evidence-informed clinical practice …...evidence-informed clinical practice recommendations for...
TRANSCRIPT
Evidence-Informed ClinicalPractice Recommendations forTreatment of Type 1 DiabetesComplicated by ProblematicHypoglycemiaDiabetes Care 2015;38:1016–1029 | DOI: 10.2337/dc15-0090
Problematic hypoglycemia, defined as two or more episodes per year of severehypoglycemia or as one episode associated with impaired awareness of hypoglyce-mia, extremeglycemic lability, ormajor fear andmaladaptivebehavior, is a challenge,especially for patients with long-standing type 1 diabetes. Individualized therapy forsuch patients should include a composite target: optimal glucose control withoutproblematic hypoglycemia. Therefore, we propose a tiered, four-stage algorithmbased on evidence of efficacy given the limitations of educational, technological, andtransplant interventions. All patientswith problematic hypoglycemia should undergostructured or hypoglycemia-specific education programs (stage 1). Glycemic andhypoglycemia treatment targets should be individualized and reassessed every 3–6months. If targets are not met, one diabetes technologydcontinuous subcutaneousinsulin infusion or continuous glucose monitoringdshould be added (stage 2). Forpatients with continued problematic hypoglycemia despite education (stage 1) andone diabetes technology (stage 2), sensor-augmented insulin pumps preferably withan automated low-glucose suspend feature and/or very frequent contact with aspecialized hypoglycemia service can reduce hypoglycemia (stage 3). For patientswhose problematic hypoglycemia persists, islet or pancreas transplant should beconsidered (stage 4). This algorithm provides an evidence-informed approach to re-solving problematic hypoglycemia; it should be used as a guide, with individualpatient circumstances directing suitability and acceptability to ensure the prudentuse of technology and scarce transplant resources. Standardized reporting of hypo-glycemia outcomes and inclusion of patients with problematic hypoglycemia in stud-ies of new interventions may help to guide future therapeutic strategies.
TYPE 1 DIABETES AND PROBLEMATIC HYPOGLYCEMIA: BALANCING THEEFFECTIVENESS AND SAFETY OF INTERVENTIONS
Hypoglycemia is a common and greatly feared complication of type 1 diabetes (T1D)(1–4). Severe hypoglycemia (SH), an event that because of profound neuroglycope-nia requires the assistance of another person for recovery (5), is experienced by one-third of patients with T1D at least once a year (6–9). Many such events are singleepisodes caused by insulin dosing errors, exercise, and alcohol (Table 1). Conversely,problematic hypoglycemia is a condition in which episodes of SH are unpredictable,cannot be easily explained or prevented, and, therefore, have a significant negative
1Diabetes Research Group, King’s College Lon-don, London, U.K.2Department ofMedicine, Division of Endocrinol-ogy, Diabetes, and Metabolism, University ofPennsylvania Perelman School of Medicine, Phil-adelphia, PA3Department ofMedicine, Division of Endocrinol-ogy, University of Alberta, Edmonton, Canada4Endocrinology and Metabolism Department,INSERM U1190, European Genomics Institutefor Diabetes, Lille University Hospital, Lille Cedex,France5Diabetes Research Institute, Scientific InstituteOspedale San Raffaele, Milan, Italy6Immunology and Diabetes Unit, St. Vincent’sInstitute, University of Melbourne, Melbourne,Australia7Diabetes Clinic and Research Center, Vrije Uni-versiteit Brussel, Brussels, Belgium8Department of Diabetes and Clinical Nutrition,Kyoto University, Kyoto, Japan9Diabetes Center, Institute for Clinical and Exper-imental Medicine, Prague, Czech Republic10Department of Endocrinology and Diabetol-ogy, University of Zurich, Zurich, Switzerland11Schulze Diabetes Institute and Department ofSurgery, University of Minnesota, Minneapolis,MN
Corresponding author: Bernhard J. Hering,[email protected].
Received 14 January 2015 and accepted 9March2015.
P.C., M.R.R., P.A.S., and M.-C.V. contributedequally as primary authors.
R.L. and B.J.H. contributed equally as seniorauthors.
© 2015 by the American Diabetes Association.Readers may use this article as long as the workis properly cited, the use is educational and notfor profit, and the work is not altered.
See accompanying articles, pp. 968,971, 979, 989, 997, 1008, 1030, and1036.
Pratik Choudhary,1 Michael R. Rickels,2
Peter A. Senior,3
Marie-Christine Vantyghem,4
Paola Maffi,5 Thomas W. Kay,6
Bart Keymeulen,7 Nobuya Inagaki,8
Frantisek Saudek,9 Roger Lehmann,10
and Bernhard J. Hering11
1016 Diabetes Care Volume 38, June 2015
TYPE1DIABETES
ATACROSSROADS
impact on health and quality of life (QoL).The criteria of problematic hypoglycemiainclude two ormore episodes of SH in the
past 12 months or one episode of SH inthe past 12 months associated with im-paired awareness of hypoglycemia (IAH),
extreme glycemic lability, or major fearand maladaptive behavior. Simple toolsare available clinically to quantitate IAH
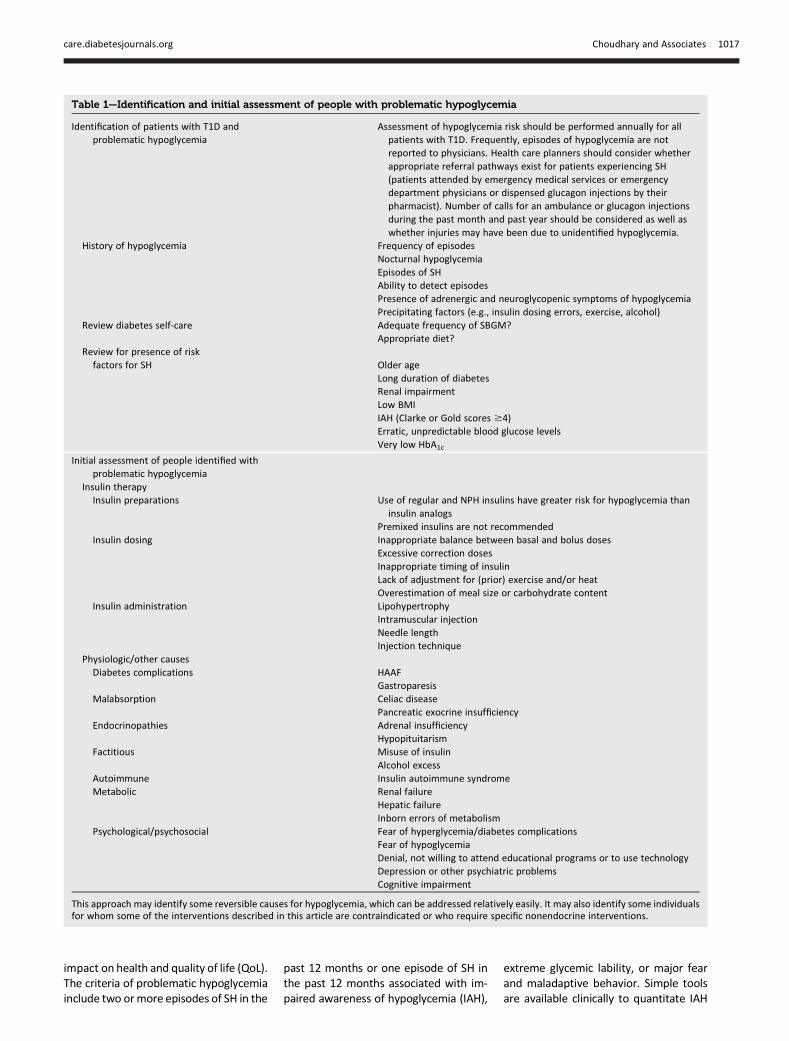
Table 1—Identification and initial assessment of people with problematic hypoglycemia
Identification of patients with T1D andproblematic hypoglycemia
Assessment of hypoglycemia risk should be performed annually for allpatients with T1D. Frequently, episodes of hypoglycemia are notreported to physicians. Health care planners should consider whetherappropriate referral pathways exist for patients experiencing SH(patients attended by emergency medical services or emergencydepartment physicians or dispensed glucagon injections by theirpharmacist). Number of calls for an ambulance or glucagon injectionsduring the past month and past year should be considered as well aswhether injuries may have been due to unidentified hypoglycemia.
History of hypoglycemia Frequency of episodesNocturnal hypoglycemiaEpisodes of SHAbility to detect episodesPresence of adrenergic and neuroglycopenic symptoms of hypoglycemiaPrecipitating factors (e.g., insulin dosing errors, exercise, alcohol)
Review diabetes self-care Adequate frequency of SBGM?Appropriate diet?
Review for presence of riskfactors for SH Older age
Long duration of diabetesRenal impairmentLow BMIIAH (Clarke or Gold scores $4)Erratic, unpredictable blood glucose levelsVery low HbA1c
Initial assessment of people identified withproblematic hypoglycemia
Insulin therapyInsulin preparations Use of regular and NPH insulins have greater risk for hypoglycemia than
insulin analogsPremixed insulins are not recommended
Insulin dosing Inappropriate balance between basal and bolus dosesExcessive correction dosesInappropriate timing of insulinLack of adjustment for (prior) exercise and/or heatOverestimation of meal size or carbohydrate content
Insulin administration LipohypertrophyIntramuscular injectionNeedle lengthInjection technique
Physiologic/other causesDiabetes complications HAAF
GastroparesisMalabsorption Celiac disease
Pancreatic exocrine insufficiencyEndocrinopathies Adrenal insufficiency
HypopituitarismFactitious Misuse of insulin
Alcohol excessAutoimmune Insulin autoimmune syndromeMetabolic Renal failure
Hepatic failureInborn errors of metabolism
Psychological/psychosocial Fear of hyperglycemia/diabetes complicationsFear of hypoglycemiaDenial, not willing to attend educational programs or to use technologyDepression or other psychiatric problemsCognitive impairment
This approach may identify some reversible causes for hypoglycemia, which can be addressed relatively easily. It may also identify some individualsfor whom some of the interventions described in this article are contraindicated or who require specific nonendocrine interventions.
care.diabetesjournals.org Choudhary and Associates 1017

(10,11), hypoglycemia severity (12), andglycemic lability (12).Recurrent hypoglycemia impairs
counterregulatory hormonal responsesto and awareness of hypoglycemia, pre-disposing patients to more frequenthypoglycemia and SH (13). IAH, whichincreases in prevalence with diabetesduration, is found in 20–40% of patientswith T1D (11,14–16) and increases therisk of SH by 6–20-fold (6,10,11). Recur-rent SH (two or more episodes annually)is reported by 21% of patients with T1D(6) and by 66% of patients whose T1D iscomplicated by IAH (11). Recurrent hy-poglycemia can cause significant mor-bidity (4,17) and mortality. Amongindividuals with T1D, 4–10% of alldeaths are attributed to SH (18,19),and risk of death 5 years after an epi-sode of SH is increased 3.4-fold in thosewho report SH (20).The risk factors for SH depend mainly
on residual C-peptide secretion, which re-duces glycemic variability (21–23). Re-lated to residual C-peptide secretion arethe patient’s age at onset of T1D and dis-ease duration (21). Other risk factorsinclude autonomic failure, insulin sensi-tivity, BMI, genetics, andpsychosocial fac-tors (24) (Table 1). In the Diabetes Controland Complications Trial, residual endoge-nous insulin secretion was associatedwith a reduced risk of SH, regardless oftreatment intensity (25). Unfortunately,most patients with T1D lose all measur-able C-peptide within 10–15 years afterdiagnosis (26),making itmore challengingfor those with long-standing (.15 years)T1D to avoid hypoglycemia.Besides a reduction of microangio-
pathic complications, long-term follow-upof the Diabetes Control and Complica-tions Trial cohort demonstrated a re-duction in cardiovascular morbidity (27)and all-cause mortality (28) in patientswith an HbA1c ,7.0% (53 mmol/mol),which concurs with Swedish and Aus-trian registries (29,30). However, evenat that HbA1c level, the residual risk forcardiovascular and all-cause mortalityremained twice as high in patients withT1D than in nondiabetic control subjects(29–31). A large U.S. registry of.20,000patients demonstrated a U-shaped rela-tionship between SH and HbA1c level,with the lowest risk of SH occurringwhen the HbA1c level is between 7.0%(53 mmol/mol) and 7.5% (58 mmol/mol)(9). Therefore, the selection of glycemic
targets in each patient should be individ-ualized to the lowest HbA1c level thatdoes not cause SH, that preserves hypo-glycemia awareness, and that avoidslong-term micro- and macrovascularcomplications (32).
