female hormones and contraception
TRANSCRIPT
FEMALE HORMONES AND CONTRACEPTION
RESIDENT: FARIHA FATIMA
JR-2
Scheme Of Presentation:
Introduction Estrogens Selective Estrogen Receptor Modulator Progestins Anti-Progestins Selective Progesterone Receptor Modulator Contraception
Introduction
Estrogens and progestins are steroid hormones with numerous physiological
actions.
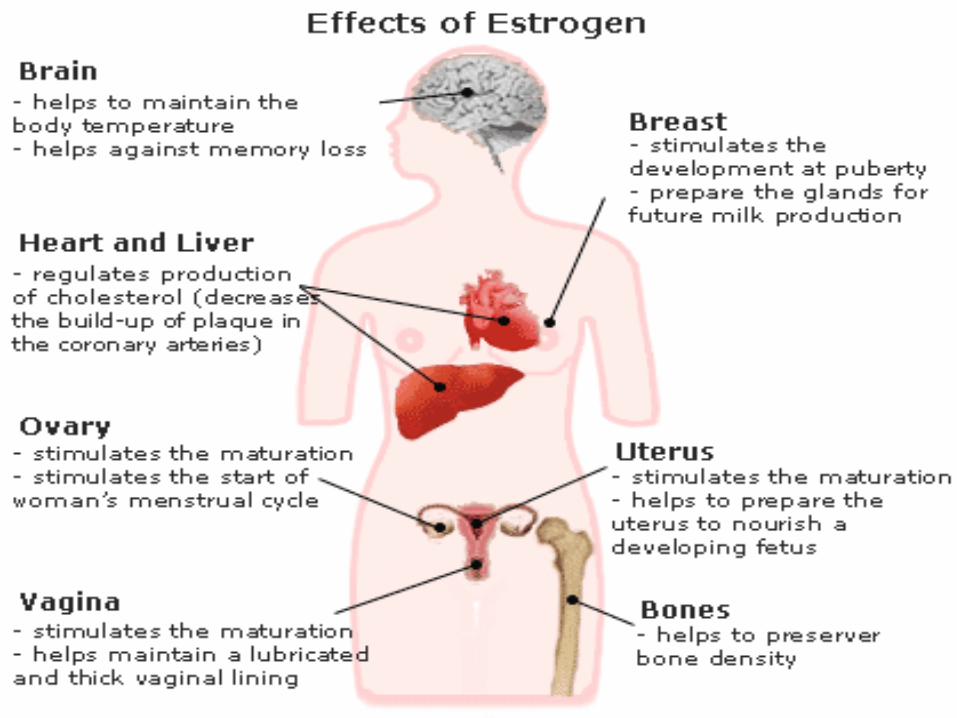
In women, these include developmental effects, control of ovulation, cyclical
preparation of the reproductive tract for fertilization and implantation, and
metabolic actions.
Estrogens also have important actions in males, including effects on bone,
