exercise as treatment for anxiety: systematic review and...
TRANSCRIPT
ORIGINAL ARTICLE
Exercise as Treatment for Anxiety: SystematicReview and Analysis
Gregory L. Stonerock, Ph.D. & Benson M. Hoffman, Ph.D. &Patrick J. Smith, Ph.D. & James A. Blumenthal, Ph.D.
# The Society of Behavioral Medicine 2015
AbstractBackground Exercise has been shown to reduce symptomsof anxiety, but few studies have studied exercise in individualspreselected because of their high anxiety.Purpose The objective of this study is to review and criticallyevaluate studies of exercise training in adults with either highlevels of anxiety or an anxiety disorder.Methods We conducted a systematic review of random-ized clinical trials (RCTs) in which anxious adults wererandomized to an exercise or nonexercise control condi-tion. Data were extracted concerning anxiety outcomesand study design. Existing meta-analyses were alsoreviewed.Results Evidence from 12 RCTs suggested benefits of exer-cise, for select groups, similar to established treatments andgreater than placebo. However, most studies had significantmethodological limitations, including small sample sizes, con-current therapies, and inadequate assessment of adherence andfitness levels.Conclusions Exercise may be a useful treatment for anx-iety, but lack of data from rigorous, methodologicallysound RCTs precludes any definitive conclusions aboutits effectiveness.
Keywords Exercise . Physical activity . Anxiety . Anxietydisorders . Systematic review
Introduction
Anxiety, a psychological state characterized by apprehensiveexpectation or fear, is among the most commonly experiencedpsychiatric symptoms [1]. Data from the National Comorbid-ity Study-Replication suggest that in the USA, the lifetimeprevalence of any anxiety disorder is approximately one inthree, more than any other diagnostic category [2]. Some ele-vation in anxiety symptoms, whether affective (fear, appre-hension) or physiological (racing heart, trembling, etc.), is acriterion common to all of these disorders. However, otherdiagnostic criteria for anxiety disorders can be quite heteroge-neous, such as the frequency and severity of symptoms as wellas whether triggers for these symptoms are specific or moregeneralized. Subsyndromal anxiety symptoms also can impairindividuals’ psychosocial functioning and can necessitate useof health care resources [3]. Anxiety represents a risk factorfor lower health-related quality of life [4], increased risk of all-cause mortality [5], and a variety of physical health problems,particularly cardiovascular disease (CVD).
Findings from a number of prospective epidemiologicalstudies report a strong association of anxiety with mortalityin healthy individuals [5–7] and in CVD patients [8–14]. It hasbeen shown that elevated anxiety scores were associated withincreased risk of mortality after accounting for established riskfactors in 934 men and women with CVD [15]. Moreover,elevated anxiety symptoms have been shown to be associatedwith a 2-fold increased risk of mortality in coronary bypasspatients [11–13] and in outpatients with CVD [9, 16, 17]. Onestudy [10] reported that CVD patients with generalized anxi-ety disorder (GAD) assessed 2 months following hospital dis-charge showed a 2.3-fold increased risk of adverse cardiacevents and another [17] reported a 2.8-fold increased risk ofadverse events in acute post-MI patients in which anxiety wasmeasured 1 month following hospital discharge. Similarly, a
G. L. Stonerock (*) : B. M. Hoffman : P. J. Smith :J. A. BlumenthalDepartment of Psychiatry and Behavioral Sciences, Duke UniversityMedical Center, Box 3119, Durham, NC 27710, USAe-mail: [email protected]
ann. behav. med.DOI 10.1007/s12160-014-9685-9

2-fold increased risk of adverse events was observed in stableCVD patients with elevated anxiety during annual clinic visits[18]. High anxiety has also been associated with increased riskfor the development of hypertension [19], heart disease [20],and increased cancer mortality in longitudinal studies of earlyadults [5, 21], even when controlling for other medical riskfactors. Among healthy individuals, anxiety can be associatedwith unhealthy behaviors such as physical inactivity, smoking,and poor diet, leading to increased risk for developing healthissues [22, 23].
Several empirically supported treatments have shown effi-cacy for anxiety reduction, including cognitive-behavioraltherapy (CBT) [24–26] and psychotropic medications, partic-ularly selective serotonin reuptake inhibitors (SSRIs) [25,27–29]. However, these treatments may be associated withsignificant drawbacks and treatment barriers. For example,although SSRIs can be effective for some, they are not effec-tive for everyone and may be associated with adverse sideeffects [30], which can lead to treatment dropout [31]. Al-though CBT also has empirical support as a structured inter-vention for anxiety disorders, access can be limited by a myr-iad of factors, including availability of trained providers andeconomical considerations [32]. Such issues represent barriersto effective treatment for individuals with elevated anxiety,creating the need for alternative therapies.
Exercise may represent a promising, affordable, and easilyaccessible treatment option for individuals with anxiety. Ex-ercise is distinguished from other forms of physical activity inthat it is a planned, structured, repetitive endeavor with thegoal of improving physical fitness [33]. A number of obser-vational studies document an inverse association of exerciseand symptoms of anxiety. For example, in one study of 8098adults [34], individuals exercising “regularly” had a reducedrisk of being diagnosed with an anxiety disorder compared totheir sedentary counterparts (odds ratios [OR] from 0.64 to0.78 for exercisers). In another study of 19,288 participantsin the Netherlands Twin Registry [35], individuals reporting240min a week ofmoderate exercise reported less anxiety andneuroticism compared with nonexercisers. Although encour-aging, data from observational studies cannot prove that exer-cise caused reduced risk for an anxiety disorder. Anxious per-sons may be less likely to be physically active and engage inexercise [35].
Interventional studies of healthy individuals without ananxiety disorder have demonstrated reductions in stateanxiety immediately after performing single bouts of ex-ercise [36–39]. However, such studies do not address thequestion of whether accumulated bouts of exercise reduceanxiety levels nor do they address whether individualswith an anxiety disorder could benefit from repeatedbouts of exercise. Interventional studies also have exam-ined the effects of multiple bouts of exercise on anxiety,albeit primarily among individuals who were not selected
on the basis of high anxiety levels. For example, onestudy of 357 older adults found that assignment to regularexercise participation was associated with significant anx-iety reduction at 12 months compared to assignment tocontrol [40]. Similarly, state and trait anxiety decreasedamong participants with elevated blood pressure in astudy of a 12-week Tai Chi program, compared with sed-entary controls [41]. However, participants in these trialswere not experiencing clinically significant anxiety priorto intervention.
Depression may co-occur with anxiety [2, 9, 42, 43],and a number of comprehensive reviews of the literatureon exercise for depression have been conducted [44–46].However, there have been relatively few reviews of theliterature on exercise for anxiety. Those that exist havenot distinguished studies that targeted anxious individualsa priori nor have they provided a critical analysis of thequality of the research. Reviews that included results ofexercise interventions on anxiety outcomes typically havefound a robust and beneficial relationship [47, 48]. How-ever, these reviews have primarily included studies ofnonanxious participants, and the clinical significance ofreduced anxiety in nonanxious individuals is question-able. Other reviews have failed to differentiate single-bout and chronic exercise [48] or anxious and nonanxiousindividuals [49]. In one recent review [50], only studies ofindividuals with diagnosed anxiety disorders were includ-ed, possibly omitting important information from thosewith significant anxiety but without a specific diagnosis.A critical review is needed in order to establish the qualityand quantity of available evidence that this potentiallyvaluable intervention is effective for treating anxiousindividuals.
The purpose of this review is to describe and criticallyevaluate published exercise interventions targeting individualswith elevated anxiety or with a diagnosis of an anxiety disor-der. We also provide a review of meta-analyses of researchconcerning the relationship between exercise and anxiety, tocomplement our review of the randomized clinical trials(RCTs) that have been conducted targeting participants withelevated anxiety levels.
Method
We conducted a systematic search (July 2014) for RCTs inwhich participants were preselected on the basis of either adiagnosis of an anxiety disorder or elevated symptoms of anx-iety and then randomized to treatment with exercise as one ofthe treatment arms of the trial. These criteria were chosen sothat all experimental data concerning exercise as an interven-tion for anxious individuals would be included.
ann. behav. med.

Inclusion Criteria
We included all RCTs that met the following criteria: (1) arti-cle published in English in a peer-reviewed journal, (2) par-ticipants were at least 18 years old, (3) participants had ele-vated anxiety symptoms using a validated assessment instru-ment or were diagnosed with an anxiety disorder, (4) exerciseintervention consisted of >1 exercise sessions, and (5) anxietywas an outcome measure. Several studies have examined theimmediate effects of single bouts of exercise on anxiety [37,38, 51], which were not included in this review. We did in-clude RCTs of participants with posttraumatic stress disorder(PTSD), although DSM-5 now classifies PTSD separatelyfrom anxiety disorders [1].
Procedures
We first conducted a comprehensive search using CINAHL,EMBASE, MEDLINE, PsycINFO, and the Cochrane Library.Articles were identified with titles or abstracts that includedterms, or variants thereof, from each of the following groups:(1) physical activity or exercise, (2) anxiety or phobia or panic,and (3) randomly or randomized or clinical trial. These arti-cles were compiled in an EndNote database. Next, everyunique abstract in the database was examined to determinewhether any inclusion criteria for the review were unequivo-cally unmet (e.g., study of children or nonhumans, partici-pants without elevated anxiety, etc.). Those articles werediscarded, and the remaining studies were retained for dataextraction. A random subset of articles (N=25) was selectedfor double review, to confirm that the articles should be ex-cluded and to establish inter-rater reliability. No discrepancieswere observed during this double review (100 % agreement).If there was any uncertainty about whether inclusion criteriawere met, the article was retained for further examination.
Next, two randomly assigned raters independentlyreviewed the full text of each remaining article and removedthose in which basic inclusion criteria were not met (e.g.,absence of an exercise intervention). We also removed publi-cations from consideration that either did not report anxietyoutcomes or did not compare exercise to a control or compar-ison group. This level of review was conducted using a stan-dardized form enumerating the inclusion criteria. Some of thestudies reviewed during this step allowed individuals to par-ticipate if they had either elevated anxiety or another condition(e.g., depression, medical comorbidities). In these cases, weeliminated studies that did not provide data on anxiety-relatedoutcomes specifically for the participants with elevated pre-treatment anxiety.
Each of the remaining publications was randomly assignedto two reviewers for data extraction. Information gathered inthis step included study sample characteristics, experimentaldesign, measures of anxiety, modality, intensity, and duration
of exercise, methodological features such as intention to treat,blinding, and allocation concealment, primary (i.e., anxiety-related) and secondary outcomes, and results. Extracted datawere compiled on a standardized form and reviewed for inter-rater discrepancies, which reviewing authors resolved via mu-tual discussion. In the rare instances in which discrepanciesremained after this discussion, these were resolved by a thirdindependent rater.