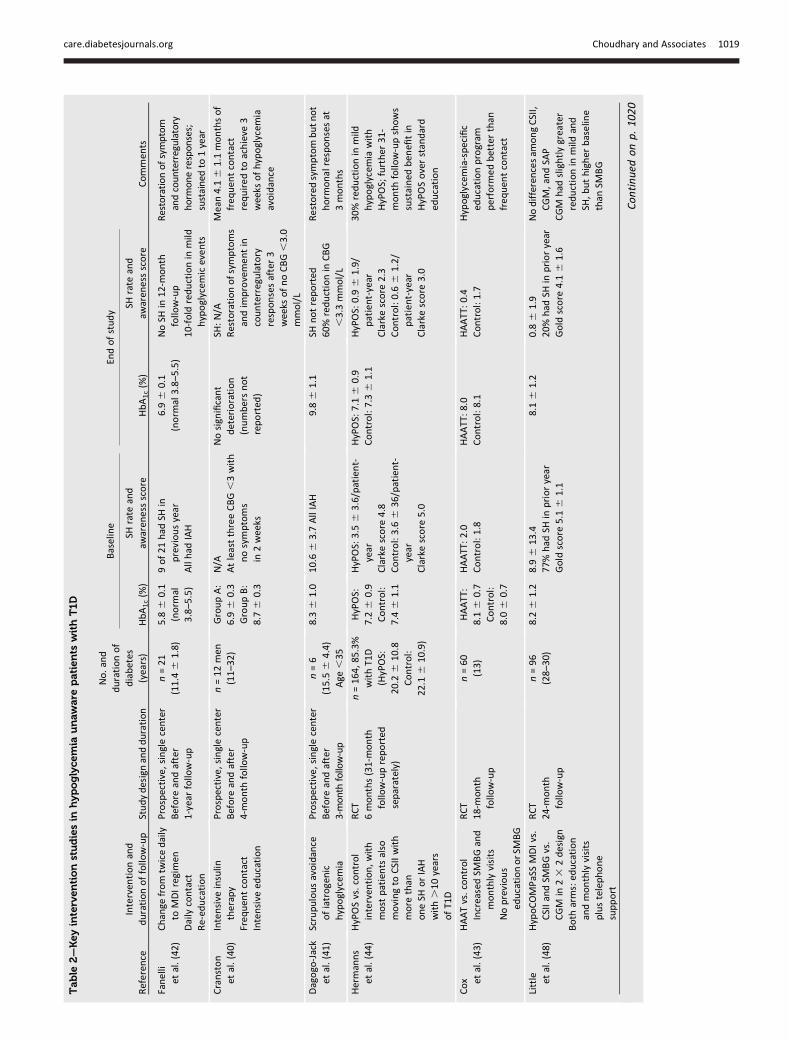
The objectives of this review articleare to examine the evidence on educa-tional, technological, and transplantinterventions in patients with T1Dcomplicated by problematic hypoglyce-mia (Table 2) and to propose clinicalpractice recommendations (Table 3)in a tiered, four-stage treatment algo-rithm (Fig. 1). To achieve these ob-jectives, an international group ofendocrinology clinician-investigatorswith expertise in evaluating all threetreatment categories in this patientpopulation was formed to critically ap-praise the available evidence and toformulate a consensus approach.
EDUCATIONAL INTERVENTIONS
Muhlhauser et al. (33) demonstratedthat intensified insulin therapy, whencombined with a 5-day teaching pro-gram, improved glycemic control with-out increasing SH. A similar programwascalled Dose Adjustment For Normal Eat-ing (DAFNE) (16). Such educational in-terventions typically consist of a 30- to40-h group-learning curriculum basedon adult learning principles around car-bohydrate counting, frequent self-monitoring of blood glucose (SMBG), andadjustment of insulin doses in responseto exercise, alcohol, and illness. To dif-ferentiate it from fixed-dose multipledaily injections (MDIs), active adjust-ment of insulin doses is often termed“functional insulin therapy.”
Large-scale audits of educational in-terventions in various countries foundreliable and sustained (up to 6 years)reductions in the incidence of SH by50–70% as well as an improvement inthe mean HbA1c level to ;7.6% (60mmol/mol) in unselected patients withT1D (16,34). A subanalysis of 341 pa-tients with three or more episodes ofSH in the prior year demonstrated re-ductions in both the incidence of SH(from 6.1 to 1.4 per patient annually)and the mean length of hospitalization(from 8.6 to 3.9 days per patient annu-ally) as well as improvements in themean HbA1c level (34,35). The DAFNEprogram showed similar reductions inthe incidence of SH, with restoration of
hypoglycemia recognition in 43% of pa-tients reporting IAH at baseline.
Blood glucose awareness training(BGAT) is a psychoeducational programdeveloped by Cox et al. (36) to increaseself-awareness of personal cues for de-tecting hypoglycemia. Originally devel-oped as 8 weekly sessions, BGAT hasundergone numerous iterations andhas been successfully piloted as an onlineprogram. It has consistently resulted inimproved detection of hypoglycemia, es-pecially in patients with IAH and sus-tained reductions in SH and even inthose with a high incidence of SH at base-line (37,38).
Few studies have examined educa-tional interventions specifically in pa-tients with IAH (Table 2). In the early1990s, three small studies demonstratedimprovement in symptom responses,with some (but variable) improvementin epinephrine responses after meticu-lous avoidance of hypoglycemia (39–42).Those improvements were achieved byextensive re-education, physiologic distri-bution of insulin with MDIs, and, mostimportantly, intensive contact and sup-port (up to four telephone calls per day)from the study team.
Three large randomized clinical trials(RCTs) specifically recruited patientswith problematic hypoglycemia. Coxet al. (43) randomized Bulgarian patientswith very little access to SMBG and atleast three episodes of SH annually toSMBG with and without hypoglycemiaanticipation, awareness, and treatmenttraining (HAATT) and found that the in-cidence of SH decreased with HAATT butnot with increased SMBG alone.
Hermanns et al. (44) randomized 164patients with more than one episode ofSH or with IAH despite MDI and continu-ous subcutaneous insulin infusion (CSII)to either a hypoglycemia-specific educa-tion program (HyPOS) or a standard edu-cation program. They demonstratedgreater improvement in awareness withHyPOS with a trend to a lower incidenceof SH 1 year after completing HyPOS thatbecame statistically significant at 31months of follow-up.
Decision making is central to hypogly-cemia avoidance, andqualitative researchhas identified fear of hypoglycemia andlack of concern regarding hypoglycemiaas important factors beyond skills andeducation that predispose to IAH (45,46).These findings may explain the success
1018 Type 1 Diabetes Complicated by Hypoglycemia Diabetes Care Volume 38, June 2015
Table
2—Keyinterven
tionstudiesin
hypoglyce
mia
unaw
are
patients
withT1D
Baseline
Endofstudy
Referen
ceInterven
tionand
durationoffollow-up
Studydesignandduration
No.and
durationof
diabetes
(years)
HbA1c(%
)SH
rate
and
awaren
essscore
HbA1c(%
)SH
rate
and
awaren
essscore
Commen
ts
Fanelli
etal.(42)
Chan
gefrom
twicedaily
toMDIregimen
Dailycontact
Re-ed
ucation
Prospective,singlecenter
Before
andafter
1-year
follow-up
n=21
(11.46
1.8)
5.86
0.1
(norm
al3.8–5.5)
9of21
had
SHin
previousyear
Allhad
IAH
6.96
0.1
(norm
al3.8–5.5)
NoSH
in12
-month
follow-up
10-fold
reductionin
mild
hypoglycem
iceven
ts
Restoration
ofsymptom
andcoun
terregulatory
horm
onerespon
ses;
sustainedto
1year
Cranston
etal.(40)
Intensive
insulin
therapy
Freq
uen
tcontact
Intensive
education
Prospective,singlecenter
Before
andafter
4-month
follow-up
n=12
men
(11–
32)
GroupA:
6.96
0.3
GroupB:
8.76
0.3
N/A
AtleastthreeCBG,3with
nosymptoms
in2weeks
Nosign
ificant
deterioration
(numbersnot
reported
)
SH:N/A
Restorationofsymptoms
andim
provemen
tin
counterregulatory
responsesafter3
weeks
ofnoCBG,3.0
mmol/L
Mean4.16
1.1monthsof
freq
uen
tcontact
required
toachieve
3weeks
ofhypoglycem
iaavoidance
Dagogo-Jack
etal.(41)
Scrupulousavoidance
ofiatrogenic
hypoglycem
ia
Prospective,singlecenter
Before
andafter
3-month
follow-up
n=6
(15.56
4.4)
Age
,35
8.36
1.0
10.6
63.7AllIAH
9.86
1.1
SHnotreported
60%reductionin
CBG
,3.3mmol/L
Restoredsymptombutnot
horm
onalresponsesat
3months
Hermanns
etal.(44)
HyPOSvs.control
interven
tion,w
ith
mostpatientsalso
movingto
CSIIwith
more
than
oneSH
orIAH
with.10
years
ofT1D
RCT
6months(31-month
follow-upreported
separately)
n=16
4,85.3%
withT1D
(HyPOS:
20.2
610
.8Control:
22.1
610
.9)
HyPOS:
7.26
0.9
Control:
7.46
1.1
HyPOS:3.56
3.6/patient-
year
Clarkescore
4.8
Control:3.66
36/patient-
year
Clarkescore
5.0
HyPOS:7.16
0.9
Control:7.36
1.1
HyPOS:0.96
1.9/
patient-year
Clarkescore
2.3
Control:0.66
1.2/
patient-year
Clarkescore
3.0
30%reductionin
mild
hypoglycem
iawith
HyPOS;further
31-
month
follow-upshows
sustained
ben
efitin
HyPOSoverstan
dard
education
Cox et
al.(43)
HAATvs.control
IncreasedSM
BGand
monthlyvisits
Noprevious
educationorSM
BG
RCT
18-m
onth
follow-up
n=60
(13)
HAATT:
8.16
0.7
Control:
8.06
0.7
HAATT:2.0
Control:1.8
HAATT:8.0
Control:8.1
HAATT:0.4
Control:1.7
Hypoglycem
ia-specific
educationprogram
perform
edbetterthan
freq
uen
tcontact
Little etal.(48)
HypoCOMPaSSMDIvs.
