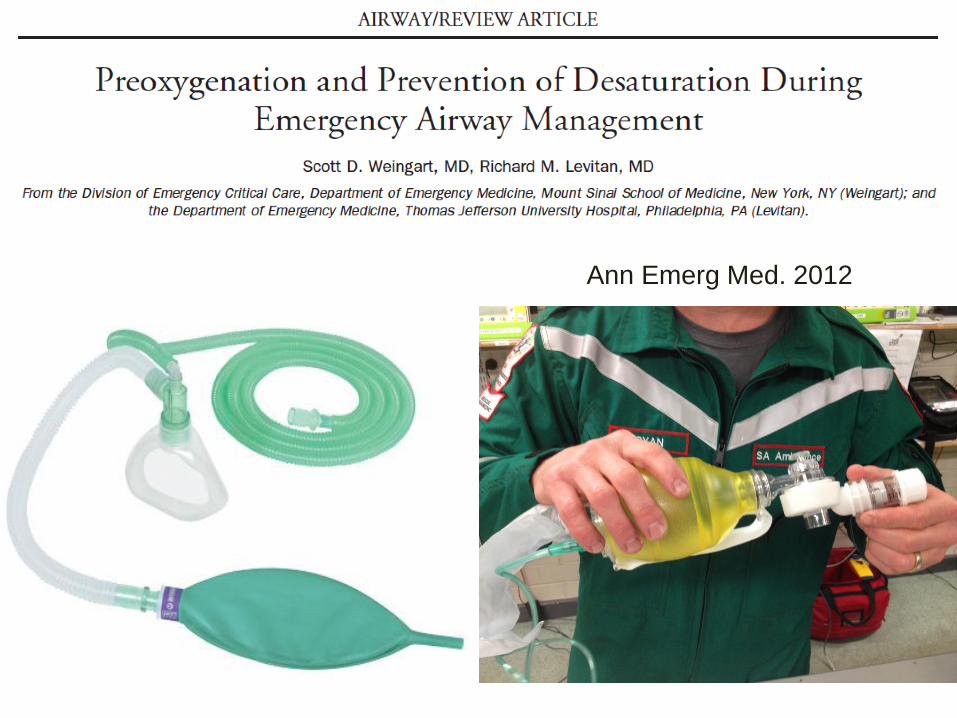
Ann Emerg Med. 2012
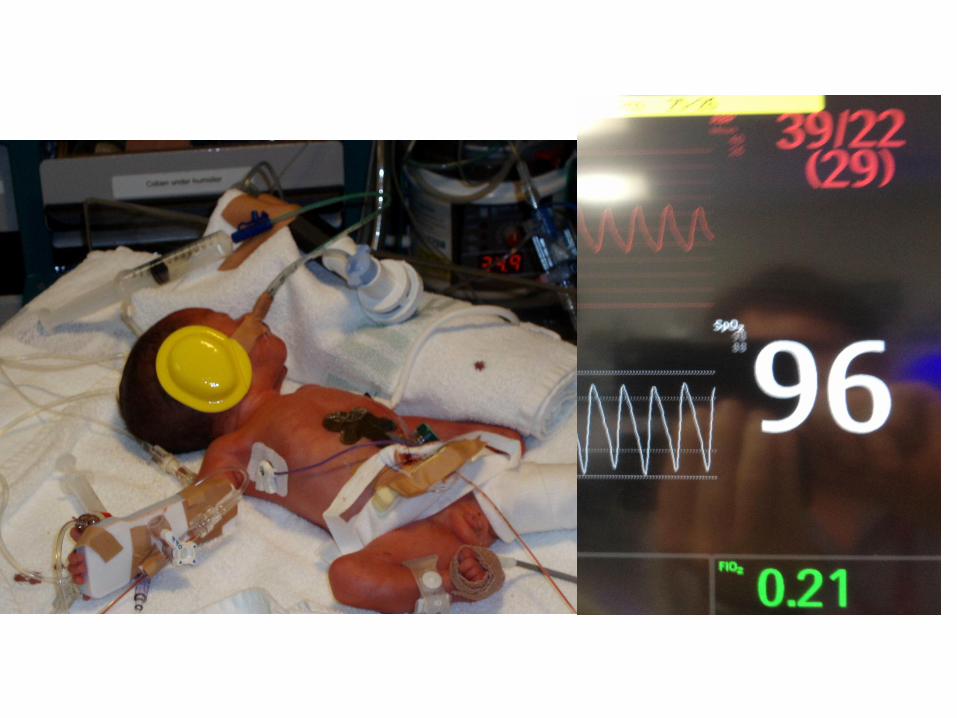
Kids have smaller FRC
Greater VO2 than adults
Rapid desaturation (with stress and apnoea)
Ann Emerg Med. 2012
Ann Emerg Med. 2012
Levitan: Dentition, disruption, disproportion, dysmobility

Levitan: 4Ds
“Doctor, He’s Tiring!”
