fine needle aspiration biopsy of renal mucinous tubular and spindle cell carcinoma: report of two...
TRANSCRIPT
Fine Needle Aspiration Biopsy ofRenal Mucinous Tubular andSpindle Cell Carcinoma:Report of Two CasesDeborah A. Marks-Jones, M.D.,1 Debra L. Zynger, M.D.,1
Anil V. Parwani, M.D., Ph.D.,1 and Guoping Cai, M.D.1,2*
Mucinous tubular and spindle cell carcinoma (MTSCC) is arare renal tumor. Here we report two cases of MTSCC whichwere initially evaluated by fine needle aspiration biopsy (FNAB)and followed by surgical resection of the tumors. The cytomor-phologic features of MTSCC were characterized by aggregatesof relatively uniform, predominantly oval to spindle cellsintermixed with abundant metachromatic myxoid matrix. Onlyrare epithelioid tumor cells with vacuolated cytoplasm werepresent. Immunohistochemically, the tumor cells were positivefor CK7, CK19, CD10, vimentin, E-cadherin, alpha-methyl CoAracemase, and negative for CK903 and CK20. EMA and car-bonic anhydrase IX immunoreactivity was seen in one of the twocases. Multiple chromosomal losses involving chromosomes 1, 2,17 and likely chromosome 7 were revealed by fluorescence insitu hybridization (FISH). These cytomorphologic, immunophe-notypic, and cytogenetic features were helpful for including thisentity in the differential diagnosis of renal cell carcinomas.Diagn. Cytopathol. 2010;38:51–55. ' 2009 Wiley-Liss, Inc.
Key Words: mucinous tubular and spindle cell carcinoma;kidney; fine needle aspiration biopsy; cytomorphology
Mucinous tubular and spindle cell carcinoma (MTSCC)
of the kidney is a rare, newly recognized low-grade re-
nal epithelial neoplasm.1–5 It has distinct histomorpho-
logic features, characterized by tightly packed small
elongated tubules embedded in pale mucinous matrix.
The epithelial cells that line the tubules are cuboidal but
often have spindle cell configuration. MTSCC seems to
have a favorable prognosis as compared to other renal
cell carcinomas.5 However, a significant sarcomatoid
component can be seen in some cases of MTSCC, which
may be associated with a more aggressive clinical
course.6–8
MTSCC, though histomorphologically distinct, may
impose a diagnostic challenge in small specimens such
as fine needle aspiration biopsy (FNAB). There have
been only four reported cases in the English literature
describing the cytomorphologic features of the tu-
mor.9–12 Here we report two cases of MTSCC of the
kidney which were initially evaluated by FNAB and
confirmed with surgical follow-up. Their cytomorpho-
logic, immunophenotypic, and cytogenetic features are
described.
Case Reports
Case 1
The patient is a 51-year-old man with a history of lung
carcinoma, status post right upper lobectomy, and liver
transplant for hepatitis C. Routine laboratory work
revealed an elevated creatinine (1.8 mg dL�1; normal
range 0.5–1.2 mg dL�1) and blood urea nitrogen (31 mg
dL�1; normal range 7–18 mg dL�1). Renal ultrasound
identified a 2.7 cm hypoechoic, solid mass in the mid
pole of the left kidney. Follow-up MRI confirmed the
presence of a 2.7-cm mass which was hypovascular,
rounded, and solid with possible hemorrhage. The patient
underwent an ultrasound-guided FNAB of this renal mass
with a 25-gauge spinal needle. The aspirates were
smeared and stained with standard Diff-Quik and Papani-
colaou techniques. Additional aspirates were fixed in 4%
formalin solution and processed for a cell block. A cyto-
logical diagnosis of renal cell carcinoma with clear cell
1Department of Pathology, University of Pittsburgh Medical Center,Pittsburgh, Pennsylvania
2Department of Pathology, Yale University School of Medicine,New Haven, Connecticut
*Correspondence to: Guoping Cai, M.D., Department of Pathology,Yale University School of Medicine, 430 Congress Avenue, P. O. Box208023, New Haven, CT 06520-8023.E-mail: [email protected]
Received 2 April 2009; Accepted 10 June 2009DOI 10.1002/dc.21151Published online 22 July 2009 in Wiley InterScience (www.
interscience.wiley.com).