CSIIandSM
BGvs.
CGM
in23
2design
Both
arms:ed
ucation
andmonthlyvisits
plustelephone
support
RCT
24-m
onth
follow-up
n=96
(28–
30)
8.26
1.2
8.96
13.4
77%had
SHin
prioryear
Gold
score
5.16
1.1
8.16
1.2
0.86
1.9
20%had
SHin
prioryear
Gold
score
4.16
1.6
Nodifferencesam
ongCSII,
CGM,andSA
PCGM
had
slightlygreater
reductionin
mild
and
SH,b
uthigher
baseline
than
SMBG
Con
tinuedon
p.10
20
care.diabetesjournals.org Choudhary and Associates 1019
Table
2—Continued
Baseline
Endofstudy
Referen
ceInterven
tionand
durationoffollow-up
Studydesignandduration
No.and
durationof
diabetes
(years)
HbA1c(%
)SH
rate
and
awaren
essscore
HbA1c(%
)SH
rate
and
awaren
essscore
Commen
ts
Pedersen-
Bjergaard
etal.(56)
HypoAnastudy
[Analoginsulin
(detem
irandaspart)vs.
human
insulin
(NPH
andregu
lar)]
Multicen
ter,open
-lab
el,
crossoverRCT(1:1)
2-year
follow-up
n=15
98.06
1.0
Allhad
2ormore
episodes
ofSH
inprioryear
Decreaseof0
.13%
with
analogtreatm
ent
compared
with
human
insulin
(P=0.02
)
Insulin
analogs:10
5ep
isodes
ofSH
Human
insulin:13
6ep
isodes
ofSH
Absolute
rate
reductionof
0.51
episodes
ofSH
per
patient-yearwithinsulin
analogs
Lyet
al.(65)
CSIIvs.SA
Pin
young
patientswithIAH
RCT
6-month
follow-up
n=95
(11.0)
7.46
0.2
SAP-LGS:6SH
and
0.22
/patient-year
Clarkescore
5.96
1.5
CSII:6SH
and0.25/
patient-year
Clarkescore
6.46
1.5
7.46
0.2in
both
arms
SAP-LG
S:0even
ts=0/
patient-year
Clarkescore
4.7(4.0–5.1)
CSII:6even
ts=0.26/
patient-year
Clarkescore
5.1(5.5–6.4)
Youngpatients
with
shortdurationSA
P-LG
SreducedSH
compared
withCSIIalone,
although
even
trates
werelow
Reduced
time,70
and
,60
mg/dL
inLG
Sarm
deZoysa
etal.(47)
DAFN
E-HART
6sessionsbased
on
cogn
itivebeh
avioral
therap
yand
motivational
interviewing
1-year
follow-up
Smalltrial;2sites
Uncontrolledpilot
clinicaltrial
n=24
(316
12)
Previous
DAFN
E8
CSII
7.86
1.1
Med
ian3.0(0–10
3)Clarkescore
5.46
1.2
Ryanscore
948
7.86
1.2
Med
ian0(0–3)
70%reported
no
further
SHClarkescore
3.86
1.8
Ryanscore
372
9of20restoredaw
aren
ess
SomeacceptedCSIIor
CGM,whichthey
were
resistan
tto
previously
Choudhary
etal.(66)
Observationalclinical
auditofCGM
inpatientswithSH
despiteprevious
DAFN
EandCSII
1-year
follow-up
Retrospective
audit
n=35
(29.66
13.6)
8.16
1.2
SH8.16
13.6/patient-year
Gold
score
5.16
1.5
7.66
1.0
0.66
1.2/patient-year
Gold
score
5.26
1.9
54%reported
subjective
improvemen
tin
awaren
ess
Red
uctionin
SHwithCGM
23of35
usedSA
P-LG
S3withSH
onSA
Phad
no
further
episodes
on
SAP-LG
S
Gim
enez
etal.(58)
CSIIanded
ucation
program
with2–3-
month
follow-up
Small,uncontrolled
pilottrial
2-year
follow-up
n=20
(16.2)
6.76
1.1
1.256
0.4/patient-year
Clarkescore
5.56
1.2
6.36
0.9
SH0.05/patient-year
at2years
Clarkescore
1.66
2.03
16of19
restored
awaren
ess
Red
ucedmild
hypoglycem
iaTime,70
mg/dL
reducedfrom
13.7to9.1%
Samann
etal.(35)
Structureded
ucation
5-day
course(DTTP)
9,58
3patients
at96
centers
1-year
follow-up
Subgroupanalysisof
patientswith3or
more
SHat
baseline
n=34
1(18.76
11.1)
7.46
1.9
6.16
9.6/patient-year
7.26
1.5
1.46
5.4/patient-year
56%had
1,20
%had
2,andonly15
%had
more
than
3SH
even
tsRed
ucedtimein
hospital
8.66
15.4to
3.96
10.7
days/patient-year
Con
tinu
edon
p.10
21
1020 Type 1 Diabetes Complicated by Hypoglycemia Diabetes Care Volume 38, June 2015
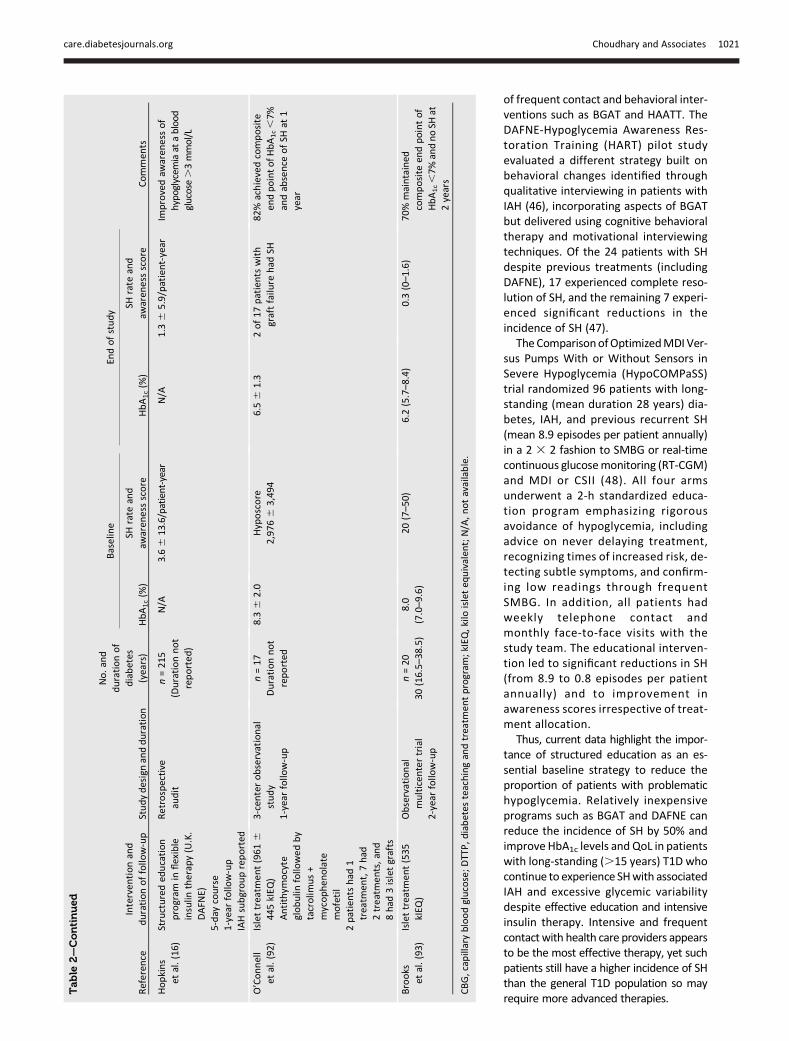
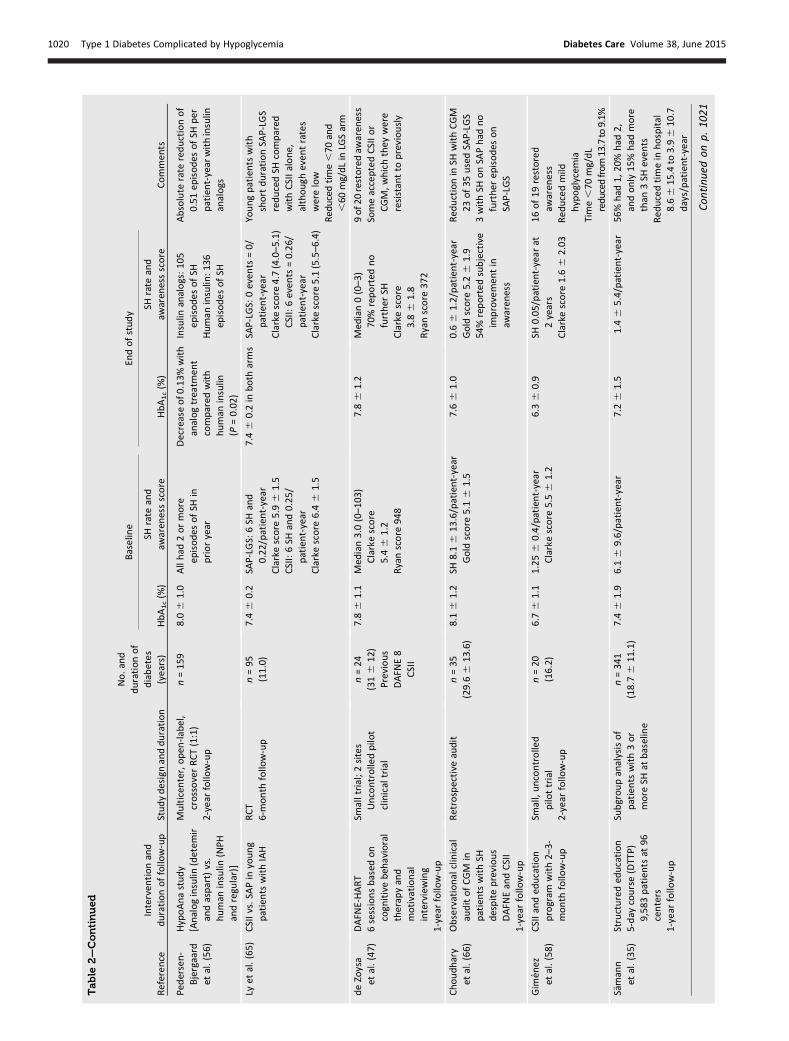
of frequent contact and behavioral inter-ventions such as BGAT and HAATT. TheDAFNE-Hypoglycemia Awareness Res-toration Training (HART) pilot studyevaluated a different strategy built onbehavioral changes identified throughqualitative interviewing in patients withIAH (46), incorporating aspects of BGATbut delivered using cognitive behavioraltherapy and motivational interviewingtechniques. Of the 24 patients with SHdespite previous treatments (includingDAFNE), 17 experienced complete reso-lution of SH, and the remaining 7 experi-enced significant reductions in theincidence of SH (47).
