establishing provider-based clinics: advanced topics · establishing provider-based clinics:...
TRANSCRIPT
Provider-Based Rule: Advanced Topics March 5, 2015
Florida Hospital Association 1
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 1
Establishing Provider-Based Clinics:
Advanced Topics
Version 12.2 - 2014
Notes © 1996-2015, Abbey & Abbey, Consultants, Inc.
CPT® Codes – © 2014-2015 AMA
Hosted By:
www.FHA.org
Presented By:
Duane C. Abbey, Ph.D., CFP
Abbey & Abbey, Consultants, [email protected] http://www.aaciweb.com
http://www.APCNow.com http://www.HIPAAMaster.com
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 2
This workshop and other material provided are designed to provide accurate and
authoritative information. The authors, presenters and sponsors have made every
reasonable effort to ensure the accuracy of the information provided in this
workshop material. However, all appropriate sources should be verified for the
correct ICD-9-CM Codes, ICD-10-CM Diagnosis Codes, ICD-10-PCS Procedure
Codes, CPT/HCPCS Codes and Revenue Center Codes. The user is ultimately
responsible for correct coding and billing.
The author and presenters are not liable and make no guarantee or warranty;
either expressed or implied, that the information compiled or presented is error-
free. All users need to verify information with the Fiscal Intermediary, Carriers,
other third party payers, and the various directives and memorandums issued by
CMS, DOJ, OIG and associated state and federal governmental agencies. The
user assumes all risk and liability with the use and/or misuse of this information.
Disclaimer
Provider-Based Rule: Advanced Topics March 5, 2015
Florida Hospital Association 2
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 3
Presentation Faculty
Duane C. Abbey, Ph.D., CFP – Dr. Abbey is a healthcare consultant and educator with over 20
years of experience. He has worked with hospitals, clinics,
physicians in various specialties, home health agencies and other health care providers.
His primary work is with optimizing reimbursement under various Prospective Payment
Systems. He also works extensively with various compliance issues and performs
chargemaster reviews along with coding and billing audits.
Dr. Abbey is the President of Abbey & Abbey, Consultants, Inc. A wide range of consulting
services is provided across the country including charge master reviews, APC compliance
reviews, in-service training, physician training, and coding and billing reviews.
Dr. Abbey is the author of fourteen books on health care, including:
•“Non-Physician Providers: Guide to Coding, Billing, and Reimbursement”
•“Emergency Department: Coding, Billing and Reimbursement”, and
•“Chargemasters: Strategies to Ensure Accurate Reimbursement and Compliance”.
Recent books include: “Compliance for Coding, Billing & Reimbursement A Systematic
Approach to Developing a Comprehensive Program”, “Introduction to Healthcare
Payment Systems”, “Fee Schedule Payment Systems” and “Prospective Payment
Systems” from Taylor and Francis. He has just finished the fourth book in the Healthcare
Payment System Series; “Cost-Based, Charge-Based and Contractual Payment Systems”.
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 4
Provider-Based Clinics - Advanced
Introduction
Provider-Based Status – PBS Previously, Called Hospital-Based What Is It?
• Be Careful With Terminology Provider-Based Clinics Provider-Based Clinical ServicesGeneral Provider-Based Rule (PBR)
• General Rules Apply To Both Inpatient and Outpatient Owned, Operated and Fully Integrated With Hospital
• Criteria To Achieve Hospital (Main Provider) Includes CAHs (and Other Providers) Operational Definition Provider-based means filing a UB-04 –
Provider-based clinics file (or there is filed) both a UB-04 (CMS-1450) and a 1500 (CMS-1500)
CMS Interested Only Where There Is A Payment Differential – Clinics and Clinical Services Fall Into This Category – Application/Approval vs. Attestation
RHCs and FQHCs Are Partially Outside These Rules – 42 CFR §413.65
• Still Referred To As ‘Provider-Based’
• Special Rules
• Difficulties With APC Interface
Provider-Based Rule: Advanced Topics March 5, 2015
Florida Hospital Association 3
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 5
Provider-Based Status – PBS - Continued
Freestanding Is The Opposite Of Being Provider-Based
The Provider-Based Rule Is Complex and There Is Confusion
Fundamental Terminology – ‘Facility or Organization’
• CMS is now using PBD – Provider-Based Department
Must Understand Multiple References
Cost Report Involvement
OIG Concerns
• Really Don’t Want PBS Clinics At All!
• Should Be No Payment Differential
The Emergency Department (ED) Is A Special Provider-Based ‘Clinic’
Many of the CDM concerns for general provider-based clinics are also
present for the ED
• Professional coding/billing versus technical component
coding/billing
EMTALA – Emergency Medical Treatment and Labor Act
• Creates a special set of requirements for the ED (technically the
DED or Dedicated Emergency Department)
When does a provider-based clinic become a DED?
Special EMTALA requirements for off-campus provider-based clinics.
Provider-Based Clinics - Advanced
Introduction
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 6
Provider-Based Clinics - Advanced
Introduction
Acronyms – As with other areas of healthcare organizations and
associated coding, billing and reimbursement, there are many acronyms.
PBR – Provider-Based Rule 42 CFR §415.65
PBS – Provider-Based Status
PBD – Provider-Based Department
• This terminology has been used only in the last couple of years.