During this process, if multiple publications were found tobe referring to the same RCT, a final round of data extractionwas conducted. A third reviewer, treating the articles as asingle study, extracted data that was submitted for discrepancyresolution with the preceding reviewers. Thus, if critical infor-mation had only been reported in one of the publications, thequality of the RCTwas evaluated on the basis of all availablestudy data.
Study quality and relative risk of bias from design of eachRCTs were also assessed using the PEDro Scale [52], a widelyused instrument to rate the overall quality of RCTs. PEDroscores are summarized across domains, and those with higherscores (range 0–10) are considered to have better quality.Briefly, after the first PEDro item, specification of eligibilitycriteria, the remaining ten items are worth 1 point apiece andcomprise the following criteria: random allocation of partici-pants to groups, allocation concealment, similarity of groupsat baseline, blinding of participants, blinding of intervention-ists, blinding of assessors of at least one key outcome, obtain-ment of a key outcome variable from 85 % or more partici-pants, intention-to-treat data collection and analysis, resultsreported for between-group differences on at least one keyoutcome, and point measurements and measurements of var-iability reported for at least one key outcome. Because of ourselection criteria, all studies automatically received a pointeach for randomizing participants to conditions and forreporting between-group differences on a key outcome. How-ever, all studies also lost 2 points total for items 5 (blinding ofall subjects) and 6 (blinding of all therapists), which were notrelevant, as participants were randomized to receive exerciseand the interventionists delivering the exercise treatment ob-viously could not be blinded to treatment condition.
Review of Meta-analyses
In addition to our review of individual RCTs, we also sur-veyed the existing meta-analyses on exercise and anxiety.Our article search initially returned 203 unique records thatwere either review articles or meta-analyses. We includedmeta-analyses identified through our search that met similarcriteria to the RCTs: anxiety as a primary focus of the meta-analysis, exercise as an intervention for anxiety, adult partici-pants, and random assignment to treatment groups, in which atleast one treatment was exercise. Our literature search did notreveal any meta-analyses that concerned both elevated anxiety
ann. behav. med.
symptoms (not diagnoses alone) and multiple sessions of ex-ercise. Because of the few meta-analyses and critical reviewsin the area, we elected not to exclude meta-analyses that per-mitted single-bout exercise interventions.
Results
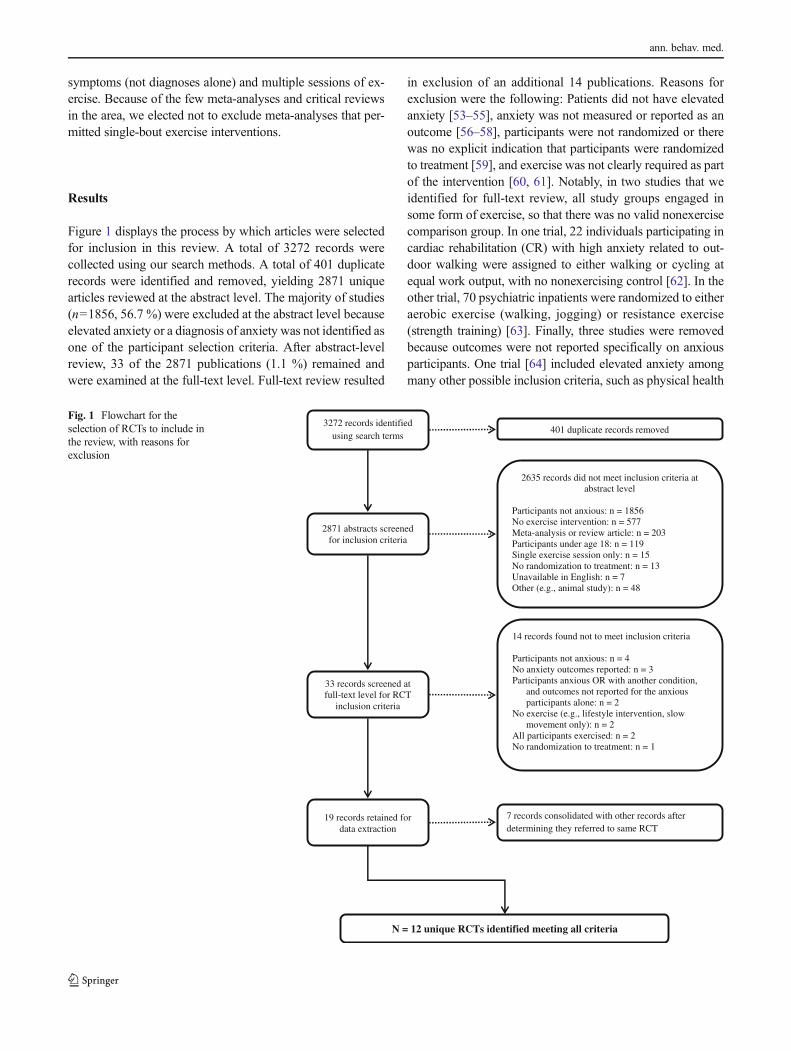
Figure 1 displays the process by which articles were selectedfor inclusion in this review. A total of 3272 records werecollected using our search methods. A total of 401 duplicaterecords were identified and removed, yielding 2871 uniquearticles reviewed at the abstract level. The majority of studies(n=1856, 56.7 %) were excluded at the abstract level becauseelevated anxiety or a diagnosis of anxiety was not identified asone of the participant selection criteria. After abstract-levelreview, 33 of the 2871 publications (1.1 %) remained andwere examined at the full-text level. Full-text review resulted
in exclusion of an additional 14 publications. Reasons forexclusion were the following: Patients did not have elevatedanxiety [53–55], anxiety was not measured or reported as anoutcome [56–58], participants were not randomized or therewas no explicit indication that participants were randomizedto treatment [59], and exercise was not clearly required as partof the intervention [60, 61]. Notably, in two studies that weidentified for full-text review, all study groups engaged insome form of exercise, so that there was no valid nonexercisecomparison group. In one trial, 22 individuals participating incardiac rehabilitation (CR) with high anxiety related to out-door walking were assigned to either walking or cycling atequal work output, with no nonexercising control [62]. In theother trial, 70 psychiatric inpatients were randomized to eitheraerobic exercise (walking, jogging) or resistance exercise(strength training) [63]. Finally, three studies were removedbecause outcomes were not reported specifically on anxiousparticipants. One trial [64] included elevated anxiety amongmany other possible inclusion criteria, such as physical health
3272 records identified using search terms
2871 abstracts screened for inclusion criteria
2635 records did not meet inclusion criteria at abstract level
Participants not anxious: n = 1856 No exercise intervention: n = 577 Meta-analysis or review article: n = 203 Participants under age 18: n = 119 Single exercise session only: n = 15 No randomization to treatment: n = 13 Unavailable in English: n = 7 Other (e.g., animal study): n = 48
33 records screened at full-text level for RCT
inclusion criteria
N = 12 unique RCTs identified meeting all criteria
14 records found not to meet inclusion criteria
Participants not anxious: n = 4 No anxiety outcomes reported: n = 3 Participants anxious OR with another condition,
and outcomes not reported for the anxious participants alone: n = 2
No exercise (e.g., lifestyle intervention, slow movement only): n = 2
All participants exercised: n = 2 No randomization to treatment: n = 1
401 duplicate records removed
19 records retained for data extraction
7 records consolidated with other records after determining they referred to same RCT
Fig. 1 Flowchart for theselection of RCTs to include inthe review, with reasons forexclusion
ann. behav. med.
Tab
le1
Sum
maryof
random
ized
clinicaltrials
Author
Num
ber
Country
Anxiety
inclusion
criteria
% Female
Age
(M)
Exercisecondition(s)
Control
condition(s)
Modality
Co-
interventio
nFrequency
Duration/intensity
Broman-Fulks
etal.,2008
35USA
Symptom
sof
high
anxietysensitivity
7919
Aerobic:b
risk
walking
orjogging
None
Sixsessions
over
2weeks
20min,60–90
%HRR
Waitlist
Broocks
etal.,1998
Bandelowetal.,2000
Broocks
etal.,2003
46Germany
Diagnosisof
PDwith
agoraphobia
5033
Aerobic:running
None
Four+weekly
sessions
over
10weeks
4-miroute,gradual
pace
increase
encouraged
1.Clomipramine
2.Placebo
Carmelietal.,
2009
24Israel
“Diagnosed
with
anxiety”
6251
Aerobic:b
icycleor
treadm
illNone
Three
sessions
weeklyfor
26weeks
35min,50–70
%HRR
1.Leisure
program
focused
onstability,flexibility,
balance
2.Vocationalactivities
Goldinetal.,2012
Jazaierietal.,2012
Goldinetal.,2013
56USA
Diagnosisof
SAD,
moderateor
more;
fear
in5+
social
situations
5233
Aerobic:g
ymexercise
None
Three
weekly
sessions
for
8weeks
Not
specified,
unsupervised
Mindfulness-based
stress
reduction—
1-dayretreat
andeightw
eekly
sessions,150
mina
Gutierrez
etal.,2012
60Sp
ain
Symptom
sof
anxiety,
moderateor
more;
comorbid
depression
100
64Aerobic:g
roup
exercise
None
6monthsof
increasing
sessions,one
tothreeweekly
50–60min,60–
85%
HRRat
endof
study
Waitlist
Herring
etal.,2011
Herring
etal.,2012
30USA
Diagnosisof
GAD
100
23Resistance(RET)
group:
legpresses,
curls,extensions;
Aerobic(A
ET)
group:
cycling
None
Twelve
sessions
over
6weeks
RET:1
6min,
gradualincrease
from
50%
of1R
MAET:equalwork
output
toRET
Waitlist
Hovland
etal.,2013
36Norway
Diagnosisof
PD81
38Com
binedaerobicand
resistance:g
roup
exercise
None
Three
weekly
sessions
for
12weeks
90min,60–80
%HRR
Group
CBTforPD
Kim
etal.,2013
28USA
Symptom
sof
PTSD
9746
Mindfulness-based
stretching
anddeep
breathingexercise
(MBX)
None
Twoweekly
sessions
for
8weeks
60min,gradually
increasing
intensity
Nointerventio
nor
waitlist
identified
Merom
etal.,2008
Phongsavan
etal.,2008
85Australia
DiagnosisofGAD,PD,
orSA
D78
39Participant’s
choice
Group
CBT
5days
aweekfor
8weeks
encouraged
30min,“moderate”
intensity
encouraged,
unsupervised
Group
CBTplus
healthy
eatin
geducation
(GCBT+ED)
Oldridgeetal.,1991
Oldridgeetal.,1995
201
USA
Symptom
sof
anxiety,
moderate,with
depressive
symptom
s
1154
Aerobic:cardiac
rehabilitation
Group
CBT,
relaxatio
ntraining
Twoweekly
sessions
for
8weeks
50min
Usualcare
bylocalp
hysician
Smits
etal.,2008
60USA
Symptom
sof
high
anxietysensitivity
7521
Aerobic:treadmill
Cognitiv
erestructuring
(subsample)
Sixsessions
over
2weeks
26min
at70
%HRR
Waitlist
Wedekindetal.,2010
75Germany
Diagnosisof
PD69
32Aerobic:running
Randomized
toparoxetineor
placebo
Three
weekly
sessions
for
10weeks
45min
each,
gradualintensity
increase
encouraged
Relaxationtraining,daily
plus
once
weeklywith
atrainer
Author
ITTused
%Attrition
Blin
dedoutcom
eassessment
EXsupervised
Fitnessim
proved
PEDro
scalescore
Anxiety
outcom
eFindings
ann. behav. med.
