fissure sealant presentation
TRANSCRIPT
In the name of GOD
Pit and fissure sealantsNarges shojaei
1

the Centers for Disease Control and Prevention (CDC):
profession is dental caries, a chronic disease affecting more than 90% of adults aged 20 to 64 years.1 Although chronic diseases are among the most common and costly of all health problems, they are also among the most preventable
2
Epidemiology of Pit and Fissure Caries
dramatic improvements in the prevention of caries have occurred :
I. fluoride exposure
II. enhanced awareness of the benefits of early care
III. increased access to dental care
IV. increased financial coverage by insurance companies
V. group plans, and government-funded programs of preventive and restorative dental procedures for children
3

According to the National Institute for Dental and Craniofacial Research, 20% of the population bears at least 60% of the caries
• Dental caries :children living in poverty
• five time
• Minority populations
• specific tooth surfaces
• almost 25% of the decayed, missing, filled surfaces (dmfs) index
• 90% of caries in permanent
• two thirds of caries
4
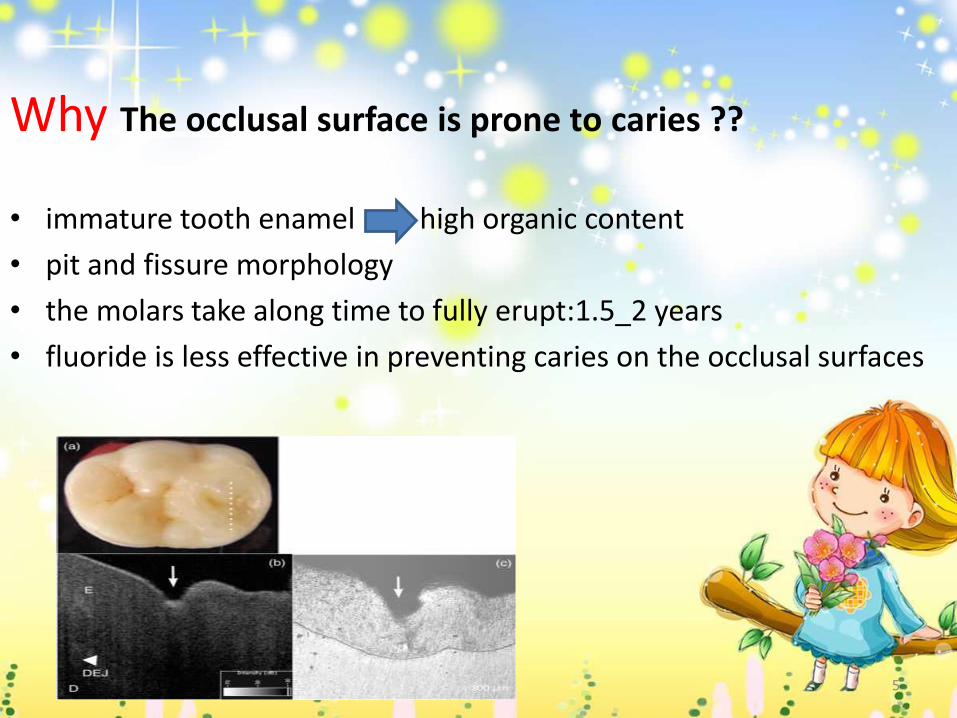
Why The occlusal surface is prone to caries ??
• immature tooth enamel high organic content
• pit and fissure morphology
• the molars take along time to fully erupt:1.5_2 years
• fluoride is less effective in preventing caries on the occlusal surfaces
5
in 1955, Dr. Michael Buonocore revolutionized dentistry with the first reserch on adhesive dentistry
a physical barrier over susceptible pits and fissures and, in effect, “seal” out caries, preventing the carious process
In 1971 the first dental sealant, Nuva-Seal
the theory of sealing the occlusal surfaces of teeth in an effort to maximize “the power of prevention.”
6

Sealant Effectiveness
Unquestionably, dental sealants prevent pit and fissure caries in both primary and permanent teeth
Healthy People 2010 set a goal for the prevalence of sealants in children and adolescents to increase to 50%
Low usage :
1. lack of confidence in the bonding of sealants to enamel
2. concern for sealing over caries
3. difficulty of achieving isolation
4. lack of reimbursement for sealant placement
7