EMTALA – Emergency Medical Treatment and Labor Act
ED – Emergency Department
CBR – Coding, Billing and Reimbursement
CDM – Charge Description Master or Chargemaster
SOS - Site-of-Service (Differential)
POS – Place of Service (1500 Claim Form)
MAC – Medicare Administrative Contractor
RO – Regional Office
MOB – Medical Office Building
RBRVS – Resource Based Relative Value Scale
MPFS – Medicare Physician Fee Schedule
APCs – Ambulatory Payment Classifications
RVUs – Relative Value Units

Provider-Based Rule: Advanced Topics March 5, 2015
Florida Hospital Association 4
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 7
To review the Provider-Based Rule (PBR).
To understand the differences between freestanding and provider-based
clinics.
To understand the economic advantages of provider-based clinics.
To review and appreciate special requirements for provider-based clinics.
To appreciate special compliance concerns associated with provider-based
status.
To discuss coding and billing issues for provider-based clinics.
To understand how to qualify clinics that are outside the 35-mile default
limit.
To discuss signage and proper identification for provider-based
operations. To discuss complicated issues such as joint use of space and
time-share space utilization.
Provider-Based Clinics - Advanced
Objectives
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 8
Provider-Based Clinics - Advanced
Objectives
To understand provider-based reporting requirements and the CMS-855
forms.
To explore the application of the physician supervision requirement for
outpatient services.
To discuss operation issues such as setting fees, patient relations and
medical staff organizational structuring.
To review on-going ambiguities in the Provider-Based Rule affecting
provider-based operations.
To work through several case studies involving special issues in the
establishment of the provider-based clinics.
Note: This workshop assumes that participants have a basic
knowledge of the Provider-Based Rule and provider-based clinics along
with a background with the more common challenges and regulatory
requirements.
Provider-Based Rule: Advanced Topics March 5, 2015
Florida Hospital Association 5
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 9
The Apex Medical Center owns and operates a family practice clinic that is
located on its campus right across the street. There is a sky-walk and
there is a large parking ramp right next to the clinic. The physicians and all
the staff personnel are employees of the hospital. Due to competitive
pressures, the only billing made is the professional component on a 1500.
Is this a provider-based clinic?
Yes?
No?
• What if this clinic meets all the PBR requirements, do we have to
file a UB-04? What about Place-of-Service on the 1500?
Is the ED at the Apex Medical Center a provider-based department (clinic)?
Yes?
No?
Maybe?
Provider-Based Clinics
Introduction - Warm-Up Exercises
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 10
Provider-Based Clinics
Introduction - Warm-Up Exercise
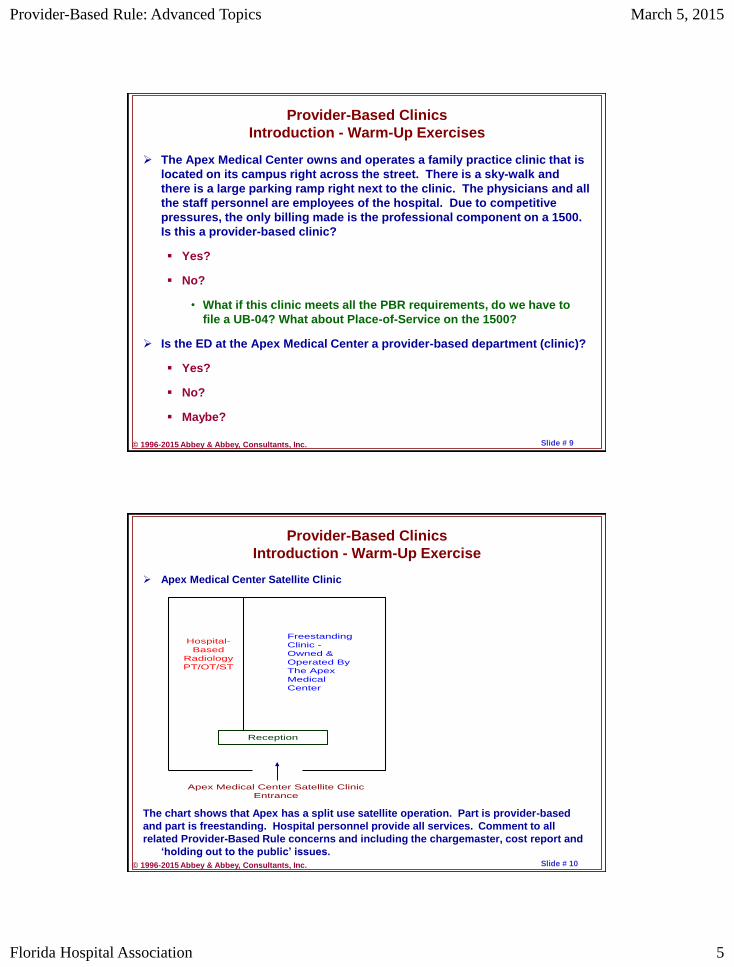
Apex Medical Center Satellite Clinic
The chart shows that Apex has a split use satellite operation. Part is provider-based
and part is freestanding. Hospital personnel provide all services. Comment to all
related Provider-Based Rule concerns and including the chargemaster, cost report and
‘holding out to the public’ issues.