Tab
le1
(contin
ued)
Author
ITTused
%Attrition
Blindedoutcom
eassessment
EXsupervised
Fitnessim
proved
PEDro
scalescore
Anxiety
outcom
eFindings
Broman-Fulks
etal.,2008
N31
N/A
Y?c
4ASI-R
ASI-R:exercisebetterthan
waitlist.
exercise
27.92(15.36),waitlist41.0
(25.68)
Broocks
etal.,1998
Bandelowetal.,2000
Broocks
etal.,2003
Yb
20Y
Partial
N7
BAI
CGI
PAS
HAM-A
HAM-A
,BAI:EXandclom
ipramine
betterthan
placebo;
nodifference
betweenEXandCL.
PAS(observer)andCGI:
Clomipraminebetterthan
EX,both
betterthan
placebo.
Carmelietal.,
2009
N33
YY
?c4
HAM-A
(modified)
HAM-A
:Decreased
atposttestin
exercise
group(50%)andleisure
program
group(37.5%),butn
otcontrolg
roup
(0%).
Goldinetal.,2012
Jazaierietal.,2012
Goldinetal.,2013
N25
N/A
N?c
4LSA
S-SR
SIAS-S
LSA
S-SR
,SIA
S-S:
both
groups
improved,nosignificantd
ifference
betweengroups.A
bout
25%
ofparticipantshadclinically
significantimprovem
entinSA
D.
Gutierrez
etal.,2012
N5
N/A
YN
5HAM-A
(Spanish)
HAM-A
:exercisegroupsignificantly
improved
atposttest(p<0.01
for
participantswith
minor
anxiety,
p<0.05
formajor
anxiety).N
ochange
incontrolg
roup.
Herring
etal.,2011
Herring
etal.,2012
Y0
YY
RETgrouponly
7PO
MS
PSWQ
POMS-tensionscores:R
ETbetterthan
waitlist.N
SforAET.
PSWQ:exerciseconditionsbetterthan
waitlistwhengrouped,butp
airw
ise
NS.
Hovland
etal.,2013
Y3
YY
Y7
ACQ
BAI
BSQ
MI
STAI
STAI,BAI:no
group×tim
eeffect.
ACQ;B
SQ;M
I:CBTshow
edmore
anxietyreductionthan
exercise.
Kim
etal.,2013
Y5
N/A
Y?c
5PC
L-C
PCL-C:M
BXbetterthan
aerobic
exercise
group(reduced
bymeanof
−13.6)
atposttest;effectm
aintained
8weeks
afterinterventio
n
Merom
etal.,2008
Phongsavan
etal.,2008
N52
NN
N5
DASS
-21
DASS
-21:
Allgroups
improved.N
osignificantg
roup
differencesin
anxiety;
change
scores
were−6
.1(exercise)
vs.−
4.6(control)at
posttest.
Oldridgeetal.,1991
Oldridgeetal.,1995
N7
N/A
YY
5PO
MS
STAI
STAI-State:exercise
betterthan
UCat
8weeks
butN
Sat4,8,and
12months.
POMStension-anxiety:
exercise
better
than
UCat8weeks
butN
Sat
12months.
ann. behav. med.
problems or depression, and anxiety outcomes were not re-ported separately. Similarly, one study [65] selected partici-pants on the basis of any nonpsychotic DSM diagnosis, andanother study [66] enrolled patients with elevated symptomsof anxiety or depression, and these groups were not distin-guished from one another.
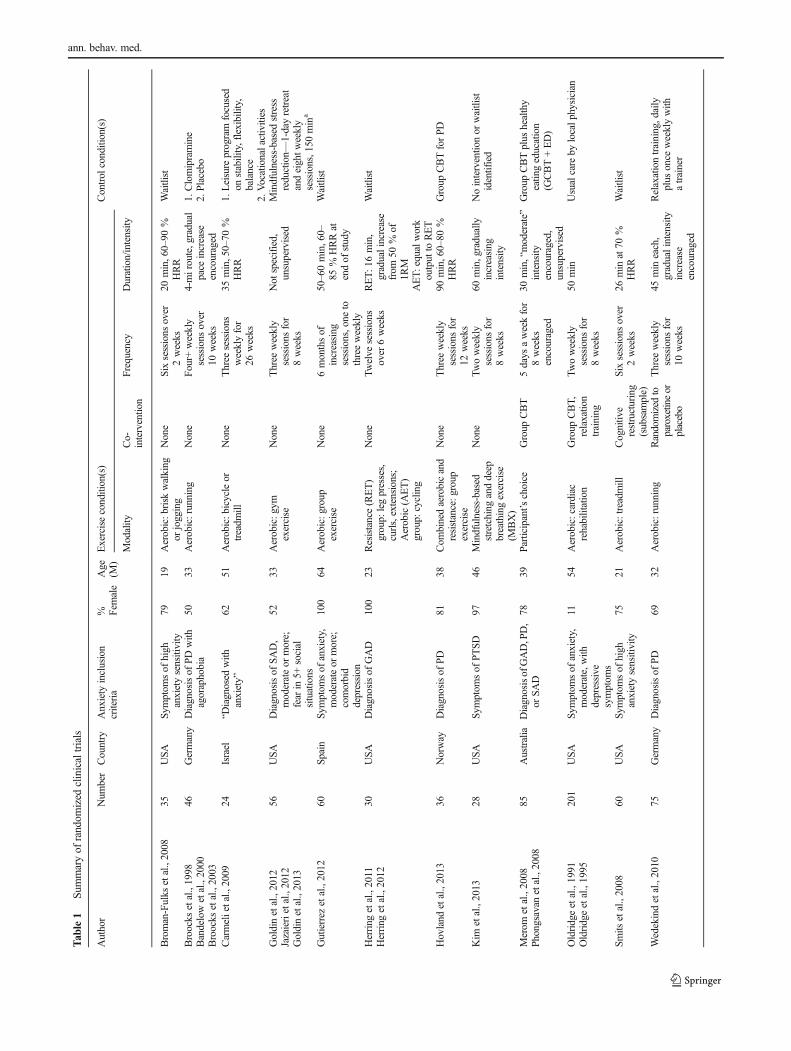
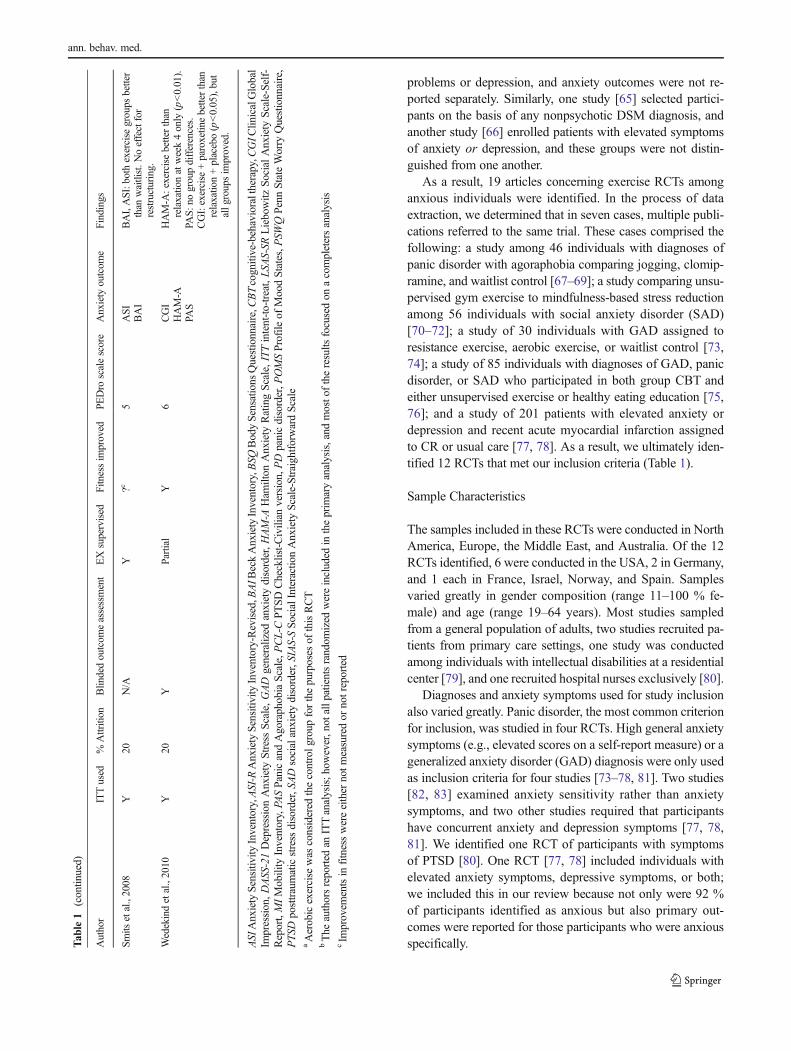
As a result, 19 articles concerning exercise RCTs amonganxious individuals were identified. In the process of dataextraction, we determined that in seven cases, multiple publi-cations referred to the same trial. These cases comprised thefollowing: a study among 46 individuals with diagnoses ofpanic disorder with agoraphobia comparing jogging, clomip-ramine, and waitlist control [67–69]; a study comparing unsu-pervised gym exercise to mindfulness-based stress reductionamong 56 individuals with social anxiety disorder (SAD)[70–72]; a study of 30 individuals with GAD assigned toresistance exercise, aerobic exercise, or waitlist control [73,74]; a study of 85 individuals with diagnoses of GAD, panicdisorder, or SAD who participated in both group CBT andeither unsupervised exercise or healthy eating education [75,76]; and a study of 201 patients with elevated anxiety ordepression and recent acute myocardial infarction assignedto CR or usual care [77, 78]. As a result, we ultimately iden-tified 12 RCTs that met our inclusion criteria (Table 1).