spermatogenesis, and behavior.

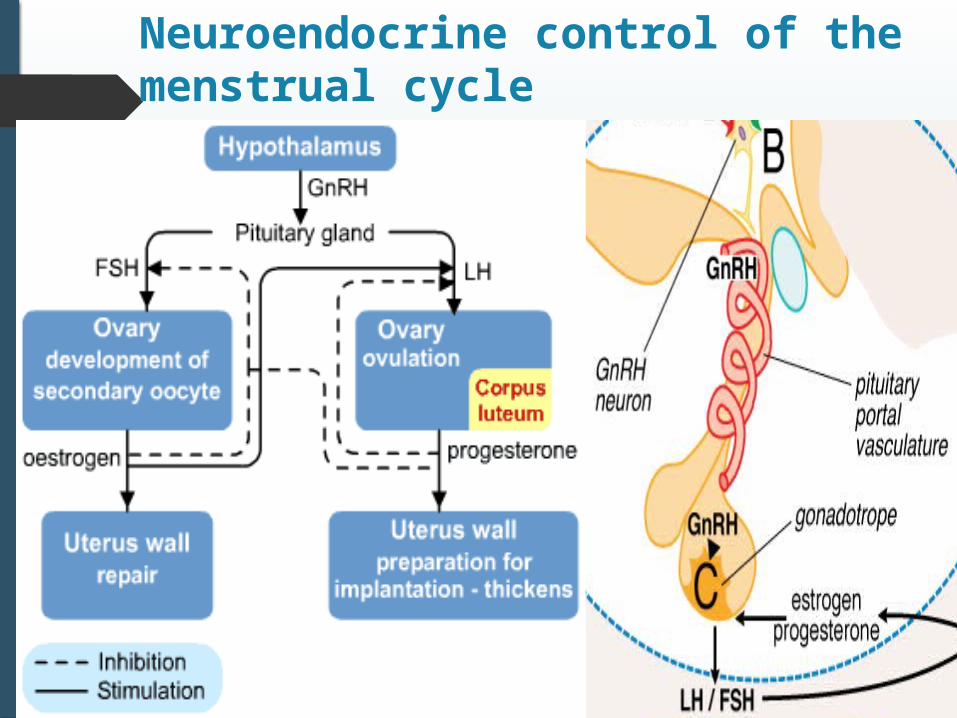
Neuroendocrine control of the menstrual cycle
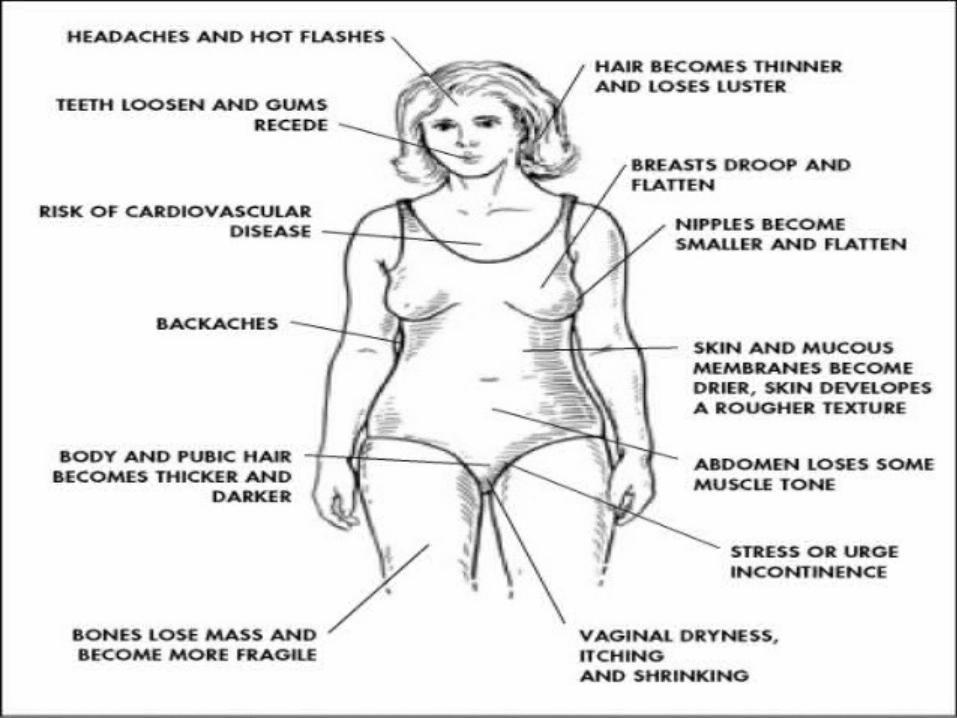
Untoward Responses:
CONCERN ABOUT CARCINOGENIC ACTIONS:
Early studies established that estrogens can induce tumors of the breast, uterus, testis, bone,
kidney, and other tissues in various animal species.
Estrogen use during pregnancy also can increase the incidence of nonmalignant genital
abnormalities in both male and female offspring; pregnant women should not be given
estrogens.
In men: gynaecomastia, feminization, decreased libido
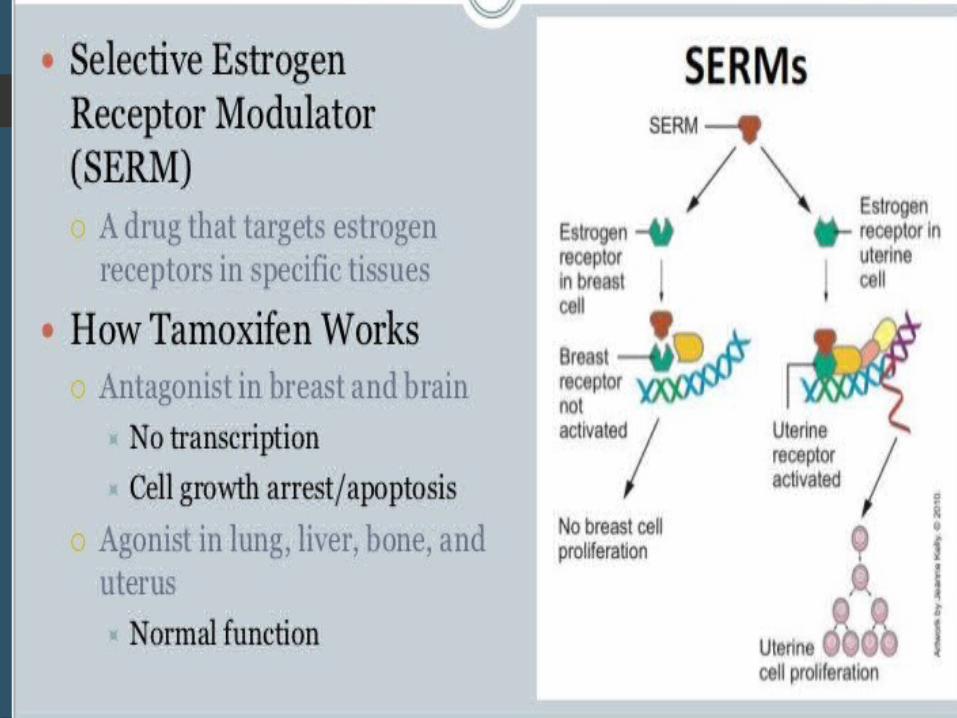
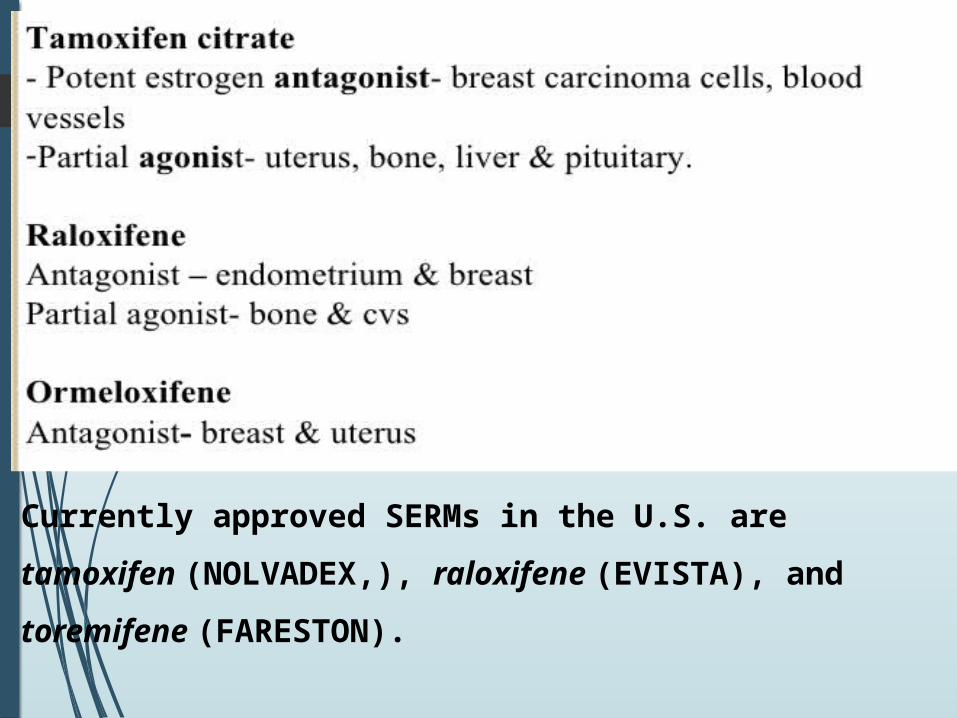