Current sealant utilization:
8
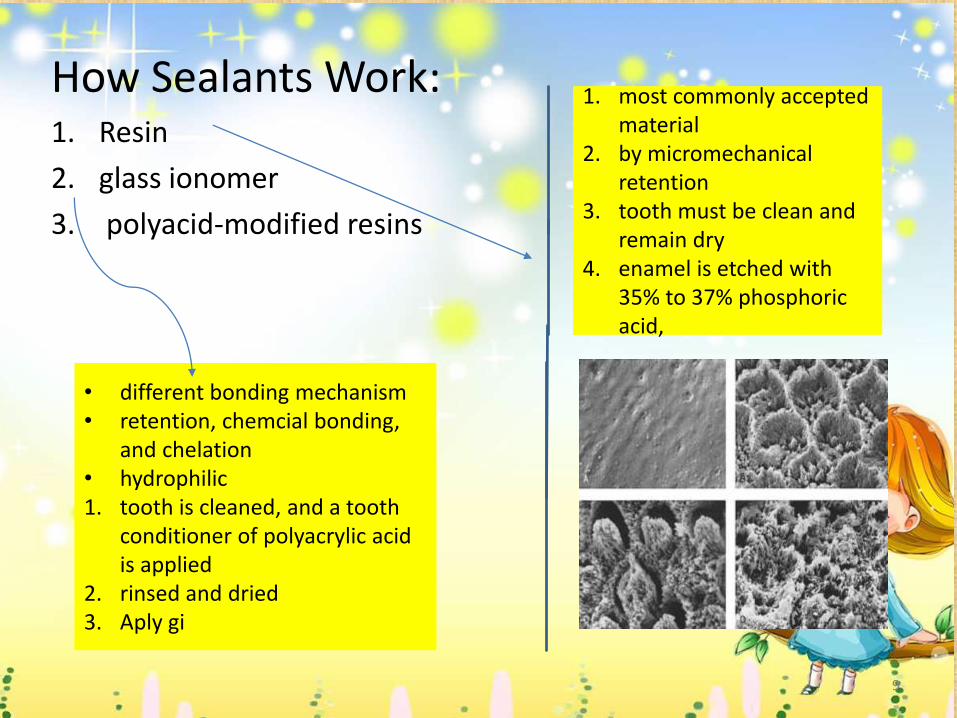
How Sealants Work:1. Resin
2. glass ionomer
3. polyacid-modified resins
1. most commonly accepted material
2. by micromechanical retention
3. tooth must be clean and remain dry
4. enamel is etched with 35% to 37% phosphoric acid,
• different bonding mechanism• retention, chemcial bonding,
and chelation• hydrophilic 1. tooth is cleaned, and a tooth
conditioner of polyacrylic acid is applied
2. rinsed and dried3. Aply gi
9

Types of sealants:
variety of materials, colors, and viscosities
Resin-based sealants :
• unfilled, filled
• clear, colored
• visible light–polymerized, autopolymerizing (chemically cured
• fluoride-releasing materials
earliest sealants :autopolymerizing but now replaced by self cured sealants
10
Why?
1. sets in 10 to 20 seconds
2. No mixing and air bubble
3. the viscosity of the sealant remains constant
4. sealant material does not set until it is light activated
5. similar retention rates and similar strengths.
11