Sample Characteristics
The samples included in these RCTs were conducted in NorthAmerica, Europe, the Middle East, and Australia. Of the 12RCTs identified, 6 were conducted in the USA, 2 in Germany,and 1 each in France, Israel, Norway, and Spain. Samplesvaried greatly in gender composition (range 11–100 % fe-male) and age (range 19–64 years). Most studies sampledfrom a general population of adults, two studies recruited pa-tients from primary care settings, one study was conductedamong individuals with intellectual disabilities at a residentialcenter [79], and one recruited hospital nurses exclusively [80].
Diagnoses and anxiety symptoms used for study inclusionalso varied greatly. Panic disorder, the most common criterionfor inclusion, was studied in four RCTs. High general anxietysymptoms (e.g., elevated scores on a self-report measure) or ageneralized anxiety disorder (GAD) diagnosis were only usedas inclusion criteria for four studies [73–78, 81]. Two studies[82, 83] examined anxiety sensitivity rather than anxietysymptoms, and two other studies required that participantshave concurrent anxiety and depression symptoms [77, 78,81]. We identified one RCT of participants with symptomsof PTSD [80]. One RCT [77, 78] included individuals withelevated anxiety symptoms, depressive symptoms, or both;we included this in our review because not only were 92 %of participants identified as anxious but also primary out-comes were reported for those participants who were anxiousspecifically.T
able1
(contin
ued)
Author
ITTused
%Attrition
Blindedoutcom
eassessment
EXsupervised
Fitnessim
proved
PEDro
scalescore
Anxiety
outcom
eFindings
Smits
etal.,2008
Y20
N/A
Y?c
5ASI
BAI
BAI,ASI:b
othexercise
groups
better
than
waitlist.N
oeffectfor
restructuring.
Wedekindetal.,2010
Y20
YPartial
Y6
CGI
HAM-A
PAS
HAM-A
:exercisebetterthan
relaxationatweek4only
(p<0.01).
PAS:
nogroupdifferences.
CGI:exercise
+paroxetin
ebetterthan
relaxation+placebo(p<0.05),but
allg
roupsim
proved.
ASI
AnxietySensitiv
ityInventory,ASI-R
AnxietySensitiv
ityInventory-Revised,B
AIB
eckAnxietyInventory,BSQ
BodySensations
Questionnaire,C
BTcognitive-behavioraltherapy,C
GIC
linicalGlobal
Impression,DASS-21DepressionAnxiety
StressScale,GAD
generalized
anxietydisorder,HAM-A
Ham
ilton
Anxiety
RatingScale,ITTintent-to-treat,LSA
S-SR
Liebowitz
SocialAnxiety
Scale-Self-
Report,MIMobility
Inventory,PA
SPanicandAgoraphobiaScale,PCL-C
PTSDChecklist-Civilian
version,PDpanicdisorder,P
OMSProfile
ofMoodStates,P
SWQPenn
StateWorry
Questionnaire,
PTSD
posttraumaticstress
disorder,SADsocialanxietydisorder,S
IAS-SSocialInteractio
nAnxiety
Scale-StraightforwardScale
aAerobicexercise
was
considered
thecontrolg
roup
forthepurposes
ofthisRCT
bThe
authorsreported
anITTanalysis;h
owever,not
allp
atientsrandom
ized
wereincluded
intheprim
aryanalysis,and
mosto
ftheresults
focusedon
acompletersanalysis
cIm
provem
entsin
fitnesswereeither
notm
easuredor
notreported
ann. behav. med.

Six studies assessed pretreatment anxiety using structureddiagnostic interviews, and five studies relied on self-reportmeasures. One study reported that participants had been “di-agnosed with anxiety” without providing further information[79].
Exercise Interventions
Aerobic exercise was the most common exercise modality,employed in eight RCTs (66 %) and in tandem or comparedto resistance exercise in two others. Six of the RCTs reportedexercise intensity, ranging from 50 to 90 % of maximum heartrate or work output. The length of the exercise interventionswas also highly variable and ranged from2weeks to 6months.In one RCT [70–72], participants were directed to exercise ontheir own for 24 sessions over 8 weeks, but participants werenot observed and adherence to the exercise prescription appar-ently was not measured. In their study design, aerobic exercisewas used a control group and compared to mindfulness-basedstress reduction.
Exercise was supervised in eight of the RCTs. In two others[67–69, 84], participants had only one of three weekly runningsessions supervised by an exercise trainer. Exercise was notsupervised in the remaining two studies [70–72, 75, 76].
None of the RCTs compared different levels of exerciseintensity or examined a dose-response relationship betweenexercise intensity and anxiety reduction.
Two studies [62, 63] of anxious participants involved mul-tiple sessions of exercise but were excluded in the final reviewbecause all participants exercised, leaving no appropriatecomparison group. One study that was included [73, 74] com-pared two different modalities of exercise (aerobic vs. resis-tance), at equal work output, to a waitlist control. One otherstudy [80] compared participants completing a mindfulness-based stretching exercise routine to individuals receiving nointervention. Although the intensity of exercise was not stip-ulated as part of the intervention, the routine was characterizedas increasing in intensity over several weeks. Thus, we electedto include this study for further review.
In half of the studies, RCTs compared exercise interven-tions to a waitlist condition or no intervention or usual care. Inthe other studies, the efficacy of exercise was compared to thatof psychological interventions such as CBT [75, 76, 85], re-laxation training [84], mindfulness-based stress reduction[70–72], psychiatric medication or placebo [67–69], ornonexercise physical activity and vocational activities [79].
Study Quality
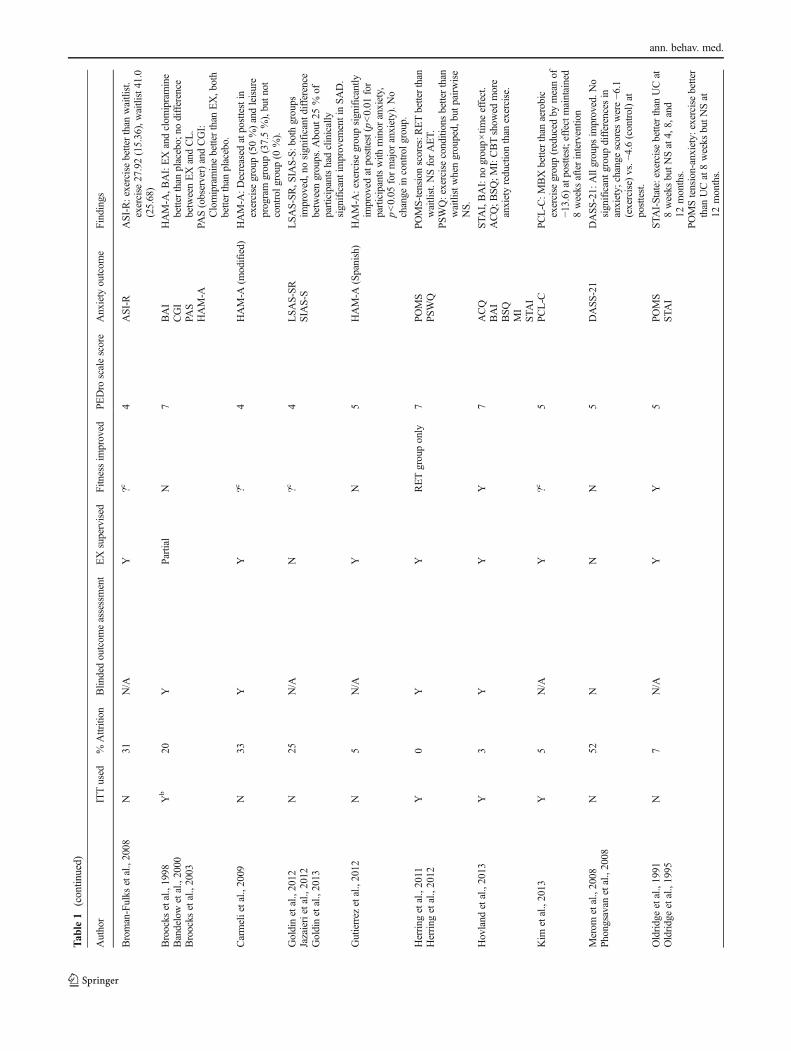
We compiled information concerning study design to deter-mine relative strength and quality of the RCTs. Blinded out-come assessments were conducted in 5 of the 12 studies; 5 ofthe remaining 7 used self-report outcome measures
exclusively. Similarly, only five studies controlled for outsideprotocol interventions for anxiety, directing participants todiscontinue or avoid starting another treatment prior to enter-ing the study. One of the RCTs [73, 74] found that 4 of 30participants had been exposed to an outside intervention dur-ing the study, although post hoc analyses showed no signifi-cant difference in primary outcomes between these and otherparticipants. A third of the studies included a co-interventionfor some or all participants, either medication or talk therapy.
With respect to sample size, only one of the 12 RCTs had asample size over 100 participants [77, 78]; in half of the stud-ies, fewer than 50 participants were included in the trial, withno more than 19 participants assigned to exercise. The partic-ipant attrition rate tended to be high, ranging from 0 to 52 %(mean attrition=18.4 %). Half the studies reported 20 % orgreater attrition, with three studies having more than a 30 %dropout rate. Intent-to-treat (ITT) analysis was employed inonly 50 % of studies. Of note, at least one study indicated thatan ITTanalysis was performed but reported primarily an anal-ysis of study completers [67–69]. Only one of the RCTs [85]made reference to allocation concealment duringrandomization.
Regarding quality ratings, PEDro scores were calculatedusing all applicable methodological characteristics, such asrandomization, blinding, attrition rate, analysis, and risk ofreporting bias. All PEDro scores for the RCTs fell within thelow to medium range, between 4 and 7. However, it is impor-tant to note that each study started with a minimum of 2 pointsbased on the eligibility criteria for inclusion in our review(random assignment to groups, outcomes reported on key var-iable), and studies were penalized 2 points because partici-pants and interventionists could not be blinded to treatmentcondition (exercise versus nonexercise control). In addition, itshould be noted that summary scores provide a limited assess-ment of study bias, particularly regarding threats to internalvalidity [86–88]. For example, contamination of exercise withconcurrent therapies was observed in some of the RCTs, suchas mindfulness training [80] and CBT [77, 78]; although thisis not counted as a methodological weakness within the PE-Dro scoring system, it poses a major threat to the internalvalidity of the study.