' 2009 WILEY-LISS, INC. Diagnostic Cytopathology, Vol 38, No 1 51
features was rendered. Subsequent partial nephrectomy
was performed 5 weeks after the FNAB, which resulted
in a diagnosis of MTSCC with pathological staging of
pT1aNxMx. The patient was followed for 16 months and
imaging studies show no evidence of local recurrence or
distant metastasis.
Case 2
The patient is a 54-year-old man with a past medical his-
tory significant for nephrolithiasis. A CT scan revealed
slight enlargement of the left kidney as well as perineph-
ric stranding and hydronephrosis with multiple calculi
bilaterally. A 5-cm solid mass was revealed in the lower
pole of the left kidney. An ultrasound-guided FNAB of
the renal mass was performed with a 25-gauge spinal nee-
dle. The Diff-Quik and Papanicolaou stained smear slides
as well as cell block sections were available for cytologi-
cal evaluation. The final cytopathologic diagnosis was re-
nal cell carcinoma. One week later, the patient underwent
a laparoscopic left nephrectomy. Histopathologic exami-
nation demonstrated a MTSCC of the kidney with patho-
logical staging of pT1bNxMx. The patient was followed
for 3 years and 3 months and showed no evidence of
local recurrence or distant metastasis.
Pathologic Findings
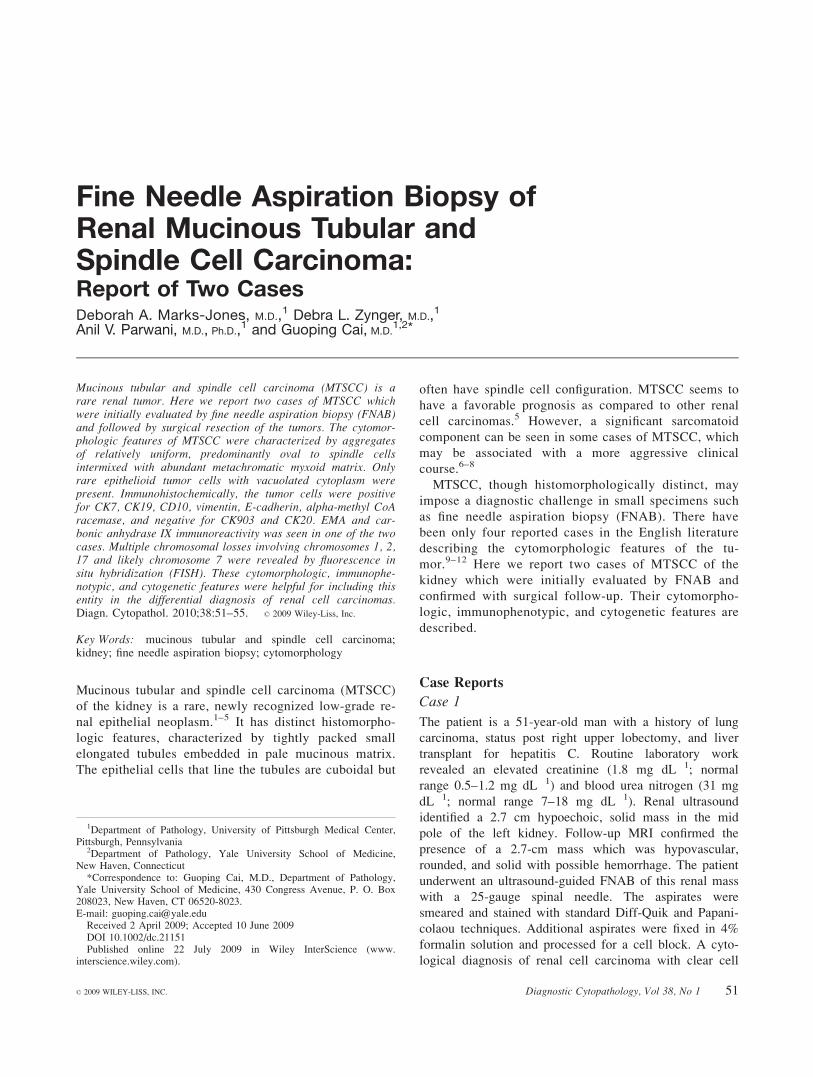
The aspirates for both cases were cellular and shared sim-
ilar cytomorphologic features. The aspirates revealed
loosely cohesive clusters of predominantly oval to spindle
tumor cells arranged in sheets, branching clusters or
pseudo-papillary aggregates (Fig. 1A). No definite fibro-
vascular cores were identified. Scattered tumor cells were
present singly, some as naked nuclei. Abundant amor-
phous, metachromatic mucinous/myxoid matrix was pres-