The ComparisonofOptimizedMDI Ver-sus Pumps With or Without Sensors inSevere Hypoglycemia (HypoCOMPaSS)trial randomized 96 patients with long-standing (mean duration 28 years) dia-betes, IAH, and previous recurrent SH(mean 8.9 episodes per patient annually)in a 2 3 2 fashion to SMBG or real-timecontinuous glucosemonitoring (RT-CGM)and MDI or CSII (48). All four armsunderwent a 2-h standardized educa-tion program emphasizing rigorousavoidance of hypoglycemia, includingadvice on never delaying treatment,recognizing times of increased risk, de-tecting subtle symptoms, and confirm-ing low readings through frequentSMBG. In addition, all patients hadweekly telephone contact andmonthly face-to-face visits with thestudy team. The educational interven-tion led to significant reductions in SH(from 8.9 to 0.8 episodes per patientannually) and to improvement inawareness scores irrespective of treat-ment allocation.
Thus, current data highlight the impor-tance of structured education as an es-sential baseline strategy to reduce theproportion of patients with problematichypoglycemia. Relatively inexpensiveprograms such as BGAT and DAFNE canreduce the incidence of SH by 50% andimprove HbA1c levels and QoL in patientswith long-standing (.15 years) T1D whocontinue to experience SHwith associatedIAH and excessive glycemic variabilitydespite effective education and intensiveinsulin therapy. Intensive and frequentcontact with health care providers appearsto be the most effective therapy, yet suchpatients still have a higher incidence of SHthan the general T1D population so mayrequire more advanced therapies.
Table
2—Continued
Baseline
Endofstudy
Referen
ceInterven
tionand
durationoffollow-up
Studydesignandduration
No.and
durationof
diabetes
(years)
HbA1c(%
)SH
rate
and
awaren
essscore
HbA1c(%
)SH
rate
and
awaren
essscore
Commen
ts
Hopkins
etal.(16)
Structureded
ucation
program
inflexible
insulin
therapy(U.K.
DAFN
E)5-day
course
1-year
follow-up
IAHsubgroupreported
Retrospective
audit
n=21
5(Durationnot
reported
)
N/A
3.66
13.6/patient-year
N/A
1.36
5.9/patient-year
Improvedaw
aren
essof
hypoglycem
iaat
ablood
glucose.3mmol/L
O’Connell
etal.(92)
Islettreatm
ent(961
644
5kIEQ
)Antithym
ocyte
globulin
followed
by
tacrolim
us+
mycophen
olate
mofetil
2patients
had
1treatm
ent,7had
2treatm
ents,and
8had
3isletgrafts
3-centerobservational
study
1-year
follow-up
n=17
Durationnot
reported
8.36
2.0
Hyposcore
2,97
66
3,49
46.56
1.3
2of17
patients
with
graftfailure
had
SH82
%achievedcomposite
endpointofHbA1c,7%
andabsence
ofSH
at1
year
Brooks
etal.(93)
Islettreatm
ent(535
kIEQ
)Observational
multicen
tertrial
2-year
follow-up
n=20
30(16.5–38
.5)
8.0
(7.0–9.6)
20(7–50
)6.2(5.7–8.4)
0.3(0–1.6)
70%maintained
composite
endpointof
HbA1c,7%
andnoSH
at2years
CBG,cap
illarybloodglucose;DTTP,d
iabetes
teachingandtreatm
entprogram
;kIEQ
,kilo
isleteq
uivalen
t;N/A,notavailable.
care.diabetesjournals.org Choudhary and Associates 1021

TECHNOLOGICAL INTERVENTIONS
Before implementing diabetes technolo-gies in treatment, insulin therapies shouldbe optimized, with preference given to in-sulin analogs. Most studies of insulin ana-logs have excluded high-risk patients withprior SH or IAH (49) and used a noninfe-riority design and strict, treat-to-targetdosing algorithms (50) so are likely tohave underestimated benefits for patientswith problematic hypoglycemia. Rapid-acting insulin analogs (aspart, glulisine, lis-pro)with faster onset and shorter durationthan regular insulin are associated with a20% reduction in the incidence of SH and a45% reduction in the incidence of noctur-nal hypoglycemia (51). Basal analogs,which have less intraindividual variabilityin bioavailability than neutral protamineHagedorn (NPH) insulin (52), are also ef-fective, providing a 27% reduction in theincidence of SH and a 31% reduction inthe incidence of nocturnal hypoglycemiacompared with NPH insulin (53,54). Newerbasal insulin analogs (e.g., degludec andU300 glargine) may be even less variableand further reduce hypoglycemia risk.Studies of degludec found a 25% reductionin the incidence of symptomatic nocturnalhypoglycemia but no difference in the in-cidence of SH (55). In the single trial con-ducted in patients with problematichypoglycemia, insulin analogs reducedthe incidence of SH by 29% comparedwith regular and NPH insulin (56).The effectiveness of CSII in patients
with problematic hypoglycemia has notbeen tested in robust RCTs, but a meta-analysis found a fourfold reduction in theincidence of SH and a 0.6% improvementin HbA1c levelwith CSII (57). Older age andmore frequent episodes of SH were inde-pendentpredictors of a reduced incidenceof SH with CSII. A small pilot study of CSIIin 19 patients with IAH demonstratedrestoration of awareness in 16 at 1 year(58).Although a cornerstone of therapy in
T1D, SMBG may only be effective in re-ducing the incidence of SH when com-bined with education (e.g., HAATT) (43).Although blinded CGM may be useful asa diagnostic tool to identify periods ofhypoglycemia, a systematic review ofblinded CGM versus SMBG did not dem-onstrate improved HbA1c levels and wasunable to analyze hypoglycemia rates(because of heterogeneity in definitionsand assessment of hypoglycemia) (59).
In contrast, a meta-analysis showed thatRT-CGM, which can alert patients to im-pending hypoglycemia, decreased HbA1clevels without increasing hypoglycemicepisodes (60). Because patientswith priorSH or IAH were excluded from this study,the proportion with major hypoglycemicepisodes was numerically lower with RT-CGM but was not significantly differentfrom the proportion with SMBG.
In the context of intensive educationand frequent contact, no differences in re-ducing the incidence of SH or in restoringawareness were found between MDI ver-sus CSII and SBGM versus RT-CGMS in theHypoCOMPaSS trial. CGM tended to showgreater reductions in the incidence of SHpossibly because of a higher incidence ofSH at baseline (48). A substudy of theHypoCOMPaSS trial found improvementsin symptom and catecholamine responsesto experimental hypoglycemia, withtrends to greater improvements withCSII and to a lesser degree with CGM (61).
Clinical trials of sensor-augmentedpumps (SAPs), which are CSII deviceswith an integrated CGM system, havefound superior glycemic control but nodifference in the incidence of SH com-pared with MDI (and SMBG) (62). Manypatients were noted to sleep throughnocturnal alarms (63). One RCT of a de-vice with an automated threshold-suspend feature (where insulin deliveryis automatically suspended for up to 2 hif the sensor glucose falls below a pre-specified threshold) demonstrated a38% reduction in the duration of noctur-nal hypoglycemia (64) compared withSAP. Another RCT in children and adoles-cents with IAH showed a reduction in theincidence of SH with SAP compared withCSII alone but no improvement in theepinephrine response to experimentalhypoglycemia (65). A small observa-tional study demonstrated significantreductions in the incidence of SH (from8.1 to 0.6 episodes per patient annually)using SAP in patients with IAH but noimprovement in awareness (66).
Clinical trials of fully automated inte-grated CGM/CSII technologies (artificialpancreas) have been reported (67,68).Somehaveuseddual pumps to administerboth insulin and glucagon, although glu-cagon was not required to protect fromnocturnal hypoglycemia in a head-to-head study (69). Although potentially ofgreat benefit, these technologies havenot yet been evaluated in patients with
problematic hypoglycemia and are notyet commercially available.
TRANSPLANT INTERVENTIONS
Pancreas and, now, islet transplants caneffectively prevent hypoglycemia and re-store normoglycemia and may stabilizethe complications of T1D (70–75). Patientswith T1D who undergo an islet or a pan-creas transplant exhibit recovery of physi-ologic islet cell hormonal responses toinsulin-induced hypoglycemia wherebyendogenous insulin secretion is sup-pressed and glucagon secretion restored(76,77), although in islet transplant recipi-ents, the glucagon response remains par-tial likely due to lower islet mass beingtransplanted as evidenced from b-cell se-cretory capacity testing (78,79). Both isletand pancreas transplant recipients alsohave improved epinephrine and normal-ized autonomic symptom responses tohypoglycemia, providing evidence ofamelioration of hypoglycemia-associatedautonomic failure (HAAF) (76,77). Theseimproved counterregulatory defensemechanisms may be sustained for morethan a decade of pancreas graft function(80). Most importantly, islet and pancreastransplantation have been shown to nor-malize the endogenous (predominantlyhepatic) glucose production response toinsulin-induced hypoglycemia (77,81),thereby affording recipients protectionand recovery from low blood glucose.
Pancreata procured from leaner andyounger donors often are preferredfor whole-organ pancreas transplants,whereas islets can be isolated from obeseand older donors (82) unsuitable forwhole-organ transplants, thereby increas-ing the proportion of donated organs thatcan contribute to the treatment of T1D.Thus, islet and pancreas transplants areevolving as complementary approachesto b-cell replacement for the eliminationof problematic hypoglycemia in T1D.
