evolving trends in atrial fibrillation management and...
TRANSCRIPT
Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 1
Evolving Trends in Atrial
Fibrillation Management and Stroke Risk Reduction
Emerging Challenges in Primary Care: Update 2013 1
Faculty
• Jan Basile, MD − Professor of Medicine, Seinsheimer Cardiovascular Health Program, Division of
General Internal Medicine, Medical University of South Carolina, Ralph H. Johnson VA Medical Center, Charleston, SC
• Keith C. Ferdinand MD, FACC, FAHA - Chair, National Forum for Heart Disease and Stroke Prevention, Professor of
Clinical Medicine, Tulane University School of Medicine, Tulane Heart and Vascular Institute, New Orleans, LA
• Valerian L. Fernandes, MD, MRCP, FACC - Associate Professor of Medicine, Medical University of South Carolina, Director-
Cardiac Catheterization Laboratories, Ralph H. Johnson VA Medical Center, Charleston, SC
• Louis Kuritzky, MD − Clinical Assistant Professor, Department of Community Health & Family
Medicine, University of Florida, Gainesville, FL
2
Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 2
Faculty Disclosure
3
• Jan Basile, MD − Speaker – Boehringer Ingelheim, Daiichi Sankyo, Forest Labs, Takeda − Consultant - Forest Labs, Takeda
• Keith C. Ferdinand MD, FACC, FAHA - Consultant – Takeda, Novartis, Forest, Daiichi Sankyo - Speaker – AstraZeneca, Takeda
• Valerian L. Fernandes, MD, MRCP, FACC - Spouse is a Consultant for Ipsen
• Louis Kuritzky, MD − Nothing to disclose
Learning Objectives
• Use the CHADS2 Score to Risk Stratify AF patients
• Choose appropriate pharmacologic Rx for AF patients
• Recognize the role of catheter ablation in AF patients
• Effectively manage antithrombotic therapy in the perioperative setting
4
Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 3
ARS #1 Clinical Scenario: Steve E.
Steve E, a 79 y/o hispanic male with a history of HTN and a left hemispheric stroke 2 years ago, was asymptomatic until 2 days ago when he developed intermittent palpitations and presented to your office. EKG: AF at 120 bpm. Steve’s CHADS2 score is:
1) 1 2) 2 3) 4 4) 6 5) Not sure 5
ARS # 2
1) All of the newer agents are statistically superior to warfarin for stroke risk reduction 2) The major reason to provide warfarin is because overall costs with warfarin are much less than other agents 3) In the absence of head-to-head trials, it is not possible to know if any one of the newer agents is superior to another 4) Major bleeding risk with newer agents is markedly less than with warfarin
A 62 year dermatologist has recently been diagnosed with AF. He has hypertension and type 2 diabetes, both of which are well controlled. Being a physician, he asks "I've read about all the treatments; which is the best treatment for my AF?" You should answer
6
Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 4
ARS #3 Perioperative Management of Tomas, a 62 Y.O. with
AF, HTN, DM Tomas is undergoing CV surgery. His INR has been in the therapeutic range about 75% of the time on warfarin 5 mg/d. What should be done about his warfarin dose perioperatively?
1) Continue 5 mg/d without interruption 2) Discontinue warfarin 3 days preop, resume 12-24
hrs after adequate hemostasis 3) Discontinue 5 days preop, resume 12-24 hrs after
adequate hemostasis 4) Switch to clopidogrel 75 mg/d 3 days preop, then
resume warfarin 12-24 hrs after adequate hemostasis and discontinue clopidogrel
7
1. 80 year old with persistent atrial fibrillation 2. 68 year old symptomatic patient after 2 trials of
antiarrhythmic Rx with paroxysmal atrial fibrillation 3. Obese asymptomatic patient with sleep apnea and
paroxysmal atrial fibrillation 4. 64 year old with EF of 35% and LA size of 5.5 cms 5. 74 year old hypertensive with atrial fibrillation for the past
2 years and symptomatic palpitations
ARS #4 Which Patient is Best Suited for RF Ablation?
8

Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 5
Allison has new onset AF resistant to several steps of pharmacotherapy. She has well controlled HTN and T2DM. She has a high level of awareness of her rapid heart rate, which impairs her QOL. She has heard of catheter ablation. If she undergoes successful ablation and is in sinus rhythm, what should be done about anticoagulation? 1) Anticoagulation can be omitted once she is in sinus rhythm 2) Anticoagulation should be used for 4-6 weeks post ablation 3) Anticoagulation should be used indefinitely despite sinus
rhythm 4) Anticoagulation should be used for 2-3 months post
ablation
ARS #5 Clinical Scenario: Allison M A 58 y.o. Woman with Resistant Symptomatic AF
9
On a scale of 1 to 5, please rate how confident you would be in treating a patient with atrial
fibrillation.
1. Not at all confident 2. Slightly confident 3. Moderately confident 4. Pretty much confident 5. Very confident
10

Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 6
AF: Major Teaching Points • Stroke reduction with antithrombotic therapy (warfarin,
dabigatran, rivaroxaban, apixaban) is VERY SUBSTANTIAL (±66% or more)
• ICH risk with warfarin is VERY LOW (<1%/yr) and EVEN LOWER with new agents (dabigatran, rivaroxaban, apixaban)
• Perioperative regimens for antithrombotic and antiplatelet therapies are specific to individual agents
• Catheter ablation for AF is promising, and often provides excellent symptom relief
• Antithrombotic therapy post-ablation is continued indefinitely, despite restoration of sinus rhythm 11
Atrial Fibrillation
What’s The Risk of Stroke?
12

Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 7
..
AF Warfarin Trials: Reduction in Stroke Rates and Mortality
Hart et al. Ann Intern Med. 1999;131:492-501.
Stro
ke/y
r (%
)
AFASAK SPAF BAATAF CAFA SPINAF EAFT
• N=2,900 • Mean age = 69 • 20% > age 75 • Stroke rates reduced 62%
2.7 3.8 1.4 3.2 2.5
8.9
warfarin
placebo
13
All cause mortality RRR = 26%
Intracranial Hemorrhage During Long-Term Anticoagulation With Warfarin
Levine MN, et al. “Hemorrhagic Complications of Anticoagulant Rx” Chest 2001;119:108S-121S
ICH
%/Y
ear
Fihn (AF)
INR <3.0
INR <3.0
Fihn (>75)
Turpie (PV*)
SPAF II (≤75)
SPAF II (AF)
Pengo(PV*)
SPAF II (>75)
SPAF III (AF)
INR 2.0-4.5
INR 2.0-3.0 INR
2.5-3.5
INR 3.0-4.5
INR 2.0-4.5
INR 2.0-4.5
1%
14

Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 8
Atrial Fibrillation: Gaining Confidence in Risk Stratification
How to Use the CHADS2
Score
15
Case: Martha T, a 74 y.o. Black Female
• Brought by 46 y.o. daughter for HTN & DM re-check
• Hx: No prior arrhythmia, but reports ‘my heart seems to go a little faster sometimes in these last couple months’
• Sister deceased due to stroke • Meds: metformin, simvastatin, chlorthalidone,
lisinopril
16

Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 9
Martha T, a 74 y.o. Black Female: PE • HR 94, irregularly irregular • BP 138/84 • BMI: 30.4 • Cardiac: No Murmur • Chest: Clear • Abd: WNL • Neuro: WNL • Extremities: no edema, pulses good
17
Martha T, a 74 y.o. Black Female: LAB • EKG Today: Atrial Fib HR 94 • Previous EKG (1 yr ago)
♦ NSR (72) ♦ LVH (voltage) ♦ No-ST-T wave abnormalities
• CBC, CMP WNL (3 months ago) • A1c 7.3 (3 months prior) • TSH = 2.1, LDL = 80
18

Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 10
Martha T, a 74 y.o. Black Female with Diabetes and Hypertension
• What is Martha’s CHADS2 Score? 1) 1 2) 2 3) 4 4) Unsure 5) What’s a CHADS2 Score?
19
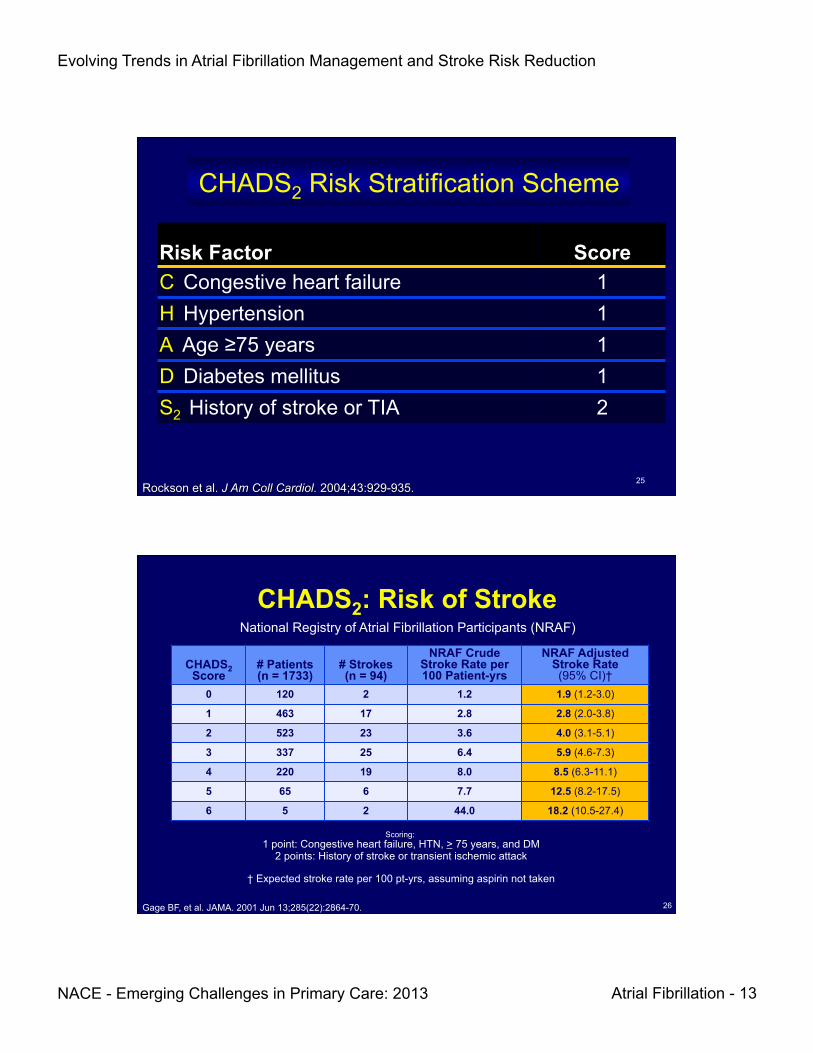
CHADS2 Risk Stratification Scheme
Risk Factor Score C Congestive heart failure 1 H Hypertension 1 A Age ≥75 years 1 D Diabetes mellitus 1 S2 History of stroke or TIA 2
Rockson et al. J Am Coll Cardiol. 2004;43:929-935. 20

Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 11
Why CHADS2 ?
“The CHADS2 score is the most validated risk scheme, having been independently tested
in at least 10 separate cohorts after its original derivation.”
You JJ, et al “Antithrombotic Therapy for Atrial Fibrillation” CHEST 2012;141(2)(Suppl):e531S-e575S
21
When
MIGHT THE CHA2DS2-VASc
Score Help?
22

Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 12
CHA2DS2-VASc Case Study
Tina is a 72 y.o. woman with incidentally discovered atrial fibrillation when pulse
irregularity was noted. She is asymptomatic, and takes no chronic medications. Her only
chronic medical problem is tinnitus, for which she receives no treatment. Will this patient be better served by CHADS or CHA2DS2-VASc?
23
Tina, a 72 y.o. White Female
• What is Tina’s CHADS2 Score? 1) 0 2) 1 3) 2 4) Unsure
24
Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 13
CHADS2 Risk Stratification Scheme
Risk Factor Score C Congestive heart failure 1 H Hypertension 1 A Age ≥75 years 1 D Diabetes mellitus 1 S2 History of stroke or TIA 2
Rockson et al. J Am Coll Cardiol. 2004;43:929-935. 25
CHADS2: Risk of Stroke
CHADS2 Score # Patients (n = 1733)
# Strokes (n = 94)
NRAF Crude Stroke Rate per 100 Patient-yrs
NRAF Adjusted Stroke Rate (95% CI)†
0 120 2 1.2 1.9 (1.2-3.0)
1 463 17 2.8 2.8 (2.0-3.8)
2 523 23 3.6 4.0 (3.1-5.1)
3 337 25 6.4 5.9 (4.6-7.3)
4 220 19 8.0 8.5 (6.3-11.1)
5 65 6 7.7 12.5 (8.2-17.5)
6 5 2 44.0 18.2 (10.5-27.4)
National Registry of Atrial Fibrillation Participants (NRAF)
Scoring: 1 point: Congestive heart failure, HTN, > 75 years, and DM
2 points: History of stroke or transient ischemic attack
† Expected stroke rate per 100 pt-yrs, assuming aspirin not taken
Gage BF, et al. JAMA. 2001 Jun 13;285(22):2864-70. 26

Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 14
Tina, a 72 y.o. White Female
• What is Tina’s CHA2DS2-VASc Score? 1) 1 2) 2 3) 4 4) Unsure
27
CHA2DS2-VASc Risk Factor Score C CHF 1 H HTN 1 A2 Age ≥75 years 2 D Diabetes mellitus 1 S2 History of stroke or TIA 2 V Vascular disease (MI, peripheral arterial disease, aortic atherosclerosis)
1
A Age 65-74 years old 1 Sc Sex category (female) 1
Lip GY, et al. Am J Med. 2010;123(6):484-488. Camm AJ, et al. Eur Heart J. 2010;31(19):2369-2429.
28

Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 15
CHA2DS2-VASc When CHADS2 Score 0
1 Year Follow-up 12 Years Follow-up
Person Yrs Events Stroke rate (95%CI) Person Yrs Events Stroke rate (95%CI)
CHADS2 score 0–1 40,272 1,405 3.49 (3.31–3.68) 187,200 4,599 2.46 (2.39–2.53)
CHA2DS2-VASc = 0 6,919 58 0.84 (0.65–1.08) 39,500 299 0.76 (0.68–0.85)
CHA2DS2-VASc = 1 8,880 159 1.79 (1.53–2.09) 45,926 662 1.44 (1.34–1.56)
CHA2DS2-VASc = 2 11,863 435 3.67 (3.34–4.03) 51,595 1,489 2.89 (2.74–3.04)
CHA2DS2-VASc = 3 11,473 660 5.75 (5.33–6.21) 45,799 1,933 4.22 (4.04–4.41)
CHA2DS2-VASc = 4 1,137 93 8.18 (6.68–10.02) 4,380 216 4.93 (4.32–5.64)
CHADS2 score = 0 17,327 275 1.59 (1.41–1.79) 92,531 1182 1.28 (1.21–1.35)
CHA2DS2-VASc = 0 6,919 58 0.84 (0.65–1.08) 39,500 299 0.76 (0.68–0.85)
CHA2DS2-VASc = 1 6,811 119 1.75 (1.46–2.09) 35,079 504 1.44 (1.32–1.57)
CHA2DS2-VASc = 2 3,347 90 2.69 (2.19–3.31) 16,710 353 2.11 (1.90–2.34)
CHA2DS2-VASc = 3 250 8 3.20 (1.60–6.40) 1,242 26 2.09 (1.43–3.07)
CHADS2 Score = 1 22,945 1,130 4.92 (4.65–5.22) 94,669 3417 3.61 (3.49–3.73)
CHA2DS2-VASc = 1 2,069 40 1.93 (1.42–2.64) 10,847 158 1.46 (1.25–1.70)
CHA2DS2-VASc = 2 8,516 345 4.05 (3.65–4.50) 34,885 1136 3.26 (3.07–3.45)
CHA2DS2-VASc = 3 11,223 652 5.81 (5.38–6.27) 44,557 1907 4.28 (4.09–4.48)
CHA2DS2-VASc = 4 1,137 93 8.18 (6.68–10.02) 4,380 216 4.93 (4.32–5.64)
Refines stroke risk stratification in AF patients: nationwide cohort
Olesen JB, Torp-Pedersen C, Hansen ML, Lip GY. Thromb Haemost. 2012 June;107(6):1172-9. 29
AF Rx as Per CHADS2 Score: AT9 (2012)
CHADS2
0
1
> 2
No Rx (2B)
Oral Anticoagulant (1B)
Oral Anticoagulant (1A)
Rx
You JJ, et al. CHEST 2012;141(2)(Suppl):e531S-e575S
If patient chooses treatment, then ASA 81-325 mg/d (2B)
If patient unwilling or unsuitable, then ASA + clopidogrel (2B)
If patient unwilling or unsuitable, then ASA + clopidogrel (1B)
Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 16
Fibrin Clot
XII
VII VIII
IX
XI
II
V
X
I
Unfractionated Heparin
Warfarin Low Molecular
Weight Heparin
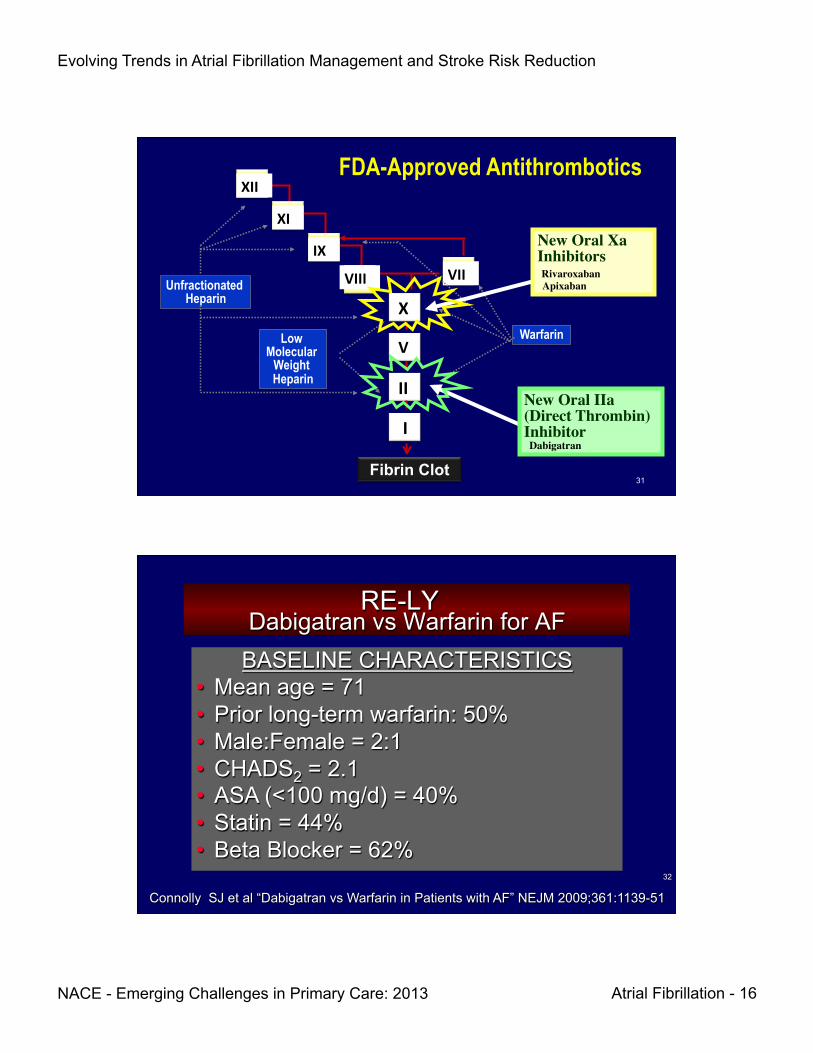
FDA-Approved Antithrombotics
New Oral IIa (Direct Thrombin) Inhibitor Dabigatran
New Oral Xa Inhibitors Rivaroxaban ��� Apixaban
31
RE-LY Dabigatran vs Warfarin for AF
BASELINE CHARACTERISTICS • Mean age = 71 • Prior long-term warfarin: 50% • Male:Female = 2:1 • CHADS2 = 2.1 • ASA (<100 mg/d) = 40% • Statin = 44% • Beta Blocker = 62%
Connolly SJ et al “Dabigatran vs Warfarin in Patients with AF” NEJM 2009;361:1139-51
32

Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 17
RE-LY Stroke/Systemic Embolism
Connolly SJ et al “Dabigatran vs Warfarin in Patients with AF” NEJM 2009;361:1139-51
0.05-
0.04-
0.03-
0.02-
0.01-
0.00- 0 6 12 18 24 30
HR
Months
RR = 0.66 p < 0.00l
Dabigatran 150 mg Dabigatran 110 mg Warfarin
33
RE-LY: Major Bleeding
3.5- 3.0- 2.5- 2.0- 1.5- 1.0- 0.5-
% major bleed
3.36% 2.71%
3.11%
warfarin dabigatran 110 mg bid
dabigatran 150 mg bid
p=0.31
p=0.003
Connolly SJ et al “Dabigatran vs Warfarin in Patients with AF” NEJM 2009;361:1139-51 34
Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 18
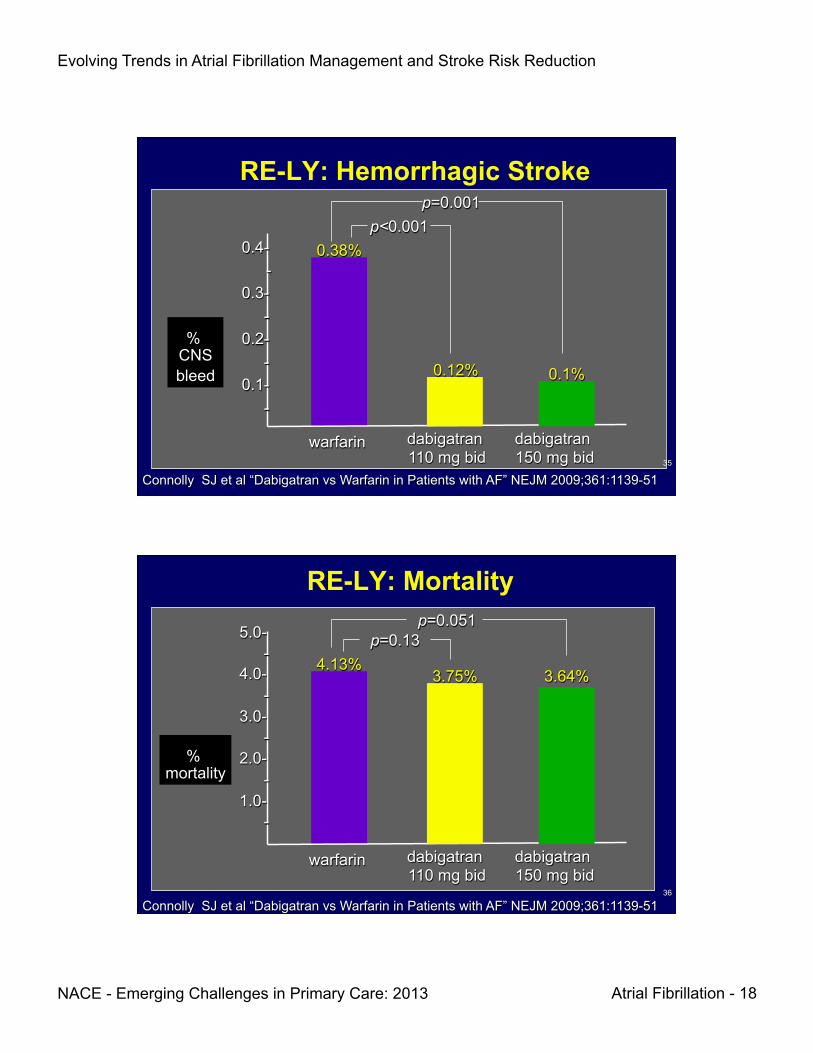
RE-LY: Hemorrhagic Stroke
0.4- - 0.3- - 0.2- - 0.1- -
% CNS bleed
0.38%
0.12% 0.1%
warfarin dabigatran 110 mg bid
dabigatran 150 mg bid
p<0.001 p=0.001
Connolly SJ et al “Dabigatran vs Warfarin in Patients with AF” NEJM 2009;361:1139-51 35
RE-LY: Mortality
5.0- - 4.0- - 3.0- - 2.0- - 1.0- -
% mortality
4.13% 3.75%
warfarin dabigatran 110 mg bid
dabigatran 150 mg bid
p=0.051 p=0.13
3.64%
Connolly SJ et al “Dabigatran vs Warfarin in Patients with AF” NEJM 2009;361:1139-51 36

Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 19
Dabigatran Dosing
• Dosing ♦ 150mg PO b.i.d.
• Renal impairment: • CrCL 15-30 mL/min : 75mg b.i.d. • CrCL <15 mL/min/dialysis: unknown
• Hepatic impairment: No dose adjustment
Dabigatran Prescribing Information 2010 37
ROCKET AF Rivaroxaban vs Warfarin for AF
• Study: High Risk AF pts (n=14,269) with Hx of stroke/TIA/embolism OR ≥2 of § CHF § Age ≥ 75 § DM § HTN
• Rx (≤ 32 months): § Rivaroxaban 20 mg QD
Ø 15 mg QD if eGFR 30-49 § Warfarin INR target 2.5 (INR 2.0-3.0)
Patel MR, et al N Engl J Med 2011;365(10):883-91 38
Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 20
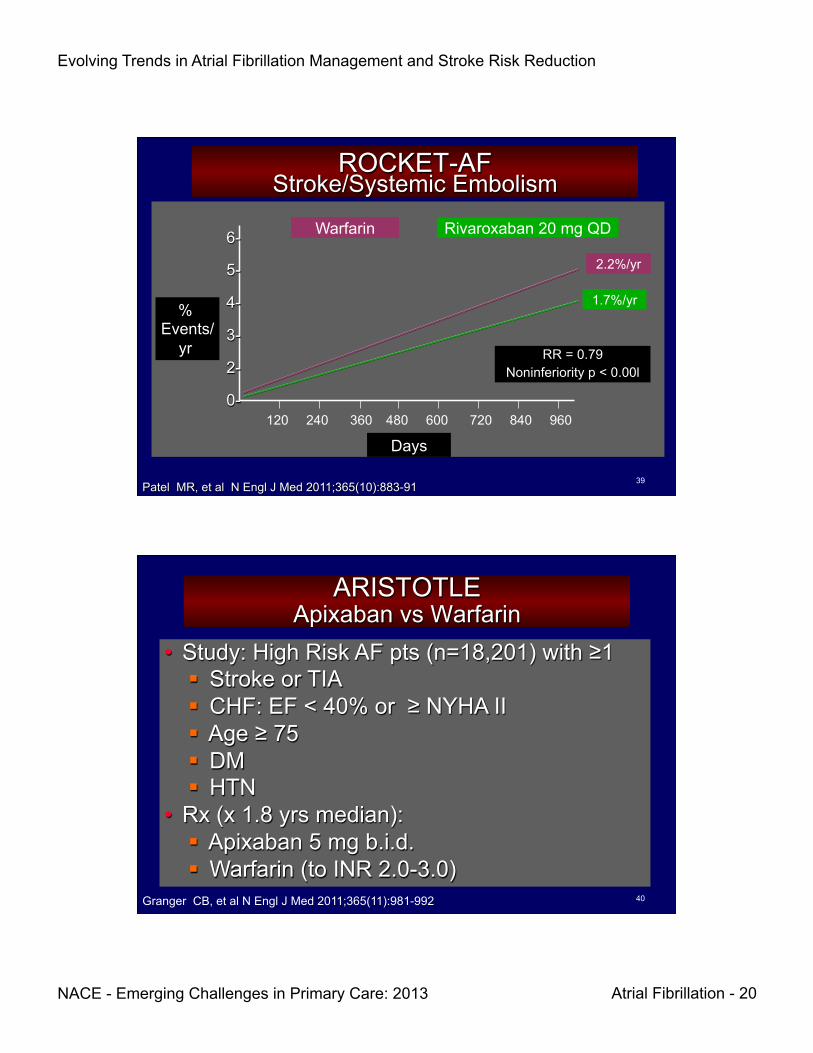
ROCKET-AF Stroke/Systemic Embolism
6-
5-
4-
3-
2-
0-
% Events/
yr
Days
RR = 0.79 Noninferiority p < 0.00l
Rivaroxaban 20 mg QD Warfarin
Patel MR, et al N Engl J Med 2011;365(10):883-91
120 240 360 480 600 720 840 960
2.2%/yr
1.7%/yr
39
ARISTOTLE Apixaban vs Warfarin
• Study: High Risk AF pts (n=18,201) with ≥1 § Stroke or TIA § CHF: EF < 40% or ≥ NYHA II § Age ≥ 75 § DM § HTN
• Rx (x 1.8 yrs median): § Apixaban 5 mg b.i.d. § Warfarin (to INR 2.0-3.0)
Granger CB, et al N Engl J Med 2011;365(11):981-992 40
Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 21
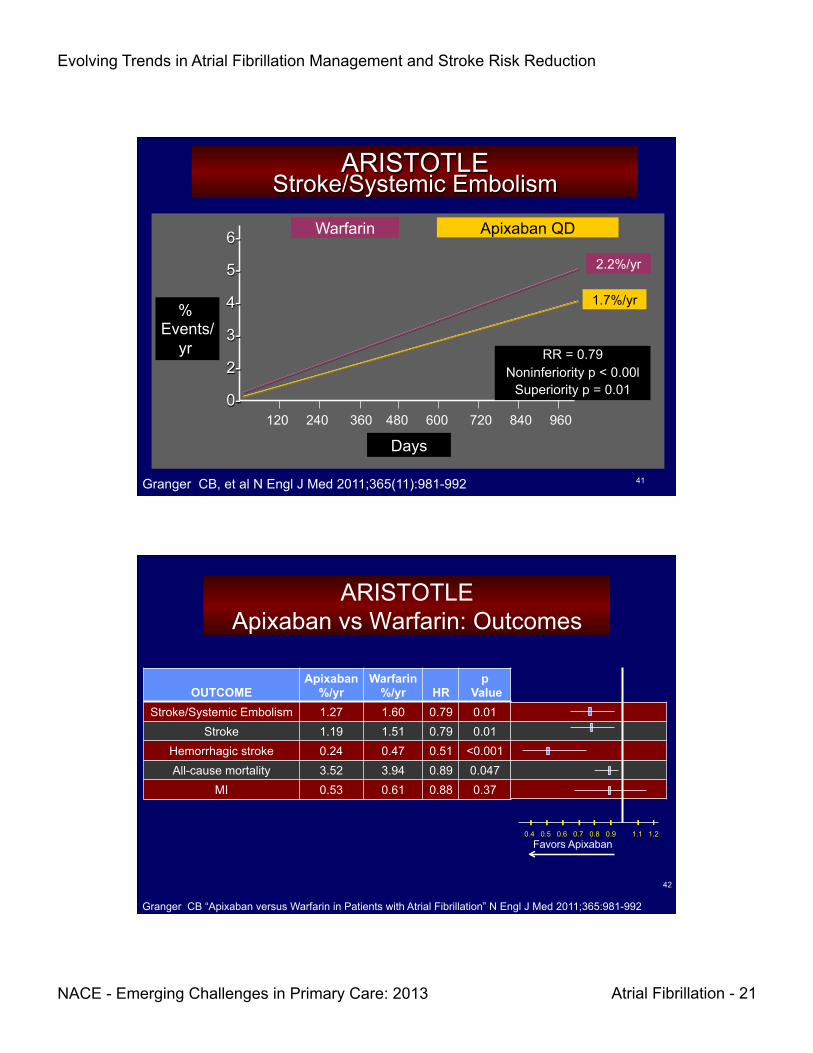
ARISTOTLE Stroke/Systemic Embolism
6-
5-
4-
3-
2-
0-
% Events/
yr
Days
RR = 0.79 Noninferiority p < 0.00l
Superiority p = 0.01
Apixaban QD Warfarin
120 240 360 480 600 720 840 960
2.2%/yr
1.7%/yr
Granger CB, et al N Engl J Med 2011;365(11):981-992 41
ARISTOTLE Apixaban vs Warfarin: Outcomes
OUTCOME
Apixaban %/yr
Warfarin %/yr
HR
p Value
Stroke/Systemic Embolism 1.27 1.60 0.79 0.01 Stroke 1.19 1.51 0.79 0.01
Hemorrhagic stroke 0.24 0.47 0.51 <0.001 All-cause mortality 3.52 3.94 0.89 0.047
MI 0.53 0.61 0.88 0.37
0.4 0.5 0.6 0.7 0.8 0.9
- - - - -
1.1 1.2
Granger CB “Apixaban versus Warfarin in Patients with Atrial Fibrillation” N Engl J Med 2011;365:981-992
Favors Apixaban
42

Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 22
Apixaban vs Warfarin: Safety Outcomes
OUTCOME
Apixaban %/yr
Warfarin %/yr
HR
p Value
Major Bleeding 2.13 3.09 0.69 <0.001 Intracranial Bleed 0.33 0.80 0.42 <0.001
Non-Intrancranial Bleed 1.79 2.27 0.79 0.004 GI Bleed 0.76 0.86 0.89 0.37
0.4 0.5 0.6 0.7 0.8 0.9
- - - - -
1.1 1.2 Favors Apixaban
-
0.3
Granger CB “Apixaban versus Warfarin in Patients with Atrial Fibrillation” N Engl J Med 2011;365:981-992
43
AF Warfarin Comparison Trials RE-LY ROCKET-AF ARISTOTLE
n 18,113 14,264 18,201 Age (mean) 72 73 70 Prior CVA 20% 55% 19%
CHADS (mean) 2.1 3.5 2.1 TTR (mean) 64% 55% 62%
CVA %/yr
1.11 vs 1.71 p < 0.001
2.12 vs 2.42 p = 0.12
1.27 vs 1.60 p <0.001
Bleed (major) %/yr
3.32 vs 3.57 p = 0.31
3.45 vs 3.6 p = 0.58
2.13 vs 3.09 p <0.001
Bleed (ICH) %/yr
0.3 vs 0.74 p < 0.001
0.49 vs 0.74 p = 0.019
0.24 vs 0.47 p < 0.001
Mortality NS NS 3.52 vs 3.94 p 0.047
44 Adapted from Table2 and 3 Katsnelson M et al. Stroke 2012;43: 1179—1185.

Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 23
ARS Question
1. 80 year old with persistent atrial fibrillation 2. 68 year old symptomatic patient after 2 trials of
antiarrhythmic Rx with paroxysmal atrial fibrillation 3. Obese asymptomatic patient with sleep apnea and
paroxysmal atrial fibrillation 4. 64 year old with EF of 35% and LA size of 5.5 cms 5. 74 year old hypertensive with atrial fibrillation for
the past 2 years and symptomatic palpitations
Which Patient is Best Suited for Radiofrequency Catheter Ablation?
45
Treatment Goals and Strategies
Rhythm Control Antithrombotic Rx
Nonpharmacologic
Class IA Class IC Class III β-blocker
Catheter ablation Pacing Surgery
Implantable devices
Pharmacologic • Warfarin • Aspirin
• Thrombin Inhibitor • Factor Xa inhibitor
Nonpharmacologic • Removal/isolation
LA appendage
Rate control
Pharmacologic • Ca2+ blockers
• β-blockers • Digitalis
• Amiodarone
Nonpharmacologic • Ablate and pace
Pharmacologic
46

Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 24
47
Antiarrhythmic Drug Efficacy for Chronic AF:
MUCH less than Perfect Sinus Rhythm Rate Retention
(%) Mean (range)
No. Studies
No drug 31 (15 - 56) 12 Quinidine 41 (11 - 54) 11 Disopyramide 49 (44 - 54) 3 Propafenone 39 (30 - 46) 3 Flecainide 62 (49 - 81) 3 Sotalol 42 (37 - 49) 3 Amiodarone 53 (36 - 83) 4
Studies followed patients for at least 6 months after cardioversion
Crijns HJGM, Gosselink ATM. Cardio 1994;7:31.
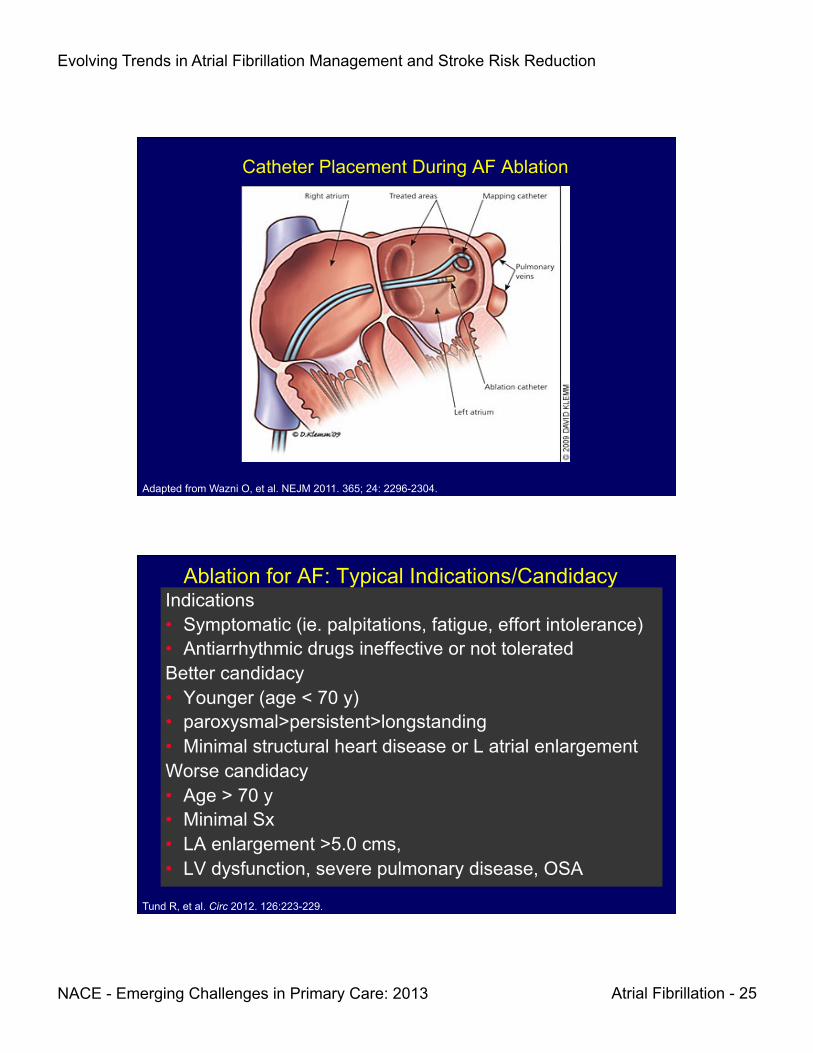
Pulmonary Vein Isolation
• The most common triggers of AF are ectopic atrial beats that arise from the muscle sleeves of the pulmonary vein (PV), clustered in the vicinity of the pulmonary vein-left atrial junction.
Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 25
Adapted from Wazni O, et al. NEJM 2011. 365; 24: 2296-2304.
Catheter Placement During AF Ablation
Ablation for AF: Typical Indications/Candidacy Indications • Symptomatic (ie. palpitations, fatigue, effort intolerance) • Antiarrhythmic drugs ineffective or not tolerated Better candidacy • Younger (age < 70 y) • paroxysmal>persistent>longstanding • Minimal structural heart disease or L atrial enlargement Worse candidacy • Age > 70 y • Minimal Sx • LA enlargement >5.0 cms, • LV dysfunction, severe pulmonary disease, OSA
Tund R, et al. Circ 2012. 126:223-229.
Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 26
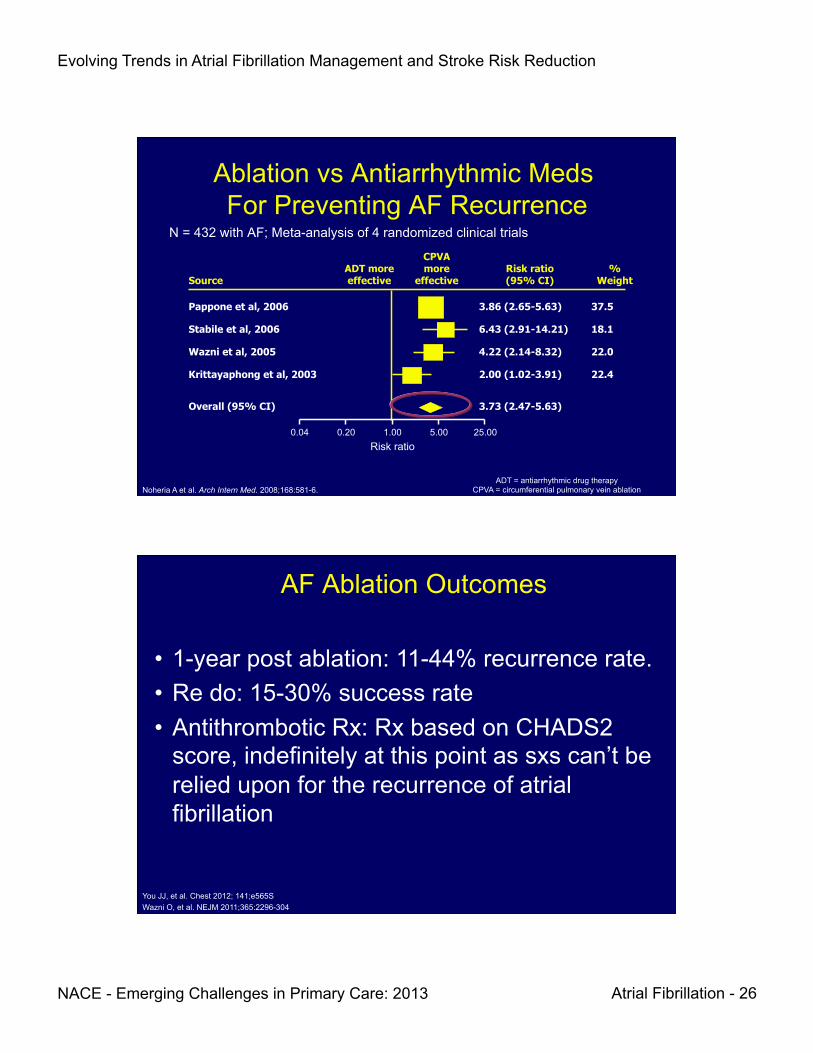
Source ADT more effective
CPVA more
effective Risk ratio (95% CI)
% Weight
Pappone et al, 2006
Stabile et al, 2006
Wazni et al, 2005
Krittayaphong et al, 2003
Overall (95% CI)
3.86 (2.65-5.63)
6.43 (2.91-14.21)
4.22 (2.14-8.32)
2.00 (1.02-3.91)
3.73 (2.47-5.63)
37.5
18.1
22.0
22.4
Ablation vs Antiarrhythmic Meds For Preventing AF Recurrence
N = 432 with AF; Meta-analysis of 4 randomized clinical trials
0.04 0.20 1.00 5.00 25.00 Risk ratio
ADT = antiarrhythmic drug therapy CPVA = circumferential pulmonary vein ablation Noheria A et al. Arch Intern Med. 2008;168:581-6.
AF Ablation Outcomes
• 1-year post ablation: 11-44% recurrence rate. • Re do: 15-30% success rate • Antithrombotic Rx: Rx based on CHADS2
score, indefinitely at this point as sxs can’t be relied upon for the recurrence of atrial fibrillation
You JJ, et al. Chest 2012; 141;e565S Wazni O, et al. NEJM 2011;365:2296-304

Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 27
Asymptomatic Episodes More Common After Catheter Ablation for Atrial Fibrillation (DISCERN)*
• Implantable Cardiac Monitor (ICM) placed 3 months before and for a mean of 18 months after RF ablation for AF in 50 pts
• The ratio of asymptomatic to symptomatic AF episodes increased from 1.1 to 3.7 (p=0.002)
• Post-ablation state is the strongest predictor of asymptomatic AF with 12% of patients having asx recurrences only
• The presence of sxs can not be used to predict recurrence of AF
(DISCERN) Discerning Symptomatic and Aymptomatic Episodes Pre and Post Radiofrequency Ablation of Atrial Fibrillation Verma A et al. Jama Internal Medicine 2013;173 (2):149-156.
• Ablation should generally be considered only after the failure of at least 1 AA drug.
• The success of AF ablation depends on patient selection. AF responds best to ablation in its early stages. Paroxysmal AF responds better than persistent AF which responds better than permanent AF.
• Recurrent AF post ablation occurs in up to 30% to 40% of patients. In nearly all redo procedures, the problem was the unrecognized gaps in conduction between the pulmonary vein and left atrium making the first ablation ineffective.
Summary of AF Ablation
Wazni O, et al. NEJM 2011;365:2296-304
Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 28
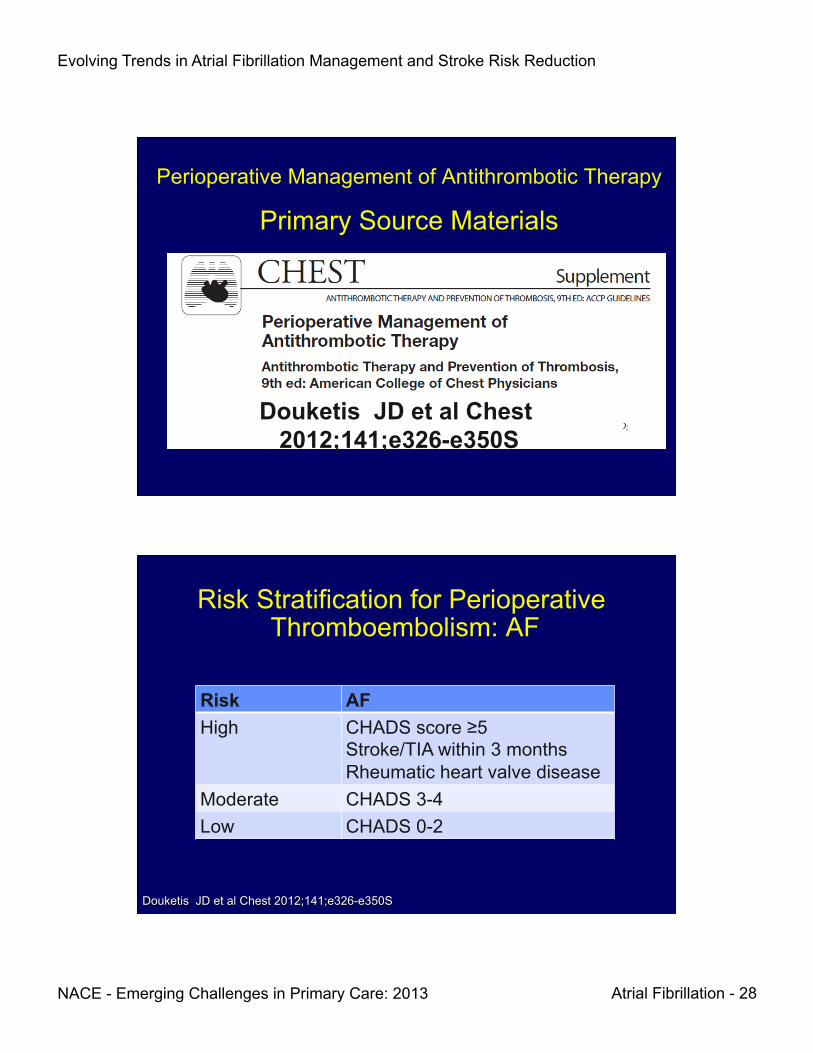
Perioperative Management of Antithrombotic Therapy
Primary Source Materials
Douketis JD et al Chest 2012;141;e326-e350S
Risk Stratification for Perioperative Thromboembolism: AF
Risk AF High CHADS score ≥5
Stroke/TIA within 3 months Rheumatic heart valve disease
Moderate CHADS 3-4 Low CHADS 0-2
Douketis JD et al Chest 2012;141;e326-e350S

Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 29
Primary Recommendations When Warfarin Must Be Withheld for Surgery
• Stop VKA 5 days preop (not less) • Resume VKA 12-24 hr postop (not later)
assuming adequate hemostasis • AF, Mechanical Heart Valve, VTE
♦ LOW risk: no bridging ♦ HIGH risk: bridging ♦ INTERMEDIATE: individualize
Douketis JD et al Chest 2012;141;e326-e350S
Where Did the Warfarin ‘5 days before surgery’ thing come from?
• Study: prospective cohort study of warfarin DC 5 d pre-op (n=224)
• Measured: INR 1 day pre-op • Outcome (% INR >1.5) = 7% • Prior trial DC 2-3 d pre-op à mean INR = 1.8
Douketis JD et al Chest 2012;141;e326-e350S

Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 30
Primary Recommendations Minor Surgery & VKA
Douketis JD et al Chest 2012;141;e326-e350S
Procedure VKA Additional Minor dental Continue Pro-hemostatic agent
OR Minor dental D-C 2-3 days pre-op None Minor dermatologic
Continue Optimize local hemostasis
Cataract Continue None
Peri-operative Risk From Dental Surgery in Perspective
“In reviewing the available literature, there are no well-documented cases of serious bleeding
problems from dental surgery in patients receiving therapeutic levels of continuous
warfarin… but there were several documented cases of serious embolic complications in
patients whose warfarin therapy was withdrawn for dental treatment.”
Wahl MJ “Dental Surgery in Anticoagulated Patients” Arch Intern Med 1998;158:1610-1616
Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 31
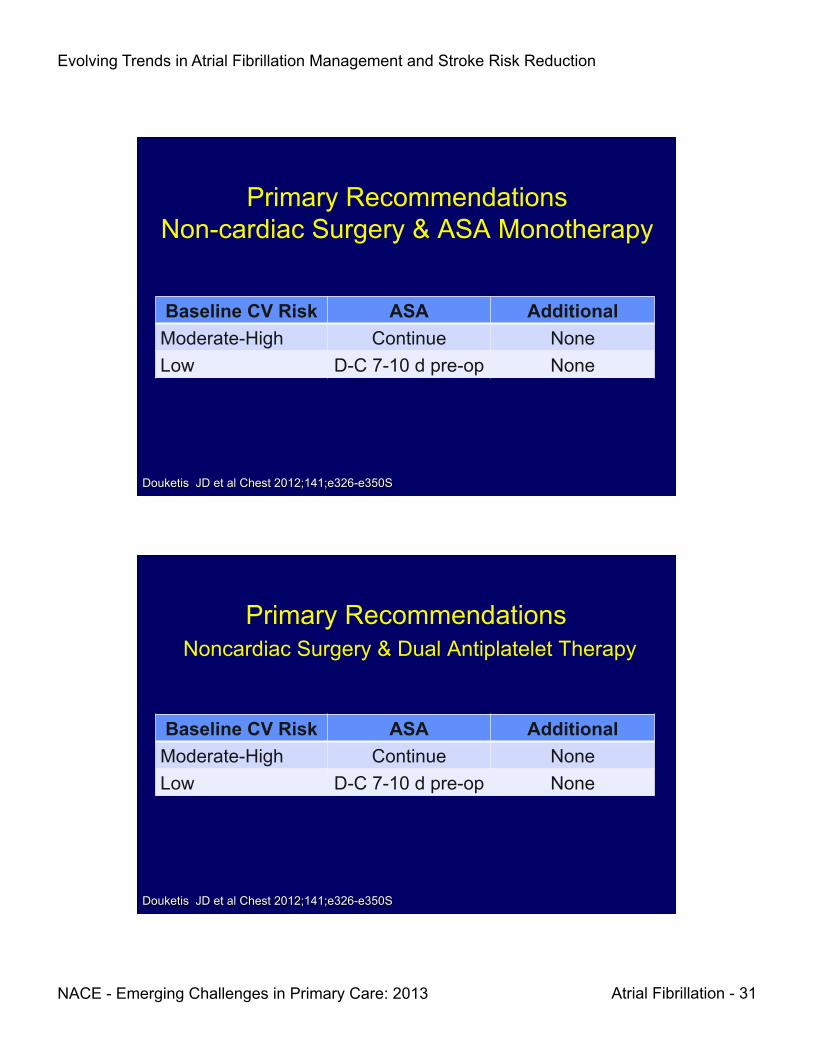
Primary Recommendations Non-cardiac Surgery & ASA Monotherapy
Douketis JD et al Chest 2012;141;e326-e350S
Baseline CV Risk ASA Additional Moderate-High Continue None Low D-C 7-10 d pre-op None
Primary Recommendations Noncardiac Surgery & Dual Antiplatelet Therapy
Baseline CV Risk ASA Additional Moderate-High Continue None Low D-C 7-10 d pre-op None
Douketis JD et al Chest 2012;141;e326-e350S

Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 32
What About The New Kids On the Block Peri-operatively?
Apixaban (Eliquis) Dabigatran (Pradaxa) Rivaroxaban (Xarelto)
Surgery: Dabigatran (Pradaxa)
• GFR ≥50 mL/min: DC 1-2 days pre-op • GFR < 50 mL/min: DC 3-5 days pre-op • Consider longer for
♦ major surgery ♦ spinal puncture ♦ spinal or epidural catheter/port ♦ Need for complete hemostasis
Dabigatran Prescribing Information
Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 33
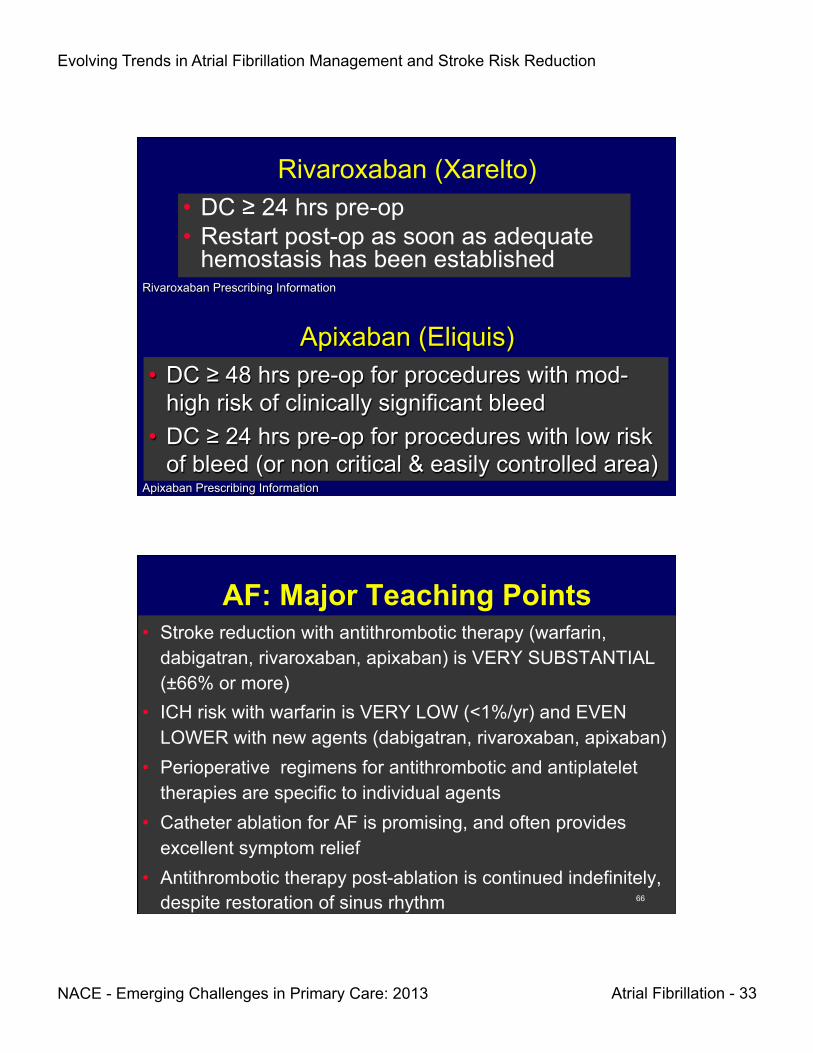
Rivaroxaban (Xarelto) • DC ≥ 24 hrs pre-op • Restart post-op as soon as adequate
hemostasis has been established Rivaroxaban Prescribing Information
• DC ≥ 48 hrs pre-op for procedures with mod-high risk of clinically significant bleed
• DC ≥ 24 hrs pre-op for procedures with low risk of bleed (or non critical & easily controlled area)
Apixaban Prescribing Information
Apixaban (Eliquis)
AF: Major Teaching Points • Stroke reduction with antithrombotic therapy (warfarin,
dabigatran, rivaroxaban, apixaban) is VERY SUBSTANTIAL (±66% or more)
• ICH risk with warfarin is VERY LOW (<1%/yr) and EVEN LOWER with new agents (dabigatran, rivaroxaban, apixaban)
• Perioperative regimens for antithrombotic and antiplatelet therapies are specific to individual agents
• Catheter ablation for AF is promising, and often provides excellent symptom relief
• Antithrombotic therapy post-ablation is continued indefinitely, despite restoration of sinus rhythm 66

Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 34
ARS #1 Clinical Scenario: Steve E.
Steve E, a 79 y/o hispanic male with a history of HTN and a left hemispheric stroke 2 years ago, was asymptomatic until 2 days ago when he developed intermittent palpitations and presented to your office. EKG: AF at 120 bpm. Steve’s CHADS2 score is:
1) 1 2) 2 3) 4 4) 6 5) Not sure 67
ARS #2
1) All of the newer agents are statistically superior to warfarin for stroke risk reduction 2) The major reason to provide warfarin is because overall costs with warfarin are much less than other agents 3) In the absence of head-to-head trials, it is not possible to know if any one of the newer agents is superior to another 4) Major bleeding risk with newer agents is markedly less than with warfarin
A 62 year dermatologist has recently been diagnosed with AF. He has hypertension and type 2 diabetes, both of which are well controlled. Being a physician, he asks "I've read about all the treatments; which is the best treatment for my AF?" You should answer
68
Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 35
ARS # 3 Perioperative Management of Tomas, a 62 Y.O. with
AF, HTN, DM • Tomas is undergoing CV surgery. His INR has been in
the therapeutic range about 75% of the time on warfarin 5 mg/d. What should be done about his warfarin dose perioperatively? 1) Continue 5 mg/d without interruption 2) Discontinue warfarin 3 days preop, resume 12-24
hrs after adequate hemostasis 3) Discontinue 5 days preop, resume 12-24 hrs after
adequate hemostasis 4) Switch to clopidogrel 75 mg/d 3 days preop, then
resume warfarin 12-24 hrs after adequate hemostasis and discontinue clopidogrel
69
1. 80 year old with persistent atrial fibrillation 2. 68 year old symptomatic patient after 2 trials of
antiarrhythmic Rx with paroxysmal atrial fibrillation 3. Obese asymptomatic patient with sleep apnea and
paroxysmal atrial fibrillation 4. 64 year old with EF of 35% and LA size of 5.5 cms 5. 74 year old hypertensive with atrial fibrillation for the past
2 years and symptomatic palpitations
ARS #4 Which Patient is Best Suited for RF Ablation?
70
Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 36
Allison has new onset AF resistant to several steps of pharmacotherapy. She has well controlled HTN and T2DM. She has a high level of awareness of her rapid heart rate, which impairs her QOL. She has heard of catheter ablation. If she undergoes successful ablation and is in sinus rhythm, what should be done about anticoagulation? 1) Anticoagulation can be omitted once she is in sinus rhythm 2) Anticoagulation should be used for 4-6 weeks post ablation 3) Anticoagulation should be used indefinitely despite sinus
rhythm 4) Anticoagulation should be used for 2-3 months post
ablation
ARS # 5 Clinical Scenario: Allison M
A 58 y.o. Woman with Resistant Symptomatic AF
71
On a scale of 1 to 5, please rate how confident you would be in treating a patient with atrial
fibrillation.
1. Not at all confident 2. Slightly confident 3. Moderately confident 4. Pretty much confident 5. Very confident
72
Evolving Trends in Atrial Fibrillation Management and Stroke Risk Reduction
NACE - Emerging Challenges in Primary Care: 2013 Atrial Fibrillation - 37
Which of the statements below describes your approach to anticoagulation of patients
with atrial fibrillation?
1. I do not manage atrial fibrillation, nor do I plan to this year. 2. I did not manage patients with atrial fibrillation before this course,
but as a result of attending this course I’m thinking of managing it now.
3. I do manage patients with atrial fibrillation and this course helped me change my treatment methods.
4. I do manage patients with atrial fibrillation and this course confirmed that I don’t need to change my treatment methods.
73