Anxiety Measures
Measures used to assess anxiety outcomes were highly vari-able. The most common instruments were the Hamilton Anx-iety Rating Scale (HAM-A) [89], with an original, modified,or translated version used in 4 of the 12 studies, and the BeckAnxiety Inventory (BAI) [90], used in 3 of the 12 studies.Other instruments included the Agoraphobia CognitionsQuestionnaire (ACQ) [91], Anxiety Sensitivity Inventory(ASI) [92], and ASI-Revised (ASI-R) [93]; Body SensationsQuestionnaire (BSQ) [91]; Clinical Global Impression (CGI);
ann. behav. med.

[94]; Depression Anxiety Stress Scale-21 (DASS-21) [95];Liebowitz Social Anxiety Scale-Self-Report (LSAS-SR)[96]; Mobility Inventory (MI) [97]; Panic and AgoraphobiaScale (PAS) [98]; PTSD Checklist-Civilian version (PCL-C)[99, 100]; Profile of Mood States (POMS) [101]; Penn StateWorry Questionnaire (PSWQ); [102]; Social Interaction Anx-iety Scale-Straightforward Scale (SIAS-S) [103]; and State-Trait Anxiety Inventory (STAI) [104]. Of note, five studiesemployed measures that were not used in any of the otherRCTs.
Results of the Exercise Interventions
Regarding the effectiveness of exercise interventions, 4 of the12 studies reported that the group receiving an exercise inter-vention showed superior anxiety outcomes compared to thoseof the control group, such as reduction in anxiety symptoms[80, 81] or reduction in anxiety sensitivity [82, 83]. ThreeRCTs showed no significant posttest difference between exer-cise and no-exercise groups [71, 72, 75, 76, 85]. In one ofthese cases [85], participants who performed aerobic and re-sistance showed comparable improvements on general anxi-ety symptom measures to those who received group CBT.However, on several measures of panic and agoraphobia, theCBT group showed greater improvement compared to theexercise group.
The remaining five studies also had mixed results. Onestudy of patients with intellectual disability in a residentialsetting [79] compared aerobic exercise with a leisure programconsisting of large body movements focused on stability, flex-ibility, and balance, as well as vocational activities as a controlcondition. The aerobic or leisure programs, but not vocationalactivities, were associated with significant reductions in anx-iety symptoms. Another RCT found that resistance exercise,but not aerobic exercise, yielded significant reductions insymptoms of GAD [73, 74]. In a study of patients recoveringfrom acute myocardial infarction, participants in CR and usualcare both exhibited similar reductions in anxiety symptoms,though those who engaged in the rehabilitation achieved im-provement sooner [77, 78]. Patients who enrolled in CR alsoparticipated in group-based CBT, however, so one cannot at-tribute these benefits specifically to exercise. In a study ofindividuals with panic disorder [67–69], clomipramineshowed equivalent or superior outcomes to aerobic exercise,although both treatments performed better than placebo. Fi-nally, in a comparison of exercise and relaxation training fortreating panic disorder [84], both treatment groups improved.Exercise showed greater improvement than relaxation trainingat 4 weeks, but this effect did not persist after 6, 8, and10 weeks.
Surprisingly, only four of the 12 RCTs reported significantimprovements in fitness after exercise treatment. One study[67–69] observed statistically significant improvements in
HAM-A and BAI scores for participants who either ran ortook clomipramine for 10 weeks, compared to controls, al-though a measure of fitness—timed running distance—wascomparable at posttest for all study groups, including thenonexercisers. In another study, Herring and colleagues [73,74] observed improvements in leg strength for resistance ex-ercisers but not aerobic exercisers. In three other studies, ex-ercise and control groups showed no significant differences infitness levels after training. In five studies, fitness levels orpostexercise improvements were not reported or measured.
Only two of the 12 RCTs included posttreatment follow-upto assess the sustained effects of the intervention. In one study[80], mindfulness-based exercise, but not aerobic exercise,showed a benefit at 8 weeks after training was completed. Inthe other study [77, 78] that found CR patients to show im-provements in anxiety compared to patients in usual care, thisdifference did not persist after the completion of the 8-weekprogram. The extent to which participants continued to exer-cise after the intervention period was not assessed in eitherstudy.
Review of Meta-analyses
From the 203 records identified as reviews or meta-analyses,we identified 5 published meta-analyses of studies of exerciseinterventions on anxiety [47–49, 105, 106] (Table 2). Themost inclusive of these meta-analyses included any type ofexercise intervention [106], whereas the most restrictive anal-ysis required a 3-week minimum of exercise participation[47]. Of the five meta-analyses, four concluded that exerciseis an effective treatment for anxiety, with effect sizes rangingfrom 0.22 (small) to 0.56 (moderate). However, participantswithout elevated anxiety or with no anxiety diagnosis wereincluded in these analyses. Because only one meta-analysisrestricted its scope to include only participants without elevat-ed anxiety [48], the utility of exercise to ameliorate anxiety inclinical samples could not be determined.
The remaining meta-analysis by Bartley and colleagues[105] addressed exercise RCTs among individuals with anydiagnosed anxiety disorder (aside from PTSD). Results foundno significant difference between exercise and control condi-tions for anxiety outcomes (ES=0.02). Moderator analysessuggest that this nonsignificant finding could be attributed tobetween-study heterogeneity. When analysis was restricted tostudies comparing exercise with placebo or waitlist controls,exercise showed a significant effect (SMD=1.42), but no sig-nificant difference was found for exercise compared to otheranxiolytic treatments such as CBT (SMD=−0.28). Thus, re-sults of the meta-analysis suggested that exercise providedsimilar benefit to other established treatments for anxietyand resulted in superior outcomes compared with treatmentor placebo treatment. It should be noted that moderator anal-yses based on a subsample of available studies are problematic
ann. behav. med.

because only seven studies met inclusion criteria for the fullanalysis and the analysis combined a heterogeneous group ofanxiety disorders into a single entity. RCTs among individualswith elevated anxiety symptoms but without an anxiety diag-nosis were not included, and the diagnoses present were sim-ilarly heterogeneous to those found in our current review.
Discussion
The present systematic review sought to describe what isknown about the efficacy of exercise for treatment of anxiety.Our search identified 12 RCTs and 5 meta-analyses that satis-factorily addressed this issue. We systematically reviewed theextant studies and extracted data on sample characteristics,study design, key methodological features, and anxiety out-comes. The majority of studies concluded that, as a treatmentfor elevated anxiety or anxiety disorders, exercise offers ben-efits comparable to established treatments, including medica-tion or CBT, and better than those of placebo or waitlist con-trol. However, review of available RCTs and meta-analysesrevealed that most studies suffer from significant methodolog-ical limitations that leave the issue of the use of exercise totreat anxiety unresolved.
Because of the heterogeneity in the definition of “anxiety”and “exercise” across the various RCTs, we believe that it isinappropriate to combine the data from these diverse studies ina quantitative way. We therefore elected to perform a compre-hensive, qualitative review of the extant studies. This ap-proach contrasts with prior reviews [49, 50], which haveattempted to evaluate the exercise-anxiety relationship statis-tically, including through meta-analysis. Given the importantmethodological differences and shortcomings of the studieswe identified, we instead elected to provide a more qualitativeand critical analysis of the existing literature.
One recent review [50] limited its scope to exercise RCTsonly among individuals with anxiety diagnoses. This grouplocated a total of 8 RCTs meeting their inclusion criteria.Three of the trials evaluated by this group [67–69, 75, 76,84] also met the inclusion criteria for the present review. Theremaining five studies did not meet our inclusion criteria.These studies comprised trials (a) among individuals withany nonpsychotic psychiatric diagnosis, not anxiety alone[65], (b) with a single-bout exercise intervention [37], (c) withno nonexercise control group [63], (d) with an interventionthat did not require exercise for all participants receiving it[60], and (e) with an outcome measure encompassing generalquality of life rather than anxiety specifically [57]. Our per-spective is that these studies by design cannot provide suffi-cient evidence either for or against the hypothesis that exercisereduces symptoms of anxiety in anxious individuals. In con-trast, nine additional RCTs were included in the presentT
able2
Meta-analyses
concerning
exercise-anxiety
relatio
nship
Study
Inclusioncriteria
Sam
ple
Results
RCTs
Only
Exercise
Control
Other
Studies
N
Bartleyetal.,2013
Yes
Morethan
onesession
Any
alternative
interventio
nAnxiety
d/ootherthan
PTSD
7407
Exerciseissimilar,ES=0.02.
Conn,2010
No
Any
nonacuteinterventio
nto
increase
physicalactiv
ityN/A
Noelevated
anxietyor
anxietyd/o
193789
Exerciseissuperior,E
S=0.22.
Herring
etal.,2010
Yes
Atleast3weeks
ofanyexercise
Nonexercise
comparison
conditionsonly
Sedentaryadultswith
chronicillness
402914
Exerciseissuperior,E
S=0.29.
Petruzzello
etal.,
1991
No
Any
exercise,singleor
multip
lebouts
N/A
N/A
104
3048
Exerciseiseffectiveforstateanxiety
(ES=0.24),
traitanxiety
(ES=0.34),and
psychophysiologicalcorrelatesof
anxiety
(ES=0.56).
Wipflietal.,
2008
Yes
Any
exercise,singleor
multip
lebouts
Any
alternative
interventio
nNoco-interventionforexercise
condition
493566
Exerciseissuperior,E
S=−0
.48.
ann. behav. med.

review. These studies comprised five exercise trials to reduceanxiety among individuals with anxiety diagnoses, to includesocial anxiety disorder [70–72], GAD [73, 74], PTSD [80],panic disorder [85], and any anxiety diagnosis [79]. In addi-tion, our review included four trials among individuals withelevated symptoms of anxiety [77, 78, 81] or anxiety sensitiv-ity [82, 83]. We believe that including these trials more accu-rately represents the available evidence concerning exercise asa treatment for anxiety.
Unlike depression, for which many RCTs exist and havebeen the subject of many reviews and meta-analyses [44–46],research on exercise in patients with anxiety is significantlymore limited. Furthermore, whereas depressive symptomsmay be conceptualized along a single continuum [107, 108],anxiety disorders represent distinct clusters of symptomswith-in a broad constellation of diagnoses. One exception to thispattern would be GAD. However, GAD and broad anxietysymptoms were studied in only three RCTs. The most com-monly represented disorder in our review, panic disorder (4 of12 RCTs), has a lifetime prevalence of less than 5 %, wellbelow the lifetime 30 % prevalence of anxiety disorders as awhole [2]. Because of the great heterogeneity in inclusioncriteria in exercise RCTs for anxiety, we cannot be confidentthat exercise will improve symptoms of anxiety in any givendiagnostic group.