ent, often intimately intermingled with tumor cell clusters
(Fig. 1B). The matrix was magenta on the Diff-Quik stain
and pale blue on the Papanicolaou stain. The tumor cells
showed mild pleomorphism and had delicate cytoplasm
with indistinct cell borders and oval to spindle nuclei
with relatively smooth nuclear contours and conspicuous
Fig. 1. FNA cytomorphological features of mucinous tubular and spindle cell carcinoma of the kidney. The aspirates revealed clusters of epithelioid tospindle cells intermingled with metachromatic matrix (A: Diff-Quik, 3100). The tumor cells were predominantly oval to spindle shaped with blandcytomorphology (B: Papanicolaou, 3400; C: Diff-Quik, 3400). Few tumor cells had round nuclei and conspicuous cytoplasmic vacuoles (D: Diff-Quik, 3600). [Color figure can be viewed in the online issue, which is available at www.interscience.wiley.com.]
MARKS-JONES ET AL.
52 Diagnostic Cytopathology, Vol 38, No 1
Diagnostic Cytopathology DOI 10.1002/dc
nucleoli. Distinct fine cytoplasmic vacuoles were present
in some of the tumor cells (Fig. 1C). In addition, a few
clusters of tumor cells with vacuolated cytoplasm and
round nuclei were also present (Fig. 1D).
Grossly, the tumors were 2.6 and 6 cm in size, respec-
tively, well-circumscribed and confined within the kidney
without capsular invasion. Focal hemorrhage was identified
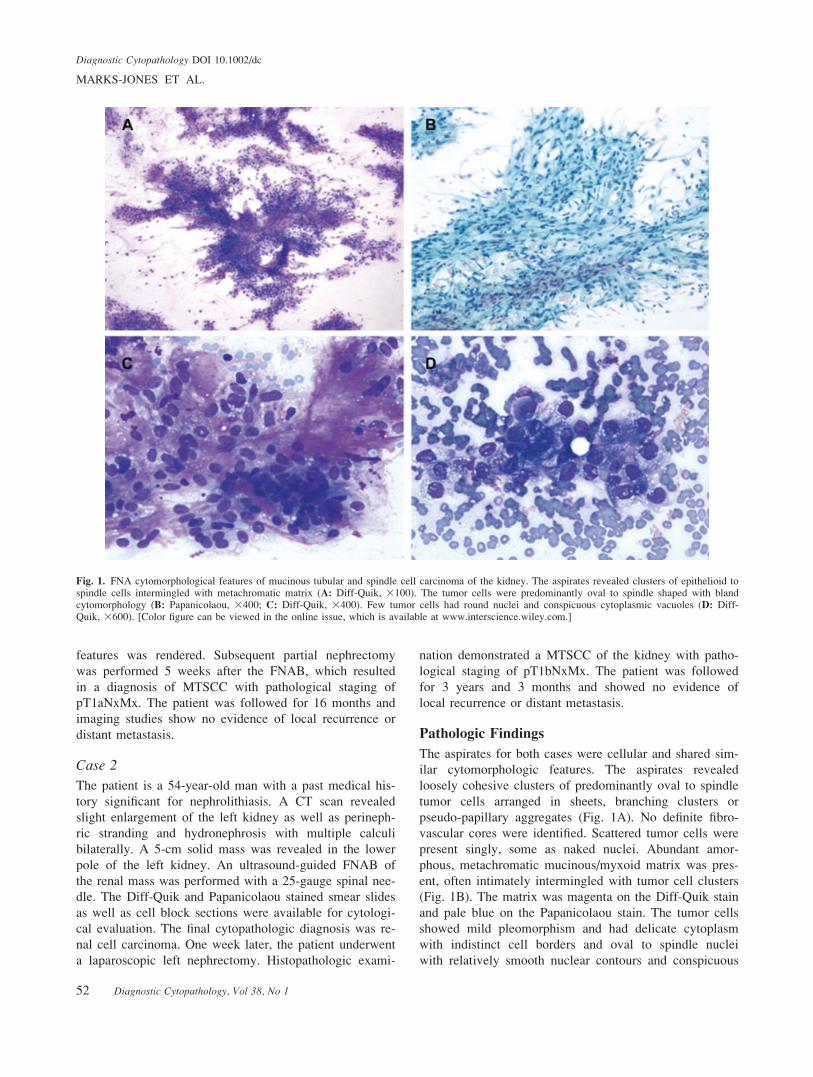
in case 2. On histopathologic examination, both tumors
showed tightly packed elongated tubules with intervening
pale mucinous/myxoid matrix (Fig. 2A). The cells lining
the tubules were mainly oval to spindle shaped with rela-
tively bland nuclear features (Fig. 2B). However, focal