Reception
Apex Medical Center Satellite Clinic
Entrance
Freestanding
Clinic -
Owned &
Operated By
The Apex
Medical
Center
Hospital-
Based
Radiology
PT/OT/ST
Provider-Based Rule: Advanced Topics March 5, 2015
Florida Hospital Association 6
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 11
The PBR Is Complex and There Is Confusion Several Areas Where The Rules Are Not Clear See PM A-03-030 Directions to FIs –Attestations vs. Determinations
Provider-Based Clinics 1980’s Additional Income From Both A UB-04 Technical Component and CMS-
1500 Professional Component Very Little Reduction in Payment for Professional Component – Site-Of-
Service Differential Applied To Only A Few Codes Savvy Hospitals Started Using This Organizational Concept See MAP
– Model Ambulatory Practice – Clinics Mid-1990’s – CMS (Then HCFA) Became Concerned About Proliferation of
Provider-Based Clinics Issued the Infamous PM A-96-7 (Re-Issued As PM A-99-24) 8-Criteria For Being Provider-Based Clinic Not Legislated and Not In Code of Federal Regulations Variable Guidance from Fiscal Intermediaries and Carriers Very few codes subject to physician payment reduction.
• See the implementation of the Medicare Physician Fee Schedule (MPFS) through RBRVS (Resource Based Relative Value Scale).November 24, 1991 Federal Register Entry
Provider-Based Clinics
Provider-Based Rule – Very Brief History
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 12
April 7, 2000 – Issued New Comprehensive Rule
Note: Yes, this was issued in the APC FR Entry
The new Provider-Based Rule went beyond just considering outpatient
situations. Inpatient situations are also included to some degree.
The new PBR formalized the criteria issued in PM A-96-7.
CY2001 – CY2014
Over these years the PBR continued to evolve.
• Some degree of change has occurred almost every year.
• Some changes are explicit, while other changes are more
operational, that is, the way CMS and MACs treat certain issues.
• Example: Attestation is a process of indicating that a given
operation meets the PBR. A request for determination is a long
form requesting approval. Today attestations equal determinations.
• Example: Use of phrase ‘Provider-Based Departments’ or PBDs.
Starting in CY2008 started to make significant changes (CMS maintains
they are only clarifications).
To Understand PBR – You Must Master and Understand Multiple
References – CFR Sections, Federal Register and Associated Sources
• See AACI’s APC Website To Download Documents
www.APCNow.com/PBRInformationToolkit.htm
Provider-Based Clinics
Provider-Based Rule – Very Brief History
Provider-Based Rule: Advanced Topics March 5, 2015
Florida Hospital Association 7
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 13
Basically Eight Criteria See Famous PM A-96-7 – Repeated as A-99-24
Geographic Proximity
Integral and Subordinate Part
Under Same Accreditation
Common Ownership and Control
Day-to-Day Supervision
Clinical Services Integration
Held Out To The Public
Financial Integration
These “old” criteria where brought forward and placed in §413.65 of the
CFR
Some Changes Accreditation to Licensure (& Accreditation)
The new rules basically formalized the old rules with much more explicit
terminology.
The PBR goes well beyond directives made prior to CY2000.
The old rules addressed only ‘clinics’ while the revised PBR addresses all
departments of the hospital, both inpatient and outpatient.
Note that much discussion pertains to ‘off-campus’ clinics, but over the
years this concept has expanded to provider-based departments
(PBDs) apparently of all types.
Provider-Based Clinics
Provider-Based Rule - “Old” Criteria
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 14
Provider-Based Clinics - Advanced
Fundamental Concepts/Analysis
Geographic Location Of Clinic
In The Hospital
• As of 2010, we have a formal definition.
Out Of The Hospital, On Campus
• Recent Physician Supervision Requirements – New Guidance
Off Campus Within 35 Miles
Off Campus More Than 35 Miles (May be able to get exception.)
Definition Of “Campus”
250 Yard Rule
May Need Special Determination By RO (Regional Office)
ZIP Code Analysis – More Than 35 Miles
75%-75% Overlap
75% Rule
Off-Campus Provider-Based Clinic Obligations
Physician Supervision See Updated Guidance & Controversy
Integrate With EMTALA
Patient Notice Of Two Co-Payments
• Slight Change August 12, 2005 FR Entry If Only One Co-Payment
vs. Two Co-Payments
Provider-Based Rule: Advanced Topics March 5, 2015
Florida Hospital Association 8
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 15
Licensure
Licensure Is A State Level Process
State Level Idiosyncrasies – See Also Certification
Licensure versus Accreditation
Operation Under Ownership and Control of Main Provider
100% Ownership See 3-Day Pre-Admission Window (Wholly Owned
or Operated)
Main Provider – Final Administrative Responsibility
Administration and Supervision
Clinical Services
Professional Staff – Same Privileges
Medical Director
Medical Staff Organization
Medical Records – Integrated (Cross Referenced)
Financial Integration
Tax Identification Numbers – Accounting Purposes?
National Provider Identifiers? See CMS-855 Forms–Billing Privileges
Public Awareness Patients must know entering hospital.
Location In Immediate Vicinity
Provider-Based Clinics - Advanced
PBR - Qualifying For PBS
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 16
Provider-Based Status
EMTALA Changes For Off-Campus
• New Definition – “Dedicated Emergency Department”
• Off-Campus Without DED – “Call 911” versus Working With Main
Provider ED
Inappropriate Treatment as Provider-Based
• Inappropriate Billing
• Good Faith Effort
• What Are The Penalties?
Physician Supervision Changes
• Definitions and Requirements – Off-Campus vs. On-Campus
• Mid-Levels – Non-Physician Practitioners – Recognition as
Supervisors
Other Changes
• Joint Ventures – Acceptable For On-Campus
• Management Contracts – Acceptable For On-Campus
• Under Arrangements – Never Changed or Explained (!)