We also observed great variation in exercise interventions,with studies involving different modes of exercise for differentdurations and varied intensities. We were surprised to discoverthat aerobic fitness often was not measured, and when it was,it often did not improve after exercise interventions, despitethe fact that anxiety was reduced. For example, participants inone study [67–69] showed lower HAM-A and BAI scoresamong participants assigned to running, but at 10-week post-test, their timed running distance was not different from con-trols. Interestingly, in the one RCT that compared two exercisemodalities [73, 74], resistance exercise showed better fitnessand lower POMS-T scores at posttest, but aerobic exercise didnot. Most studies failed to document improvements in cardio-respiratory function associated with exercise training (e.g.,changes in VO2 or submaximal heart rates at matching work-loads), which also is problematic, as such changes in physicalfitness would provide an important manipulation check toverify that the exercise intervention was sufficient to produceexpected cardiopulmonary benefits and improved functionalcapacity. Similarly, few studies used the same instruments tomeasure anxiety outcomes, and in many cases, these measuresappear to be specific to one population (e.g., those with panicsymptoms or PTSD symptoms), limiting generalizability.
Existing RCTs also had other methodological problemsthat limit our ability to draw definitive conclusions. One thirdof the trials did not control for outside interventions for anx-iety. For example, in the one RCT that had a sample of over100 participants, participants assigned to exercise also
received CBT and relaxation training concurrently [77, 78],which seriously detracted from the methodological quality ofthe study. Another RCTonly delivered exercise in the contextof a mindfulness intervention [80]. Attrition of 20% or greaterwas noted in half of the trials. Intent-to-treat analysis wasreported in only half of the studies, with one of these reportingprimarily an analysis of completers [67–69]. In many cases,self-report outcomes were the only posttest measures of anx-iety employed. Taken together, examination of what are wide-ly considered the most important methodological quality indi-cators revealed that existing studies have significant method-ological weaknesses and a moderate risk of bias.
One way to determine the strength of exercise as an effec-tive treatment for anxious individuals is to observe a dose-response effect. Such evidence would be critical to establish-ing a direct treatment effect of exercise on anxiety. Unfortu-nately, this important issue has been minimally explored in theliterature. A prior meta-analysis [49], which found an overallbenefit of exercise for anxiety reduction, attempted to quantifya dose-response relationship. One trial of individuals withpanic disorder did compare directly the effects of a single boutof light or heavy physical activity on panic symptoms, findingthat more intense activity did have a greater antipanic effect[37]. However, this study enrolled a sample of only 18 partic-ipants and had no nonexercise control group. Because no rig-orous RCTs have conducted a direct, experimental compari-son of exercise volume (intensity and duration) on anxiousparticipants, an optimal dose of exercise cannot be deter-mined. Randomizing participants to differing intensities orfrequencies of exercise is needed to determine the optimaldose of exercise to reduce anxiety. This approach has beenused successfully in research on exercise for depression[109] but has not been investigated for anxiety.
Our review revealed that exercise interventions often wereunsupervised and that intensity and frequency of exercise wastypically either not reported or not manipulated as part of thestudy design. For example, some running interventions en-couraged participants to increase their pace over severalweeks, but only one session per week was supervised[67–69, 84], and in other RCTs, participants were directed todo exercise of their choosing [70–72]. Of note, some trials ofsingle-bout exercise have suggested that a dose-response ef-fect may exist, though findings have been equivocal. For ex-ample, one study found that healthy individuals completing20 min of low-intensity resistance exercise with weightliftingmachines had immediate reductions in state anxiety, whereasanxiety increased among the high-intensity group [110]. An-other study found significant reductions in anxiety sensitivityfor healthy individuals completing low- and high-intensitytreadmill exercise, with greater reductions among the high-intensity group [111]. Importantly, individuals can give differ-ing self-reports of their affective response after a single bout ofexercise, depending on how soon this self-report is solicited
ann. behav. med.

[112]. Further research to address the optimal dose of exerciseis needed.
Few studies have examined exercise as an adjunctivetreatment. We identified one RCT [75, 76] that examinedthe effect of exercise compared to education controlamong anxious participants receiving group CBT; notreatment group differences were observed. Another study[84] used a 2×2 design to explore the utility of aerobicexercise and an SSRI (paroxetine), separately and com-bined, with no differences for combined versus unimodaltreatment. Further research is needed to confirm whetheradding exercise to other treatments confers a benefit toindividuals with anxiety.
The issue of the mechanism(s) by which exercise affectsanxiety seldom has been studied, although several potentialpathways have been identified [113]. Potential physiologi-cal explanations include regulation of the hypothalamic-pituitary-adrenal (HPA) axis, increases in serotonergic andnoradrenergic levels in the brain, and endogenous opioidrelease. Psychological factors may also play a key role.For example, interventions such as CBT for anxiety oftenemploy exposure to feared sensations or situations, com-bined with prevention of maladaptive responses that pro-vide short-term relief [24]. The mechanism by which CBTis effective remains poorly understood [114]. However, inthis case, the intervention is intended to promote habitua-tion and a reduction in anxiety symptoms [24]. Indeed, twoof the studies we reviewed [82, 83] aimed to reduce anxietysensitivity through aerobic exercise, which can create sensa-tions similar to anxiety or panic (e.g., rapid heartbeat). Inter-estingly, one study that did not meet our inclusion criteria [62]involved individuals participating in CR who had elevatedanxiety specific to walking. Anxiety improved among indi-viduals who were assigned to walk for exercise but not inthose assigned to cycling, suggesting that exposure to a spe-cific feared stimulus may have helped. Alternatively, exercisemay improve self-efficacy through progressive positive feed-back, such as fitness gains [113]. Existing evidence fromRCTs does not adequately address whether exercise can re-duce anxiety via improvements in fitness and related physio-logical changes, psychological changes, or a combination offactors; indeed, the relative paucity of evidence leaves openthe question of whether a direct mechanism for exercise toreduce anxiety exists.
We included studies in our review in which participants’anxiety symptoms did not necessarily meet criteria for anx-iety disorders in DSM-5. For example, two of the identifiedRCTs address high anxiety sensitivity, a marker that mayserve as a precursor to panic attacks or GAD. In addition,oneRCT [80]was conducted among individualswith PTSD,a diagnosis which is now in a separate classification fromanxiety disorders [1]. We included these RCTs to addressanxiety as broadly as possible, in light of the scarcity of the
existing literature and the heterogeneity of populations sam-pled; we also did not identify any completed RCTs amongindividuals with DSM-5-diagnosed anxiety disorders.
Although a few RCTs included participants with one ofseveral anxiety diagnoses, no single study addressed the issueof whether one anxiety disorder was more responsive to exer-cise than another, or whether situational anxiety symptomsresponded as well to exercise as did persistent symptoms ofanxiety. Testing for such moderator effects would be valuablebut would require trials with larger samples than have beenused to date.
The present review has several limitations. We did not per-sonally contact researchers about unpublished RCTs, so thepotential bias of the “file drawer effect” [115, 116] could notbe determined. However, because such unpublished studieswere likely to suffer from significant methodological weak-nesses or yield “null” effects, it is unlikely that these additionaldata would alter our conclusions. Second, we limited oursearch to individuals of ages 18 years and over. Althoughwe elected to not include children in our review, we performedan additional search of our database for studies of exercise inanxious children. We failed to identify a single RCT of exer-cise training in persons under 18 years old that met our inclu-sion criteria. Therefore, we cannot comment on the potentialbenefits of exercise for children with elevated anxiety andsuggest that this is an important, and understudied, area forfuture research.
In summary, findings from the present review suggestthat exercise could be a useful, affordable, accessible treat-ment for anxiety. However, there appears to be a paucityof data from well-designed RCTs, and the methodologicallimitations in the existing trials of exercise preclude draw-ing definitive conclusions about its effectiveness. Indeed,the existing literature is marked by small trials with weakinternal validity. At present, the existing body of evidenceis not of sufficient scientific rigor to recommend it as atreatment among individuals with clinically elevated anxi-ety. Future research will require robust experimental de-signs and greater attention to critical methodological de-tails including appropriate control groups, adequate samplesizes, use of intent-to-treat analysis, blinding of assessors,allocation concealment, monitoring of exercise adherenceand intensity, documentation of aerobic “training effects,”and selection of well-validated instruments to assess anxietybefore and following treatment.
Acknowledgments The authors wish to acknowledge José Sandoval,DukeUniversity, for his assistance with article review and data extraction.This manuscript was supported, in part, by Grant HL080664-01 from theNational Institutes of Health, Bethesda, Maryland.
Authors’ Statement of Conflict of Interest Authors Stonerock, Hoff-man, Smith, and Blumenthal declare that they have no conflicts ofinterest.
ann. behav. med.
References
1. Diagnostic and Statistical Manual of Mental Disorders: DSM-5.Washington, DC: American Psychiatric Association; 2013.
2. Kessler RC, Petukhova M, Sampson NA, Zaslavsky AM, WittchenH-U. Twelve-month and lifetime prevalence and lifetime morbidrisk of anxiety and mood disorders in the United States. Int JMethods Psychiatr Res. 2012; 21: 169-184.
3. Haller H, Cramer H, Lauche R, Gass F, Dobos G. The prevalenceand burden of subthreshold generalized anxiety disorder: a system-atic review. BMC Psychiatry. 2014; 14: 128.
4. Stein MB, Roy-Byrne PP, Craske MG, et al. Functional impact andhealth utility of anxiety disorders in primary care outpatients. MedCare. 2005; 43: 1164-1170.
5. Tolmunen T, Lehto SM, Julkunen J, Hintikka J, Kauhanen J. Traitanxiety and somatic concerns associate with increased mortalityrisk: a 23-year follow-up in aging men. Ann Epidemiol. 2014; 24:463-468.
6. Roest AM, Martens EJ, de Jonge P, Denollet J. Anxiety and risk ofincident coronary heart disease: a meta-analysis. J Am Coll Cardiol.2010; 56: 38-46.
7. Janszky I, Ahnve S, Lundberg I, Hemmingsson T. Early-onset de-pression, anxiety, and risk of subsequent coronary heart disease: 37-year follow-up of 49,321 young Swedish men. J Am Coll Cardiol.2010; 56: 31-37.
8. Roest AM,Martens EJ, Denollet J, de Jonge P. Prognostic associationof anxiety post myocardial infarction with mortality and new cardiacevents: a meta-analysis. Psychosom Med. 2010; 72: 563-569.
9. Frasure-Smith N, Lespérance F. Depression and anxiety as predic-tors of 2-year cardiac events in patients with stable coronary arterydisease. Arch Gen Psychiatry. 2008; 65: 62-71.