Color:
available as clear or opaque white:
Advantage of an opaque sealant:
1. easy to see during application
2. easy to monitor its retention at a recall visit
3. . Assessment of a clear sealant requires tactile
4. No apparent difference in the clinical efficacy of either type of sealant
being able to quickly and correctly assess
sealant retention is clinically important.
12

newer materials
1.color properties:Clinpro (3M ESPE, St. Paul, Minn.)
• that is pink upon application and turns white when cure
• . This color change provides no clinical advantage and has been described as a “perceived marketing benefit
2:(Ivoclar Vivadent, Amherst, N.Y.).
• containing a photochromic dye
• correct wavelengths :change from clear/yellow to green
• is clinically relevant because it may assist a provider in assessing the sealant’s retention upon recall examination
• But:using a polymerizing lamp
• have similar properties andcaries-protective as other resin-based sealants
13
1
Filler Content:physical characteristics
unfilled sealants deeper into the fissures :
• low viscosity:longer resin tags, and therefore be better retained
• other studies have found similar retention rates with unfilled and filled sealants
• clear advantage of the unfilled sealant :
1. lower rates of microleakage
2. better penetration into the fissures
3. occlusal adjustment is not necessary(necessity to adjust the occlusion increases the time and cost of the procedure)
Viscosityflowability,and resistance to wear
14
flowable composite: inferior retention and microleakage
utilizing a bonding agent improves fissure penetration and decreases microleakage
need for a bonding agent and occlusal adjustment
the conventional unfilled resin-based sealant appears to be the most appropriate preventive therapy.
Fluoride-Releasing Sealants:salivary fluoride levels are the same before and after
no long-lasting release of fluoride
marketing benefit by manufacturers
15
Glass Ionomer:as an alternative to resin-based
1. fluoride-releasing
2. recharging ability
3. moisture toleration
4. easy application
But poor retention rates the use of resin-based sealant
usage:
ART(high-viscosity sealants placed with “finger pressure)
compromise sealant placement
Preventin of caries resin baced sealant
Retention resin based sealant16
Polyacid-Modified Resin Composites (Compomers):• the esthetic property of composite
• fluoride-releasing property and adhesion of glass ionomer
similar to composites
Similar to GI:release fluoride( GI )
poor marginal integrity,retention and occlusal wear
• contain no water hydrophobic
• polymerization• lack the ability to
bond to tooth• require bonding
agents
17
Who Really Needs Sealants?
18

19
Age at Placement:
• caries incidence occurring shortly after tooth eruption and then tapering
• occlusal surface was most vulnerable(first few years after eruption )
• that fluorides may have caused a delay in pit and fissure caries resulting in occlusal surfaces that decay at a later age
• adults should receive sealants when the tooth or the patient is at risk of experiencing caries
• place a sealant should not be based on how long ago the tooth erupted but on the clinical impression of whether a sealant is necessary to prevent caries
20

Which Teeth Should Be Sealed?
Traditionally: non carious first and second permanent molars
with deep fissures
now any tooth at risk of developing caries
• including primary teeth
• permanent molars with incipient, noncavitated lesions, and/or premolars.
21
Indications :
deep, retentive pits and fissures”(cause wedging or catching of an explorer)
stained pits and fissures with minimal appearance of decalcification or opacification (no cavitation)
no RG or clinical evidence of interproximal
use of other preventive treatment, such as fluoride therapy
possibility of isolation
22

Contraindications :
well-coalesced, self-cleaning pits and fissures
interproximal caries in need of restoration
interproximal lesions or restorations with no preventive plan/treatment to inhibit caries formation
life expectancy of the primary tooth is limited
no possibility of isolation from salivary (due to either eruption status or patient behavior.)
23
Diagnosing Occlusal Caries
dentists correctly diagnose only 42% of cases
Usage of expelorer : yes or no ?
No :
Yes :
eliminate plaque in the fissures
determine surface roughness of incipient lesions
time-tested tool
Tactile diagnosis :specific criteria for detection and diagnosis of pit and fissure lesions
does not increase dentists’ ability
tactile examination unreliable
enamel defects(cavitation
24
Caries is present when :
1. explorer catches or resists removal after the insertion into a pit or fissure
2. when this is accompanied by one or more of the fallowing
• A softness at the base of the area
• Opacity adjacent to the pit or fissure
• Softened enamel adjacent to the pit or fissure
25