What does the under arrangement prohibition mean?
Provider-Based Clinics - Advanced
PBR – On-Going Changes
Provider-Based Rule: Advanced Topics March 5, 2015
Florida Hospital Association 9
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 17
Qualifying and Application/Attestation This Involves Determination of Provider-Based Status Situations Such
As Clinics and Other Activities
Prohibitions Prohibitions Can Apply To Any and All Hospital Activities
Obligations Obligations Can Apply To Any and All Hospital Activities
Reporting Report Any ‘Material Changes’ Relationship to CMS-855 Reporting
• Updating Attestation Forms (?)
These four items must be considered for a wide range of circumstances.
Provider-Based Clinics - Advanced
PBR - Overall Analysis Template
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 18
Provider-Based Clinics - Advanced
Provider-Based Clinics - Billing
Split Billing – Chargemaster Issue
1500 + UB-04
Only Required To Split-Bill Medicare
What About Other Third-Party Payers?
What About Secondary Payers
• Split-Bill Medicare Primary ONLY??
How To Set Fees
• Take Current Physician Fee Schedule & Divide?
• Medicare Charging Rule - Compliance
• Example
Current Physician Fee = $80.00
New Physician Fee = $60.00
Technical Component = $20.00
Any Problems?
o Physician Fee
o Technical Component Fee
• Note: We are making certain to bill all patients the same amount.
Notice of Two Co-Payments
• What must be done to meet this requirement for off-campus
clinics?
Provider-Based Rule: Advanced Topics March 5, 2015
Florida Hospital Association 10
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 19
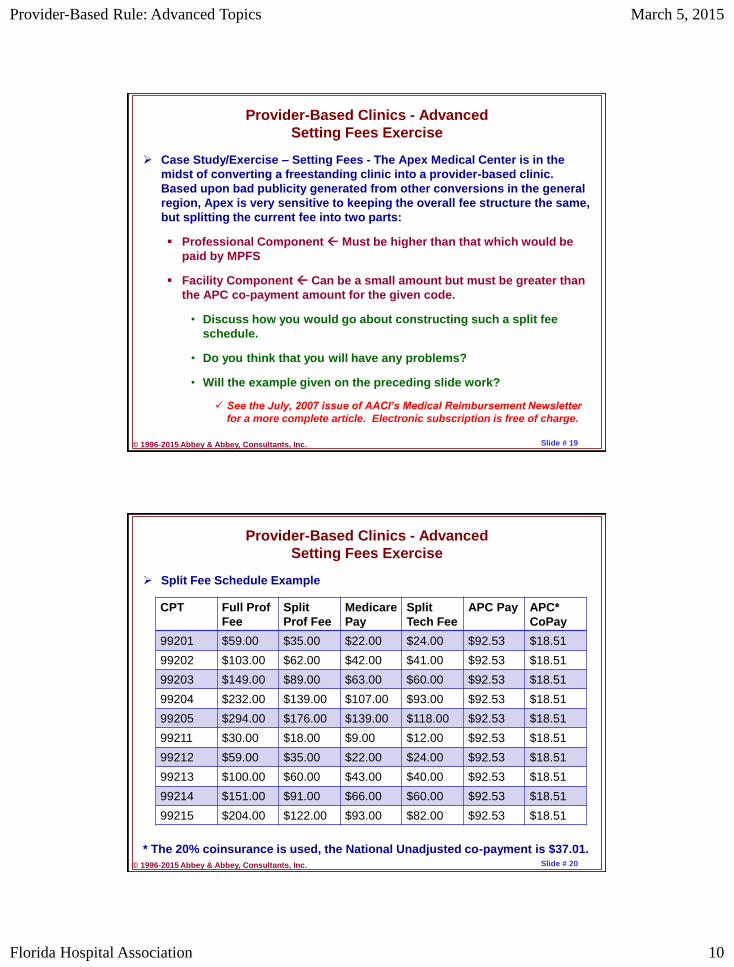
Provider-Based Clinics - Advanced
Setting Fees Exercise
Case Study/Exercise – Setting Fees - The Apex Medical Center is in the
midst of converting a freestanding clinic into a provider-based clinic.
Based upon bad publicity generated from other conversions in the general
region, Apex is very sensitive to keeping the overall fee structure the same,
but splitting the current fee into two parts:
Professional Component Must be higher than that which would be
paid by MPFS
Facility Component Can be a small amount but must be greater than
the APC co-payment amount for the given code.
• Discuss how you would go about constructing such a split fee
schedule.
• Do you think that you will have any problems?
• Will the example given on the preceding slide work?
See the July, 2007 issue of AACI’s Medical Reimbursement Newsletter
for a more complete article. Electronic subscription is free of charge.
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 20
Provider-Based Clinics - Advanced
Setting Fees Exercise
Split Fee Schedule Example
* The 20% coinsurance is used, the National Unadjusted co-payment is $37.01.