Most pancreas transplants are per-formed simultaneously with a kidneytransplant. Simultaneous pancreas-kidney (SPK) transplants confer superiorlong-term graft function compared withpancreas transplant alone or pancreastransplant after a kidney transplant. The5-year pancreas graft survival rate for re-cipients of pancreas transplant alone andpancreas transplant after a kidney trans-plant is between 55 and 70%; for SPKrecipients, it is .85% (83). With SPKtransplants, most recipients can expect
1022 Type 1 Diabetes Complicated by Hypoglycemia Diabetes Care Volume 38, June 2015

amelioration of problematic hypoglyce-mia for more than a decade (83–85).Pancreas transplants are usually under-
taken in patientswho are relatively young(,50 years) and nonobese (,30 kg/m2)and who do not have coronary artery dis-ease. These patient selection criteria min-imize operative mortality (,1%) andreduce early technical pancreas graftloss (;10%) (86,87). Removal of techni-cally failed grafts and routine complica-tions of abdominal surgery have led to areoperation rate as high as 40% (85).Islet transplantation, a minimally inva-
sive procedure, allows for inclusion ofolder patients and patients with coronaryartery disease who would be ineligiblefor a whole-pancreas transplant. In non-obese recipients, the target islet dose of$5,000 islet equivalents/kg can be iso-lated from a deceased donor pancreas(71).Most islet transplants are performedin nonuremic patients with T1D and prob-lematic hypoglycemia and related exces-sive glycemic lability (12,71,88). Carefulselection of patients and protocol optimi-zation have led to substantial clinical im-provements (71). Importantly, refinedrecipient treatment has improved long-term outcomes of islet transplants; insu-lin independence can now be maintainedfor 5 years in 50% of recipients (89,90).Although restoring insulin indepen-
dence remains an important objective,several multicenter clinical trials of islettransplants in patients with T1D and prob-lematic hypoglycemia, including the phase3 licensure trial of human islets conductedby the Clinical Islet Transplantation Con-sortium, have adopted a combination ofnear-normal glycemic control (HbA1c,7.0% [53 mmol/mol]) together with theelimination of SH as the primary end pointand the clinically relevant dual goal of in-tervention (91–93). After having reportedsuccessful achievement of that goal in 82%of patients at 1 year (92) and in 70% at 2years posttransplant (93), islet transplantsare now approved and reimbursed in sev-eral countries for the treatment of prob-lematic hypoglycemia in T1D. In the U.S.,although a phase 3 trial of islet transplantsin this patient population has beencompleted, a formal license applicationawaits submission, review, and approval.Even with partial islet graft function,
the endogenous glucose production re-sponse to insulin-induced hypoglycemiaimproves (94), so islet grafts protectagainst problematic hypoglycemia even
when insulinmay be required tomaintainnear-normoglycemia. This protectionfrom hypoglycemia has been confirmedin CGM studies showing a near absenceof time at glucose ,70 mg/dL/,3.9mmol/L (77). The reductions in mean glu-cose, glucose variability, and time spenthypoglycemic (,54mg/dL/,3.0mmol/L)relative to T1D were similar for bothinsulin-independent and insulin-requiringislet recipients (95), and those reductionswere sustained for 18 months in onestudy (96). Importantly, Vantyghemet al. (23) showed that minimal islet graftfunction is sufficient to abrogate hypogly-cemia (,54 mg/dL/,3.0 mmol/L), con-firming that even suboptimal function(requiring insulin) significantly improvesmean glucose and glucose variability.That the islet graft imparts these glycemiccontrol benefits has been further sup-ported by the demonstration of sig-nificant continuous associations withstimulated C-peptide levels in islet trans-plant recipients (97). This avoidance ofhypoglycemia with islet or pancreastransplants as documented by CGM bestexplains the documented reversal of HAAFas well as the recovery of glucose counter-regulation and hypoglycemia symptomrecognition, thereby reversing the vicioushypoglycemia-begets-hypoglycemia cyclein T1D (98). Data from the CollaborativeIslet Transplant Registry indicate thatproblematic hypoglycemia amelioratedfor the duration of islet graft function is
currently retained in 90% of recipients at4 years posttransplant (71).
In addition to procedural risks andlimited organ availability, the currentneed for lifelong immunosuppressivetherapy represents a major limitationto widespread implementation ofb-cell replacement therapies for pa-tients with problematic hypoglycemiarefractory to educational and techno-logical interventions. Because kidneytransplant recipients are already com-mitted to immunosuppressive therapy,the addition of an islet or pancreastransplant may be considered tonormalize glycemia, stabilize diabetescomplications, and prevent recurrentdiabetic nephropathy. In such T1D kidneytransplant recipients, islet transplan-tation can be considered simultaneously with or after a kidney trans-plant for patients who are not surgicalcandidates for or willing to accept therisks of a pancreas transplant (85). At 5years (99) and 13 years (85) post-transplant, the insulin independencerate was higher for pancreas than for isletrecipients; however, the islet recipientsexperienced significantly fewer opera-tive complications, and both the pan-creas and islet recipients experiencedsignificantly improved glycemic controland a reduction of .90% in the inci-dence of SH (85).
Thus, regardless of b-cell replace-ment approach (pancreas or islets), the
Figure 1—Proposed treatment algorithm for patients with T1D and problematic hypoglycemia.
care.diabetesjournals.org Choudhary and Associates 1023

majority of recipients can anticipateamelioration from problematic hypogly-cemia for at least 5 years together withnear-normal glycemic control. In fact,islet and pancreas transplants are theonly approaches to date that conferboth sustained recovery from HAAFand restoration of glucose counterregu-lation (by endogenous glucose produc-tion) and, thereby, reliable protectionfrom SH in patients with long-standing(.15 years) T1D.
TREATMENT ALGORITHM
The treatment algorithm has to takeinto account the number of patientswith T1D who have problematic or re-current SH, existing educational toolsand technologies to reduce hypoglyce-mia, and the available resources for var-ious treatment strategies, includingtransplants. Individual countries or re-imbursement plans might need to adaptthe algorithm in accordance with theirresources.Individualized treatment targetsmust
balance the risk of complications withthat of hypoglycemia in an effort toachieve the lowest attainable HbA1c
level without problematic hypoglycemia(32). Published studies have indicatedthat educational and technological in-terventions can prevent SH while main-taining HbA1c levels between 7.2 and8.0% (55 and 64 mmol/mol) (Table 2).Many patients rarely or never inform
their physician about episodes of hypo-glycemia (100); therefore, health carepractitioners must routinely inquireabout a given patient’s frequency ofand risk factors for hypoglycemia andglycemic lability (12) and must screenfor impaired awareness. Commonlyused validated scores are those byClarke et al. (10) and Gold et al. (11)where a score $4 indicates hypoglyce-mia unawareness, but increasingly,other measures are used, such as glu-cose SD (.40 mg/dL/.2.8 mmol/L)(23), low blood glucose index (101), oraverage daily risk range (102).
THE FOUR STAGES OF THEPROPOSED TIERED ALGORITHM
Stage 1All MDI therapy patients using SMBGshould have routine evaluation of hypo-glycemia awareness status using vali-dated scores along with assessment of
glycemic control. Patients with prob-lematic hypoglycemia should be regu-larly evaluated for possible underlyingcauses of hypoglycemia (Table 1), forthe presence of hypoglycemia unaware-ness, and for meeting their own individ-ual HbA1c level and other treatmenttargets (32). If the patient is not at tar-get, first-line therapy is a structurededucation or hypoglycemia-specific ed-ucation program (Fig. 1). A robustevidence base supports functional insu-lin therapy (33) through educationalprograms such as DAFNE (16) and be-havioral interventions such as BGAT(36). These programs reduce the inci-dence of SH by 50–70% and restorehypoglycemia awareness in up to 40%of patients (Table 2). Some data suggestadditional benefits with programs fo-cused on hypoglycemia avoidance,such as HyPOS, over standard educa-tion. The choice of insulin in patientswith SH has been tested in only onetrial, which demonstrated a 29% re-duction in SH using analogs comparedwith regular or NPH insulin (56). But nodata exist so far regarding the impacton IAH of newer insulins, such as de-gludec, U300 glargine, or pegylatedinsulin (103).
Stage 2Robust evidence exists for the use of CSIIas second-line therapy to reduce SH (57).Although a paucity of randomized evi-dence supports the use of RT-CGM andless evidence supports the use of RT-CGMin patients with T1D for the purpose ofreducing the incidenceof SH, this technol-ogy offers a logical step forward for indi-vidual patients. Limitations to the use oftechnology must be considered, and datasuggest that CGM must be used continu-ously for sustained benefit (104).
Stage 3If the composite treatment target of noSH, Clarke score ,4, and HbA1c ,8.0%(64 mmol/mol) is still not met (Fig. 1),the use of SAP, preferably with low-glucose suspension (LGS), and/or veryfrequent contact with a specialized hy-poglycemia service should be consid-ered for third-line therapy (Fig. 1).Small-scale nonrandomized trials ofpsychoeducational therapies such asDAFNE-HART and BGAT suggested thatthey offer further benefit, especially in
patients with behavioral contributors torecurrent SH (39–41).
Because most trials of SAP in T1D ex-cluded patients with problematic hypo-glycemia, only anecdotal evidencesupports the use of SAP alone for reduc-ing the incidence of SH in this patientpopulation. Studies using threshold sus-pension of insulin were successful in re-ducing hypoglycemia over and aboveSAP alone, suggesting that this may bethe preferred evidence-based option inpatients with T1D and problematic hy-poglycemia (64,65). In patients with on-going problematic hypoglycemia, veryfrequent and intensive contact with anexpert diabetes team can restore theirawareness of symptoms and, to someextent, counterregulatory responses,but such contact may not always be fea-sible in the clinical scenario. Weekly tomonthly contact as offered in theHypoCOMPaSS trial seem to be effectivein reducing the incidence of SH, but res-torationof awareness ismodest (Table 2).
The algorithmproposed in Fig. 1 showsthe level of evidence supporting each in-tervention. The system should be flexible,and clinicians will make individual deci-sions based on specific circumstances,taking into account the preference ofthe patient as well as the patient’s in-volvement and possibilities. For certainpatients with behavioral issues, furtherbehavioral programs such as BGAT,HyPOS, or DAFNE-HART may be benefi-cial. For others, more expensive treat-ment such as CSII with and withoutRT-CGM may be more appropriate.
Stage 4Pancreas and islet transplants, thefourth-line therapy, are very effectivein achieving the composite target ofeliminating SH with near-normal HbA1clevels, but lifelong immunosuppressivetherapy and its possible complicationsrepresent a major limiting factor. Be-cause islet and pancreas transplantsare both effective in preventing SHand achieving near-normoglycemia,the optimal treatment option will re-quire individualized discussion of multi-ple factors, including the proceduralrisks (which are higher for a pancreastransplant), importance of insulin inde-pendence, waiting time, and sensitiza-tion. Some contraindications to apancreas transplant (age .50 years,high cardiac risk) are common in
1024 Type 1 Diabetes Complicated by Hypoglycemia Diabetes Care Volume 38, June 2015

patients with problematic hypoglyce-mia; they may only be eligible for anislet transplant. Yet, a small proportionof patients may be ineligible for an islettransplant because of their weight orinsulin requirements. The transplantteam should consider each patient’spreferences and perceptions of risksand benefits.In the absence of contraindications,
the main determinant of which type oftransplant to choose is the patient’s kid-ney function. A living donor kidneytransplant might be the best optionfor a given patient with chronic kidneydisease followed by either an islet or apancreas transplant (105). If a living do-nor is not available, then a simultaneousdeceased donor kidney transplant andislet or pancreas transplant may be in-dicated (Fig. 2).For patients requiring a kidney trans-
plant, it is clear that both pancreasand islet transplants, either simulta-neously or sequentially, are effective inpreventing SH and protecting the kidneygraft from hyperglycemia (85). How-ever, how best to treat problematichypoglycemia in patients with an inter-mediate estimated glomerular filtrationrate (eGFR) (30–60 mL/min) (Fig. 2) isunclear because the immunosuppres-sive therapy required after a pancreasor islet transplant can increase the riskof end-stage renal failure in these pa-tients (106,107).
Currently, organ donation rates in theU.S. and Europe are stalled at between10 and 35 donors per million population(108,109), yet potentially 1,000 patientswith T1D per million population are af-fected by recurrent SH (6–9). The organshortage is the second major factor (inaddition to lifelong immunosuppression)limiting b-cell replacement. Until newsources of b-cells are available, b-cell re-placement bymeans of a whole-pancreastransplant or an isolated islet transplantwill be limited to a carefully selectedgroup of patients with problematic hypo-glycemia refractory to medical and tech-nological interventions.