the use of explorers is not necessary for the detection of early lesions
Visual examination alone (of a clean, dry tooth) is sufficient to detect early lesions
26
Sealing Over Incipient Caries:
If sealants are applied properly and are monitored periodically, caries arrest beneath a sealant
sealant placement greatly reduces the number
of carious lesions that progress
decreases the viable bacteria
Acid etching eliminates 75% of the viable microorganisms
100% reduction in total viable bacteria
27
. Whenever a situation occurs in which the practitioner is certain that a restoration is not yet warranted but is unsure of whether the fissure is simply stained or is exhibiting signs of incipient caries, the practitioner should err on the side of placing a sealant rather
than monitoring the lesion.
28
Cleaning the tooth:
For flow in the fissures it must be cleand:several method:
historically:pumice ,prophy cap ,bristle brush
Other method: explorer ,air water spray or dry bristle brush
Sup cleaninig method: cavitron prophy-jet(air polishing)
Advantage: remove more debry ,increase resin tags
but not standard
equipment cost and complication
No difference in retention29
Mechanical preparation:
Invasive technique minimally described:
Enameloplasty and fissurotomy:
Better penetration
Increase surface area fore etching
Dosent decrease microleakage
Air abrasion :
another technique but cant substitute etching
Some studies show that air abrasion in combination with
Etching improved retention30
Disadvantage :
• limits delegation of sealant placement to axilliaries
• Decrease cost effectiveness
• Expose child to handpiese
the plaque should be removed but removal of tooth structure by bur unnecessary
Effect of fluoride treatment
Multiple studies confirm sealant bond strength and retention
Are not affected by fluoride treatment before sealant
application
31