Currently approved SERMs in the U.S. are tamoxifen
(NOLVADEX,), raloxifene (EVISTA), and toremifene (FARESTON).
ANTIESTROGENS: CLOMIPHENE AND FULVESTRANT
These compounds are pure antagonists in all tissues.
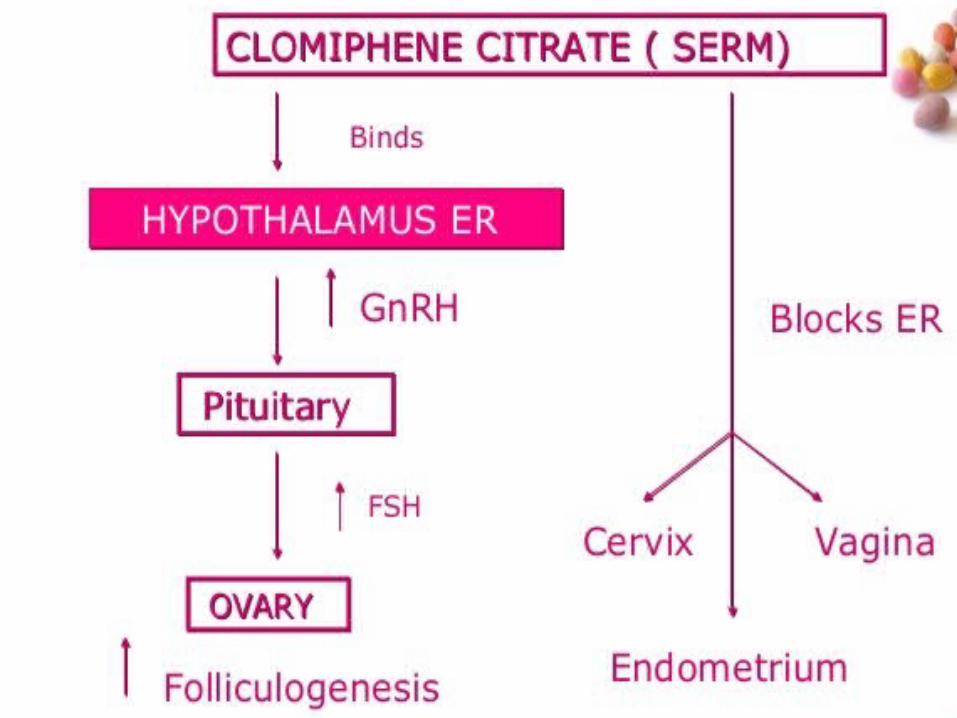
Clomiphene (CLOMID, SEROPHENE, others) is approved for the
treatment of infertility in anovulatory women;
Fulvestrant (FASLODEX, ICI 182,780) is used to treat breast cancer
in women with disease progression after tamoxifen.
Fulvestrant:
It is a pure anti-estrogen( a selective estrogen receptor
downregulator)
It downregulates ER by promoting degradation of receptors by
proteosomal enzymes.
Used to treat tamoxifen resistant breast cancer.