areas with epithelioid cells were also present (Fig. 2C).
Immunohistochemical studies were performed on the
cell-block sections and/or resection specimens with appro-
priate negative and positive controls. In both cases, the tu-
mor cells were immunoreactive with CK7, CK19, CD10,
vimentin, E-cadherin, alpha-methyl CoA racemase
(P504S), and negative for CK20, CK903 (Table I). The
immunostains for epithelial membrane antigen (EMA)
and carbonic anhydrase IX (CA-9) were positive in case 2
but negative in case 1.
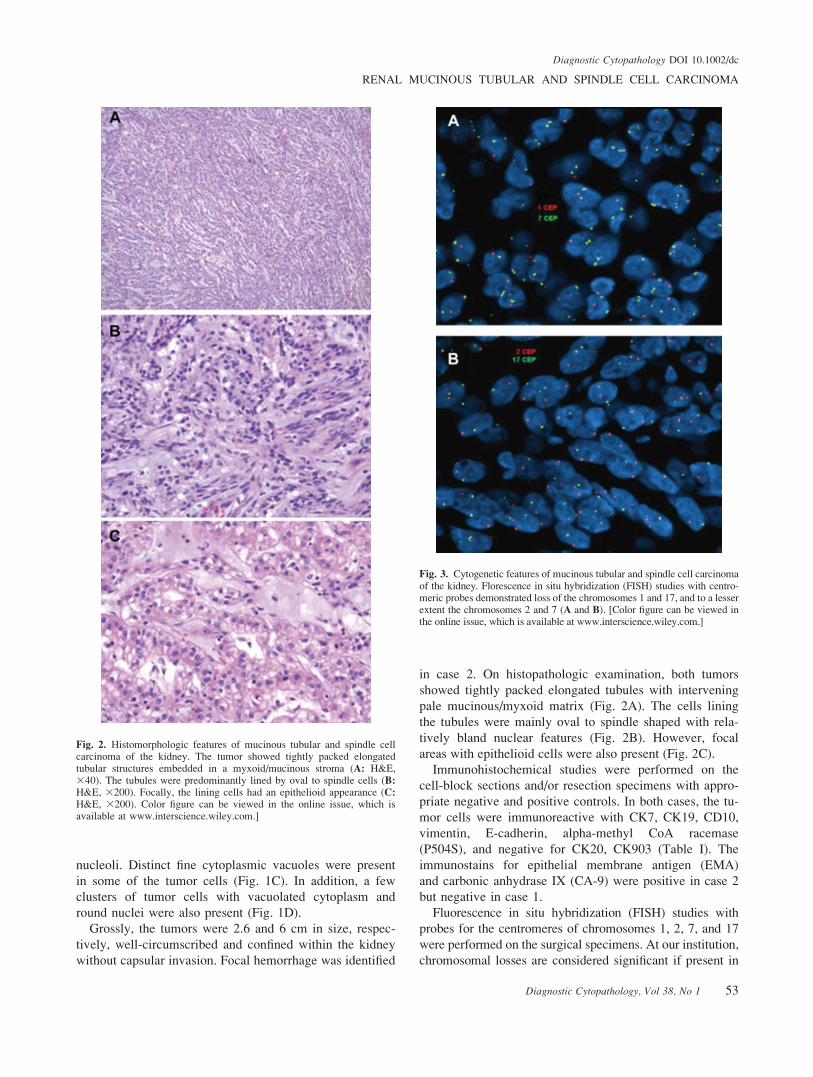
Fluorescence in situ hybridization (FISH) studies with
probes for the centromeres of chromosomes 1, 2, 7, and 17
were performed on the surgical specimens. At our institution,
chromosomal losses are considered significant if present in
Fig. 2. Histomorphologic features of mucinous tubular and spindle cellcarcinoma of the kidney. The tumor showed tightly packed elongatedtubular structures embedded in a myxoid/mucinous stroma (A: H&E,340). The tubules were predominantly lined by oval to spindle cells (B:H&E, 3200). Focally, the lining cells had an epithelioid appearance (C:H&E, 3200). Color figure can be viewed in the online issue, which isavailable at www.interscience.wiley.com.]
Fig. 3. Cytogenetic features of mucinous tubular and spindle cell carcinomaof the kidney. Florescence in situ hybridization (FISH) studies with centro-meric probes demonstrated loss of the chromosomes 1 and 17, and to a lesserextent the chromosomes 2 and 7 (A and B). [Color figure can be viewed inthe online issue, which is available at www.interscience.wiley.com.]
RENAL MUCINOUS TUBULAR AND SPINDLE CELL CARCINOMA
Diagnostic Cytopathology, Vol 38, No 1 53
Diagnostic Cytopathology DOI 10.1002/dc