Factors affecting sealant success:
Etching
Drying agent and time
Curing
Isolation
Time of sealant placement
Auxiliary application
Four-handed delivery
32
Etchant :
Phosphoric acid , self etching system , liquids and gel
Historically:ething:60 s and rinsing time :at least 10 s
Etching time for fluoride tooth should be increased
Usual recommendation : etching:30 s rinsing :20 -30 s
It is important that removal of all etching agent from surface
No difference between liquids or gel system in bond strength
And retention
Self etching needs a separate etching step
Not recommended
33
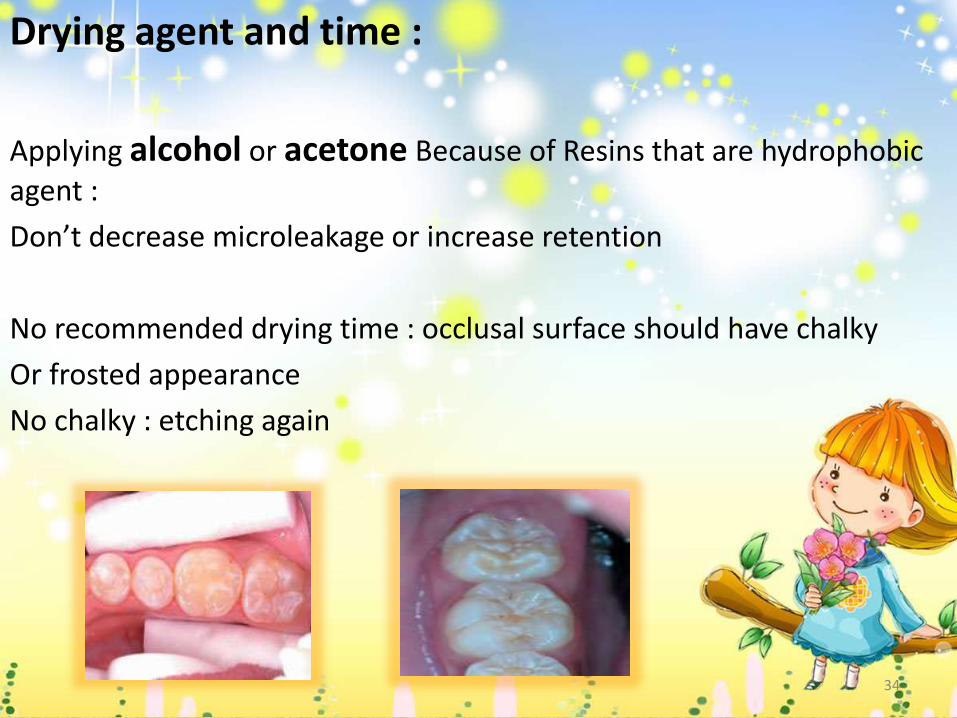
Drying agent and time :
Applying alcohol or acetone Because of Resins that are hydrophobic agent :
Don’t decrease microleakage or increase retention
No recommended drying time : occlusal surface should have chalky
Or frosted appearance
No chalky : etching again
34
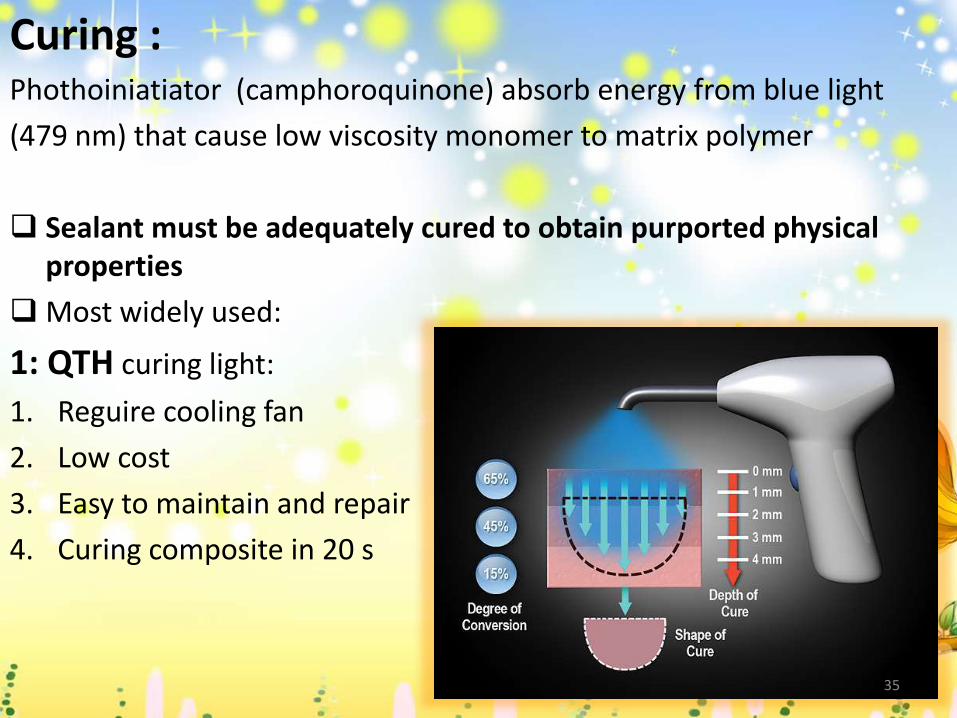
Curing :Phothoiniatiator (camphoroquinone) absorb energy from blue light
(479 nm) that cause low viscosity monomer to matrix polymer
Sealant must be adequately cured to obtain purported physical properties
Most widely used:
1: QTH curing light:
1. Reguire cooling fan
2. Low cost
3. Easy to maintain and repair
4. Curing composite in 20 s
35
2: LED : First LED curing had low energy output ,recent LED increase out put intensity
Latest LED s advertise 5s curing in<torbo> or <plasma> method
May be concerns with such quick cures:
1. Significant rise temperature(pulp injuries)
2. May cause undesirable physical properties
3. Increase polymerization contraction
4. More internal stress
5. Reduced flexural fatigue
Highest level of cure:40 s exposure with
the tip of the Light source placed directly
over sealant36
Several factors affect level of cure :
1. Shade of the materials
2. Filler content
3. Thickness of material
4. Intensity of light curing
5. Distance between light source and sealant surface
clear sealant can be cured to deeper level than opaque sealant in same curing time
37
Isolation
Resin based sealant are moisture sensitive:
Saliva prevent the formation resin tag decrease retention
Isolation is a critical step to the success of sealant
Considered a key concept in clinical procedures
Rubber dam:
Some studies show increased retention
Whenever possible especially if cocorurrent
Operative treatment is provided rubberdam
should be used
38
Timing of sealant placement :
• Correlated with overall retention:
• Partially erupted teeth require repair or replacement more than other
• When operculum extended over distal marginal ridge:50% of teeth to be resealed
• When it was at level of marginal ridge : reseal 26%
• When achieving isolatoin is difficult or precooperative :using
Glass ionomer
39
Use of intermediate bonding agent :An intermediate layer between tooth and sealant
advantage
Increase retention rate
Decreased microleakage
Increased penetration of sealant into fissures
Not only permanent tooth : primary as well
Hypomineralized teeth(at higher risk than normal)
disadvantage
Proper sealant placement technique
Increased chair time
Cost
whould inhance sealant retention on clinical
Situation 40

