filariasis and fascioliasis
TRANSCRIPT

FILARIASIS AND FASCIOLIASIS
ANUBHAV AGRAWAL
GROUP 514
OUTLINE OF PRESENTATION
• Introduction
• Epidemiology
• Morphology
• Mode of transmission
• Life cycle
• Pathogenesis
• Signs and symptoms
• Laboratory diagnosis
• Prevention and Control

FILARIASIS

INTRODUCTION
• Filariasis is the pathological condition caused by infection of filarial nematodes transmitted by different vectors.
• Infection occurs in blood vessels, lymphatic system , connective tissues and serous cavities of man.
• Disease of tropical warm lands.
• Caused by different worms and are characterized by different clinical features.
EPIDEMIOLOGY
• Lymphatic filariasis is caused by infection with nematodes of the family Filarioidea: 90% of infections are caused byWuchereria bancrofti and most of the remainder by Brugia malayi.
• Humans are the exclusive host of infection with W. bancrofti. Although certain strains of B. malayi can also infect some animal species (felines and monkeys), the life cycle in these animals generally remains epidemiologically distinct from that in humans.
• The major vectors of W. bancrofti are mosquitoes of the genus Culex (in urban and semi-urban areas), Anopheles (in rural areas of Africa and elsewhere) and Aedes(in islands of the Pacific).


MORPHOLOGY
Wuchereria bancrofti
• Adult worm are long hair like transparent nematodes, filariform in shape with tapering ends.
• Male measures 2.5 to 4 cm in length by 0.1 mm in thickness and female measures 8 to 10 cm in length and 0.3 mm in thickness.
• Tail end of male worm is curved ventrally while that of female worm is narrow and abruptly pointed.

Brugia malayi
• The adult females of B malayiresembles to W. bancrofti but the adult males differ .
Brugia timori
• Similar to B. malayi .
Loa loa
• The male measures 3 cm in length and 0.35 mm in breadth . The female measures 6 cm in length by 0.5 mm in breadth.

MODE OF TRANSMISSION
• Transmitted by vectors
• Bancroftian filariasis is transmitted by Culex, Aedes and Anopheles mosquito.
• Malayan filariasis is transmitted by Anopheles and Mansonia spp.
• Loiasis is transmitted by Tabonid or horse fly of Chrysops spp.
• When the vectors suck blood from infected person, the microfilariae reaches the of vector , which then enters the thorax where by development of larvae takes place. Infective larvae enters the mouth parts and are shed on the skin of healthy human host when the vectors takes blood meal.
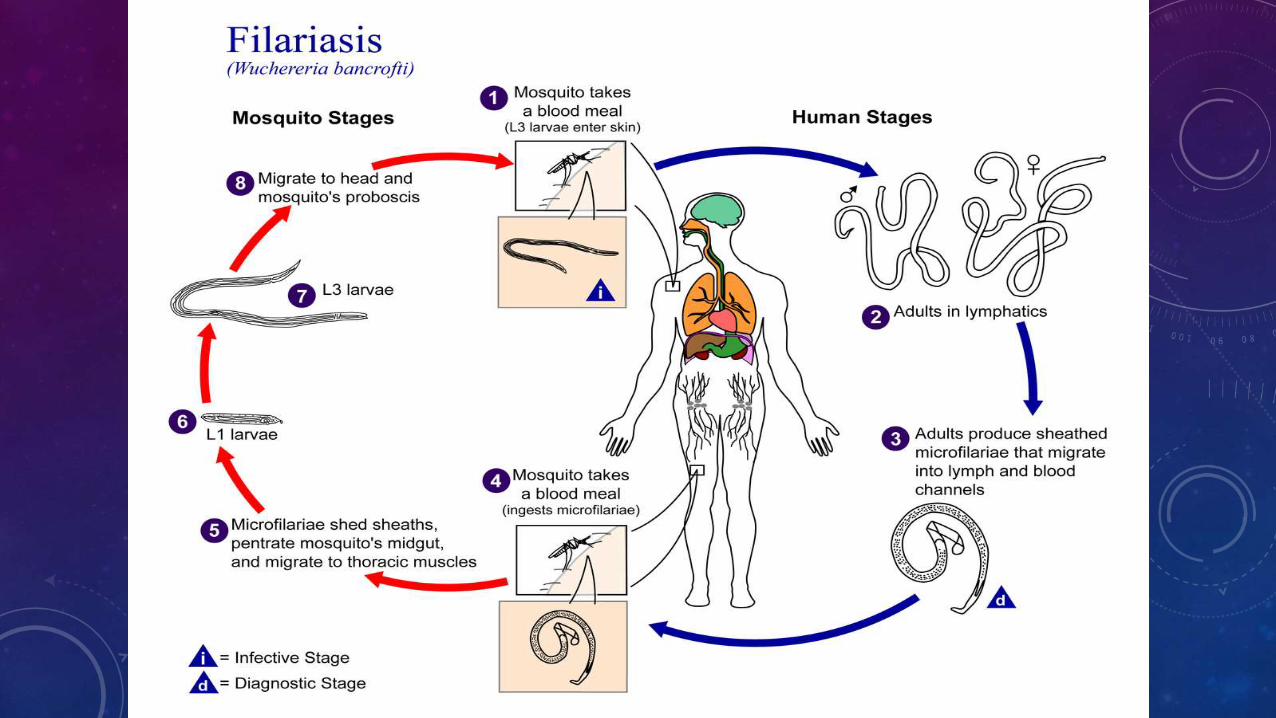
Life cycle of Wuchereria bancrofti

