fibrinolytic activity inhibition of plasminogen activation
TRANSCRIPT

Ada Medica Scandinavica. Vol. 172, fasc. 6, 1962
From the Laboratory, Medical Department F (Head: F. Wulff, M. D.), Copenhagen County Hospital, Hellerup, Denmark
Fibrinolytic Activity
Inhibition of Plasminogen Activation
BY
JOHS. GORMSEN
In recent years fibrinolytic phenomena have been studied with growing interest. Some authors suggest that an impaired fibrinolytic mechanism may underly the pathogenesis of atherosclerosis. Fibrin deposition is an integral part of all acute inflammatory reactions and the fibrinolytic process is a basis repair mechanism operative throughout the organism (1).
Three types of assay methods for determination of the active proteolytic enzyme plasmin have been used; fibrin- olytic assays, proteolytic assays and assays utilizing synthetic substrates such as lysine and arginine esters. Fibrin is the most physiological substrate, and fibrin- olytic assays have proven most sensitive but least reproducible. Although the fibrin plate method does constitute a valuable assay method for plasminogen activator and plasmin, it suffers from some disadvantages such as the long incubation period required and its in- efficacy in demonstrating reduced ac- tivity. Submitted for publication April 30, 1962. 42 --623003, Acta M e d . Scand. Vol. 172.
In 1961 Nilsson et al. ( 5 ) described a patient who had had since childhood progressive symptoms of massive venous thrombosis. Coagulation studies showed a high content of serum components in- hibiting the activation of plasminogen by streptokinase and urokinase. Further they described a method €or deter- mination of the inhibitor. The inhibiting component was found in the fraction containing a,-globulins, it was not di- alysable and not adsorbed to BaSO,. I t was destroyed by heating at 56" C for 30 minutes. The antiplasmin activity and the trypsin-inhibiting activity of the patient's serum were also increased but could be distinguished clearly from the actual inhibitor, by the method de- scribed.
The aim of the present work has been to determine the concentration of these serum inhibitors in some patients in whom the fibrinolytic activity might be impaired, to compare the results with those obtained by the plate method, and to examine whether any relation-
65 7

658 JOHS. GORMSEN
90
a0
70
bo
50
40
30
20
10
C U T L E I S IN MIN.
'
'
r 90
80
'10
(0
SO
40
30
20
10
I 12.5 25 SO
SEllVll CONC. IN PER CEWF.
Fig. 1. Fibrinolytic activity measured by Nils- son's method in 33 patients with uncomplicated atherosclerosis. Clot-lysis above 100 min. is not marked out (5 patients, serum concentration 50 yo). Normal range between the solid lines.
ship between fibrinolytic activity and heparin-resistance in vitro could be dem- onstrated.
Methods Serum inhibitors of plasminogen activation.
Nilsson's technique ( 6 ) was followed in all details and identical preparations of fibrinogen, thrombin, urokinase, strep- tokinase, plasminogen, buffers and so on were used.
CLOT LEIS IN m.
t
12.5 25 SERUM CONC. IN PER CENT.
SO
Fig. 2. Fibrinolytic activity measured by Nils- son's method in 23 patients with acute heart infarction. The values given are from the day of admission. Clot-lysis above 100 min. is not marked out (10 patients, serum concentration 50 %). Normal range between the solid lines.
The jibrin plate method assay according t o Astrup and Mullertz (2) was carried out by 0. Storm.
Fibrinogen. The concentration was es- timated spectrophotometrically.
Heparin-tolerance test was carried out ac- cording to the principles earlier described (3).
Results Normal controls
Determination of serum inhibitors ac- cording to Nilsson et al. ( 5 ) was carried

FIBRINOLYTIC ACTIVITY
u -
5 0 -
co
30.
10
10
659
-
.