Auxiliary application :
No difference in retention of sealant when applied by dentist or trained dental auxiliary
Four-hand delivery : No difference in retention
Expert opinion support use of trained dental assistant
Improve quality and efficiency of sealant placement
Isolation
Shorten placement time
Reduce fatigue and enhance patien care
41
School based sealant program:
Increase sealant using
Reduceing careis
Provide prevention service to child less likely to receive dental care
It is important and effective public health approach that complements clinical care systems
in promoting oral health
42
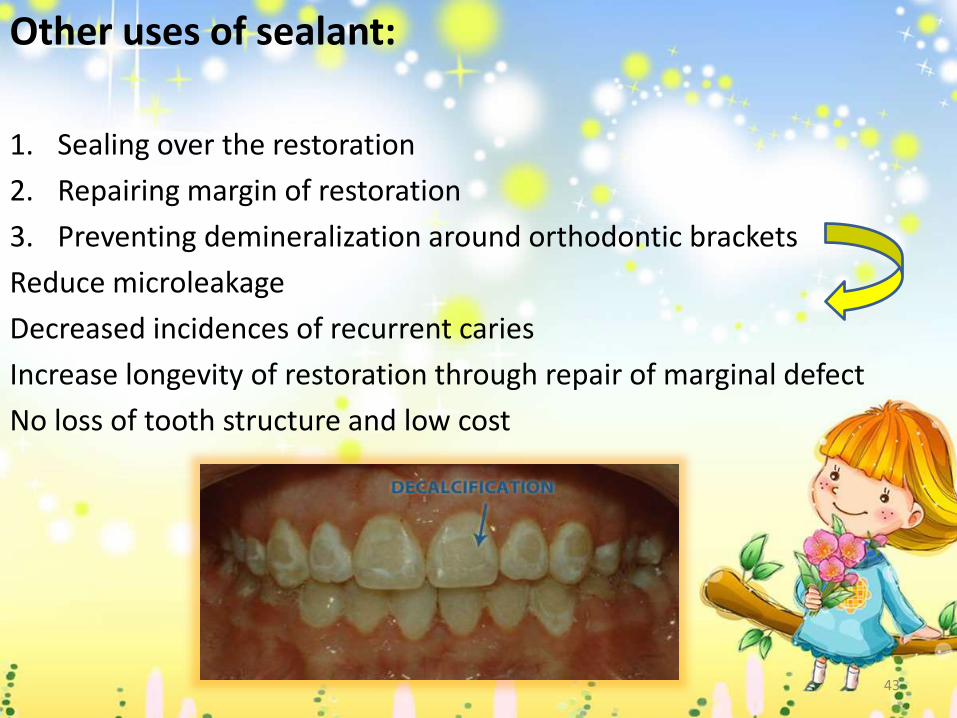
Other uses of sealant:
1. Sealing over the restoration
2. Repairing margin of restoration
3. Preventing demineralization around orthodontic brackets
Reduce microleakage
Decreased incidences of recurrent caries
Increase longevity of restoration through repair of marginal defect
No loss of tooth structure and low cost
43