10. Frasure-Smith N. In-hospital symptoms of psychological stress aspredictors of long-term outcome after acute myocardial infarction inmen. Am J Cardiol. 1991; 67: 121-127.
11. Tully PJ, Baker RA, Knight JL. Anxiety and depression as riskfactors for mortality after coronary artery bypass surgery. JPsychosom Res. 2008; 64: 285-290.
12. Tully P, Baker R, Turnbull D, Winefield H. The role of depressionand anxiety symptoms in hospital readmissions after cardiac sur-gery. J Behav Med. 2008; 31: 281-290.
13. Szekely A, Balog P, Benko E, et al. Anxiety predicts mortality andmorbidity after coronary artery and valve surgery—a 4-year follow-up study. Psychosom Med. 2007; 69: 625-631.
14. Moser DK, McKinley S, Riegel B, et al. Relationship of persistentsymptoms of anxiety to morbidity and mortality outcomes in patientswith coronary heart disease. Psychosom Med. 2011; 73: 803-809.
15. Watkins LL, Koch GG, Sherwood A, et al. Association of anxietyand depression with all‐cause mortality in individuals with coronaryheart disease. J Am Heart Assoc. 2013; 2.
16. Rothenbacher D, Hahmann H, Wusten B, Koenig W, Brenner H.Symptoms of anxiety and depression in patients with stable coro-nary heart disease: prognostic value and consideration of pathoge-netic links. Eur J Cardiovasc Prev Rehabil. 2007; 14: 547-554.
17. Strik JJ, Denollet J, Lousberg R, Honig A. Comparing symptoms ofdepression and anxiety as predictors of cardiac events and increasedhealth care consumption after myocardial infarction. J Am CollCardiol. 2003; 42: 1801-1807.
18. Shibeshi WA, Young-Xu Y, Blatt CM. Anxiety worsens prognosisin patients with coronary artery disease. J Am Coll Cardiol. 2007;49: 2021-2027.
19. Markovitz JH, Matthews KA, Kannel WB, Cobb JL, D’AgostinoRB. Psychological predictors of hypertension in the FraminghamStudy. Is there tension in hypertension? J AmMed Assoc. 1993; 270:2439-2443.
20. Kawachi I, Sparrow D, Vokonas PS, Weiss ST. Symptoms of anx-iety and risk of coronary heart disease. The Normative Aging Study.Circulation. 1994; 90: 2225-2229.
21. McCarron P, Gunnell D, Harrison GL, Okasha M, Davey Smith G.Temperament in young adulthood and later mortality: prospectiveobservational study. J Epidemiol Community Health. 2003; 57: 888-892.
22. Bonnet F, Irving K, Terra J-L, et al. Anxiety and depression areassociated with unhealthy lifestyle in patients at risk of cardiovas-cular disease. Atherosclerosis. 2005; 178: 339-344.
23. Jonas BS, Franks P, Ingram DD. Are symptoms of anxiety anddepression risk factors for hypertension? Longitudinal evidencefrom the national health and nutrition examination survey I epide-miologic follow-up study. Arch Fam Med. 1997; 6: 43-49.
24. Barlow DH. Clinical handbook of psychological disorders: A step-by-step treatment manual. 5th ed. New York, NY: The GuilfordPress; 2014.
25. Barlow DH, Gorman JM, Shear M, Woods SW. Cognitive-behavioral therapy, imipramine, or their combination for panic dis-order: a randomized controlled trial. J Am Med Assoc. 2000; 283:2529-2536.
26. Butler AC, Chapman JE, Forman EM, Beck AT. The empiricalstatus of cognitive-behavioral therapy: a review of meta-analyses.Clin Psychol Rev. 2006; 26: 17-31.
27. Kapczinski F, Lima MS, Souza JS, Schmitt R. Antidepressants forgeneralized anxiety disorder. Cochrane Database Syst Rev. 2003.
28. Stahl SM, Gergel I, Li D. Escitalopram in the treatment of panicdisorder: a randomized, double-blind, placebo-controlled trial. JClin Psychiatry. 2003; 64: 1322-1327.
29. Davidson JRT, Bose A, Korotzer A, Zheng H. Escitalopram in thetreatment of generalized anxiety disorder: double-blind, placebo con-trolled, flexible-dose study. Depression Anxiety. 2004; 19: 234-240.
30. Baldwin DS, Anderson IM, Nutt DJ, et al. Evidence-based guide-lines for the pharmacological treatment of anxiety disorders: recom-mendations from the British Association for Psychopharmacology.J Psychopharmacol. 2005; 19: 567-596.
31. Pampallona S, Bollini P, Tibaldi G, Kupelnick B, Munizza C.Patient adherence in the treatment of depression. Br J Psychiatry.2002; 180: 104-109.
32. Gunter RW, Whittal ML. Dissemination of cognitive-behavioraltreatments for anxiety disorders: overcoming barriers and improv-ing patient access. Clin Psychol Rev. 2010; 30: 194-202.
33. Caspersen CJ, Powell KE, Christenson GM. Physical activity, exer-cise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep. 1985; 100: 126-131.
34. Goodwin RD. Association between physical activity and mentaldisorders among adults in the United States. Prev Med. 2003; 36:698-703.
35. De Moor MHM, Beem AL, Stubbe JH, Boomsma DI, De GeusEJC. Regular exercise, anxiety, depression and personality: apopulation-based study. Prev Med. 2006; 42: 273-279.
36. Strickland JC, Smith MA. The anxiolytic effects of resistance exer-cise. Front Psychol. 2014; 5: 753.
37. Esquivel G, Diaz-Galvis J, Schruers K, et al. Acute exercise reducesthe effects of a 35%CO2 challenge in patients with panic disorder. JAffect Disord. 2008; 107: 217-220.
38. Yeung RR. The acute effects of exercise on mood state. JPsychosom Res. 1996; 40: 123-141.
39. Berger BG, Owen DR. Relation of low and moderate intensity ex-ercise with acute mood change in college joggers. Percept MotSkills. 1998; 87: 611-621.
40. King AC, Taylor CB, Haskell WL. Effects of differing intensitiesand formats of 12 months of exercise training on psychologicaloutcomes in older adults. Health Psychol. 1993; 12: 292-300.
41. Tsai J-C,WangW-H, Chan P, et al. The beneficial effects of Tai ChiChuan on blood pressure and lipid profile and anxiety status in a
ann. behav. med.
randomized controlled trial. J Altern Complement Med. 2003; 9:747-754.
42. Stavrakaki C, Vargo B. The relationship of anxiety and depression: areview of the literature. Br J Psychiatry. 1986; 149: 7-16.
43. ZungWW,Magruder-Habib K, Velez R, AllingW. The comorbidityof anxiety and depression in general medical patients: a longitudinalstudy. J Clin Psychiatry. 1990; 51: 77-80.
44. Cooney GM, Dwan K, Greig CA, et al. Exercise for depression.Cochrane Database Syst Rev. 2013; 9: Cd004366.
45. Mead GE, Morley W, Campbell P, et al. Exercise for depression.Cochrane Database Syst Rev. 2009:Cd004366.
46. Lawlor DA, Hopker SW. The effectiveness of exercise as an inter-vention in the management of depression: systematic review andmeta-regression analysis of randomised controlled trials. BMJ.2001; 322: 763.
47. Herring MP, O’Connor PJ, Dishman RK. The effect of exercisetraining on anxiety symptoms among patients: a systematic review.Arch Intern Med. 2010; 170: 321-331.
48. Conn VS. Anxiety outcomes after physical activity interventions:meta-analysis findings. Nurs Res. 2010; 59.
49. Wipfli BM, Rethorst CD, Landers DM. The anxiolytic effects ofexercise: a meta-analysis of randomized trials and dose-responseanalysis. J Sport Exerc Psychol. 2008; 30: 392-410.
50. Jayakody K, Gunadasa S, Hosker C. Exercise for anxiety disorders:systematic review. Br J Sports Med. 2014; 48: 187-196.
51. Focht BC, Koltyn KF. Influence of resistance exercise of differentintensities on state anxiety and blood pressure. Med Sci SportsExerc. 1999; 31: 456-463.
52. Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M.Reliability of the PEDro scale for rating quality of randomized con-trolled trials. Phys Ther. 2003; 83: 713-721.
53. Annesi JJ, Gorjala S. Association of reduction in waist circumfer-ence with normalization of mood in obese women initiating exercisesupported by the Coach Approach protocol. South Med J. 2010;103: 517-521.
54. Hale BS, Raglin JS. State anxiety responses to acute resistancetraining and step aerobic exercise across 8 weeks of training. JSports Med Phys Fitness. 2002; 42: 108-112.
55. Smith JA, Greer T, Sheets T, Watson S. Is there more to yoga thanexercise? Altern Ther Health Med. 2011; 17: 22-29.
56. Mussgay L, Schmidt F, Morad E, Ruddel H. Does aerobic exercisemodulate baroreflex sensitivity in patients with anxiety and somati-zation disorders? Homeost Health Dis. 2003; 42: 277-287.
57. Oeland A-M, Laessoe U, Olesen AV, Munk-Jorgensen P. Impact ofexercise on patients with depression and anxiety. Nordic JPsychiatry. 2010; 64: 210-217.
58. Wedekind D, Sprute A, Broocks A, et al. Nocturnal urinary cortisolexcretion over a randomized controlled trial with paroxetine vs.placebo combined with relaxation training or aerobic exercise inpanic disorder. Curr Pharm Des. 2008; 14: 3518-3524.
59. Gaul-Alacova P, Boucek J, Stejskal P, et al. Assessment of the in-fluence of exercise on heart rate variability in anxiety patients.Neuroendocrinol Lett. 2005; 26: 713-718.
60. Lambert RA, Harvey I, Poland F. A pragmatic, unblindedrandomised controlled trial comparing an occupational therapy-led lifestyle approach and routine GP care for panic disorder treat-ment in primary care. J Affect Disord. 2007; 99: 63-71.
61. Kim J-H, Yang H, Schroeppel S. A pilot study examining the effectsof Kouk Sun Do on university students with anxiety symptoms.Stress Health. 2013; 29: 99-107.
62. Faulkner J, Westrupp N, Rousseau J, Lark S. A randomized con-trolled trial to assess the effect of self-pacedwalking on task-specificanxiety in cardiac rehabilitation patients. J Cardiopulm RehabilPrev. 2013; 33: 292-296.
63. Martinsen EW, Hoffart A, Solberg OY. Aerobic and non-aerobicforms of exercise in the treatment of anxiety disorders. StressMed. 1989; 5: 115-120.
64. Murphy SM, Edwards RT, Williams N, et al. An evaluation of theeffectiveness and cost effectiveness of the National Exercise ReferralScheme inWales, UK: a randomised controlled trial of a public healthpolicy initiative. J Epidemiol Community Health. 2012; 66: 745-753.