• Diaphragmatic exhaustion
• Lacks type 1 muscle fibres
• Decompress the stomach
– Often results in dramatic improvement!
• Know your vent: wt limits
– Generally TV 4-6 ml/kg
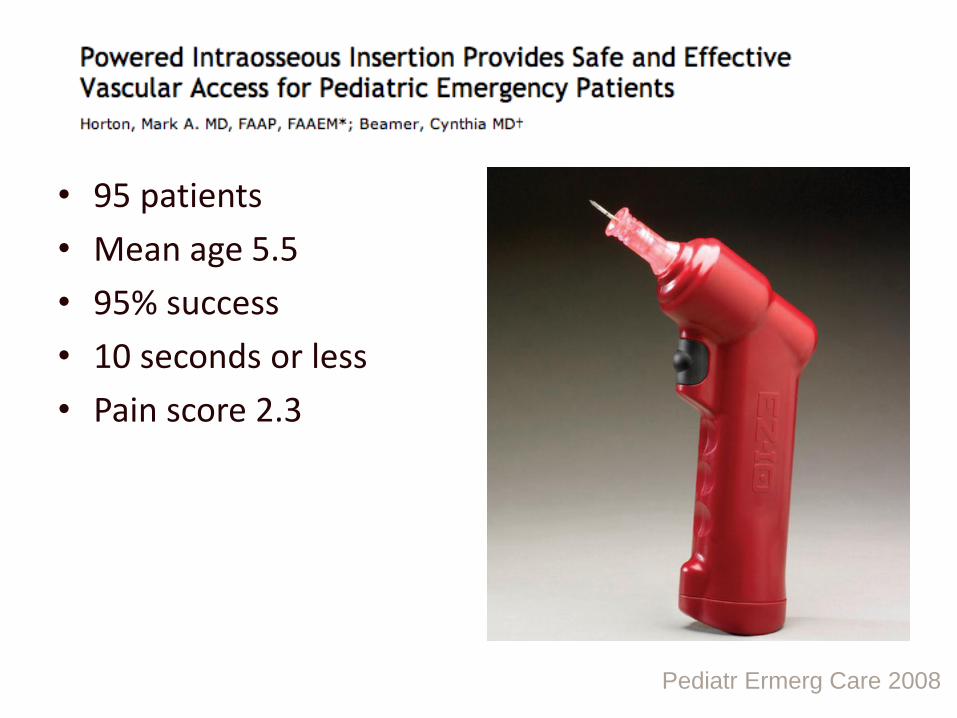
• 95 patients
• Mean age 5.5
• 95% success
• 10 seconds or less
• Pain score 2.3
Pediatr Ermerg Care 2008

SAFE study
Sepsis resuscitation (FEAST)
Trauma resusitation / massive transfusion
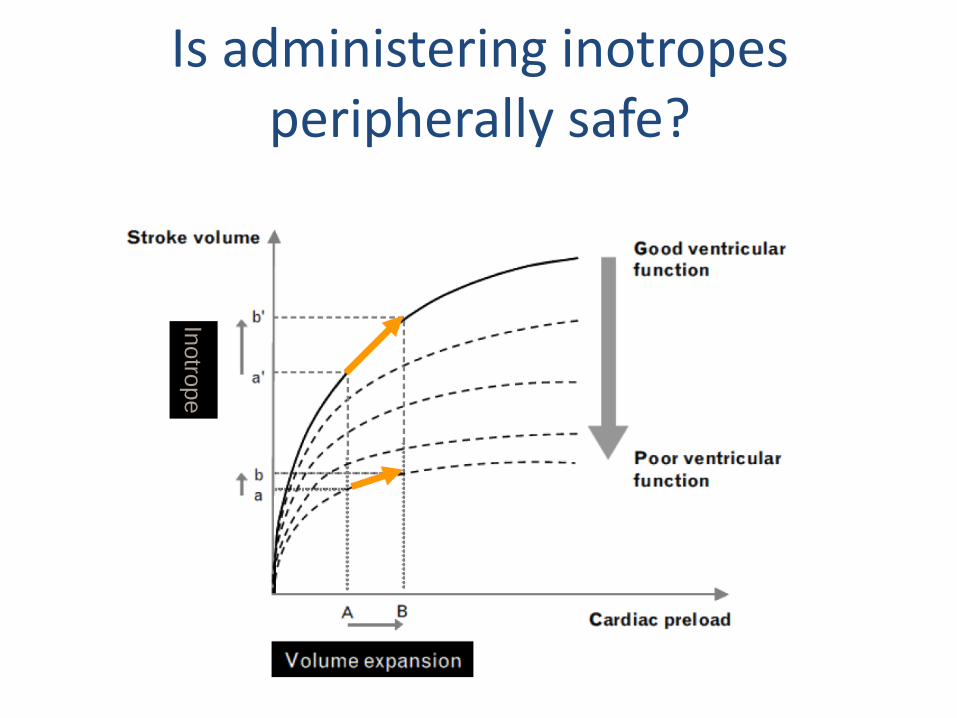
Is administering inotropes peripherally safe?