Byrne et al. (110) demonstrated thatspecialized clinics with expertise in hy-poglycemia management are essentialto concentrating limited transplant re-sources for patients who need themmost. Of 36 patients with recurrentSH referred to a specialized hypoglyce-mia service, 47.2% experienced resolu-tion of their problematic hypoglycemiawith optimal medical therapy, andanother 25% achieved clinically rele-vant improvement. Of those highlyselected patients, however, 27.8%required a transplant despite havingelevated HbA1c levels of 8.0% (64mmol/mol) and despite having accessto all educational and technologicalinterventions.
Another crucial factor is the reimburse-ment policy of each country or insurance
plan. If an expensive technology optiondoes not deliver the expected resultswithin a 6-month period, it may bediscontinued. In many countries, CSII isreimbursed by health insurance, but RT-CGM is not. The same is true for b-cellreplacement; in many countries, pan-creas transplants are reimbursed, butonly in a much smaller number of coun-tries are islet transplants reimbursed. Thecost-effectiveness of these technologieshas not been tested in larger populations;it will take many years to prove the costsavings or at least the cost-effectiveness,although QoL improves in most trials.
CLINICAL RESEARCH NEEDS
As new insulin analogs and devices be-come available, we recommend includ-ing in future trials and studies patientswith recent SH or IAH and then sepa-rately reporting changes in HbA1c level,SH, and IAH in those with prior problem-atic hypoglycemia. Doing so would allowdata on the impact of new therapies inthis complex group of patients to be-come available sooner. Also crucial inevaluating new therapies are robuststudies of changes in symptoms, coun-terregulatory hormone responses, andendogenous glucose production re-sponses to experimental hypoglycemia.
Educational interventions have theevidence base to be recommended asfirst-line therapy. Further investigationinto appropriate baseline factors thatmay aid personalization of treatment isdesirable. In the home studies usingsingle- or dual-hormone closed-loopsystems now taking place, the role ofsuch systems in patients with problem-atic hypoglycemia remains to be tested.
The effectiveness of CSII with SMBGand CGM with MDI in preventing SH inpatients with IAH remains to becompared in larger trials. AlthoughHypoCOMPaSS suggests equivalence,the technology selection may dependon the availability of systems, reim-bursement policies, and patient choice.Also remaining to be studied is whichpatients with persistent problematichypoglycemia despite structured edu-cation should use SAP as the nextintervention.
In the field of transplantation, areasthat require further clinical researchinclude improvement of islet engraft-ment to prolong graft survival and
Figure 2—Transplant options for patients with T1D (expert consensus). CGMS, continuousglucose monitoring system. +eGFR .30 and ,60 mL/min/1.73 m2: islet or pancreas trans-plantation alone, high risk for developing end-stage renal disease under calcineurin-basedimmunosuppression. *All transplant types: living kidney and deceased donor islet or pancreasafter kidney transplantation, simultaneous pancreas or islet kidney transplantation, or de-ceased donor kidney alone and islet or pancreas after kidney transplantation.
care.diabetesjournals.org Choudhary and Associates 1025

minimization of immunosuppressionthrough antigen-specific immunotherapy,adoptive transfer of immunoregulatorycells, and use of biocompatible immune-isolating devices. Moving forward, pre-clinical work is already showing potentialfor expanding the role of transplantationthrough the use of alternate tissuesources, such as porcine islet xenograftsor human stem cell–derived insulin-secreting cells.
CONCLUSIONS
Problematic hypoglycemia is anothercomplication of long-term T1D, causingmorbidity and mortality in a significantproportion of patients. It is important toscreen patients for problematic hypogly-cemia using validated tools and to imple-ment individualized therapeutic targetsbased on the balance between glycemiccontrol and hypoglycemia risk. Problem-atic hypoglycemia can be resolved withappropriate educational and technologicalinterventions inmost patientswith accept-able glycemic control; however, in a subsetof patients, transplants offer the only so-lution. Especially for that subset, existinginterventions need to be more thoroughlyevaluated and new therapies developed.
Acknowledgments. The authors thankMary E.Knatterud, University of Minnesota, for experteditorial assistance.
Funding. P.C. is supported in part by DiabetesUK grants 14/0004865 and 13/0005643. M.R.R. issupported in part by U.S. Public Health Serviceresearch grants R01-DK-091331 and U01-DK-070430 from the National Institutes of Health.P.A.S. is supported by the Academic AlternateRelationship Plan and in part by Alberta InnovatesHealth Solutions and JDRF. M.-C.V. is supportedby the French Ministry of Health (PHRC 2001,2008, and 2009), European Community (FondEuropeen de Developpement Regional), ConseilRegional Nord Pas de Calais (IFR 114), EuropeanFP7, JDRF, Societe Francophone du Diabete, As-sociation de Recherche pour le Diabete, andAgence de Biomedecine. T.W.K. is supported bytheNationalHealth andMedical ResearchCouncil(APP1037321), JDRF, Diabetes Australia ResearchTrust, Operational Infrastructure Support schemeof the Victorian Government, and NationallyFunded Centres scheme. F.S. is supported inpart by Ministry of Health of the Czech Republicgrant NT14020-3/2013. B.J.H. is supported in partby U.S. Public Health Service research grants U01-AI-065193 and U01-AI-102463 from the NationalInstitutes of Health and by research grants 17-2012-527 and 17-2013-495 from JDRF.Duality of Interest. P.C. has participated onadvisory boards for Medtronic, Johnson andJohnson, and Roche regarding insulin pumpsand CGM and has participated in commercialresearch funded by Medtronic. P.A.S. has re-ceived research support from Novo Nordisk andEli Lilly and consulting fees from Eli Lilly, Med-tronic, and Novo Nordisk and is on the speakersbureau for Animas, Eli Lilly, Novo Nordisk, andSanofi. No other potential conflicts of interestrelevant to this article were reported.Author Contributions. P.C., M.R.R., P.A.S., andM.-C.V. researched data, conducted the system-atic review, identified studies for inclusion in thereview and rated their quality, and contributedto the writing, review, editing, and final approvalof themanuscript. P.M., T.W.K., B.K., N.I., and F.S.contributed to the design of the review and
writing, editing, and final approval of the manu-script. R.L. researched data, conducted the sys-tematic review, identified studies for inclusion inthe review and rated their quality, led thedevelopment of the comprehensive treatmentalgorithm, and contributed to the writing, review,editing, and final approval of the manuscript.B.J.H. developed the concept of a comprehen-sive treatment algorithm for patients with T1Dand problematic hypoglycemia in collaborationwith councilors of the International Pancreasand Islet Transplant Association, assembled thewriting team, researched data, conducted thesystematic review, identified studies for inclu-sion in the review and rated their quality, led thewriting of the manuscript, and contributed tothe review, editing, and final approval of themanuscript.
References1. Cryer PE. The barrier of hypoglycemia in di-abetes. Diabetes 2008;57:3169–31762. McCrimmon RJ, Sherwin RS. Hypoglycemiain type 1 diabetes. Diabetes 2010;59:2333–23393. Seaquist ER, Anderson J, Childs B, et al. Hy-poglycemia and diabetes: a report of a work-group of the American Diabetes Associationand the Endocrine Society. Diabetes Care2013;36:1384–13954. Frier BM. Hypoglycaemia in diabetes melli-tus: epidemiology and clinical implications. NatRev Endocrinol 2014;10:711–7225. Workgroup on Hypoglycemia, American Dia-betes Association. Defining and reporting hypo-glycemia in diabetes: a report from the AmericanDiabetes Association Workgroup on Hypoglyce-mia. Diabetes Care 2005;28:1245–12496. Pedersen-Bjergaard U, Pramming S, HellerSR, et al. Severe hypoglycaemia in 1076 adultpatients with type 1 diabetes: influence of riskmarkers and selection. Diabetes Metab Res Rev2004;20:479–4867. UK Hypoglycaemia Study Group. Risk of hy-poglycaemia in types 1 and 2 diabetes: effects oftreatment modalities and their duration. Diabe-tologia 2007;50:1140–11478. Gruden G, Barutta F, Chaturvedi N, et al. Se-vere hypoglycemia and cardiovascular diseaseincidence in type 1 diabetes: the EURODIAB Pro-spective Complications Study. Diabetes Care2012;35:1598–16049. Weinstock RS, Xing D, Maahs DM, et al.; T1DExchange Clinic Network. Severe hypoglycemiaand diabetic ketoacidosis in adults with type 1diabetes: results from the T1D Exchange clinicregistry. J Clin Endocrinol Metab 2013;98:3411–341910. Clarke WL, Cox DJ, Gonder-Frederick LA,Julian D, Schlundt D, Polonsky W. Reducedawareness of hypoglycemia in adults withIDDM. A prospective study of hypoglycemic fre-quency and associated symptoms. DiabetesCare 1995;18:517–52211. Gold AE, MacLeod KM, Frier BM. Frequencyof severe hypoglycemia in patients with type Idiabetes with impaired awareness of hypogly-cemia. Diabetes Care 1994;17:697–70312. Ryan EA, Shandro T, Green K, et al. Assess-ment of the severity of hypoglycemia and gly-cemic lability in type 1 diabetic subjects
Table 3—Proposed clinical practice recommendations for the treatment ofpatients with T1D complicated by problematic hypoglycemia
1 Routinely provide to allMDI therapy patientswith T1D usingSMBG structured and curriculum-based educationalprograms that reduce the incidence of SH and restoreawareness in a significant proportion of patientswith IAH.
2 Add one diabetes technology, preferably CSII with SMBG orMDI with CGM, where available, with appropriateeducation, training, and support to patients withproblematic hypoglycemia to reduce the incidence of SHand maintain or improve HbA1c.
3 Use SAPs, preferably with an automated threshold-suspendfeature, where available, or very frequent contact witha specialized hypoglycemia service in patients whoseproblematic hypoglycemia persists despite the use ofstructured education and other diabetes technologies.
4 Consult with transplant program (and payer) about theeligibility of selected patientswith persistent problematichypoglycemia for an islet or a pancreas transplant whenother interventions have not been effective andwhen therisk-benefit ratio is deemed favorable.
