facial pain and monosymptomatic hypochondriasis
TRANSCRIPT
330 CONGENITAL DEFICIENCIES OF FACTOR V AND VIII
ported that the transfusion of fresh plasma from he- mophilia A had no significant effect on a patient’s factor VIII level. Including our case, there is no report of a case where the transfusion of normal fresh plasma led to a delayed rise of both factors by newly synthesizing factors V and VIII from a common precursor. This necessitates further studies as to the existence of a common precursor.
No further transfusions were required when local hemostatic treatment was used after the transfusion of fresh plasma. We therefore believe that replace- ment therapy is necessary only to permit local he- mostatic treatment to be effective and that no fur- ther blood replacement is necessary after that point.
Summary
A case of combined congenital deficiencies of factors V and VIII is reported. The patient’s right mandibular first molar was extracted and a combi- nation of local hemostatic treatment and the trans- fusion of fresh plasma resulted in healing of the socket without further postoperative bleeding.
References
1. Oeri J. Matter M, Isenschmid H, et al: Angeborener Mange1 an Faktor V (Parahaemophilia), verbunden mit echter Haemophilia A bei zwei Brtiden. Bibliotheca Paediatrica 58:575, 1954
2. Seibert RH, Margolius A Jr, Ratnoff OD: Observation on hemophilia, parahemophilia and coexistent hemophilia and parahemophilia. J Lab Cli Med 52449, 1958
3. Jones JH, Rizza CR, Hardisty RM, et al: Combined deti- ciency of factor V and factor VIII (antihaemophilic glob- ulin). A report of three cases. Br J Haematol 8: 120, 1962
4. Seligsohn U, Ramot B: Combined factor V and factor VIII deficiency. Report of four cases. Br J Haematol 16:475, 1969
5. Smit Sibinga CTh, Gokemeyer JDM. Ten Kate LP, et al: Combined deficiency of factor V and factor VIII. Report of a family and genetic analysis. Br J Haematol 23:467, 1972
6. Gobbi F, Ascari E, Barbieri U: Combined deficiency of factor VIII (antihaemophilic globulin) and factor V (proaccelerin) in two siblings. Clinical study and genetic speculations. Thromb Diath Haemorrh 17:194, 1967
7. Girolami A, Gastaldi D, Patrassi G, et al: Combined con- genital deficiencv of factor V and factor VIII. Renort of a further case with some considerations on the hereditary transmission of this disorder. Acta Haematol55:234, 1976
8. Saito H, Shioya M, Koie K, et al: Congenital combined de- ficiency of factor V and factor VIII. A case report and the effect of transfusion of normal plasma and hemophilic blood. Thromb Diath Haemorrh 22:316, 1969
9. Menache D, Hakin J: Un noveau cas de deficit associe en facteur VIII et V. Path01 Biol Paris 16:969. 1968
J Oral Maxillofac Surg
42:330-332, 1904
Facial Pain and Monosymptomatic Hypochondriasis
KENNETH L. MALINOW, MD, AND
Occasionally in the practice of dentistry one en- counters patients in whom no organic pathology can be found yet who persist in complaints that are of a specific and seemingly physical nature.‘>* No amount of medical examination, testing, or reas- surance can change the patient’s delusional belief that they are diseased in one way or another. In spite of a sometimes successful adjustment in other
* Medical Director, Psychophysiological Clinic, University of Marvland School of Medicine. Baltimore, Marvland.
P Assistant Professor, Psychophysiological-Clinic, Depart- ment of Psvchiatrv. Universitv of Marvland School of Medicine.
Addresscorrespondence and reprint requests to Dr. Malinow: Psychophysiological Clinic, University of Maryland School of Medicine, 655 West Baltimore Street, Baltimore, MD 21201.
EDWARD G. GRACE, DDS, MAt
aspects of their lives, these patients strongly believe in their disease. Their disease is both obsessional and delusional. However, the suggestion to these patients that they have a psychological component to their illness leads them to rapidly withdraw from clinical contact and move on to another treatment facility.3>4
Many different descriptions and classifications of this type of patient have been proposed, but most have been confusing, nondescriptive, and certainly not helpful either diagnostically or therapeutically.4 We will present examples of patients with fixed de- lusions of dental disfigurement and pain who seem to fall under the diagnostic category of monosymp- tomatic hypochondriasis.
MALINOW AND GRACE
1 23 4 56 7 69 0 ,234 6 67 6 9 0
331
FEIIIA
2 Stird Dmiations
Above Mean
\ A 2 w- . .