SIGNS AND SYMPTOMS
• The most spectacular symptom of lymphatic filariasis is elephantiasis, a stage 3 lymphedema with thickening of the skin and underlying tissues. This was the first mosquito-borne disease to be discovered. Elephantiasis results when the parasites lodge in the lymphatic system and cause blockages to the flow of lymph. Infections usually begin in childhood.
• The skin condition the disease causes is called "elephantiasis tropica" (also known as "elephantiasis arabum").
• Elephantiasis mainly affects the lower extremities; the ears, mucous membranes, and amputation stumps are affected less frequently. However, various species of filarial worms tend to affect different parts of the body: Wuchereria bancrofti can affect the arms, breasts, legs, scrotum, and vulva (causing hydrocele formation), while Brugia timori rarely affects the genitals. Those who develop the chronic stages of elephantiasis are usually amicrofilaraemic and often have adverse immunological reactions to the microfilariae as well as the adult worms.

LABORATORY DIAGNOSIS
• Samples includes :
Peripheral blood , Chylous urine, Exudate of lymph varix, Hydrocele fluid,Lymph node biopsy, skin specimen
• Microscopic examination : It deals with the detection of microfilariae.
• Macroscopic examination : detection of adult worm ( lymph node biopsy )
• Haematological examination : eosoinophilic count is done.
• Serological test : Complement fixation test is performed.
• Intradermal test : immediate hypersensitivity test. Filarial antigen is injected on skin. After 30 minutes a weal over 2 cm appears.

PREVENTION AND CONTROL
Prevention :
• Destruction of breeding sites of vectors.
• Using bed nets while sleeping.
• Applying repellant creams on skin.
Control
• Treatment : diethylcarbamazine against filarial worms. Albendazole against infective larvae. Arsenical preparation against adult worm.
• Correction of lymphatic defect through surgery.
• Surveillance of disease in endemic areas.

PICTURES



FASCIOLIASIS
• Fasciolosis (also known as fascioliasis, fasciolasis, distomatosis and liver rot) is a parasitic worm infection caused by the common liver fluke Fasciola hepatica as well as by Fasciola gigantica.
• The disease is a plant-borne trematode zoonosis, and is classified as a neglected tropical disease (NTD).
• It affects humans, but its main host is ruminants such as cattle and sheep.


EPIDEMIOLOGY
• Human and animal fasciolosis occurs worldwide. While animal fasciolosis is distributed in countries with high cattle and sheep production, human fasciolosis occurs, excepting Western Europe, in developing countries. Fasciolosis occurs only in areas where suitable conditions for intermediate hosts exist.
• Studies carried out in recent years have shown human fasciolosis to be an important public health problem. Human fasciolosis has been reported from countries in Europe, America, Asia, Africa and Oceania. The incidence of human cases has been increasing in 51 countries of the five continents. A global analysis shows that the expected correlation between animal and human fasciolosis only appears at a basic level. High prevalences in humans are not necessarily found in areas where fasciolosis is a great veterinary problem. For instance, in South America, hyperendemics and mesoendemics are found in Bolivia and Peru where the veterinary problem is less important, while in countries such as Uruguay, Argentina and Chile, human fasciolosis is only sporadic or hypoendemic.



MORPHOLOGY
• Fasciola hepatica is one of the largest flukes of the world, reaching a length of 30 mm and a width of 13 mm (Fasciolagigantica, on the other hand, is even bigger and can reach up to 75 mm). It is leaf-shaped, pointed at the back (posteriorly) and wide in the front (anteriorly). The oral sucker is small but powerful and is located at the end of a cone-shape projection at the anterior end. The acetabulum is a larger sucker than the oral sucker and is located at the anterior end.


SIGNS AND SYMPTOMS
The course of fasciolosis in humans has 4 main phases:
Incubation phase: from the ingestion of metacercariae to the appearance of the first symptoms; time period: few days to 3 months; depends on number of ingested metacercariae and immune status of host
Invasive or acute phase: fluke migration up to the bile ducts. This phase is a result of mechanical destruction of the hepatic tissue and the peritoneum by migrating juvenile flukes causing localized and or generalized toxic and allergic reactions.[11] The major symptoms of this phase are:
• Fever: usually the first symptom of the disease; 40–42 °C (104–108 °F)
• Abdominal pain
• Gastrointestinal disturbances: loss of appetite, flatulence, nausea, diarrhea
• Urticaria
• Respiratory symptoms (very rare): cough, dyspnoea, chest pain, hemoptysis
• Hepatomegaly and splenomegaly
• Ascites
• Anaemia
• Jaundice
Latent phase: This phase can last for months or years. The proportion of asymptomatic subjects in this phase is unknown. They are often discovered during family screening after a patient is diagnosed.[5]
Chronic or obstructive phase


TREATMENT
• Several drugs are effective for fascioliasis, both in humans and in domestic animals. The drug of choice in the treatment of fasciolosis is triclabendazole, a member of the benzimidazole family of anthelmintics. The drug works by preventing the polymerization of the molecule tubulin into the cytoskeletal structures, microtubules. Resistance of F. hepatica to triclabendazole has been recorded in Australia in 1995 and Ireland in 1998.
• Praziquantel treatment is ineffective. There are case reports of nitazoxanide being successfully used in human fasciolosis treatment in Mexico. There are also reports of bithionol being used successfully.
• More recently, Mirazid, an Egyptian drug made from myrrh, has been investigated as an oral treatment of trematode-caused ailments including fascioliasis.
• Nitazoxanide has been found effective in trails, but is currently not recommended. The life cycle includes freshwater snails as an intermediate host of the parasite.