Therapeutic Uses: Breast Cancer Osteoporosis Infertility
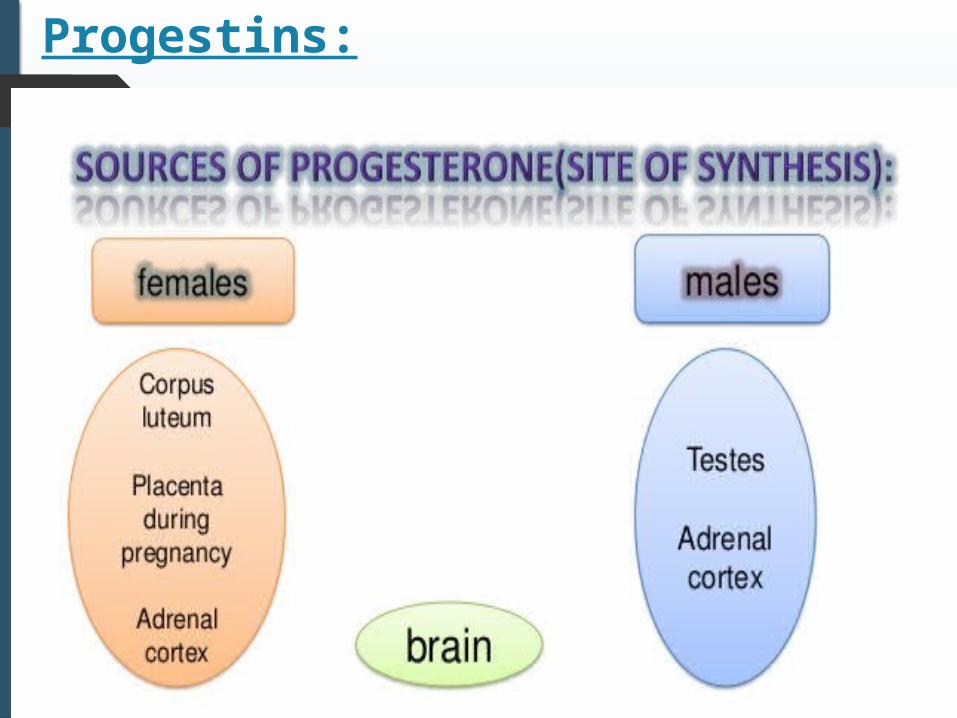
Progestins:
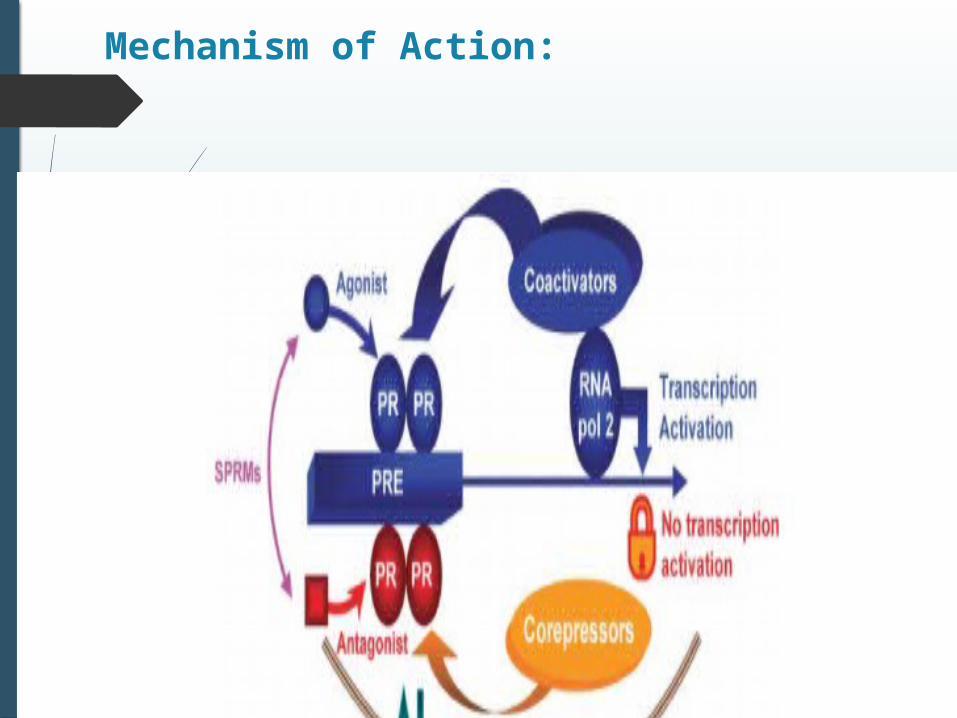
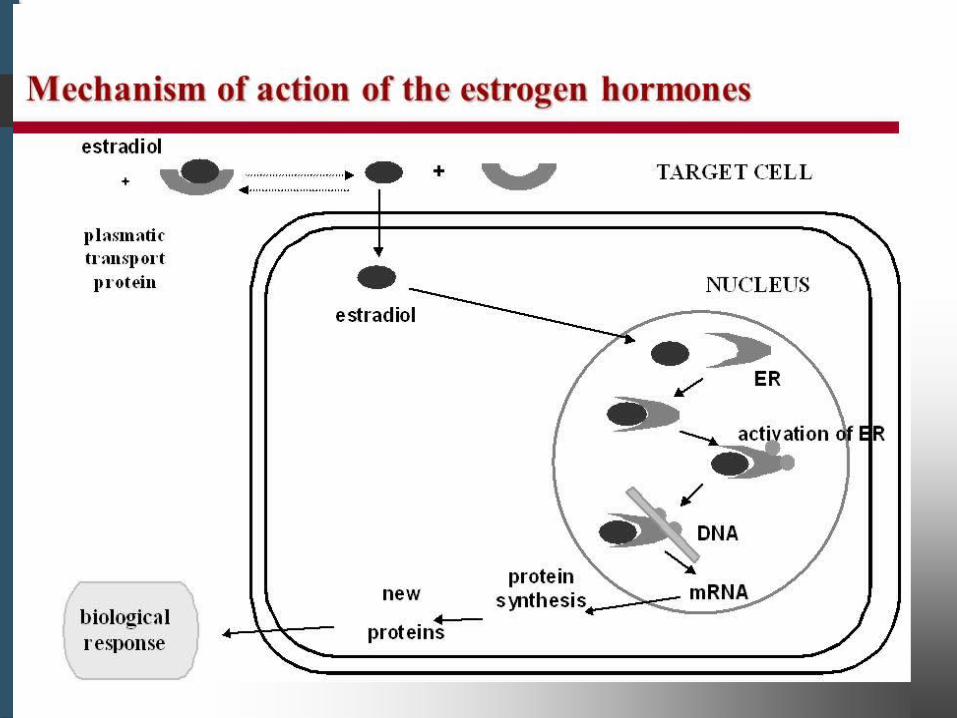
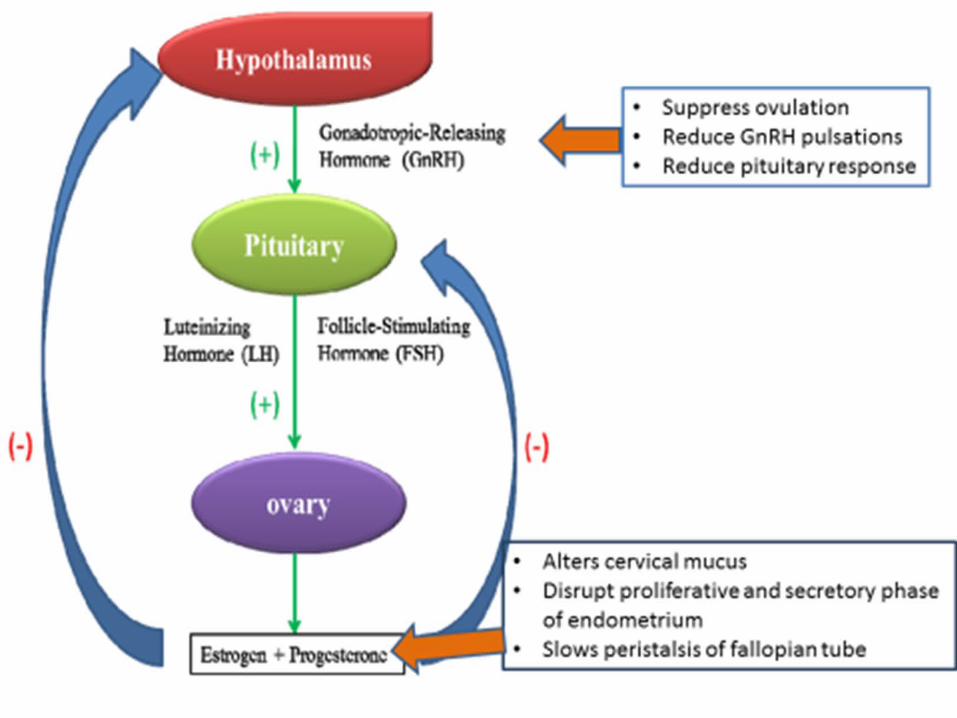
Mechanism of Action:
Physiological and Pharmacological Actions
NEUROENDOCRINE ACTIONS : Progesterone produced in the luteal phase of the
cycle decreases the frequency of GnRH pulses, which is one mechanism of action of
progestin-containing contraceptives.
REPRODUCTIVE TRACT: Progesterone decreases estrogen-driven endometrial
proliferation and induces a secretory endometrium; the abrupt decline in progesterone at
the end of the cycle is the main determinant of the onset of menstruation.
Progesterone also influences the endocervical glands, changing the abundant watery
secretion of the estrogen-stimulated structures to a scant, viscid material.
Finally, progesterone is essential to maintain pregnancy, at least partly by suppressing
uterine contractility.
MAMMARY GLAND :
Mammary gland development requires both estrogen and progesterone.
During pregnancy, and to a minor degree during the luteal phase of the cycle,
progesterone acts with estrogen to induce proliferation of the acini of the mammary
gland.
CNS EFFECTS : Progesterone increases basal body temperature by about 0.6°C
at midcycle when ovulation occurs.
ANTIPROGESTINS:
The antiprogestin, RU 38486 (often referred to as RU-486) or mifepristone, is
available for the termination of pregnancy.
Antiprogestins have several other potential applications, including uses as contraceptives, to induce labor, and to treat uterine leiomyomas, endometriosis, meningiomas, and breast cancer.
THERAPEUTIC USES: Mifepristone (MIFEPREX) is used to terminate early pregnancy.
A prostaglandin (e.g., intramuscular sulprostone, intravaginal gemeprost, or
oral misoprostol) is given 48 hours after the mifepristone(600mg oral) to
ensure expulsion of the detached blastocyst.
The success rate with such regimens is >90% among women with
pregnancies of <7 weeks’ duration.
S/E: failed abortion, prolonged bleeding, vomiting,etc.
Selective Progesterone Receptor Modulator:
Their actions differ in different organs/tissues (agonist activity
where coactivators predominate and antagonist where corepressors
are in excess). Examples include:
Ulipristal – for emergency contraception
Proellex – under clinical trials to treat endometriosis, leiomyoma,
breast CA.