\ . P
I al i
Mde
/l E .
/ .--- . ,\ 1
1 Stmulard
Dwiiion Abow Mean
.
’
.-.
/
mm t
1
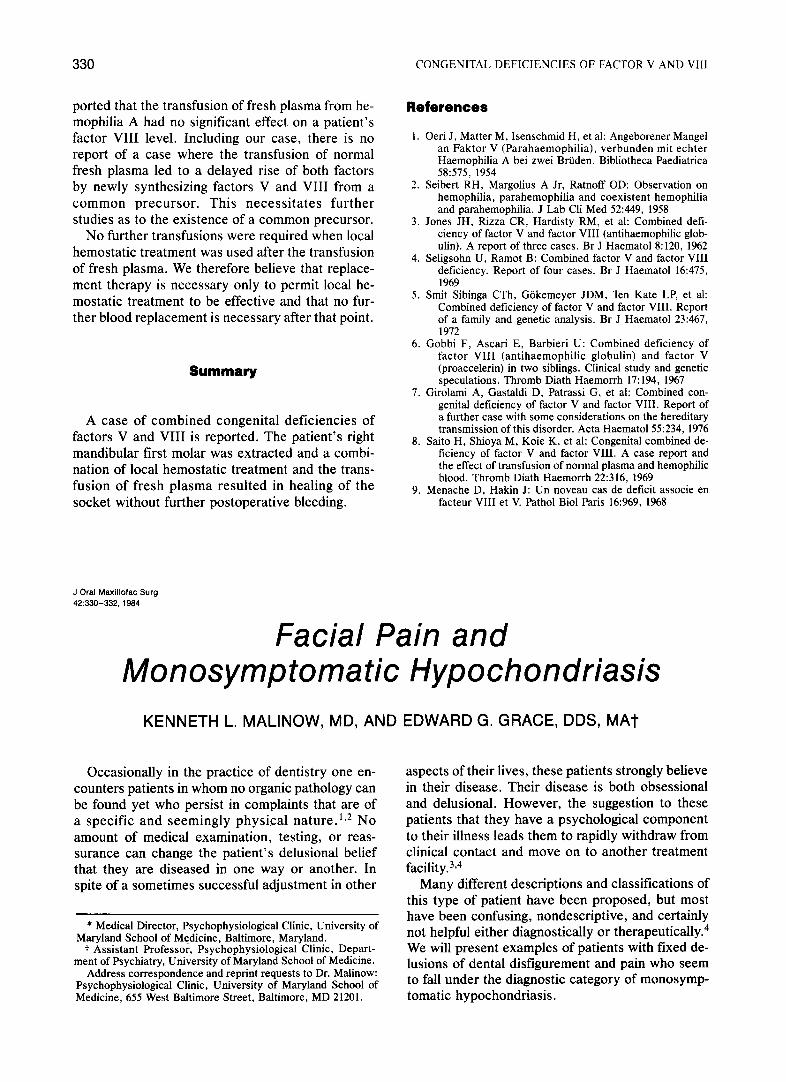
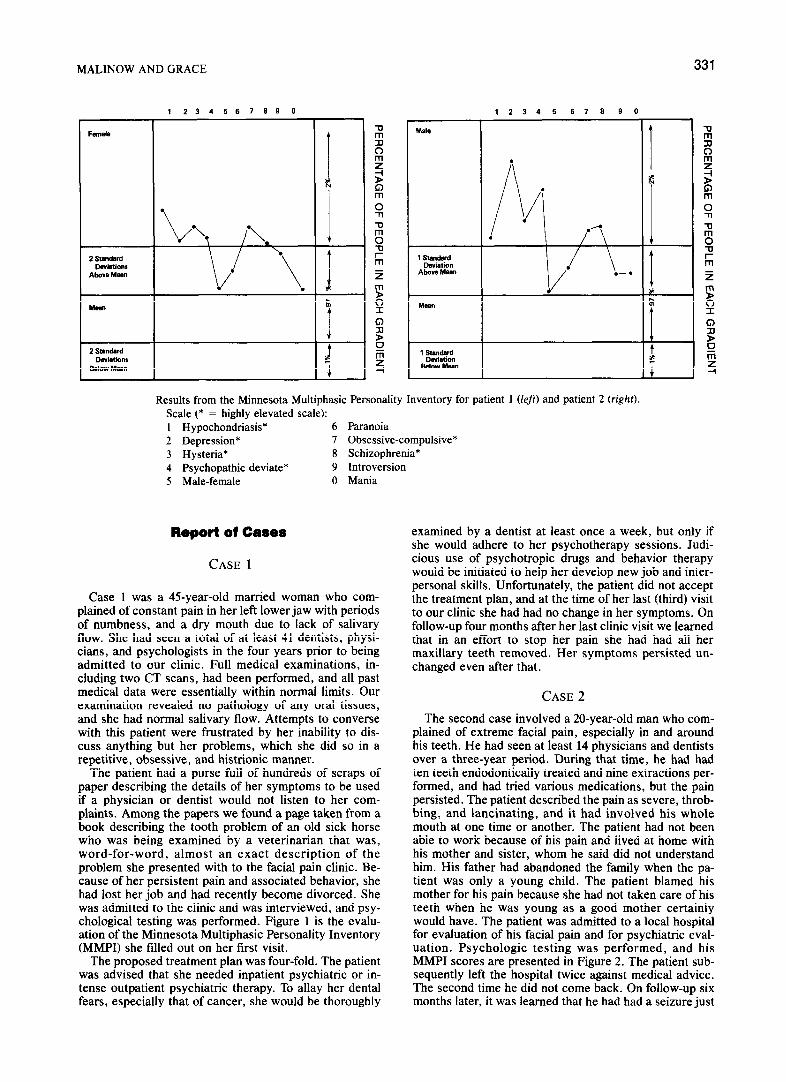
Results from the Minnesota Multiphasic Personality Inventory for patient 1 (lefr) and patient 2 (right). Scale (* = highly elevated scale): 1 Hypochondriasis* 6 Paranoia 2 Depression* 7 Obsessive-compulsive* 3 Hysteria* 8 Schizophrenia* 4 Psychopathic deviate* 9 Introversion 5 Male-female 0 Mania
Report of Cases
CASE 1
Case 1 was a 4%year-old married woman who com- plained of constant pain in her left lower jaw with periods of numbness, and a dry mouth due to lack of salivary flow. She had seen a total of at least 41 dentists, physi- cians, and psychologists in the four years prior to being admitted to our clinic. Full medical examinations, in- cluding two CT scans, had been performed, and all past medical data were essentially within normal limits. Our examination revealed no pathology of any oral tissues, and she had normal salivary flow. Attempts to converse with this patient were frustrated by her inability to dis- cuss anything but her problems, which she did so in a repetitive, obsessive, and histrionic manner.
The patient had a purse full of hundreds of scraps of paper describing the details of her symptoms to be used if a physician or dentist would not listen to her com- plaints. Among the papers we found a page taken from a book describing the tooth problem of an old sick horse who was being examined by a veterinarian that was, word-for-word, almost an exact description of the problem she presented with to the facial pain clinic. Be- cause of her persistent pain and associated behavior, she had lost her job and had recently become divorced. She was admitted to the clinic and was interviewed, and psy- chological testing was performed. Figure 1 is the evalu- ation of the Minnesota Multiphasic Personality Inventory (MMPI) she filled out on her first visit.
The proposed treatment plan was four-fold. The patient was advised that she needed inpatient psychiatric or in- tense outpatient psychiatric therapy. To allay her dental fears, especially that of cancer, she would be thoroughly