CPT Full Prof
Fee
Split
Prof Fee
Medicare
Pay
Split
Tech Fee
APC Pay APC*
CoPay
99201 $59.00 $35.00 $22.00 $24.00 $92.53 $18.51
99202 $103.00 $62.00 $42.00 $41.00 $92.53 $18.51
99203 $149.00 $89.00 $63.00 $60.00 $92.53 $18.51
99204 $232.00 $139.00 $107.00 $93.00 $92.53 $18.51
99205 $294.00 $176.00 $139.00 $118.00 $92.53 $18.51
99211 $30.00 $18.00 $9.00 $12.00 $92.53 $18.51
99212 $59.00 $35.00 $22.00 $24.00 $92.53 $18.51
99213 $100.00 $60.00 $43.00 $40.00 $92.53 $18.51
99214 $151.00 $91.00 $66.00 $60.00 $92.53 $18.51
99215 $204.00 $122.00 $93.00 $82.00 $92.53 $18.51
Provider-Based Rule: Advanced Topics March 5, 2015
Florida Hospital Association 11
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 21
Provider-Based Clinics - Advanced
Location and Space Considerations
Shared Space Situations
Many Different Situations Can Arise
The main concern is that of signage and ‘holding out to the public’.
Patients must know that they have entered hospital ‘property’.
• For off-campus situations, see special EMTALA requirements.
Space may be:
• Owned
• Rented/Leased
• Time-Shared
Each situation will need careful assessment so that the MAC/RO will
accept the attestations and/or approve the request for determination.
• Careful attention must be given to cost reporting implications.
• Consider the shared space at the Satellite Clinic described on Slide
# 10.
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 22
Provider-Based Clinics - Advanced
Location and Space Considerations
Case Study/Exercise – Split-Use Building - The Apex Medical Center has
established a provider-based clinic about 20 miles from the hospital. They
are renting space in a nice building that has an entrance with a long
hallway that splits the building into two parts. The clinic is on the left while
on the right is a real estate agency.
Discuss signage issues.
• How will the patient know they are on hospital property?
What about accreditation?
Are there going to be any local/state regulations?
Will the MAC/RO question this type of arrangement?
• What kind of documentation can you develop to justify that
provider-based requirements are being met?
Provider-Based Rule: Advanced Topics March 5, 2015
Florida Hospital Association 12
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 23
Provider-Based Clinics - Advanced
Location and Space Considerations
Case Study/Exercise – MOB - There is a Medical Office Building right next
to the Apex Medical Center. There is a skywalk between the two buildings.
Part of the offices in the building are rented by physicians who have
private (i.e., freestanding) practices. Several of the offices are slated to
become provider-based clinics.
Should there be any concern about signage in this type of case?
What about the main directory in the lobby?
What about signage for the individual offices that are part of the
hospital?
What kind of EMTALA policy should be established?
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 24
Provider-Based Clinics - Advanced
Location and Space Considerations
Case Study/Exercise – Time-Share Arrangements – Two specialists are
employed by Apex. Each of them are in different specialty that is in very
short supply in the local area. There is a smaller hospital about 25 miles
away. Each of these specialists spends one day a week at the smaller
hospital. One on Tuesdays and one on Thursdays. Each of these two
physicians provide services in a nice specialty clinic of the smaller
hospital. While the same set of examination rooms are used by each of the
two specialists, the registration and front-desk staff are provided by the
smaller hospital. Apex wants the operation for the two physicians to be
provider-based to Apex (not the smaller hospital).
Is this feasible?
What will need to be accomplished relative to signage and holding-out
to the public?
What about licensing and accreditation?
Will there be any cost-report challenges?
Provider-Based Rule: Advanced Topics March 5, 2015
Florida Hospital Association 13
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 25
Provider-Based Clinics - Advanced
Location and Space Considerations
Case Study/Exercise – Cardiologists Inside MOB - A group of cardiologist
has joined forces with the Apex Medical Center. The hospital has allocated
one-half of one floor of a Medical Office Building for the clinic. The
physician services, that is, evaluation and management, will be conducted
as a freestanding operation. The cardiologist will do their own
documentation and billing in addition to having clinical staff (i.e., nurses,
medical assistants). However, all the technical services (e.g., treadmills,
stress tests, EKGs, Holter monitors, etc.) will be performed in the same
general area only these will be under the purview of the hospital. That is,
the hospital will be billing for all these technical services as a facility.
What concerns to you have about this kind of an arrangement?
How are patients going to know that they have left the physician clinic
and are now in a hospital (facility) area?
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 26
Provider-Based Clinics - Advanced
Physician Supervision
April 7, 2000 Federal Register, Page 18525 (65 FR 18525)
“We emphasize that our proposed amendment of § 410.27 to require
direct supervision of hospital services furnished incident to a physician
service to outpatients applies to services furnished at an entity that is
located off the campus of a hospital that we designate as having
provider-based status as a department of a hospital in accordance with
the provisions of § 413.65. Our proposed amendment of § 410.27 to
require direct supervision of hospital services furnished incident to a
physician service to outpatients does not apply to services furnished in
a department of a hospital that is located on the campus of that
hospital.”
• This is the language that CMS claims that healthcare providers have
‘misinterpreted’. Questions started arising in CY2008.
Physician Supervision
Diagnostic
Therapeutic
Provider-Based Rule: Advanced Topics March 5, 2015
Florida Hospital Association 14
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 27
Provider-Based Clinics - Advanced
Physician Supervision
Diagnostic Testing
Diagnostic testing supervision involves three levels of supervisions:
• General,
• Direct, and
• Personal.
“For CY 2010, we are finalizing the proposal to require that all hospital
outpatient diagnostic services provided directly or under arrangement,
whether provided in the hospital, in a PBD of a hospital, or at a
nonhospital location, follow the physician supervision requirements for
individual tests as listed in the MPFS Relative Value File.” (74 FR
60591)
• Note: Mid-levels are not allowed to meet the diagnostic testing
supervisory requirement. They can provide the services, but are
not allowed to supervise the conduct of the services.