greater than 30% of cells and are considered artifactual if
seen in less than 20% of cells. The losses are indeterminate
if present in 20–30% of cells. Both cases showed significant
losses of chromosomes 1, 2, and 17, present as monosomies.
Loss of chromosomes 7 was significant in one case but con-
sidered indeterminate in the other (Table II, Fig. 3).
Discussion
The cytomorphologic features of MTSCC in this report
were characterized by clusters of relatively bland cells
intermixed with abundant metachromatic matrix. The tu-
mor cells seemed to be predominantly oval to spindle
with mild pleomorphism, which are similar to those previ-
ously described in FNAB aspirates,10,12 but differ from
the other with predominant epithelioid cell morphology.9
Based on the cytomorphologic features, MTSCC should
be differentiated from other renal neoplasms (Table III).
When spindle cells are the predominant morphology, the
differential diagnosis includes sarcomatoid renal cell car-
cinoma and angiomyolipoma. Papillary renal cell carci-
noma might have foci of spindle cells, which may mimic
MTSCC.13 In cases with more epithelioid cells, other re-
nal cell carcinomas such as conventional (clear cell) and
papillary variants as well as collecting duct carcinoma are
among the differential. The tumor cells in these entities
often show cytological atypia in contrast to the bland
cytomorphology seen in MTSCC. Furthermore, none of
these entities have abundant metachromatic matrix
although the lack of matrix does not exclude MTSCC
from the differential diagnosis as mucin-poor MTSCC has
been described.14 In addition, conventional (clear cell) re-
nal cell carcinoma might contain a small amount of meta-
chromatic basal membrane-like material.