Clinical procedure:1:Isolation:
Most common method :cotton roll
For maxillary isolation :
tri angular buccal shield :angle posterior
Cotton roll : maxillary vestibule
Mirror is used during entire procedure
mandibular isolation :
Cotton roll : two vestibule
Cotton roll holder or hand may be
used
Triangular shield on buccal
44
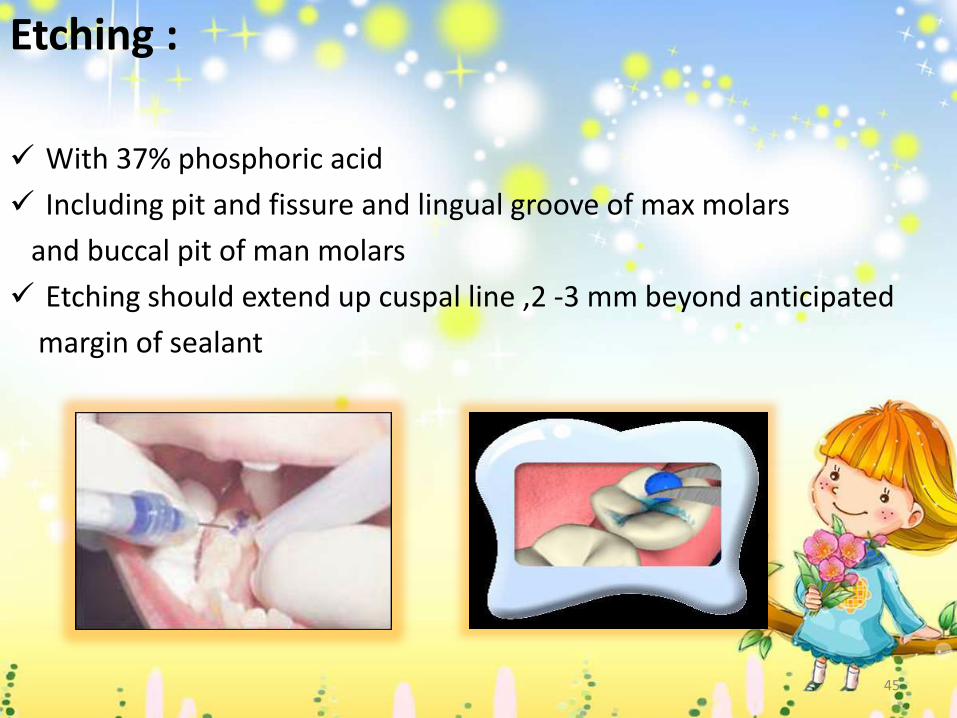
Etching :
With 37% phosphoric acid
Including pit and fissure and lingual groove of max molars
and buccal pit of man molars
Etching should extend up cuspal line ,2 -3 mm beyond anticipated
margin of sealant
45
Rinsing and drying :
Air-water spray and high volume suction
Most manufactors recommended :20-30 s
The goal of rinsing is removal all of etchant from surface
Sealant application and polymerization:
Should be applied to all pit and fissures
With : expelorer ,PICH, or small brush
Shouldn’t be over filled
• Does not extend past the etched area
• Limit occlusal interence
• Ensure adequate depth of cure
Small bubbles should be teased out of the material before polymerization
• Exposure time of 40 s is more appropriate 46

Evaluating the sealant : Visually an tactilely examine the sealant before removing isolation
Void or bubble : material can be directly added
Sealant retention :examine by attempting to dislodge by expelorer
If sealant dislodge :
Fissure inspected for Remaining debri :re etched…
Sealant pooled on distal margin created ledge tht should be removed
Sealant misplaced on inter proximal should be removed
Un polymerized layer(BPA):removed by pomice or rinsing
Occlusion Adjustment :
Yes:filled sealant and flowable composite
With:com finishing bur(high spead
,round bur,stone(low spead)
MC:centric stop on enamel
47
Periodic evaluation: It should be evaluated at every recall visit
Partial or complete loss of material failure
If only part of sealant remain : attempts can be made to dislodge with expelorer ,if it remain :no no need to remove this
MC :
5% -10% of sealant need to repaired or replaced yearly
Partialy or completely,discolored or defective old sealant should be removed
48
Troubleshooting sealant placement :
If sealant debonds upon immediate evaluation:
1. Debris remains on the fissure
Cleaning,re etching and apply material
2 .Saliva contaminated the enamel
Re etched ,dry and resealant
3. The tooth wasnot completely dry after the rinsing step
49

50