Does this make any sense??
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 28
Provider-Based Clinics - Advanced
Physician Supervision
Therapeutic Services
To What Services Does Physician Supervision Apply?
• CMS started with ‘incident-to physician’ services.
This addresses most services
• CMS has moved on to more limited categories of services as well.
See Radiation Oncology
What are the basic requirements for ‘direct physician supervision’?
• Physician/Practitioner must be interruptible.
• Physician/Practitioner must be immediately available.
• Physician/Practitioner must be able to take over care, not just
address emergencies.
What kind of documentation should be maintained?
What is special about cardiac rehab, pulmonary rehab and intensive
cardiac rehab?
• “For pulmonary rehabilitation, cardiac rehabilitation, and intensive
cardiac rehabilitation services, direct supervision must be
furnished by a doctor or medicine or osteopathy as specified in
§§410.47 and 410.49, respectively.” (Page 72008 – 75 FR 72008)
Provider-Based Rule: Advanced Topics March 5, 2015
Florida Hospital Association 15
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 29
Provider-Based Clinics - Advanced
Physician Supervision
Therapeutic Services
CMS Minimum Supervisory Standard
• “Direct supervision is the minimum standard for supervision of all
Medicare hospital outpatient therapeutic services. Considering that
hospitals furnish a wide array of very complex outpatient services
and procedures, including surgical procedures, CMS would expect
that hospitals already have the credentialing procedures, bylaws,
and other policies in place to ensure that hospital outpatient
services furnished to Medicare beneficiaries are being provided
only by qualified practitioners in accordance with all applicable
laws and regulations. For services not furnished directly by a
physician or nonphysician practitioner, CMS would expect that
these hospital bylaws and policies would ensure that the
therapeutic services are being supervised in a manner
commensurate with their complexity, including personal
supervision where appropriate.” (Transmittal 128 to Publication 100-
02 Medicare Benefits Policy Manual May 28, 2010)
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 30
Provider-Based Clinics - Advanced
Conversion of Clinics
Case Study/Exercise – Conversion of Clinics - This is a group of
oncologists who have established several infusion centers in the general
area. The farthest is 21 miles away. The plan is for the hospital to
purchase the infusion centers and then employ the oncology group. The
oncologists basically want the infusion centers to operate as they have in
the past. All of the employees are to be retained. It turns out that the
fringe benefits for the infusions centers is actually better than for the
hospital (more generous retirement, more vacation days, and better health
coverage). The oncologists want the reporting relationships in this
operation to remain the same. They, the oncologists want to do the hiring,
firing and direction of employees. The physicians have a very good
professional billing system that they want to retain. (Note that there are
significant 340b considerations.)
Are there any compliance concerns from the PBR that relate to this
kind of an arrangement.
What is the proper way to handle this kind of a challenge.
Provider-Based Rule: Advanced Topics March 5, 2015
Florida Hospital Association 16
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 31
Provider-Based Clinics - Advanced
Outside 35 Mile Default Limit
Case Study/Exercise – Infusion Centers - Consider the oncology infusion
centers described in the preceding slide. Let us change the scenario
slightly. In this case we will assume five infusion centers. However, one of
the centers is slightly outside the 35-mile default limit. Unfortunately, both
of the ZIP statistical exceptions also fail. Both the hospital and the
oncologists want all of these operations to be provider-based.
Discuss what Apex can do.
Is it possible to get approval from the MAC/RO when the 35-mile limit is
violated?
What kind of an argument would you make to convince the MAC/RO to
allow the one outlier clinic to be provider-based.
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 32
Provider-Based Clinics - Advanced
Clinic Inside Hospital
Case Study/Exercise – Physicians Inside Hospital - Apex has hired two
relatively expensive cardiovascular physicians. These two physicians will
be housed in an area of the hospital designed for physicians with several
sets of examination rooms along with a reception area. The physicians
want this operation to be freestanding. The main concern is the two co-
payment situation for Medicare beneficiaries.
Can Apex have a freestanding clinic inside the hospital?
How will patients know that this clinic is not part of the hospital?
Are there any cost-report implications?
Do physicians (or actually their employer the hospital) have to pay rent
at fair market value?
Provider-Based Rule: Advanced Topics March 5, 2015
Florida Hospital Association 17
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 33
Provider-Based Clinics - Advanced
Case Studies and Exercises
Case Study/Exercise – Physician Office Laboratory – The Apex Medical
Center developed a freestanding clinic several years ago. This clinic is
located about 20 miles from the hospital. The clinic has grown
significantly over the years. There are about 25 physicians of different
specialties. This is also a ‘Physician Office Laboratory’ at the clinic with a
drawing station to collect various samples. This laboratory also provides
services for other physician clinics in the area. Apex now wants to convert
this clinic to provider-based status.
Outline the steps that will be necessary for conversion.
What about the physician office laboratory?
• Will this laboratory create any complications?
• Will there be CLIA (Clinical Laboratory Improvement Act)
considerations.
• Should this physician office laboratory be discontinued with only
waived tests performed at the clinic?
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 34
Provider-Based Clinics - Advanced
SNF Provider-Based Clinic
Case Study/Exercise – SNF Provider-Based Clinic - The Summit Nursing
Home is a skilled nursing facility that has grown over the years and now
has almost 200 residents. Summit has difficulty getting physicians to
come to their site to provide services to the residents either on a
scheduled basis or on an urgent basis. Thus, Summit has decided to
develop their own provider-based clinic and staff the clinic with a physician
and two mid-level practitioners.
