failure to thrive
TRANSCRIPT

Failure To Thrive
(FTT)
Parisa Zarei Shargh
MSC student of nutrition science
Dec2014

Defenition of FTT
growth parameters (height and weight ,sever condition,
head circumference)
Fall over 2 or more percentiles
Are persistently below the third or fifth percentiles
Are less than the 80th percentile of median

• Severe:Height and weight at or below the 3rd percentile.
• Moderate :Either height or weight at or below the 3rd
percentile, but not both.
• Mild :Both height and weight between the 3rd and 10th
percentiles.
• None :Height and weight both above the 10th percentile.

Coleman-Jensen etal.2010Drotar etal.2000
FTT
ORGANICMajor medical
illness
NON ORGANIC
Psychological neglect
Malnutrition
Impaire immono
competence
Jeopardize growth
Deficits in cognition
Deficits in
socioaffective
compotence
Nonorganic FTT grow in the hospital, whereas organic FTT do not

Why children?
fewer reserves
higher resting energy expenditure.
are in a growth and development phase
Infants and children are very susceptible to problems of nutrition.

Nutrition-related factors contribute to about 45% of deaths in
children under five years of age.

Causes?
Social
Poverty
Food insecurity
Prematurity Despite faster linear growth rates, even late preterm children
(34-36 weeks' gestational age) are at increased risk of stunting compared with term peers
preterm and small-for-gestational-age infants are more likely to show persistent deficits in growth and in cognitive
and academic achievement at 8 years of age
The most common cause of growth faltering in former
preterm infants is inappropriate diet for corrected age.
early discontinuation of the nutrient-dense formula (preterm infant formula until they weigh at least 2000g.some data: 18month
In general; until 6 months' corrected age or when weight for length is
maintained above the 25 percentile)
initiation of solid feedings at 6th months for infant at 28
weeks whose corrected age is only 3 months

(SGA) infants are conventionally defined as
those with birth weight less than he 10th
percentile for gestational age.

Heavy use of caffeine prenatally is associated in
some studies with depressed intrauterine growth
Heavy cigarette exposure during pregnancy and
statistically significant decrements in stature at
school age, but the magnitude of the deficit (I to
2 cm)

Use of fluoxetine in breastfeeding women
was associated with some reduction in
infant weight gain between 2 weeks and
6 months of age

Fetal alcohol syndrome cases Length and head
circumference are more depressed than weight.
very low birth weight infants, children
oral-motor difficulties may limit caloric intake,
unless gastrostomy tubes are placed
inadequate care and nutrition
Though consumption of less than 15 drinks per week was not proven
to cause FAS-related effects
Pregnant women who consume approximately 144 grams of pure
alcohol per day have a 30–33% chance of having a baby with FAS.[38]

Marijuana, like smoking tobacco,
increases maternal carbon
monoxide levels and decrease fetal
oxygenation

Postnatal medical issuemost common previously undiagnosed conditions affect the
gastrointestinal tract:
chronic nonspecific
diarrhea
celiac disease
food allergies
Gastro esophageal reflux
cystic fibrosis
lactose intolerance
Subtle neurologic dysfunction manifested as fine motor and
oral motor

urinary tract infections and renal
tubular acidosis as potentially
clinically silent contributors to FTT

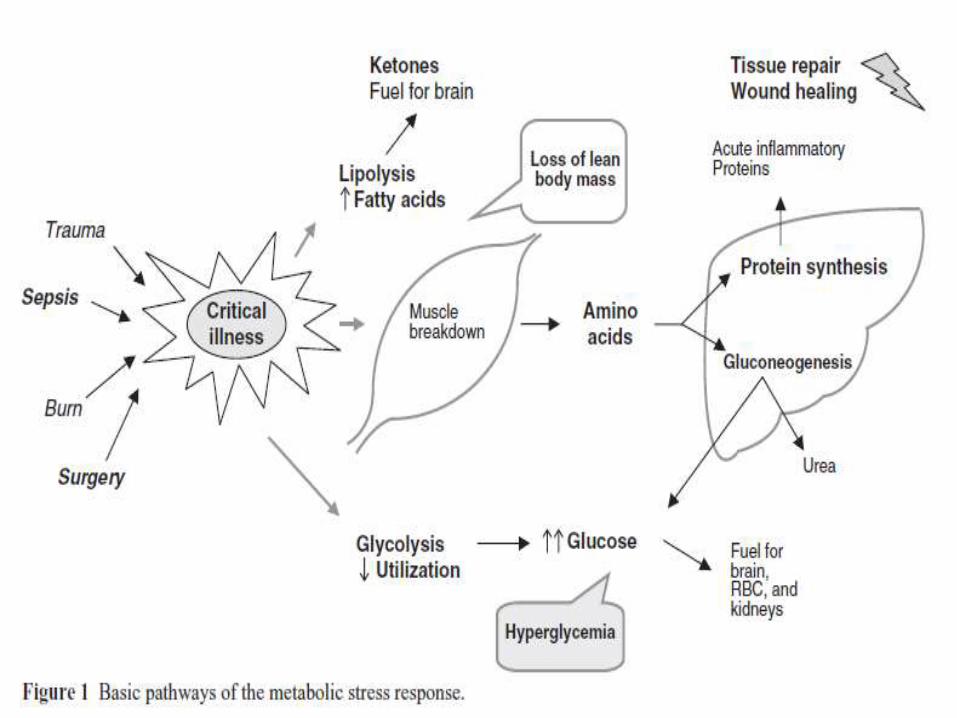
METABOLIC RESPONSE TO CRITICAL ILLNESS
Children, similar to adults, rely on the
metabolic breakdown and transfer of protein,
carbohydrates, and lipid to meet the catabolic
demands of critical illness