There are conflicting results regarding the immunophe-
notypic profile of MTSCC.1–3,15–19 The most consistent
findings are the immunoreactivity for vimentin, EMA,
and alpha-methyl CoA racemase.2,3,15,16,20 However, only
one of our two cases was positive for EMA. The staining
for high molecular weight cytokeratin seems to be incon-
sistent, as does reactivity for CK19.1,2,16,18 Both of our
specimens were immunoreactive for CK19 but not for
high molecular weight cytokeratin (CK903). CD10, which
has previously been shown to be positive only in a
minority of MTSCC, was positive in both of our tumors.
In addition, one of our cases showed immunoreactivity
for carbonic anhydrase IX, a maker for proximal tubular
origin. There is only one other study of carbonic anhy-
drase IX in MTSCC in which the authors found the tumor
to be negative.21 Overall, MTSCC appears to express the
markers for both proximal and distal renal tubules and
shows immunophenotypical overlap with papillary renal
cell carcinoma and collecting duct carcinoma.
Different subtypes of renal cell carcinomas may display
unique chromosomal abnormalities. Conventional (clear
cell) renal cell carcinoma frequently show loss of chromo-
somal 3p,22 while papillary renal cell carcinoma is charac-
terized by gains of chromosomes 7 and 17.23 In chromo-
phobe renal cell carcinoma and renal oncocytoma, multiple
chromosomal losses are often present.24,25 Several studies
using comparative genomic hybridization (CGH) or FISH
have demonstrated chromosomal abnormalities in
MTSCC.3,16,26,27 The most consistent findings are multiple
chromosomal losses. In Rakozy’s study of five MTSCC
cases,3 CGH revealed multiple losses of chromosomes 1, 4,
6, 8, 9, 13, 14, 15, and 22. However, there are conflicting
results regarding chromosomal gains, particularly for chro-
mosomes 7 and 17.3,16,27 Cossu-Rocca et al.28 examined 10
MTSCC cases using FISH and reported no gains of 7 or
17, directly disputing previous results.27 In the present
study using interphase FISH, chromosomal losses involv-
ing chromosomes 1, 2, 17, and likely chromosome 7 were
identified. The overall results of cytogenetic studies do not
support the suggestion that MTSCC is a variant of papil-
lary renal cell carcinoma.19
In summary, MTSCC has distinct cytomorphologic fea-
tures characterized by clusters of epithelioid to spindle
cells intermixed with abundant myxoid matrix. MTSCC is
immunophenotypically similar to papillary renal cell car-
Table I. Immunophenotypic Features of Mucinous Tubular and Spindle Cell Carcinoma of the Kidney
CK7 CK20 CK19 CK903 EMA CD10 VIM ECAD P504S CA-9
Case 1 + � + � � + + + + +Case 2 + � + � + + + + + �EMA, epithelial membrane antigen; VIM, vimentin; ECAD, E-cadherin; P504S, alpha-methyl CoA racemase; CA-9, carbonic anhydrase IX.
Table II. Cytogenetic Chromosomal Abnormalities of Mucinous Tubular and Spindle Cell Carcinoma of the Kidney
CEP1 CEP2 CEP7 CEP17
1 Copy 2 Copy 1 Copy 2 Copy 1 Copy 2 Copy 1 Copy 2 Copy
Case 1a 69/78 (88.5%) 9/78 (11.5%) 20/60 (33.3%) 38/60 (63.3%) 15/63 (23.8%) 43/63 (68.3%) 52/77 (67.5%) 24/77 (31.2%)Case 2 51/60 (85%) 9/60 (15%) 40/60 (66.7%) 20/60 (33.3%) 22/60 (36.7%) 38/60 (63.3%) 44/60 (73.3%) 16/60 (26.7%)
aRare tumor cells in case one showed trisomies of chromosomes 2, 7, and 17.CEP, centromere enumeration probe.
MARKS-JONES ET AL.
54 Diagnostic Cytopathology, Vol 38, No 1
Diagnostic Cytopathology DOI 10.1002/dc

cinoma but they differ in their cytogenetic abnormalities.
Increasing awareness of MTSCC and its cytomorphologic,
immunophenotypic, and cytogenetic features would be
helpful to render a more precise diagnosis.