1026 Type 1 Diabetes Complicated by Hypoglycemia Diabetes Care Volume 38, June 2015

undergoing islet transplantation. Diabetes2004;53:955–96213. Cryer PE. Mechanisms of hypoglycemia-associated autonomic failure in diabetes. NEngl J Med 2013;369:362–37214. Geddes J, Schopman JE, Zammitt NN, FrierBM. Prevalence of impaired awareness of hypo-glycaemia in adults with type 1 diabetes. DiabetMed 2008;25:501–50415. Choudhary P, Geddes J, Freeman JV, EmeryCJ, Heller SR, Frier BM. Frequency of biochemicalhypoglycaemia in adultswith type1 diabeteswithand without impaired awareness of hypoglycae-mia: no identifiable differences using continuousglucose monitoring. Diabet Med 2010;27:666–67216. Hopkins D, Lawrence I, Mansell P, et al. Im-proved biomedical and psychological outcomes1 year after structured education in flexible in-sulin therapy for people with type 1 diabetes:the U.K. DAFNE experience. Diabetes Care 2012;35:1638–164217. Frier BM. Morbidity of hypoglycemia intype 1 diabetes. Diabetes Res Clin Pract 2004;65(Suppl. 1):S47–S5218. Skrivarhaug T, Bangstad HJ, Stene LC,Sandvik L, Hanssen KF, Joner G. Long-term mor-tality in a nationwide cohort of childhood-onsettype 1 diabetic patients in Norway. Diabetologia2006;49:298–30519. Feltbower RG, Bodansky HJ, Patterson CC,et al. Acute complications and drug misuse areimportant causes of death for children andyoung adults with type 1 diabetes: resultsfrom the Yorkshire Register of diabetes in chil-dren and young adults. Diabetes Care 2008;31:922–92620. McCoy RG, Van Houten HK, Ziegenfuss JY,Shah ND, Wermers RA, Smith SA. Increasedmortality of patients with diabetes reportingsevere hypoglycemia. Diabetes Care 2012;35:1897–190121. Sherr J, Tamborlane WV, Xing D, et al.; Di-abetes Research in Children Network (DirecNet)Study Group. Achievement of target A1C levelswith negligible hypoglycemia and low glucosevariability in youth with short-term type 1 di-abetes and residual b-cell function. DiabetesCare 2012;35:817–82022. Siegelaar SE, Holleman F, Hoekstra JB,DeVries JH. Glucose variability; does it matter?Endocr Rev 2010;31:171–18223. Vantyghem MC, Raverdy V, Balavoine AS,et al. Continuous glucose monitoring after islettransplantation in type 1 diabetes: an excellentgraft function (b-score greater than 7) Is re-quired to abrogate hyperglycemia, whereas aminimal function is necessary to suppress se-vere hypoglycemia (b-score greater than 3).J Clin Endocrinol Metab 2012;97:E2078–E208324. Stuckey HL, Mullan-Jensen CB, Reach G,et al. Personal accounts of the negative andadaptive psychosocial experiences of peoplewith diabetes in the second Diabetes Attitudes,Wishes and Needs (DAWN2) study. DiabetesCare 2014;37:2466–247425. The Diabetes Control and ComplicationsTrial Research Group. Hypoglycemia in the Di-abetes Control and Complications Trial. Diabe-tes 1997;46:271–286
26. Tsai EB, Sherry NA, Palmer JP, Herold KC. Therise and fall of insulin secretion in type 1 diabetesmellitus. Diabetologia 2006;49:261–27027. Nathan DM, Cleary PA, Backlund JY, et al.;Diabetes Control and Complications Trial/Epi-demiology of Diabetes Interventions and Com-plications (DCCT/EDIC) Study Research Group.Intensive diabetes treatment and cardiovascu-lar disease in patients with type 1 diabetes. NEngl J Med 2005;353:2643–265328. Orchard TJ, Nathan DM, Zinman B, et al.;Writing Group for the DCCT/EDIC ResearchGroup. Association between 7 years of intensivetreatment of type 1 diabetes and long-termmortality. JAMA 2015;313:45–5329. Stadler M, Peric S, Strohner-KaestenbauerH, et al. Mortality and incidence of renal re-placement therapy in people with type 1 diabe-tes mellitusda three decade long prospectiveobservational study in the Lainz T1DM cohort.J Clin Endocrinol Metab 2014;99:4523–453030. Lind M, Svensson AM, Kosiborod M, et al.Glycemic control and excess mortality in type 1diabetes. N Engl J Med 2014;371:1972–198231. Schoenaker DA, Simon D, Chaturvedi N,Fuller JH, Soedamah-Muthu SS; EURODIAB Pro-spective Complications Study Group. Glycemiccontrol and all-cause mortality risk in type 1 di-abetes patients: the EURODIAB prospectivecomplications study. J Clin Endocrinol Metab2014;99:800–80732. Cryer PE. Glycemic goals in diabetes: trade-off between glycemic control and iatrogenic hy-poglycemia. Diabetes 2014;63:2188–219533. Muhlhauser I, Bruckner I, Berger M, et al.Evaluation of an intensified insulin treatmentand teaching programme as routine manage-ment of type 1 (insulin-dependent) diabetes.The Bucharest-Dusseldorf Study. Diabetologia1987;30:681–69034. Samann A, Muhlhauser I, Bender R, KloosCh, Muller UA. Glycaemic control and severehypoglycaemia following training in flexible, in-tensive insulin therapy to enable dietary free-dom in peoplewith type 1 diabetes: a prospectiveimplementation study. Diabetologia 2005;48:1965–197035. Samann A, Muhlhauser I, Bender R, Hunger-Dathe W, Kloos C, Muller UA. Flexible intensiveinsulin therapy in adults with type 1 diabetes andhigh risk for severe hypoglycemia and diabeticketoacidosis. Diabetes Care 2006;29:2196–219936. Cox D, Gonder-Frederick L, Polonsky W,Schlundt D, Julian D, Clarke W. A multicenterevaluation of blood glucose awarenesstraining-II. Diabetes Care 1995;18:523–52837. Broers S, van Vliet KP, le Cessie S, SpinhovenP, van der Ven NC, Radder JK. Blood glucoseawareness training in Dutch type 1 diabetes pa-tients: one-year follow-up. Neth J Med 2005;63:164–16938. Schachinger H, Hegar K, Hermanns N, et al.Randomized controlled clinical trial of BloodGlucose Awareness Training (BGAT III) in Swit-zerland and Germany. J Behav Med 2005;28:587–59439. Fanelli CG, Epifano L, Rambotti AM, et al.Meticulous prevention of hypoglycemia nor-malizes the glycemic thresholds and magnitudeof most of neuroendocrine responses to,symptoms of, and cognitive function during
hypoglycemia in intensively treated patientswith short-term IDDM. Diabetes 1993;42:1683–168940. Cranston I, Lomas J, Maran A, Macdonald I,Amiel SA. Restoration of hypoglycaemia aware-ness in patients with long-duration insulin-dependent diabetes. Lancet 1994;344:283–28741. Dagogo-Jack S, Rattarasarn C, Cryer PE. Re-versal of hypoglycemia unawareness, but notdefective glucose counterregulation, in IDDM.Diabetes 1994;43:1426–143442. Fanelli C, Pampanelli S, Epifano L, et al.Long-term recovery from unawareness, defi-cient counterregulation and lack of cognitivedysfunction during hypoglycaemia, following in-stitution of rational, intensive insulin therapy inIDDM (published correction appears in Diabe-tolgia 1995;38:254). Diabetologia 1994;37:1265–127643. Cox DJ, Kovatchev B, Koev D, et al. Hypogly-cemia anticipation, awareness and treatmenttraining (HAATT) reduces occurrence of severehypoglycemia among adults with type 1 diabe-tes mellitus. Int J Behav Med 2004;11:212–21844. Hermanns N, Kulzer B, Krichbaum M,Kubiak T, Haak T. Long-term effect of an educa-tion program (HyPOS) on the incidence of se-vere hypoglycemia in patients with type 1diabetes. Diabetes Care 2010;33:e3645. Rankin D, Elliott J, Heller S, et al. Experi-ences of hypoglycaemia unawareness amongstpeople with Type 1 diabetes: a qualitative in-vestigation. Chronic Illn 2013;10:180–19146. Rogers HA, de Zoysa N, Amiel SA. Patientexperience of hypoglycaemia unawareness intype 1 diabetes: are patients appropriately con-cerned? Diabet Med 2012;29:321–32747. de Zoysa N, Rogers H, Stadler M, et al. Apsychoeducational program to restore hypogly-cemia awareness: the DAFNE-HART pilot study.Diabetes Care 2014;37:863–86648. Little SA, Leelarathna L, Walkinshaw E, et al.Recovery of hypoglycemia awareness in long-standing type 1 diabetes: a multicenter 2 3 2factorial randomized controlled trial comparinginsulin pump with multiple daily injections andcontinuous with conventional glucose self-monitoring (HypoCOMPaSS). Diabetes Care2014;37:2114–212249. Little S, Shaw J, Home P. Hypoglycemiarates with basal insulin analogs. Diabetes Tech-nol Ther 2011;13(Suppl. 1):S53–S6450. Holleman F, Gale EA. Nice insulins, pityabout the evidence. Diabetologia 2007;50:1783–179051. Singh SR, Ahmad F, Lal A, Yu C, Bai Z,Bennett H. Efficacy and safety of insulin ana-logues for the management of diabetes melli-tus: a meta-analysis. CMAJ 2009;180:385–39752. Heise T, Nosek L, Rønn BB, et al. Lowerwithin-subject variability of insulin detemir incomparison to NPH insulin and insulin glarginein people with type 1 diabetes. Diabetes 2004;53:1614–162053. Monami M, Marchionni N, Mannucci E.Long-acting insulin analogues vs. NPH humaninsulin in type 1 diabetes. A meta-analysis.Diabetes Obes Metab 2009;11:372–37854. Tricco AC, Antony J, Khan PA, et al. Safetyand effectiveness of dipeptidyl peptidase-4 in-hibitors versus intermediate-acting insulin orplacebo for patients with type 2 diabetes failing
care.diabetesjournals.org Choudhary and Associates 1027