.
out in 75 normal controls aged 25-70 years with three concentrations of serum: 12.5,25 and 50 yo. As controls two blanks were used in which serum was replaced by 0.9 yo saline and a solution (0.1 yo) of epsilon-aminocaproic acid respectively. Only the results obtained by urokinase (0.05 mg/ml) are given. With the serum concentration of 12.5 yo the clot-lysis took 12.5 min. f 1.5 min. and with the 25 yo serum the clot-lysis took 3 1.4 min. f 7.2 min. Twenty determinations on the same batch gave clot-lysis times of 12 min. f 0.4 min. and 243/4 min. f 0.6 min. with 12.5 and 25 yo respectively. The results in the same person under standard con- ditions are extremely constant. No cor- relation with age or sex was demon- strated. No distinct changes after fatty meals were recorded.
Ron-complicated atherosclerosis The values found in 33 patients
suffering from atherosclerosis (not dia- betic, no acute thrombosis, no necrosis) are shown in fig. 1. The inhibitor-con- centration was not high.
Acute heart infarction The values found at the admission in
23 patients are shown in fig. 2. About one third of the patients had values within the normal range. The 4 patients who had the most retarded clot-lysis got a thromboembolic complication, and 3 of them died, the autopsy revealing a mural thrombosis in the heart. One of them died from a ruptured heart. In one-third of the patients the inhibitor concentration seemed rather low, and the clot-lysis was as quick as in patients suffering from hepatic cirrhosis with latent or manifest haemorrhagic diathesis. In diabetic patients the clot-lysis generally was retarded. During the following weeks
CLOT LYSIS IN Hm.
80
n i A
12.5 25 50 SERUM CONC. IN PER CENT.
Fig. 3. Fibrinolytic activity measured by Nils- son’s method in 29 patients with hepatic cirrhosis. Values above 100 min. are not marked out (5 patients, serum concentration 50 %). A = treated with caproic acid. x = treated with steroids.
the clot-lysis generally became acceler- ated except in some diabetics and in patients who got thromboembolic or pyogenic complications and in certain others. Treatment with phenylindane- dione did not influence the results.
Hepatic cirrhosis The values found in 29 patients suf-
fering from hepatic cirrhosis are shown in fig. 3. In most cases the diagnosis was verified by biopsy. Otherwise the diag-

660
CLOTLIS~S , in min
I30
I ao
110
100
80
LO
’(0
20
JOHS. GORMSEN
5ERUM UJNC SO% S E R W I COUC. I1 5 X
I 2
Fig. 4. Fibrinolytic activity measured by Nilsson’s method in a patient with cirrhosis, subjected to a porta-caval shunt operation. Lysis-time before operation rather short. It shortened during and after the operation. The patient bled heavily. Treatment with &-aminocaproic acid (6 g intravenously) or human albumin increased the inhibitor concentration and stopped the bleeding temporarily.
nosis was based on the usual biochemical tests including a pathological bromsul- phalein-retention. In most patients the clot-lysis was enhanced. Four patients under long-term treatment with steroids repeatedly had normal values, and in 3 cases treated with c-aminocaproic acid perorally the inhibitor concentration was high. Only in one untreated patient was the clot-lysis retarded. She died and at the autopsy a portal thrombosis was found.
In fig. 4 the values are shown for a patient subjected to a porta-caval shunt operation. The clot lysed quickly before the operation, and during and im- mediately after the operation the activity was enhanced. The patient bled heavily. Treatment with human albumin or 8-aminocaproic acid markedly increased the inhibitor concentration in the serum
and the bleeding temporarily stopped. Steroids had a similar but smaller effect.
In four patients with acute infectious hepatitis, in seven with obstructive jaundice, in 2 with cholangitis and in 4 with malignant diseases in the liver a normal or retarded clot-lysis was found.
Malignant neoplasms The values found in 19 patients
suffering from different types of malig- nant diseases are shown in fig. 5. It is well known that pancreatic cancer is often complicated with phlebothrombosis whereas prostatic cancer may be com- plicated with a haemorrhagic diathesis.
In 3 patients with pancreatic cancer (no jaundice) and in one with rectal cancer the clot-lysis was very retarded. No thromboembolic complication was demonstrated. In two patients with

FIBRINOLYTIC ACTIVITY 66 1
cLm
90
80
70
Go
50
90
30
YSIS IN MRI.
so
10
12.5 25 SERUM COIIC. IN PER CENT.
