eradication of epidemic methicillin-gentamicin-resistant staphylococcus aureus in an intensive care...
TRANSCRIPT

Eradication of Epidemic Methicillin-Gentamicin- Resistant Staphylococcus aureus in an Intensive Care Nursery
LISA M. DLJNKLE. M.D. SHEHLA H. NAQVI, M.B.. B.S. ROSE McCALLIJM R.N. J, P. LOFGREN. M.D.
St. louis. Missouri
A methicillin-resistant strain of Staphylococcus aureus (phage type 47,54,75,83A] became epidemic in our 50 bed level III nursery, with a colonization rate of 70 percent and an infection rate of more than 25 percent. This prevalence and the appearance of gentamicin re- sistance necessitated epidemic control measures. Standard measures included separate housing for infants in whom colonization had occurred and infants in whom it had not, low nurse to patient ratios, and cohorting of all personnel. Use of all antibiotics was curtailed by the requirement of infectious disease consultation. Gentamicin was available only on order of the Director.
The colonization rate fell from 55 percent to 25.4 percent, the first-week colonization rate from 31 percent to 0 percent, and the infection rate from 29.3 percent to 15.9 percent over eight weeks. The mean duration of antibiotic therapy decreased from 12.21 to 9.05 days per treated patient; however, the frequency of gentamicin usage and the proportion of gentamicin resistance were unchanged. Nurse to patient ratios were modified to allow increased admissions, but co- horting was continued for 12 weeks until all infants in whom colo- nization had occurred were discharged. With the elimination of the reservoir, no further colonization occurred and antibiotic resistance did not wappear.
Standard infection control measures can eliminate epidemics of multiple antibiotic-resistant Staph. aureus, and control of antibiotic usage may prevent re-emergence of resistant strains.
Antibiotic-resistant bacteria have become a serious epidemiologic problem over the last half decade and cause considerable morbidity via nosocomial infections. Methicillin and gentamicin-resistant strains of Staphylococcus aureus have emerged as major nosocomial patho- gens nationwide [l-4].
From the Division of Infectious Diseases and Hospital Epidemiology, Department of Pediat- tics, St. l.~~~is University School of Medicine and the Cardinal Glennon Memorial Hospital for Children. St. Louis, Section for Disease Control. Missouri Division of Health. jefferson City, Missouri. This study was presented at the 2nd International Conference on Nosocomial In- fections, held August 5-8. 1980, in Atlanta, Georgia. Requests for reprints should be ad- dressed lo Dr. Lisa M. Dunkle, 1465 South Grand Boulevard, St. Louis, MO 63104.
Resistance to methicillin and numerous other antibiotics, including aminoglycosides, has been shown to be plasmid-mediated, and transfer of resistance plasmids between strains and species of staphylococci has been carried out under laboratory conditions [5]. Plasmid transfer in the clinical situation has been suggested by laboratory studies and by epidemiologic observations. The presence of antibiotics appears to be necessary to the maintenance of resistance plasmids under clinical conditions [S].
A methicillin-resistant strain of Staph. aureus, phage type 47, 54,75,63A, became endemic in our 50 bed level III nursery in 1977. The susceptibility pattern of this organism showed resistance to ampicillin,
February 1961 The American Journal of Medicine Volume 70 455
METHICILLIN-GENTAMICIN-RESISTANT STAPH. ALJREUS IN NURSERY-DIJNKLE ET AL
3 West tuncobnizadl 0
3 East Kolonlzed) Cl
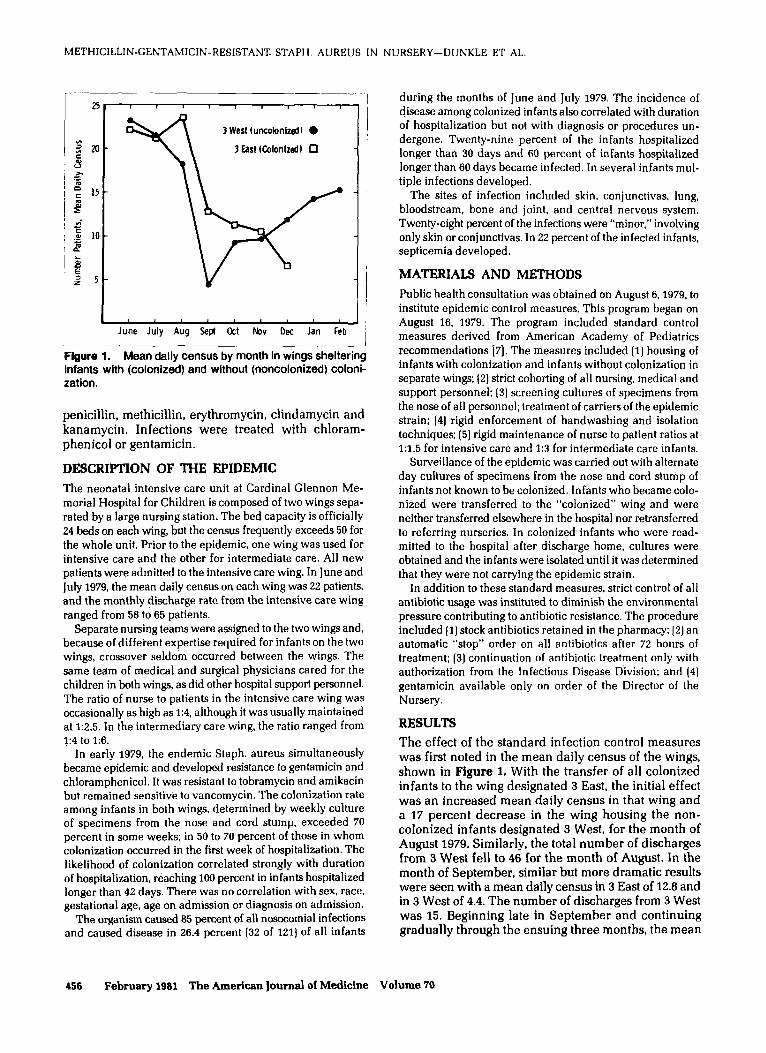
June July Aug Sept &t Nov Dee Jan Feb __.. Figure 1. Mean daily census by month in wings sheltering infants with (colonized) and without (noncolonized) coloni- zation.