Inotro
pe
• 73 of 1133 treated with vasoactive agents by peripheral IV
• Primarily Dopamine monotherapy (90%) or Dop + Ad (7%)
• 11/73 (15%) developed infiltration – all resolved without
significant intervention
• Longer duration
• Higher dose of dopamine
Pediatr Emerg Care 2010
Sugar and temperature
• Large SA: body wt (2-2.5 x BW)
• Thin skin and subcut fat (less insulation)
• No shivering
• Immature thermoregulatory center
• Sugar ALWAYS goes down in critical illness…
Lancet 2011; 377: 1011–18
• Listen to the physiology!
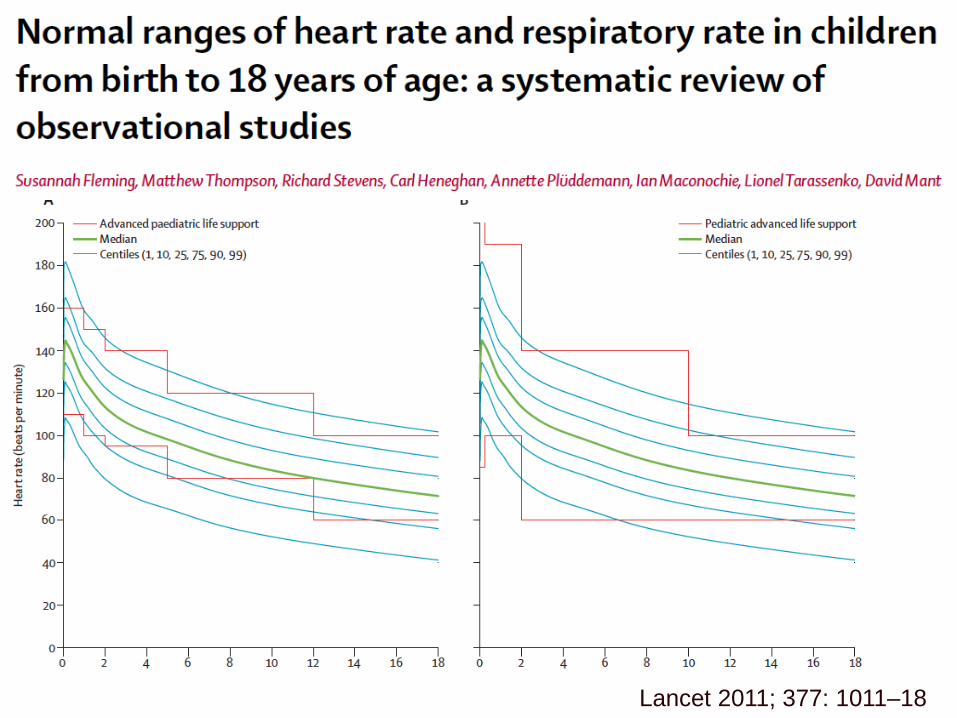
Lancet 2011; 377: 1011–18