Fig. 5. Fibrinolytic activity measured by Nils- son's method in 19 patients suffering from malig- nant diseases. Values above 100 min. are not marked out (10 patients, serum concentration 50 "/6).
prostatic cancer and in one with pul- monary cancer the clot-lysis was very quick. These patients did not bleed.
No relationship between the values found and the presence of metastases was demonstrated.
Some other diseases with a high inhibitor content A slight retarded clot-lysis was found
in patients with diabetes (14) even before vascular complications were dem- onstrated, in some patients with acute
I . . . . . . . . . . . . . . . . . I
Fig. 6 . Inhibitor concentration and heparin resist- ance after an operation. The concentration of the serum inhibitor and the heparin resistance increased postoperatively.
x-x = heparin tolerance test.
IS mn
-. = clot-lysis.
venous or arterial thrombotic compli- cations (1 3) , with pulmonary infarction (4), with papillitis necroticans in the kidneys, the retardation being severe (3), with gangrene (4), and moreover in patients with acute cholecystitis (3), cystopyelitis (2), arteritis (1) and in patients treated with steroids for tem- poral arteritis (2) or pancytopenia (2).
Fifty surgical patients were inves- tigated. About 30 yo and especially patients undergoing extensive surgery exhibited a very retarded clot-lysis during the first 5(-10) days after the operation (fig. 6).
Some other diseases with a low inhibitor con- centration A low concentration of the actual
inhibitor was found in 4 patients with thrombocytopenia (less than 5,000 platelets/mm3), in 2 patients with acute myeloblastic leukaemia and in 3 patients who bled copiously after prostatectomy for benign prostatic hypertrophy (2) and one after thyroidectomy.
662 JOHS. GORMSEN
1 2 3 1 ( 5 6 ’ DRYS
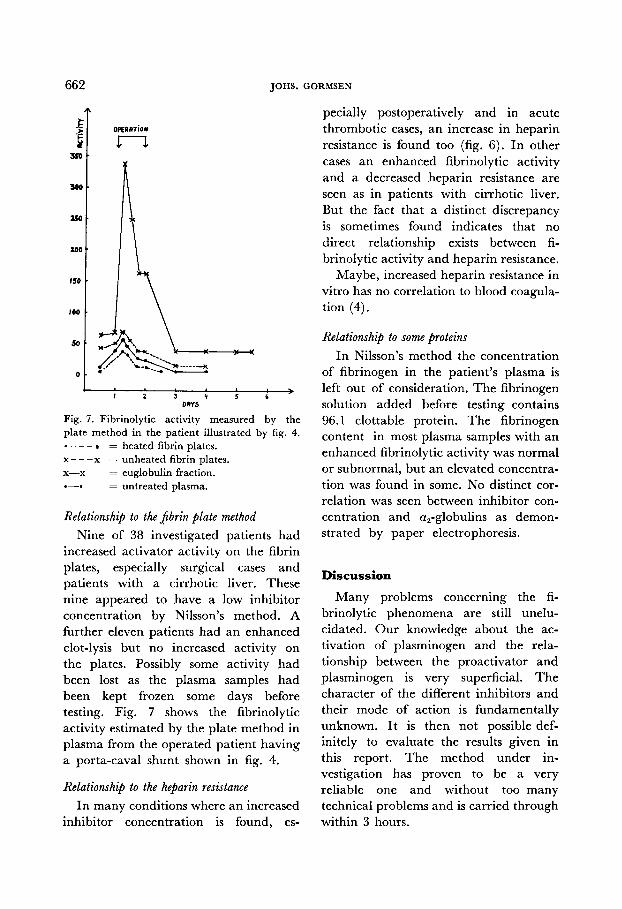
Fig. 7. Fibrinolytic activity measured by the plate method in the patient illustrated by fig. 4. - - - : heated fibrin plates.
x - - -x = unheated fibrin plates. x-x = euglobulin fraction. 0-0 = untreated plasma.