The constipation and intense food
selectivity that are more prevalent in
children with autism

infection-malnutrition cycle. With each illness,
the child's appetite and nutrient intake
decrease while nutrient requirements increase
as a result of fever, diarrhea, and vomiting

Physical Examination EvaluationPhysical Examination Evaluation

Anthropometric evaluation
weight for age
height for age
weight for height
mid-arm circumference
birth weight

Laboratory test
complete blood cell
Iron deficiency with or without anemia is a
common finding. In cases in which the CBC count
is unrevealing, measures of iron indicators.
Iron deficiency, with or without associated anemia,
is Seen in as many as one half of all children
presenting with FFT

blood urea nitrogen, creatinine and serum
electrolytes, and urine pH
renal function
renal tubular acidosis
are mandatory in children with recurrent or
persistent vomiting or diarrhea, clinically
obvious dehydration, or severe malnutrition,
which is often associated with hypokalemia.
serum albumin and pre albumin (transthyretin) to assess
protein status
determine serum alkaline phosphatase, calcium and
phosphorus concentrations.
A decreased alkaline phosphatase concentration suggests
zinc deficiency; an increased concentration, especially if
associated with a decrease of phosphorous
concentration, is suggestive of rickets

Albumin:
high specificity but low sensitivity
long plasma half-life (14-20 days)
It is not a good parameter for monitoring
nutritional status due to its low sensitivity
to acute changes.
Serum albumin concentrations may be
affected by albumin infusion, dehydration,
sepsis, trauma, and liver disease,
independent of nutritional status

Pre albumin
short half-life of two days
very sensitive and specific to changes in
the nutritional status.
Pre-albumin is a useful parameter for
monitoring, and the evolution of
nutritional status of the seriously ill
patient.

Transferrin
half-life of eight to ten days
Its value as a nutritional indicator is
lower than that of pre-albumin due to
its low sensitivity and specificity.
Its levels are altered in liver disease,
iron deficiency anaemia, nephrotic
syndrome, and the administration of
aminoglycosides and cephalosporins.

Retinol binding protein
Very short half-life of 12 hours
Its levels fall with malnutrition,liver
disease, infection, and with intense stress.
Retinol binding protein is a good marker
of the nutritional status evolution, but is
not of value in patients with renal failure.

HIV test
Serum lgA and anti-tissue trans glutaminase antibodies
screen for celiac
Serum lgE testing for food allergies

Nutritional evaluation
Feeding history adjusted for age
Breast- or formula-fed
Age solids introduced
Age switched to whole milk
Food allergy or intolerance
Vitamin or mineral supplements
Current feeding behaviors
Difficulties with sucking, chewing. or swallowing
Frequency of feeding
Duration offeeding episodes
Who feeds
Where fed (alone or held, with or separate from family, lap or high
chair)

Perceived appetite
Pica
Caregiver's nutrition knowledge
perceived as dangerous?
Adequacy offinancia l resources for food purchase
WIC
Adequacy of earned income
Recent change i n food budget (cuts or increases in benefits, new mouths to
feed, job gain
or loss)
Family's knowledge of how to budget food purchasing
Material resources for food preparation and storage and Refrigeration
Cooking facilities
Running water
24-h dietary recall : was yesterday typical?
Food frequency

Breastfeeding difficulties
Over dilution of formula
behavioral feeding problems (eg spitting out
food, tantrums during meals, food refusal)
and determine how the
parents have tried to manage the child's
problems
difficulty in the timing of feedings (restricting
a toddler to 3 meals a day), constant feedings
(grazing), and lack of a consistent feeding
schedule

Nutritional interventionThe goal of nutritional intervention in FTT
is to achieve "catch-up" growth, that is,
growth at a faster-than-normal rate for age
so that the child's relative deficit of body
source is restored
Depending on the severity of the initial
deficit, 2 days to 2 weeks may be required
to initiate catch-up growth

TNX FOR YOUR ATTENTIONS.