examined by a dentist at least once a week, but only if she would adhere to her psychotherapy sessions. Judi- cious use of psychotropic drugs and behavior therapy would be initiated to help her develop new job and inter- personal skills. Unfortunately, the patient did not accept the treatment plan, and at the time of her last (third) visit to our clinic she had had no change in her symptoms. On follow-up four months after her last clinic visit we learned that in an effort to stop her pain she had had all her maxillary teeth removed. Her symptoms persisted un- changed even after that.
CASE 2
The second case involved a 20-year-old man who com- plained of extreme facial pain, especially in and around his teeth. He had seen at least 14 physicians and dentists over a three-year period. During that time, he had had ten teeth endodontically treated and nine extractions per- formed, and had tried various medications, but the pain persisted. The patient described the pain as severe, throb- bing, and lancinating, and it had involved his whole mouth at one time or another. The patient had not been able to work because of his pain and lived at home with his mother and sister, whom he said did not understand him. His father had abandoned the family when the pa- tient was only a young child. The patient blamed his mother for his pain because she had not taken care of his teeth when he was young as a good mother certainly would have. The patient was admitted to a local hospital for evaluation of his facial pain and for psychiatric eval- uation. Psychologic testing was performed, and his MMPI scores are presented in Figure 2. The patient sub- sequently left the hospital twice against medical advice. The second time he did not come back. On follow-up six months later, it was learned that he had had a seizure just

332 MONOSYMPTOMATIC HYPOCHONDRIASIS
prior to having his 16 remaining teeth extracted by a den- tist who had agreed to do so if all else seemed to fail.