References
1. Srigley JR, Eble JN, Grignon DJ, Hartwick RWJ. Unusual renal cellcarcinoma (RCC) with prominent spindle cell change possiblyrelated to the loop of Henle. Mod Pathol 1999;12:107A.
2. Parwani AV, Husain AN, Epstein JI, et al. Low-grade myxoid renalepithelial neoplasms with distal nephron differentiation. Hum Pathol2001;32:506–512.
3. Rakozy C, Schmahl GE, Bogner S, Storkel S. Low-grade tubular-mucinous renal neoplasms: Morphologic, immunohistochemical, andgenetic features. Mod Pathol 2002;15:1162–1171.
4. Eble JN. Mucinous tubular and spindle cell carcinoma and post-neuroblastoma carcinoma: Newly recognized entities in the renalcell carcinoma family. Pathology 2003;35:499–504.
5. Srigley JR. Mucinous tubular and spindle cell carcinoma. In: EbleJN, Sauter G, Epstein JI, Sesterhenn IA, editors. World health orga-nization classification of tumors. Tumors of the urinary system andmale genital organs. Lyon: IARC Press; 2004. p 40.
6. Pillay N, Ramdial PK, Cooper K, Batuule D. Mucinous tubular andspindle cell carcinoma with aggressive histomorphology—A sarco-matoid variant. Hum Pathol 2008;39:966–969.
7. Simon RA, di Sant’agnese PA, Palapattu GS, et al. Mucinous tubu-lar and spindle cell carcinoma of the kidney with sarcomatoid dif-ferentiation. Int J Clin Exp Pathol 2008;1:180–184.
8. Dhillon J, Amin MB, Selbs E, et al. Mucinous tubular and spindlecell carcinoma of the kidney with sarcomatoid change. Am J SurgPathol 2009;33:44–49.
9. Sun W, McGregor DK, Ordonez NG, et al. Fine needle aspirationcytology of a low grade myxoid renal epithelial neoplasm: A casereport. Acta Cytol 2005;49:525–529.
10. Ortega JA, Solano JG, Perez-Guillermo M. Cytologic aspect ofmucinous tubular and spindle-cell renal carcinoma in fine-needleaspirates. Diagn Cytopathol 2006;34:660–662.
11. Otani M, Shimizu T, Serizawa H, Nagashima Y. Mucinous tubularand spindle cell carcinoma of the kidney: Report of a case withimprint cytologic features. Acta Cytol 2006;50:680–682.
12. Owens CL, Argani P, Ali SZ. Mucinous tubular and spindle cellcarcinoma of the kidney: Cytopathologic findings. Diagn Cytopathol2007;35:593–596.
13. Argani P, Netto GJ, Parwani AV. Papillary renal cell carcinomawith low-grade spindle cell foci: A mimic of mucinous tubular andspindle cell carcinoma. Am J Surg Pathol 2008;32:1353–1359.
14. Fine SW, Argani P, DeMarzo AM, et al. Expanding the histologicspectrum of mucinous tubular and spindle cell carcinoma of the kid-ney. Am J Surg Pathol 2006;30:1554–1560.
15. Hes O, Hora M, Perez-Montiel DM, et al. Spindle and cuboidalrenal cell carcinoma, a tumour having frequent association withnephrolithiasis: Report of 11 cases including a case with hybridconventional renal cell carcinoma/spindle and cuboidal renal cellcarcinoma components. Histopathology 2002;41:549–555.
16. Ferlicot S, Allory Y, Comperat E, et al. Mucinous tubular and spin-dle cell carcinoma: A report of 15 cases and a review of theliterature. Virchows Arch 2005;447:978–983.
17. Skinnider BF, Folpe AL, Hennigar RA, et al. Distribution ofcytokeratins and vimentin in adult renal neoplasms and normal renaltissue: Potential utility of a cytokeratin antibody panel in thedifferential diagnosis of renal tumors. Am J Surg Pathol 2005;29:747–754.