65. Sexton H, Maere A, Dahl NH. Exercise intensity and reduction inneurotic symptoms: a controlled follow-up study. Acta PsychiatrScand. 1989; 80: 231-235.
66. Goldstein-Shirley J, Brown M. Intervention of light, exercise andvitamins for mixed anxiety-depression. Communicating NursingResearch. Palm Springs, CA; 2002.
67. Bandelow B, Broocks A, Pekrun G, et al. The use of the Panic andAgoraphobia Scale (P & A) in a controlled clinical trial.Pharmacopsychiatry. 2000; 33: 174-181.
68. Broocks A, Bandelow B, Pekrun G, et al. Comparison of aerobicexercise, clomipramine, and placebo in the treatment of panic dis-order. Am J Psychiatr. 1998; 155: 603-609.
69. Broocks A, Meyer T, Opitz M, et al. 5-HT1A responsivity in pa-tients with panic disorder before and after treatment with aerobicexercise, clomipramine or placebo. Eur Neuropsychopharmacol.2003; 13: 153-164.
70. Goldin P, Ziv M, Jazaieri H, Gross JJ. Randomized controlled trialof mindfulness-based stress reduction versus aerobic exercise: ef-fects on the self-referential brain network in social anxiety disorder.Front Hum Neurosci. 2012.
71. Goldin P, Ziv M, Jazaieri H, Hahn K, Gross JJ. MBSR vs aerobicexercise in social anxiety: fMRI of emotion regulation of negativeself-beliefs. Soc Cogn Affect Neurosci. 2013; 8: 65-72.
72. Jazaieri H, Goldin PR, Werner K, Ziv M, Gross JJ. A randomizedtrial of MBSR versus aerobic exercise for social anxiety disorder. JClin Psychol. 2012; 68: 715-731.
73. Herring MP, Jacob ML, Suveg C, Dishman RK, O’Connor PJ.Feasibility of exercise training for the short-term treatment of gen-eralized anxiety disorder: a randomized controlled trial. PsychotherPsychosom. 2012; 81: 21-28.
74. Herring MP, Jacob ML, Suveg C, O’Connor PJ. Effects of short-term exercise training on signs and symptoms of generalized anxietydisorder. Ment Health Phys Act. 2011; 4: 71-77.
75. Merom D, Phongsavan P, Wagner R, et al. Promoting walking as anadjunct intervention to group cognitive behavioral therapy for anx-iety disorders—a pilot group randomized trial. J Anxiety Disord.2008; 22: 959-968.
76. Phongsavan P, Merom D, Wagner R, et al. Process evaluation in anintervention designed to promote physical activity among adultswith anxiety disorders: evidence of acceptability and adherence.Health Promot J Aust. 2008; 19: 137-143.
77. Oldridge N, Guyatt G, Jones N, et al. Effects on quality of life withcomprehensive rehabilitation after acute myocardial infarction. AmJ Cardiol. 1991; 67: 1084-1089.
78. Oldridge N, Streiner D, Hoffmann R, Guyatt G. Profile of moodstates and cardiac rehabilitation after acute myocardial infarction.Med Sci Sports Exerc. 1995; 27: 900-905.
79. Carmeli E, Barak S, Morad M, Kodesh E. Physical exercises canreduce anxiety and improve quality of life among adults with intel-lectual disability. Int Sport Med J. 2009; 10: 77-85.
80. Kim SH, Schneider SM, BevansM, et al. PTSD symptom reductionwith mindfulness-based stretching and deep breathing exercise: ran-domized controlled clinical trial of efficacy. J Clin EndocrinolMetab. 2013; 98: 2984-2992.
81. Gutiérrez CV, Luque GT, Medina GMÁ, et al. Influence of exerciseon mood in postmenopausal women. J Clin Nurs. 2012; 21: 923-928.
82. Broman-Fulks JJ, Storey KM. Evaluation of a brief aerobic exerciseintervention for high anxiety sensitivity. Anxiety Stress Coping.2008; 21: 117-128.
ann. behav. med.
83. Smits JAJ, Berry AC, Rosenfield D, et al. Reducing anxiety sensi-tivity with exercise. Depression Anxiety. 2008; 25: 689-699.
84. Wedekind D, Broocks A, Weiss N, et al. A randomized, controlledtrial of aerobic exercise in combination with paroxetine in the treat-ment of panic disorder.World J Biol Psychiatry. 2010; 11: 904-913.
85. Hovland A, Nordhus IH, Sjobo T, et al. Comparing physical exer-cise in groups to group cognitive behaviour therapy for the treat-ment of panic disorder in a randomized controlled trial. Behav CognPsychother. 2013; 41: 408-432.
86. Higgins JPT, Green S eds. Cochrane Handbook for SystematicReviews of Interventions, 5.1.0 [updated March 2011]: TheCochrane Collaboration, 2011. Available at www.cochrane-handbook.org.
87. Jüni P, Witschi A, Bloch R, Egger M. The hazards of scoring thequality of clinical trials for meta-analysis. J Am Med Assoc. 1999;282: 1054-1060.
88. Schulz KF, Chalmers I, Hayes RJ, Altman DG. Empirical evidenceof bias: dimensions of methodological quality associated with esti-mates of treatment effects in controlled trials. J Am Med Assoc.1995; 273: 408-412.
89. Hamilton M. The assessment of anxiety states by rating. Br J MedPsychol. 1959; 32: 50-55.
90. Beck AT, Steer RA. Manual for the Beck Anxiety Inventory. SanAntonio, TX: Psychological Corporation; 1990.
91. Chambless DL, Caputo GC, Bright P, Gallagher R. Assessment offear of fear in agoraphobics: the Body Sensations Questionnaire andthe Agoraphobic Cognitions Questionnaire. J Consult Clin Psychol.1984; 52: 1090-1097.
92. Reiss S, Peterson RA, Gursky DM, McNally RJ. Anxiety sensitiv-ity, anxiety frequency and the prediction of fearfulness. Behav ResTher. 1986; 24: 1-8.
93. Taylor S, Cox BJ. An expanded Anxiety Sensitivity Index: evidencefor a hierarchic structure in a clinical sample. J Anxiety Disord.1998; 12: 463-483.
94. Guy Wed. ECDEU Assessment Manual for Psychopharmacology-Revised. Rockville, MD: US Department of Health, Education, andWelfare, Public Health Service, Alcohol, Drug Abuse, and MentalHealth Administration; 1976.
95. Lovibond SH, Lovibond PF. Manual for the Depression AnxietyStress Scales. Sydney, N.S.W: Psychology Foundation ofAustralia; 1995.
96. Fresco DM, Coles ME, Heimberg RG, et al. The Liebowitz SocialAnxiety Scale: a comparison of the psychometric properties of self-report and clinician-administered formats. Psychol Med. 2001; 31:1025-1035.
97. Chambless DL, Caputo GC, Jasin SE, Gracely EJ, Williams C. Themobility inventory for agoraphobia.Behav Res Ther. 1985; 23: 35-44.
98. Bandelow B. Assessing the efficacy of treatments for panic disorderand agoraphobia. II. the Panic and Agoraphobia Scale. Int ClinPsychopharmacol. 1995; 10: 73-81.
99. Blanchard EB, Jones-Alexander J, Buckley TC, Forneris CA.Psychometric properties of the PTSD Checklist (PCL). Behav ResTher. 1996; 34: 669-673.
100. Weathers FW, Litz BT, Herman DS, Huska JA, Keane TM: ThePTSD Checklist (PCL). Reliability, validity, and diagnostic utility.Annual Convention of the International Society for Traumatic StressStudies. San Antonio; 1993.
101. McNair DM, Lorr M, Droppleman L. POMS: Profile of MoodStates. North Tonawanda, NY: Multi-Health Systems Inc; 1992.
102. Meyer TJ, Miller ML, Metzger RL, Borkovec TD. Developmentand validation of the Penn State Worry Questionnaire. Behav ResTher. 1990; 28: 487-495.
103. Rodebaugh TL, Woods CM, Heimberg RG. The reverse of socialanxiety is not always the opposite: the reverse-scored items of theSocial Interaction Anxiety Scale do not belong. Behav Ther. 2007;38: 192-206.
104. Spielberger CD, Gorsuch RL, Lushene R, Vagg PR, Jacobs GA.Manual for the State-Trait Anxiety Inventory. Palo Alto:Consulting Psychologists Press; 1983.
105. Bartley CA, Hay M, BlochMH. Meta-analysis: aerobic exercise forthe treatment of anxiety disorders. Prog Neuro-PsychopharmacolBiol Psychiatry. 2013; 45: 34-39.
106. Petruzzello SJ, Landers DM, Hatfield BD, Kubitz KA, Salazar W. Ameta-analysis on the anxiety-reducing effects of acute and chronicexercise: outcomes and mechanisms. Sports Med. 1991; 11: 143-182.
107. Santor DA, Zuroff DC, Ramsay JO, Cervantes P, Palacios J.Examining scale discriminability in the BDI and CES-D as a func-tion of depressive severity. Psychol Assess. 1995; 7: 131-139.
108. Slade T, Andrews G. Latent structure of depression in a communitysample: a taxometric analysis. Psychol Med. 2005; 35: 489-497.
109. Dunn AL, Trivedi MH, Kampert JB, Clark CG, Chambliss HO.Exercise treatment for depression: efficacy and dose response. AmJ Prev Med. 2005; 28: 1-8.
110. Bartholomew J, Linder D. State anxiety following resistance exer-cise: the role of gender and exercise intensity. J Behav Med. 1998;21: 205-219.
111. Broman-Fulks JJ, Berman ME, Rabian BA, Webster MJ. Effects ofaerobic exercise on anxiety sensitivity. Behav Res Ther. 2004; 42:125-136.
112. Masters KS, Spielmans GI, LaCaille RA, et al. Effects of home exer-cise on immediate and delayed affect and mood among rural individ-uals at risk for type 2 diabetes. J Soc Behav Health Sci. 2011; 5: 1-16.
113. Anderson E, ShivakumarG. Effects of exercise and physical activityon anxiety. Front Psychiatry. 2013; 4: 27.
114. Arch JJ, Craske MG. Acceptance and commitment therapy and cog-nitive behavioral therapy for anxiety disorders: different treatments,similar mechanisms? Clin Psychol Sci Pract. 2008; 15: 263-279.
115. Rosenthal R. The file drawer problem and tolerance for null results.Psychol Bull. 1979; 86: 638-641.
116. Easterbrook PJ, Gopalan R, Berlin JA, Matthews DR. Publicationbias in clinical research. Lancet. 1991; 337: 867-872.
ann. behav. med.