Can Summit establish a provider-based clinic?
Where is this clinic going to be located?
Are there any unusual PBR considerations?
Are there any special payment issues relative to SNF reimbursement?
Provider-Based Rule: Advanced Topics March 5, 2015
Florida Hospital Association 18
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 35
Provider-Based Clinics - Advanced
Medicare Enrollment
Medicare Enrollment for Provider-Based Clinics
There are six different CMS-855 forms.
• CMS-855-A Part A Hospitals
• CMS-855-B Part B Clinics
• CMS-855-I Individuals – Physicians/Practitioners
• CMS-855-O Ordering Referring
• CMS-855-R Reassignment
• CMS-855-S DME
Additional Decisions that Are Required Relative to Enrolling in Medicare
Organizational Structuring
Tax Identification Numbers
NPIs – National Provider Identification Numbers
Which forms are of interest for hospitals relative to provider-based clinics
and operations?
CMS-855-B for the clinic or group of clinics.
CMS-855-I and CMS855-R for the physicians at the clinics.
CMS-855-O for physicians who do not otherwise bill Medicare.
CMS-855-A for the hospital to address issues such as practice
locations because the provider-based clinics are part of the hospital.
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 36
Provider-Based Clinics - Advanced
Medicare Enrollment
Case Study/Exercise – (From the CMS-855-B Workshop) - Apex is a small
integrated delivery system. While many different services are provided,
among the providers are the following:
Home Health Agency DBA Aspire Home Health,
A Skilled Nursing Facility DBA the Summit Nursing Home,
Three freestanding clinics all DBA Center Clinics, and
Three provider-based clinics all DBA Family Practice Associates.
• All of these organizations are wholly owned and operated by the
Apex Medical Center. There is a single TIN for everything. Apex did
obtain separate NPIs for each of these four organizational
structures as subparts. All of the physicians along with non-
physician practitioners (NPPs) are employed by the hospital (i.e.,
Apex Medical Center).
Apex also has a DME company located off the main lobby.
Discuss this arrangement relative to NPIs, TINs, and CMS-855-A and
CMS-855-B.
• Who should be handling this?
• Assuming 35 physicians and NPPs, how many 855 forms will there
be? (Consider the CMS-855-I, 855-R and possibly the 855-O.)
Provider-Based Rule: Advanced Topics March 5, 2015
Florida Hospital Association 19
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 37
Provider-Based Clinics - Advanced
CMS-855-B Section 2C – Identifying Information
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 38
Provider-Based Clinics - Advanced
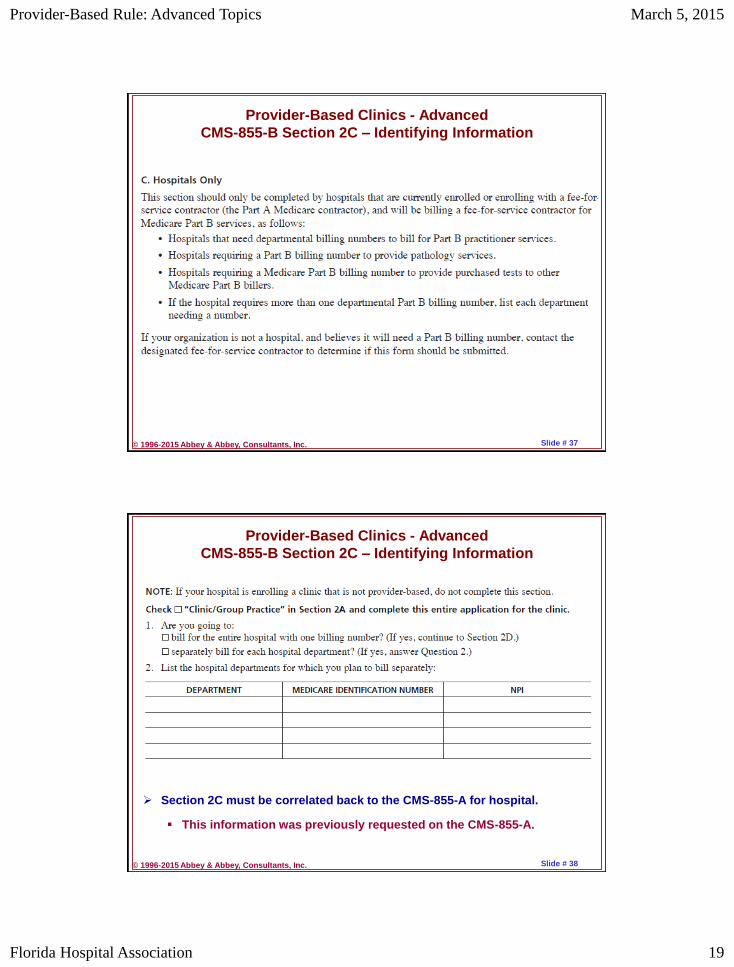
CMS-855-B Section 2C – Identifying Information
Section 2C must be correlated back to the CMS-855-A for hospital.
This information was previously requested on the CMS-855-A.
Provider-Based Rule: Advanced Topics March 5, 2015
Florida Hospital Association 20
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 39
Provider-Based Clinics - Advanced
Attestations and Determinations
Attestations versus Requests for Determination
Note: Technically, hospitals do not have to do anything other than meet
the requirements in the PBR. Thus, hospitals are not required to use
attestations or determinations, as such. There is no official form.