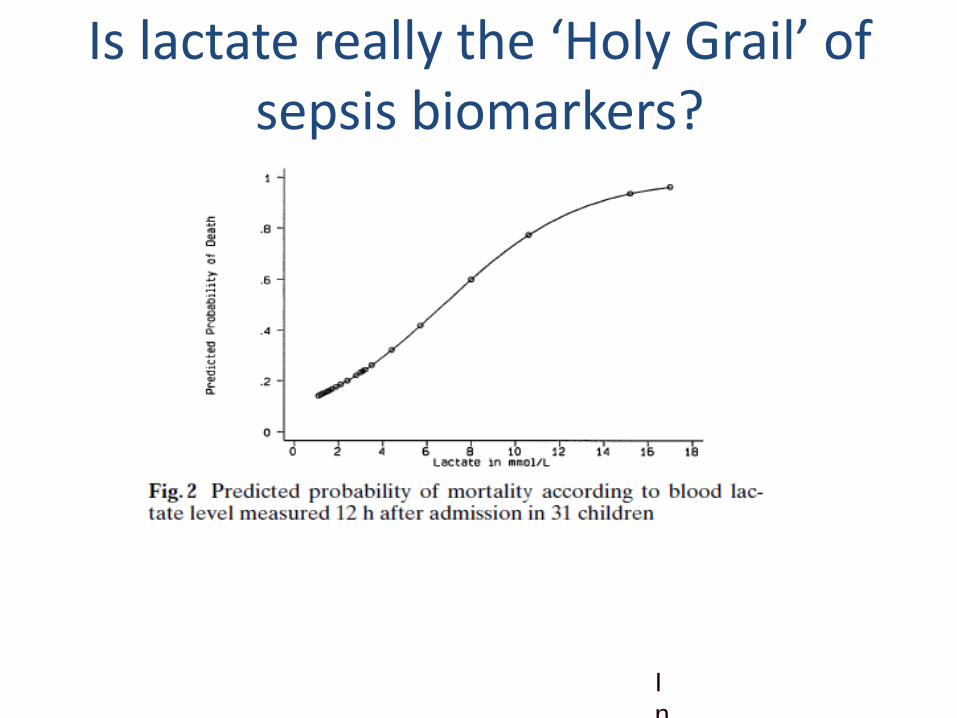
Is lactate really the ‘Holy Grail’ of sepsis biomarkers?
I
n
t
e
n
s
i
v
e
C
a
r
e
M
e
d
1
9
9
7
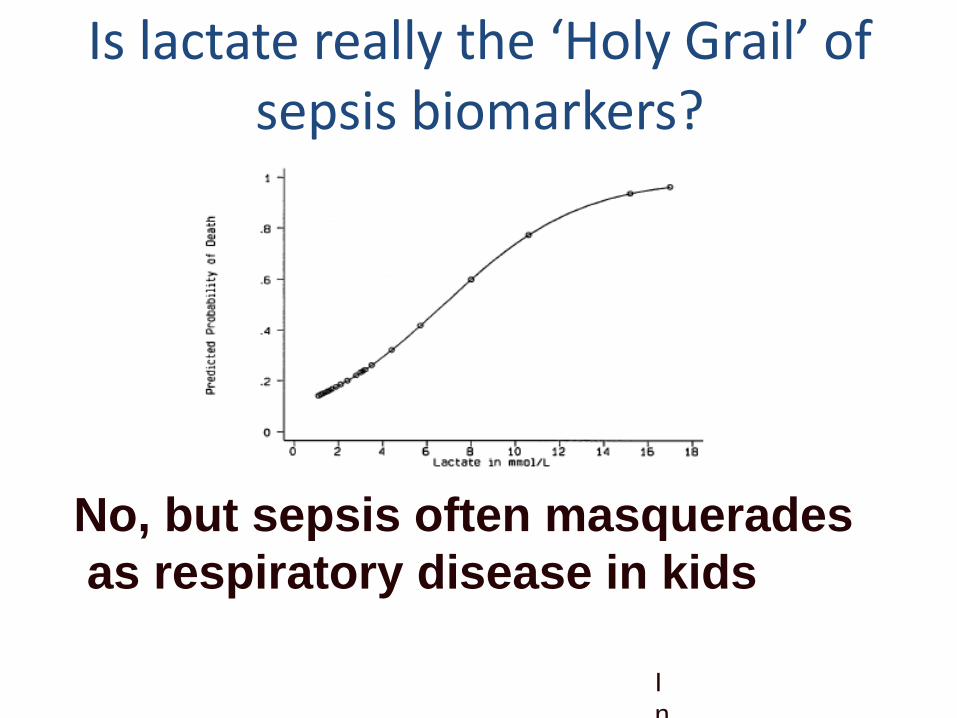
Is lactate really the ‘Holy Grail’ of sepsis biomarkers?
I
n
t
e
n
s
i
v
e
C
a
r
e
M
e
d
1
9
9
7
No, but sepsis often masquerades
as respiratory disease in kids
If you still can’t explain it…
• Always assume ingestion
• Always assume inflicted injury
Smaller but the same
• Train together??
• Golden rules
– PEEP
– NGT
– VBG + Physiology
– Early inotropes
– Ingestion / inflicted
– Pink, warm and sweet