Discussion
The similarities between these two patients are striking despite the differences in their back- grounds. They both were completely obsessed with their pain to the detriment of all other aspects of their lives. They both were insistent on the neces- sity for surgical or mutilating procedures to their head and face as a cure despite the failure of pre- vious surgical treatments to relieve their pain. Both patients sought out numerous health practitioners for diagnosis and therapy and would terminate any treatment that involved psychologic or emotional approaches to their pain and suffering.
Psychologic testing of both patients showed strik- ingly abnormal psychologic patterns, although both tests needed to be interpreted with care. Patient 1 left many of the questions unanswered, while pa- tient 2 gave conflicting answers on a greater than average number of questions. Both patients shared elevations that were two standard deviations above norm on exactly the same scales, although their pat- terns were somewhat different. Patient l’s MMPI suggests that she has a mixed character disorder with obsessive and hysterical defenses and a large amount of underlying hostility, which she expresses in a passive-aggressive manner. Patient 2 shows a pattern more typical of a psychotic patient, or atyp- ical depression, in which the neurotic defenses of denial, repression, and somatization have failed to defend against underlying hostility. It should be noted that the paranoid scale is within normal limits for both patients in spite of the delusional quality of their belief in their disease. The terms “con- verting masochistic psychosis,” “hysteria,” “atyp- ical facial neuralgia,” “anxiety neurosis,” and “obsessional paranoias” have been applied to both these patients and other patients showing a similar pattern of symptoms and psychologic difficulty. The most accurate and descriptive label possible might be monosymptomatic hypochondriasis.5,6 This di- agnosis has often been used in Europe and more recently in the United States to describe patients who manifest a delusional belief that they are dis- eased or malformed in spite of the lack of organic dysfunction or positive results from medical tests.
These patients differ from most somatizing pa-
tients in a number of important aspects. First, most hypochondriacal patients have a variety of some- what vague symptoms that range over many dif- ferent organ systems. Classically this leads them to many different specialists for complaints that can’t seem to be “pinned down.” In contrast, patients with monosymptomatic hypochondriasis have per- sistent, well-focused, and unchanging complaints that generally lead them to see a variety of special- ists in the same closely related fields (e.g., den- tistry, otorhinolaryngology, neurology). Second, these patients seem to be emotionally sicker than the more classically neurotic patients with conver- sions. This becomes readily apparent with psycho- logical testing or with an indepth psychiatric inter- view. It is this poorer contact with reality, combined with an unyielding grip on their symptoms, that makes them difficult to treat. Thus, therapy cannot consist of the demonstration of a simple psycho- physiologic mechanism (e.g., bruxism, hyperventi- lation) with concomitant use of educational tech- niques geared toward skill acquisition and mastery (muscle relaxation or deep breathing),’ but instead should consist of intensive psychotherapy.
In summary, monosymptomatic hypochondriasis should be considered as a diagnosis for patients who present with intense pain symptoms that have become an obsession and a focal point of their lives and yet who have no organic pathology or definite syndrome. It should be noted, however, that many patients who have temporomandibular joint or fa- cial pain present with very similar symptoms and pain patterns. The use of good diagnostic tech- niques, appropriate psychologic testing, and in- depth interviews is crucial in diagnostic differentia- tion and the selection of appropriate therapy.
References
1. Regs R, Harris M: Atypical odontalgia. Br J Oral Surg 16:212,1978-79
2. Kreisberg M: Atypical odontalgia: differential diagnosis and treatment. JADA 104:852, 1982
3. Audreaen N, Barduch J: Dysmorphophobia: symptom or disease? Am J Psychiatry 134:673, 1977
4. Bishop ER: Monosymptomatic hypochondriasis. Psycho- somatics 21:731, 1980
5. Monroe A: Monosymptomatic hypochondriacal psychoses. Can Psychiatry Assoc J 23:497, 1978
6. Landee GR: Hypochondriacal Syndromes. New York, El- sevier, 1966
7. Grace EG, Malinow KL: Hyperventilation and facial pain. JADA 10452, 1982