penicillin, methicillin, erythromycin, clindamycin and kanamycin. Infections were treated with chloram- phenicol or gentamicin.
DESCRIPTION OF THE EPIDEMIC
The neonatal intensive care unit at Cardinal Glennon Me- morial Hospital for Children is composed of two wings sepa- rated by a large nursing station. The bed capacity is officially 24 beds on each wing, but the census frequently exceeds 50 for the whole unit. Prior to the epidemic, one wing was used for intensive care and the other for intermediate care. All new patients were admitted to the intensive care wing. In June and July 1979, the mean daily census on each wing was 22 patients, and the monthly discharge rate from the intensive care wing ranged from 58 to 65 patients.
Separate nursing teams were assigned to the two wings and, because of diffeient expertise required for infants on the two wings, crossover seldom occurred between the wings. The same team of medical and surgical physicians cared for the children in both wings, as did other hospital support personnel. The ratio of nurse to patients in the intensive care wing was occasionally as high as 1:4, although it was usually maintained at 1:2.5. In the intermediary care wing, the ratio ranged from I:4 to 1:6.
In early 1979, the endemic Staph. aureus simultaneously became epidemic and developed resistance to gentamicin and chloramphenicol. It was resistant to tobramycin and amikacin but remained sensitiv’e to vancomycin. The colonization rate among infants in both wings, determined by weekly culture of specimens from the nose and cord stump, exceeded 70 percent in some weeks; in 50 to 70 percent of those in whom colonization occurred in the first week of hospitalization. The likelihood of colonization correlated strongly with duration of hospitalization, reaching IOO percent in infants hospitalized longer than 42 days. There was no correlation with sex, race, gestational age, age on admission or diagnosis on admission.
The organism caused 85 percent of all nosocomial infections and caused disease in 26.4 percent (32 of 121) of all infants
456 February 1961 The American Journal of Medicine Volume 70
during the months of June and July 1979. The incidence of disease among colonized infants also correlated with duration of hospitalization but not with diagnosis or procedures un- dergone. Twenty-nine percent of the infants hospitalized longer than 30 days and 60 percent of infants hospitalized longer than 60 days became infected. In several infants mul- tiple infections developed.
The sites of infection included skin, conjunctivas. lung, bloodstream, bone and joint, and central nervous system. Twenty-eight percent of the infections were “minor,” involving only skin or conJunctivas. In 22 percent of the infected infants. septicemia developed.
MATERIALS AND METHODS
Public health consultation was obtained on August 6.1979. to institute epidemic control measures. This program began on August 16, 1979. The program included standard control measures derived from American Academy of Pediatrics recommendations 17). The measures included (1) housing of infants with colonization and infants without colonization in separate wings: (2) strict cohorting of all nursing, medical and support personnel: (3) screening cultures of specimens from the nose of all personnel; treatment of carriers of the epidemic strain; (41 rigid enforcement of handwashing and isolation techniques: (51 rigid maintenance of nurse to patient ratios at l:l.5 for intensive care and 1:3 for intermediate care infants.
Surveillance of the epidemic was carried out with alternate day cultures of specimens from the nose and cord stunip of infants not known to be colonized. Infants who became colo- nized were transferred to the “colonized” wing and were neither transferred elsewhere in the hospital nor retransferred to referring nurseries. In colonized infants who were read- mitted to the hospital after discharge home, cultures were obtained and the infants were isolated until it was determined that they were not carrying the epidemic strain.
In addition to these standard measures. strict control of all antibiotic usage was instituted to diminish the environmental pressure contributing to antibiotic resistance. The procedure included (I) stock antibiotics retained in the pharmacy; 12) an automatic “stop” order on all antibiotics after 72 hours of treatment; (3) continuation of antibiotic treatment only with authorization from the Infectious Disease Division; and (41 gentamicin available only on order of the Director of the Nursery.