See PM A-03-030
Initially in 2003 -
• The idea was for hospitals to file a simple attestation indicating
compliance with the PBR.
• For off-campus clinics, a full determination was required and
extensive forms were developed to gain approval.
Today – Circumstances and Requirements Have Morphed
• The concept of attestations has really become what was used to be
requests for determination.
• Long forms are used as attestations in order to gain approval from
the MAC/RO.
• There are even hints that attestation can be updated to report
changes. (Will this meet the reporting requirement under PBR?)
See the AACI website, www.APCNow.com/PBRInformationToolkit.htm, for
examples of the attestation form from different MACs.
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 40
Provider-Based Clinics - Advanced
Attestations and Determinations
Filing Attestations
The current attestation forms are quite lengthy and detailed.
Basically, the requirements under the PBR are delineated.
• Sometimes there are simply ‘yes-no’ questions
Example – For off-campus clinics, do you have an EMTALA
policy approved by the hospital board?
• Often additional documentation is required.
Example – Organizational charts showing reporting
relationships in order to verify that the given operation is truly
a part of the hospital.
• Special Efforts May be Necessary
Example – Providing photographs of the signage at off-campus
clinics.
• Exercise – Discuss what would be required to file attestations for
the Apex Medical Center if there were five different clinics being
established or converted. Assume that all are off-campus.
Provider-Based Rule: Advanced Topics March 5, 2015
Florida Hospital Association 21
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 41
Case Study/Exercise – HBO Clinic - The Apex Medical Center has
contracted with an outside company to provide Hyperbaric Oxygen (HBO)
services. AMC is providing space in a building several blocks from the
hospital. The outside company is providing the equipment, supplies, a
physician, nursing and technical staff. Apex is providing clerical staff for
registration, billing, etc. Apex pays the outside company for the services,
and then Apex files claims with third-party payers including Medicare.
How does the Provider-Base Rule come into play in this situation?
Are there any supervisory issues?
Provider-Based Clinics - Advanced
Under Arrangements
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 42
Provider-Based Clinics - Advanced
3-Day Pre-Admission Window
Case Study/Exercise – The Apex Medical Center has more than a dozen
provider-based clinics. There is one outlying clinic where many
complaints have been made concerning the two co-payments. Thus, Apex
is now studying moving this particular clinic back to freestanding, that is,
wholly owned freestanding.
Discuss this overall process and include any concerns about the 3-Day
Pre-Admission Window.
Provider-Based Rule: Advanced Topics March 5, 2015
Florida Hospital Association 22
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 43
Provider-Based Clinics - Advanced
The Future of Provider-Based Clinics
Will the increased overall payment for provider-based clinics continue on
into the future?
OIG – Wants the payment differential done away; payment should be
the same for freestanding clinics as for provider-based clinics.
MedPAC – Recommendation to eliminate payment differential for E/M
services.
CMS Comments from December 10, 2013 Federal Register:
“We stated in the CY 2014 OPPS/ASC and MPFS proposed rules that in
order to better understand the growing trend toward hospital
acquisition of physician offices and subsequent treatment of those
locations as off-campus provider-based outpatient departments, we
were considering collecting information that would allow us to analyze
the frequency, type, and payment of services furnished in off-campus
provider-based hospital departments.” (Page 761 CMS-1601-FC)
• Potential Methods for Data
New POS for Off-Campus Provider-Based Clinics
HCPCS Modifier to Indicate Provider-Based Clinic (PO Modifier)
Separate Cost Center on Hospital Cost Report
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 44
Provider-Based Clinics - Advanced
Summary & Conclusions
Understand The Terminology and Concepts
Freestanding Clinic
Provider-Based Clinic
Significant Economic Advantage To Hospitals That Own and Operate
Clinics To Make Them Provider-Based
Medicare Site-of-Service Differential Concept – Physician Payment
Reduction – No Overhead
Physician Reduction More Than Made Up By Technical Component
Payment, That Is APCs
Cost-Benefit Analysis
• Tangibles versus Intangibles
• Properly Assessing Costs
Operational Challenges
Proper Place of Service (POS) Coding Is Critical
Chargemaster Setup
Form Follow Function
Professional vs. Technical Component Coding
E/M Levels Along With Surgical/Medical Services
Split Billing Issues – Establishing a Proper Fee Schedule

Provider-Based Rule: Advanced Topics March 5, 2015
Florida Hospital Association 23
© 1996-2015 Abbey & Abbey, Consultants, Inc. Slide # 45
Provider-Based Rules and Regulations Application/Approval versus Attestation Process Provider-Based Services versus Provider-Based Clinical Services
• Provider-Based Clinics – Separately Recognizable• Provider-Based Clinical Services – Generally On An Ad Hoc Basis –
Generally Not Separately Recognizable Units• Economic Advantages
Obligations Prohibitions Reporting – Material Changes Planning – Payment Differential Will Probably Be Available For 5 to 7
Years (?) – It will be phased out over time although the increased payments are continuing for the time being.
There Are A Number Of Special Situations and Concerns Other Issues
EMTALA Interface for Off-Campus Provider-Based Clinics Physician Supervision Requirements – See Provider-Based
Departments Medicare Enrollment–CMS-855-A, 855-B, 855-I, 855-R, and maybe 855-O
• See Also NPIs and TIN Issues Non-Physician Practitioners Issues 3-Day Payment Window
Provider-Based Clinics - Advanced
Summary & Conclusion