Asoprisnil – under investigation for treatment of leiomyoma.
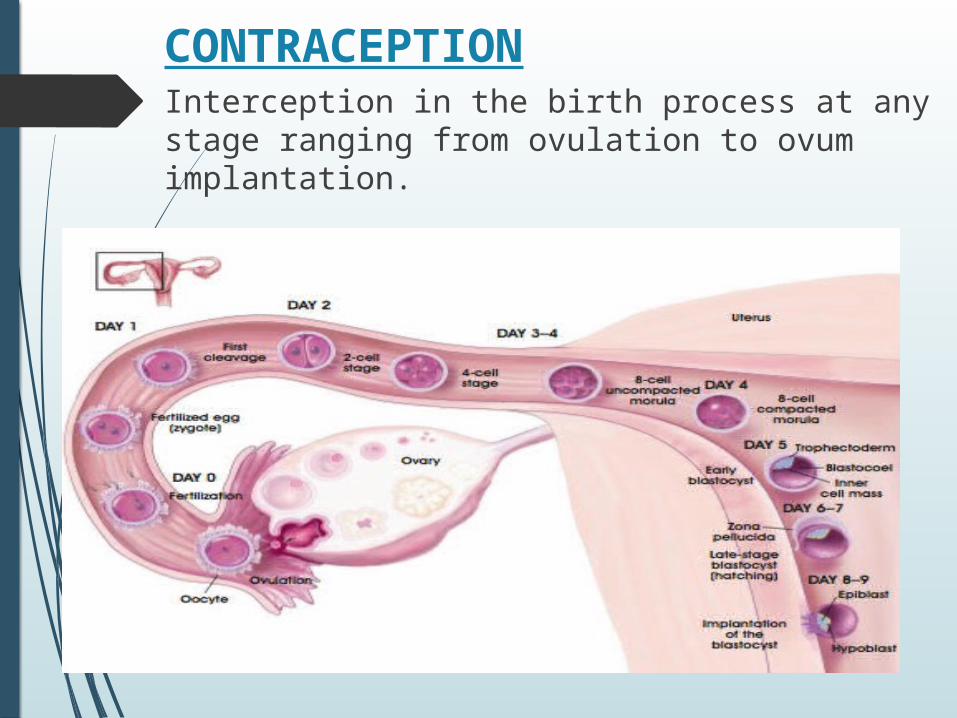
CONTRACEPTIONInterception in the birth process at any stage ranging from ovulation to ovum implantation.
A) ORAL CONTRACEPTIVES:
1) COMBINATION PILLS
Monophasic
Biphasic
Triphasic
2) MINI PILLS (PROGESTIN ONLY PILLS)
3) POST COITAL (MORNING AFTER) PILLS
4) CENTCHROMAN
B) INJECTABLE CONTRACEPTIVES:
5) ESTRADIOL VALARATE+17-HYDROXYPROGESTERONE CAPROATE
6) ESTRADIOL CYPIONATE+MEDROXYPROGESTERONE ACETATE
7) DEPOT MEDROXYPROGESTERONE ACETATE
C) RECENT CONTRACEPTIVE METHODS:
1) LEVONORGESTREL subcutaneous implant
2)LEVONORGESTREL intrauterine inserts
D) HORMONAL CONTRACEPTION IN MALES:
1) TESTOSTERONE UNDECANOATE
2) TESTOSTERONE UNDECANOATE + DMPA
3) GOSSYPOL
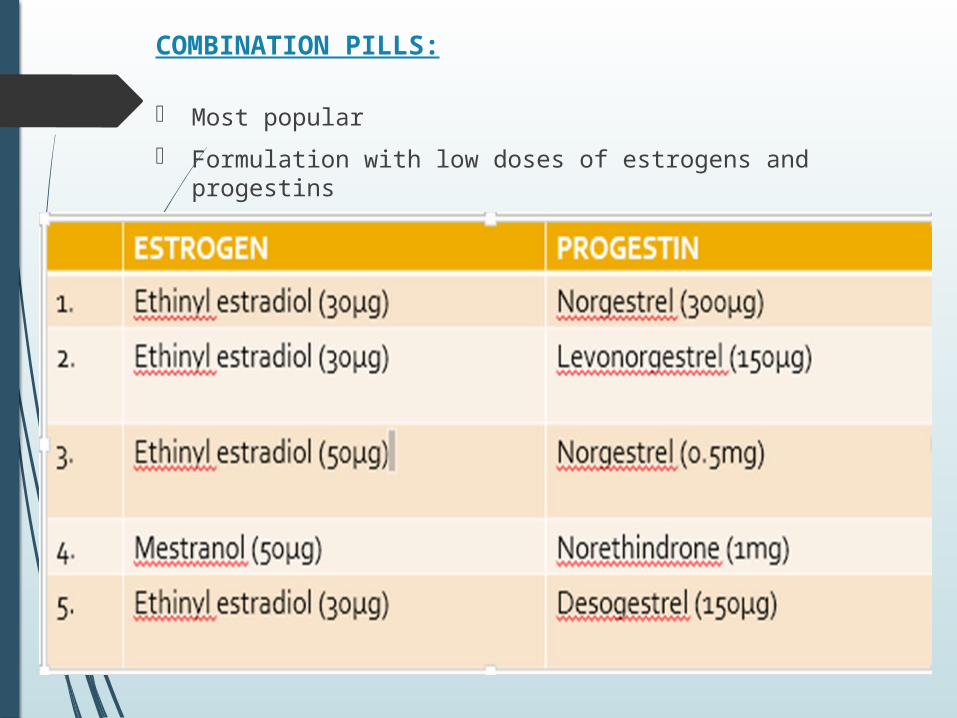
COMBINATION PILLS:
- Most popular- Formulation with low doses of estrogens and progestins
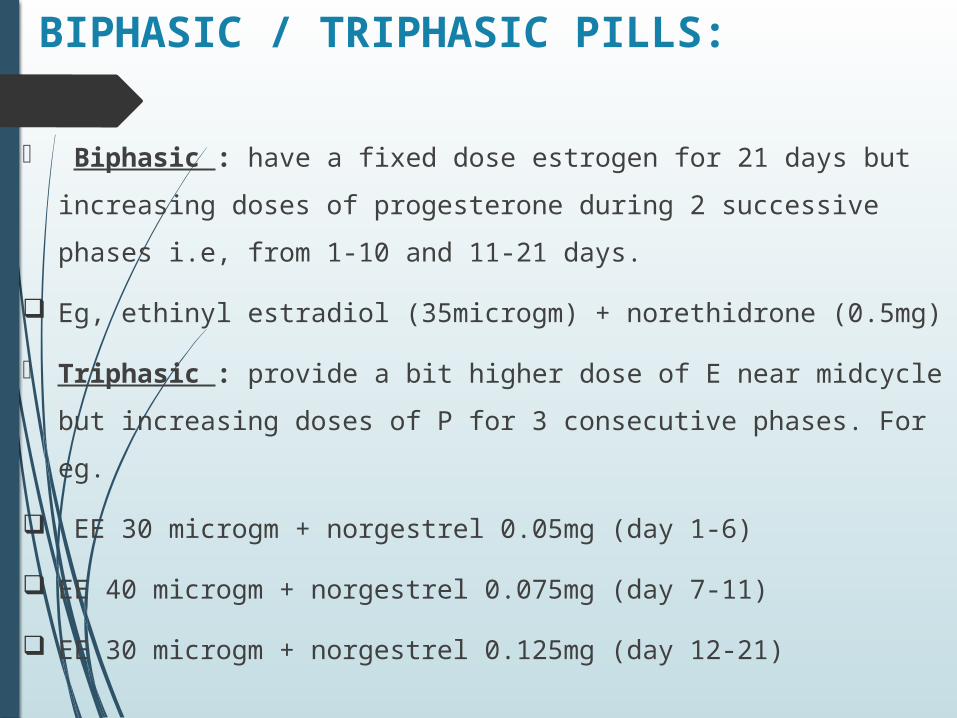