two oral antihyperglycaemic agents: a system-atic review and network meta-analysis. BMJOpen 2014;4:e00575255. Heller S, Buse J, Fisher M, et al.; BEGINBasal-Bolus Type 1 Trial Investigators. Insulindegludec, an ultra-longacting basal insulin, ver-sus insulin glargine in basal-bolus treatmentwith mealtime insulin aspart in type 1 diabetes(BEGIN Basal-Bolus Type 1): a phase 3, random-ised, open-label, treat-to-target non-inferioritytrial. Lancet 2012;379:1489–149756. Pedersen-Bjergaard U, Kristensen PL, Beck-Nielsen H, et al. Effect of insulin analogues onrisk of severe hypoglycaemia in patients withtype 1 diabetes prone to recurrent severe hypo-glycaemia (HypoAna trial): a prospective, ran-domised, open-label, blinded-endpoint crossovertrial. Lancet Diabetes Endocrinol 2014;2:553–56157. Pickup JC, Sutton AJ. Severe hypoglycaemiaand glycaemic control in type 1 diabetes: meta-analysis of multiple daily insulin injectionscompared with continuous subcutaneous insu-lin infusion. Diabet Med 2008;25:765–77458. Gimenez M, Lara M, Conget I. Sustainedefficacy of continuous subcutaneous insulin in-fusion in type 1 diabetes subjects with recurrentnon-severe and severe hypoglycemia and hypo-glycemia unawareness: a pilot study. DiabetesTechnol Ther 2010;12:517–52159. Chetty VT, Almulla A, Odueyungbo A,Thabane L. The effect of continuous subcutane-ous glucose monitoring (CGMS) versus intermit-tent whole blood finger-stick glucose monitoring(SBGM) onhemoglobin A1c (HbA1c) levels in typeI diabetic patients: a systematic review. DiabetesRes Clin Pract 2008;81:79–8760. Szypowska A, Ramotowska A, Dzygalo K,Golicki D. Beneficial effect of real-time continu-ous glucosemonitoring system on glycemic con-trol in type 1 diabetic patients: systematicreview and meta-analysis of randomized trials.Eur J Endocrinol 2012;166:567–57461. Leelarathna L, Little SA,Walkinshaw E, et al.Restoration of self-awareness of hypoglycemiain adults with long-standing type 1 diabetes:hyperinsulinemic-hypoglycemic clamp sub-study results from the HypoCOMPaSS trial. Di-abetes Care 2013;36:4063–407062. Bergenstal RM, Tamborlane WV, AhmannA, et al.; STAR 3 Study Group. Effectiveness ofsensor-augmented insulin-pump therapy intype 1 diabetes. N Engl J Med 2010;363:311–32063. Buckingham B, Block J, Burdick J, et al.; Di-abetes Research in Children Network. Responseto nocturnal alarms using a real-time glucosesensor. Diabetes Technol Ther 2005;7:440–44764. Bergenstal RM, Klonoff DC, Garg SK, et al.;ASPIRE In-Home Study Group. Threshold-basedinsulin-pump interruption for reduction of hy-poglycemia. N Engl J Med 2013;369:224–23265. Ly TT, Nicholas JA, Retterath A, Lim EM,Davis EA, Jones TW. Effect of sensor-augmentedinsulin pump therapy and automated insulinsuspension vs standard insulin pump therapyon hypoglycemia in patients with type 1 diabe-tes: a randomized clinical trial. JAMA 2013;310:1240–124766. Choudhary P, Ramasamy S, Green L, et al.Real-time continuous glucose monitoring sig-nificantly reduces severe hypoglycemia in
hypoglycemia-unaware patients with type 1 di-abetes. Diabetes Care 2013;36:4160–416267. Russell SJ, El-Khatib FH, Sinha M, et al. Out-patient glycemic control with a bionic pancreasin type 1 diabetes. N Engl J Med 2014;371:313–32568. Hovorka R, Kumareswaran K, Harris J, et al.Overnight closed loop insulin delivery (artificialpancreas) in adults with type 1 diabetes: cross-over randomised controlled studies. BMJ 2011;342:d185569. Haidar A, Legault L, Messier V, Mitre TM,Leroux C, Rabasa-Lhoret R. Comparison of dual-hormone artificial pancreas, single-hormone ar-tificial pancreas, and conventional insulin pumptherapy for glycaemic control in patients withtype 1 diabetes: an open-label randomised con-trolled crossover trial. Lancet Diabetes Endocri-nol 2015;3:17–2670. Gruessner RW, Gruessner AC. The currentstate of pancreas transplantation. Nat Rev En-docrinol 2013;9:555–56271. Barton FB, Rickels MR, Alejandro R, et al.Improvement in outcomes of clinical islet trans-plantation: 1999-2010. Diabetes Care 2012;35:1436–144572. Niclauss N, Morel P, Berney T. Has the gapbetween pancreas and islet transplantationclosed? Transplantation 2014;98:593–59973. Bassi R, Fiorina P. Impact of islet transplan-tation on diabetes complications and quality oflife. Curr Diab Rep 2011;11:355–36374. Thompson DM, Meloche M, Ao Z, et al. Re-duced progression of diabetic microvascularcomplications with islet cell transplantationcompared with intensive medical therapy.Transplantation 2011;91:373–37875. Robertson RP. Islet transplantation for type1 diabetes, 2015: what have we learned fromalloislet and autoislet successes? Diabetes Care2015;38:1030–103576. Kendall DM, Rooney DP, Smets YF, SalazarBolding L, Robertson RP. Pancreas transplanta-tion restores epinephrine response and symp-tom recognition during hypoglycemia inpatients with long-standing type I diabetesand autonomic neuropathy. Diabetes 1997;46:249–25777. Rickels MR, Fuller C, Dalton-Bakes C, et al.Restoration of glucose counterregulation byislet transplantation in long-standing type 1diabetes. Diabetes 2015;64:1713–171878. Rickels MR, Mueller R, Teff KL, Naji A. b-Cellsecretory capacity and demand in recipients ofislet, pancreas, and kidney transplants. J ClinEndocrinol Metab 2010;95:1238–124679. Rickels MR, Liu C, Shlansky-Goldberg RD,et al. Improvement in b-cell secretory capacityafter human islet transplantation according tothe CIT07 protocol. Diabetes 2013;62:2890–289780. Paty BW, Lanz K, Kendall DM, SutherlandDE, Robertson RP. Restored hypoglycemic coun-terregulation is stable in successful pancreastransplant recipients for up to 19 years aftertransplantation. Transplantation 2001;72:1103–110781. Barrou Z, Seaquist ER, Robertson RP. Pan-creas transplantation in diabetic humans nor-malizes hepatic glucose production duringhypoglycemia. Diabetes 1994;43:661–666
82. Matsumoto I, Sawada T, Nakano M, et al.Improvement in islet yield from obese donorsfor human islet transplants. Transplantation2004;78:880–88583. Gruessner AC, Sutherland DE, GruessnerRW. Long-term outcome after pancreas trans-plantation. Curr Opin Organ Transplant 2012;17:100–10584. Sollinger HW, Odorico JS, Becker YT,D’Alessandro AM, Pirsch JD. One thousand si-multaneous pancreas-kidney transplants at asingle center with 22-year follow-up. Ann Surg2009;250:618–63085. Lehmann R, Graziano J, Brockmann J, et al.Glycemic control in simultaneous islet-kidneyversus pancreas-kidney transplantation in type1 diabetes: a prospective 13-year follow-up. Di-abetes Care 2015;38:752–75986. Gruessner RW, Dunn DL, Gruessner AC,Matas AJ, Najarian JS, Sutherland DE. Recipientrisk factors have an impact on technical failureand patient and graft survival rates in bladder-drained pancreas transplants. Transplantation1994;57:1598–160687. Kandaswamy R, Sutherland DE. Pancreasversus islet transplantation in diabetes mellitus:how to allocate deceased donor pancreata?Transplant Proc 2006;38:365–36788. Senior PA, Bellin MD, Alejandro R, et al.Consistency of quantitative scores of hypogly-cemia severity and glycemic lability and com-parision with continuous glucose monitoringsystem measures in long-standing type 1 diabe-tes. Diabetes Technol Ther 2015;17:235–24289. Bellin MD, Barton FB, Heitman A, et al.Potent induction immunotherapy promoteslong-term insulin independence after islettransplantation in type 1 diabetes. Am J Trans-plant 2012;12:1576–158390. Qi M, Kinzer K, Danielson KK, et al. Five-yearfollow-up of patients with type 1 diabetes trans-planted with allogeneic islets: the UIC experi-ence. Acta Diabetol 2014;51:833–84391. Clinical Islet Transplantation Consortium.Available from http://www.isletstudy.org. Ac-cessed 2 February 201592. O’Connell PJ, Holmes-Walker DJ, GoodmanD, et al.; Australian Islet Transplant Consortium.Multicenter Australian trial of islet transplanta-tion: improving accessibility and outcomes. AmJ Transplant 2013;13:1850–185893. Brooks AM, Walker N, Aldibbiat A, et al.Attainment of metabolic goals in the integratedUK islet transplant programwith locally isolatedand transported preparations. Am J Transplant2013;13:3236–324394. Ang M, Meyer C, Brendel MD, Bretzel RG,Linn T. Magnitude and mechanisms of glucosecounterregulation following islet transplanta-tion in patients with type 1 diabetes sufferingfrom severe hypoglycaemic episodes. Diabeto-logia 2014;57:623–63295. Paty BW, Senior PA, Lakey JR, Shapiro AM,Ryan EA. Assessment of glycemic control afterislet transplantation using the continuous glu-cose monitor in insulin-independent versus in-sulin-requiring type 1 diabetes subjects.Diabetes Technol Ther 2006;8:165–17396. Gorn L, Faradji RN, Messinger S, et al. Im-pact of islet transplantation on glycemic controlas evidenced by a continuous glucose monitor-ing system. J Diabetes Sci Tech 2008;2:221–228
1028 Type 1 Diabetes Complicated by Hypoglycemia Diabetes Care Volume 38, June 2015

97. Brooks AM, Oram R, Home P, Steen N, ShawJA. Demonstration of an intrinsic relationshipbetween endogenous C-peptide concentrationand determinants of glycemic control in type 1diabetes following islet transplantation. Diabe-tes Care 2015;38:105–11298. Cryer PE. Hypoglycemia begets hypoglyce-mia in IDDM. Diabetes 1993;42:1691–169399. Gerber PA, Pavlicek V, Demartines N, et al.Simultaneous islet-kidney vs pancreas-kidneytransplantation in type 1 diabetes mellitus: a 5year single centre follow-up. Diabetologia 2008;51:110–119100. Ostenson CG, Geelhoed-Duijvestijn P,Lahtela J, Weitgasser R, Markert Jensen M,Pedersen-Bjergaard U. Self-reported non-severe hypoglycaemic events in Europe. DiabetMed 2014;31:92–101101. Kovatchev BP, Cox DJ, Gonder-Frederick LA,Young-Hyman D, Schlundt D, Clarke W. Assess-ment of risk for severe hypoglycemia amongadults with IDDM: validation of the low bloodglucose index. Diabetes Care 1998;21:1870–1875
102. Kovatchev BP, Otto E, Cox D, Gonder-Frederick L, Clarke W. Evaluation of a newmeasure of blood glucose variability in diabetes.Diabetes Care 2006;29:2433–2438103. Bode BW, Buse JB, Fisher M, et al.; BEGIN�Basal-Bolus Type 1 Trial Investigators. Insulin de-gludec improves glycaemic control with lowernocturnal hypoglycaemia risk than insulin glarginein basal-bolus treatment with mealtime insulinaspart in type 1 diabetes (BEGIN(�) Basal-BolusType 1): 2-year results of a randomized clinicaltrial. Diabet Med 2013;30:1293–1297104. Pickup JC, Freeman SC, Sutton AJ. Glycae-mic control in type 1 diabetes during real timecontinuous glucose monitoring compared withself monitoring of blood glucose: meta-analysisof randomised controlled trials using individualpatient data. BMJ 2011;343:d3805105. Wiseman AC. Pancreas transplant optionsfor patients with type 1 diabetes mellitus andchronic kidney disease: simultaneous pancreaskidney or pancreas after kidney? Curr Opin Or-gan Transplant 2012;17:80–86
106. Maffi P, Bertuzzi F, De Taddeo F, et al.Kidney function after islet transplant alone intype 1 diabetes: impact of immunosuppressivetherapy on progression of diabetic nephropa-thy. Diabetes Care 2007;30:1150–1155107. Ojo AO, Held PJ, Port FK, et al. Chronicrenal failure after transplantation of a nonrenalorgan. N Engl J Med 2003;349:931–940108. Klein AS, Messersmith EE, Ratner LE,Kochik R, Baliga PK, Ojo AO. Organ donationand utilization in the United States, 1999-2008. Am J Transplant 2010;10:973–986109. Matesanz R, Domınguez-Gil B, Coll E, de laRosa G, Marazuela R. Spanish experience as aleading country: what kind of measures weretaken? Transpl Int 2011;24:333–343110. Byrne ML, Hopkins D, Littlejohn W, et al.Outcomes for adults with type 1 diabetes re-ferred with severe hypoglycaemia and/or re-ferred for islet transplantation to a specialisthypoglycaemia service. Horm Metab Res 2015;47:9–15
care.diabetesjournals.org Choudhary and Associates 1029