Relationship to the JZbrin plate method Nine of 38 investigated patients had
increased activator activity on the fibrin plates, especially surgical cases and patients with a cirrhotic liver. These nine appeared to have a low inhibitor concentration by Nilsson’s method. A further eleven patients had an enhanced clot-lysis but no increased activity on the plates. Possibly some activity had been lost as the plasma samples had been kept frozen some days before testing. Fig. 7 shows the fibrinolytic activity estimated by the plate method in plasma from the operated patient having a porta-caval shunt shown in fig. 4.
Relationship to the heparin resistance In many conditions where an increased
inhibitor concentration is found, es-
pecially postoperatively and in acute thrombotic cases, an increase in heparin resistance is found too (fig. 6). In other cases an enhanced fibrinolytic activity and a decreased heparin resistance are seen as in patients with cirrhotic liver. But the fact that a distinct discrepancy is sometimes found indicates that no direct relationship exists between fi- brinolytic activity and heparin resistance.
Maybe, increased heparin resistance in vitro has no correlation to blood coagula- tion (4).
Relationship to some proteins In Nilsson’s method the concentration
of fibrinogen in the patient’s plasma is left out of consideration. The fibrinogen solution added before testing contains 96.1 clottable protein. The fibrinogen content in most plasma samples with an enhanced fibrinolytic activity was normal or subnormal, but an elevated concentra- tion was found in some. No distinct cor- relation was seen between inhibitor con- centration and a,-globulins as demon- strated by paper electrophoresis.
Discussion
Many problems concerning the fi- brinolytic phenomena are still unelu- cidated. Our knowledge about the ac- tivation of plasminogen and the rela- tionship between the proactivator and plasminogen is very superficial. The character of the different inhibitors and their mode of action is fundamentally unknown. It is then not possible def- initely to evaluate the results given in this report. The method under in- vestigation has proven to be a very reliable one and without too many technical problems and is carried through within 3 hours.

FIBRINOLYTIC ACTIVITY 663
In some patients a fascinating cor- relation between the concentration of the inhibitory component and the clinical picture from a haemostatic point of view was obvious, especially postoperatively. In these patients the heparin resistance generally accorded with the content of inhibitors again from a haemostatic point of view. I t might be surprising that no increase in the inhibitor con- centration was found in patients with atherosclerosis. But this finding does not pcrmit any consequent conclusion about fibrinolytic activity and atherosclerosis. The different values found in patients with acute heart infarction might be of importance from a prognostic and a therapeutic point of view.
In 7 patients with abnormal bleeding tendency and a quick clot-lysis the bleeding stopped promptly after treat- ment with aminocaproic acid. Similar results were obtained by Nilsson et al. (6).
Summary
A component in serum inhibiting the activation of plasminogen with urokinase has been estimated in 75 normal controls and in 211 patients by the method of Nilsson et al. In some acute thrombotic cases and postoperatively, especially after extensive surgery, the inhibitor content
was high. In atherosclerosis no increase in the concentration was found. In acute heart infarction the concentration varied between distinct increase and decrease. In most cases of hepatic cirrhosis the clot-lysis was quick. In patients with cellular destruction the clot-lysis most often was retarded. When a high activator content was found by the fibrin plate method the concentration of the in- hibitory component was estimated as low. In many patients a distinct relation between inhibitor concentration and heparin resistance was found. But this relationship was not precise. Increased heparin resistance in vitro might depend on proteins without any known clotting activity.
References 1. ASTRUP, T. : Connective tissue, thrombosis
and atherosclerosis. Academic Press, N. Y. and London 1959, p. 223.
2. ASTRUP, T. and MULLERTZ, S.: Arch. Bio- chem. 40: 346, 1952.
3. GORMSEN, J.: Brit. J. Haemat. 5: 257, 1959. 4. GORMSEN, J.: Proc. 8. Europ. SOC. Haemat.,
5. NILSSON, I. M., BJORKMAN, S. E. and ANDERS- SON, L.: Acta med. Scand. 170: 487, 1961.
6. NILSSON, I. M., KROOK, H., STERNBY, N.-H., SODERBERG, E. and SODERSTROM, N.: Acta med. Scand. 169: 323, 1961 and Scand. J. Clin. Lab. Invest. 14: 138, 1962.
1962, p. 447.