BIPHASIC / TRIPHASIC PILLS:
Biphasic : have a fixed dose estrogen for 21 days but increasing doses of
progesterone during 2 successive phases i.e, from 1-10 and 11-21 days.
Eg, ethinyl estradiol (35microgm) + norethidrone (0.5mg)
Triphasic : provide a bit higher dose of E near midcycle but increasing doses of P
for 3 consecutive phases. For eg.
EE 30 microgm + norgestrel 0.05mg (day 1-6)
EE 40 microgm + norgestrel 0.075mg (day 7-11)
EE 30 microgm + norgestrel 0.125mg (day 12-21)
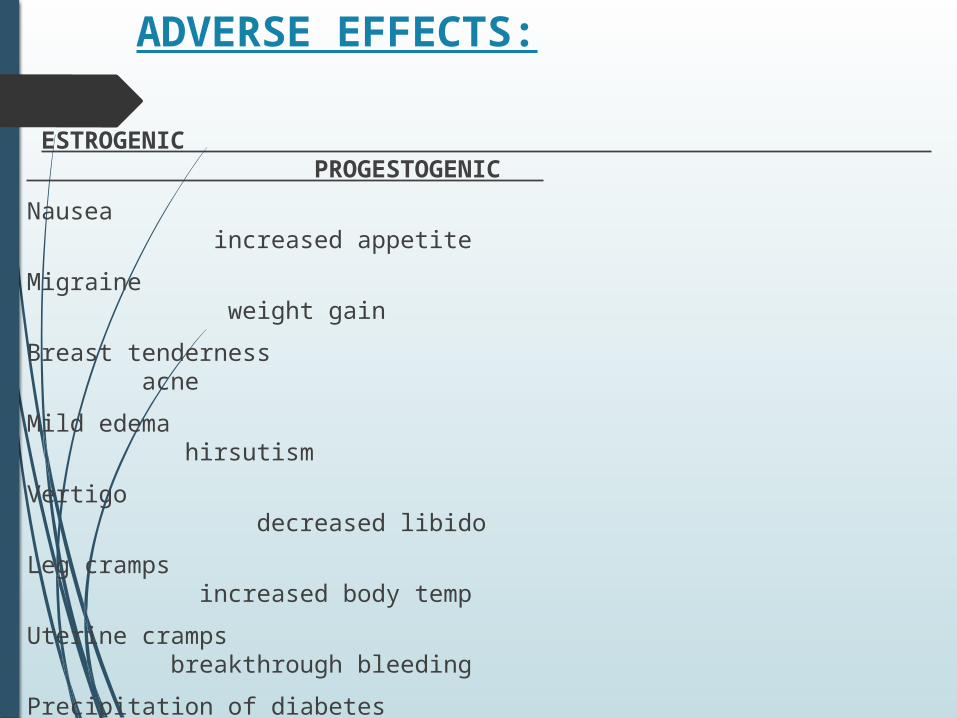
ADVERSE EFFECTS:
ESTROGENIC PROGESTOGENIC
Nausea increased appetiteMigraine weight gainBreast tenderness acneMild edema hirsutismVertigo decreased libidoLeg cramps increased body tempUterine cramps breakthrough bleedingPrecipitation of diabetes monilial vaginitis amenorrheaContraindications: genital CA, diabetes, breast CA, hypertension, undiagnosed vaginal bleeding,etc.