18. Paner GP, Srigley JR, Radhakrishnan A, et al. Immunohistochemi-cal analysis of mucinous tubular and spindle cell carcinoma andpapillary renal cell carcinoma of the kidney: Significant immuno-phenotypic overlap warrants diagnostic caution. Am J Surg Pathol2006;30:13–19.
19. Shen SS, Ro JY, Tamboli P, et al. Mucinous tubular and spindlecell carcinoma of kidney is probably a variant of papillary renalcell carcinoma with spindle cell features. Ann Diagn Pathol 2007;11:13–21.
20. Molinie V, Balaton A, Rotman S, et al. Alpha-methyl CoA race-mase expression in renal cell carcinomas. Hum Pathol 2006;37:698–703.
21. Gupta R, Balzer B, Picken M, et al. Diagnostic implications of tran-script factor PAX 2 protein and transmembrane enzyme complexcarbonic anhydrase IX immunoreactivity in adult renal epithelialneoplasms. Am J Surg Pathol 2009;33:241–247.
22. Kovacs G, Erlandsson R, Boldog F, et al. Consistent chromosome3p deletion and loss of heterozygosity in renal cell carcinoma. ProcNatl Acad Sci USA 1988;85:1571–1575.
23. Jiang F, Richter J, Schraml P, et al. Chromosomal imbalances inpapillary renal cell carcinoma: Genetic differences between histo-logical subtypes. Am J Pathol 1998;153:1467–1473.
24. Speicher MR, Schoell B, du Manoir S, et al. Specific loss ofchromosomes 1, 2, 6, 10, 13, 17, and 21 in chromophobe renal cellcarcinomas revealed by comparative genomic hybridization. Am JPathol 1994;145:356–364.
25. Brown JA, Takahashi S, Alcaraz A, et al. Fluorescence in situhybridization analysis of renal oncocytoma reveals frequent loss ofchromosomes Y and 1. J Urol 1996;156:31–35.
26. Srigley JR, Kapusta L, Reuter V, et al. Phenotypic, molecular, andultrastructural studies of a novel low-grade renal epithelial neoplasmpossibly related to the loop of Henle. Mod Pathol 2002;15:182A.
27. Brandal P, Lie AK, Bassarova A, et al. Genomic aberrations inmucinous tubular and spindle cell renal cell carcinomas. Mod Pathol2006;19:186–194.
28. Cossu-Rocca R, Eble JN, Delahunt B, et al. Renal mucinous tubularspindle carcinoma lacks the gains of chromosomes 7 and 17 andlosses of chromosome Y that are prevalent in papillary renal cellcarcinoma. Mod Pathol 2006;19:488–493.
Table III. Differential Diagnosis of Mucinous Tubular and Spindle Cell Carcinoma From Other Renal Cell Carcinomas
Cytomorophology Immunophenotype Cytogenetics
MTSCC Round, oval, spindle cells, mildpleomorphism, abundant matrix
EMA+, Vim+, P504S+, CK7+, CD10+/� Loss of multiple chromosomes
Sarcomatoid RCC Oval, spindle cells, atypia, no matrix EMA+/�, P504S�, CD10+/� UnknownClear cell RCC Round cells, variable atypia, rare matrix EMA+, Vim+, CD10+,
CK7-, P504S�, CA-9+Chromosome 3p deletion
Papillary RCC Round cells, variable atypia, no matrix EMA+, Vim+, CD10+/�, CK7+, P504S+ Gain of chromosomes 7 and 17Collecting ductcarcinoma
Round cells, atypia, no matrix EMA+/�, Vim+, CD10�,CK7+/�, P504S�, UEA-1+
Unknown
MTSCC, mucinous tubular and spindle cell carcionoma; RCC, renal cell carcinoma; EMA, epithelial membrane antigen; VIM, vimentin; P504S,alpha-methyl CoA racemase; CA-9, carbonic anhydrase IX; UEA-1, Ulex europaeus agglutinin-1.
RENAL MUCINOUS TUBULAR AND SPINDLE CELL CARCINOMA
Diagnostic Cytopathology, Vol 38, No 1 55
Diagnostic Cytopathology DOI 10.1002/dc