Minipill (progestin only pill)
A low-dose progestin only pill is taken daily continuously without
any gap. The menstrual cycle tends to become irregular and
ovulation occurs in 20-30% women,
The efficacy is lower (96-98%) compared to 98-99.9% with
combined pill.
Eg. Norethindrone 350 microgm or Norgestrel 75.
S/E: acne , hirsutism and amenorrhea.
Postcoital(emergency) contraception
Levonorgestrel 0.5 mg + ethinylestradriol 0.1mg (2 ovral tablets) taken
as early as possible but within 24hours of unprotected intercourse and
repeated after 12 hours. Till recently this regimen called the Yuzpe
method has been the most popular.
Levonorgestrel alone 0.75 mg taken twice with 12 hour gap within
72hours of intercourse.
Mifepristone 600 mg single dose taken within 72hours of intercourse
has been used in China, Europe and few other countries with high
success rates and fewer side effects than Yuzpe method.
Injectables:
Long acting progestin alone injected once month for 2-3 months Two compounds are being marketed:
(a)Depot medroxyprogesterone acetate (DMPA) 150 mg at 3-month intervals.
starting just after parturition or during the first 5 days of the cycle.
Side effects: irregular bleeding ending up in amenorrhea and anovulation.
Mechanism of action: same as that of minipills.
(b)combined estrogen progestin injectable: estradiol cypionate 5mg + DMPA 25mg im once in 2 months.
Side effects:
Mechanism of action: same as that of combination pills
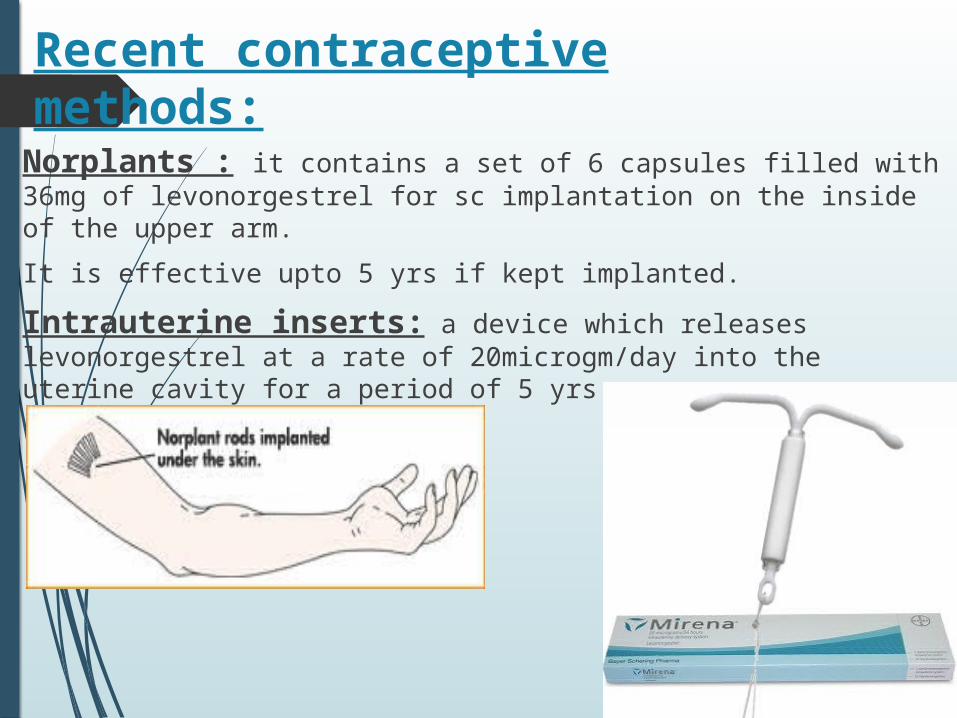
Recent contraceptive methods:
Norplants : it contains a set of 6 capsules filled with 36mg of levonorgestrel for sc implantation on the inside of the upper arm.
It is effective upto 5 yrs if kept implanted.
Intrauterine inserts: a device which releases levonorgestrel at a rate of 20microgm/day into the uterine cavity for a period of 5 yrs.
Hormonal contraception for men:
Recent WHO sponsored trials revealed that initial dose of 1000mg im of
testosterone undecanoate followed by 500 mg maintenance dose revealed
reversible azoospermia in majority of men.
In another study DMPA + testosterone undecanoate : 97% male volunteers
revealed reversible azoospermia within 3 months of initiating the study with
minimum side effects.
Gossypol : orally effective non-steroidal drug obtained from cotton seed and used in
China.
Dose: 20mg/day for initial 2-3 months followed by 50-60mg/day as maintenance dose for not more than 2yrs at a stretch decreases sperm motility drastically within 3 months.
Side effects: hypokalemia,
muscle weakness,
transient paralysis.