RESULTS
The effect of the standard infection control measures was first noted in the mean daily census of the wings, shown in Figure 1. With the transfer of all colonized infants to the wing designated 3 East, the initial effect was an increased mean daily census in that wing and a 17 percent decrease in the wing housing the non- colonized infants designated 3 West, for the month of August 1979. Similarly, the total number of discharges from 3 West fell to 46 for the month of August. In the month of September, similar but more dramatic results were seen with a mean daily census in 3 East of 12.8 and in 3 West of 4.4. The number of discharges from 3 West was 15. Beginning late in September and continuing gradually through the ensuing three months, the mean
METHICILLIN-GENTAMICIN-RESISTANT STAPH. AUREUS IN NURSERY-DIJNKLE ET AL.
daily census in the wing housing the colonized infants
gradually fell to 6.7 in December and the mean daily census in 3 West (the wing housing the noncolonized infants) gradually increased to 11.96.
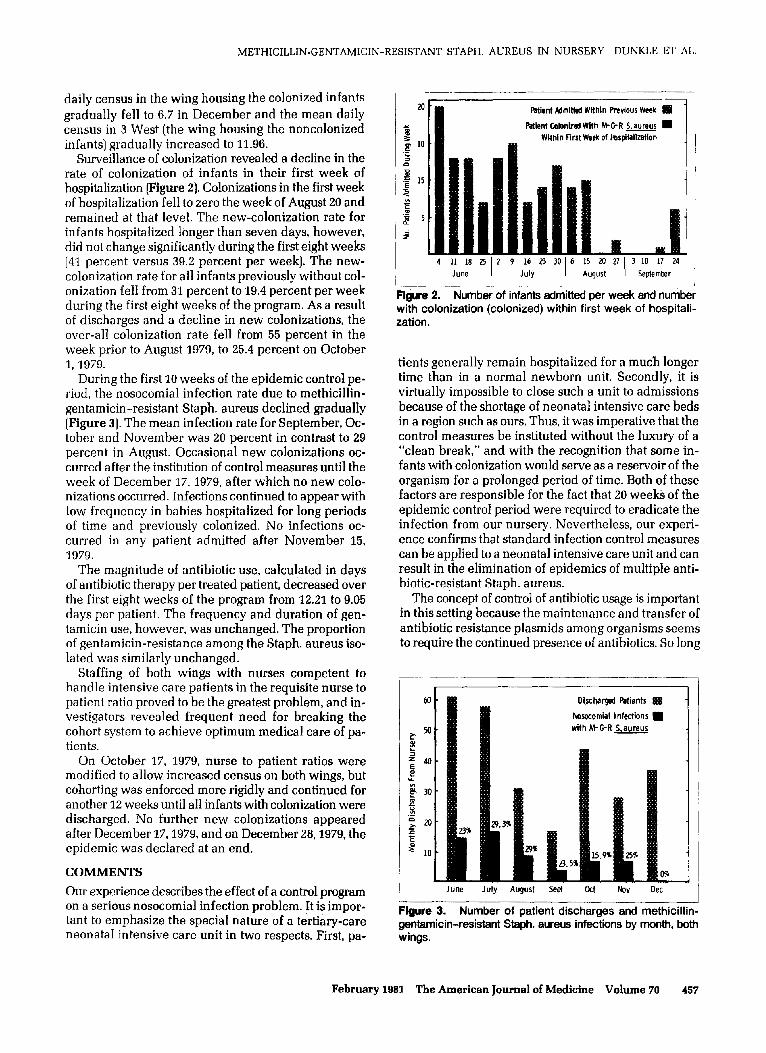
Surveillance of colonization revealed a decline in the rate of colonization of infants in their first week of hospitalization [Figure 2). Colonizations in the first week of hospitalization fell to zero the week of August 20 and remained at that level. The new-colonization rate for infants hospitalized longer than seven days, however, did not change significantly during the first eight weeks (41 percent versus 39.2 percent per week). The new- colonization rate for all infants previously without col- onization fell from 31 percent to 19.4 percent per week during the first eight weeks of the program. As a result of discharges and a decline in new colonizations, the over-all colonization rate fell from 55 percent in the week prior to August 1979, to 25.4 percent on October 1, 1979.
During the first 10 weeks of the epidemic control pe- riod, the nosocomial infection rate due to methicillin- gentamicin-resistant Staph. aureus declined gradually (Figure 3). The mean infection rate for September, Oc- tober and November was 20 percent in contrast to 29 percent in August. Occasional new colonizations oc- curred after the institution of control measures until the week of December 17,1979, after which no new cola- nizations occurred. Infections continued to appear with low frequency in babies hospitalized for long periods of time and previously colonized. No infections oc- curred in any patient admitted after November IS, 1979.
The magnitude of antibiotic use, calculated in days of antibiotic therapy per treated patient, decreased over the first eight weeks of the program from 12.21 to 9.05 days per patient. The frequency and duration of gen- tamicin use, however, was unchanged. The proportion of gentamicin-resistance among the Staph. aureus iso- lated was similarly unchanged.
Staffing of both wings with nurses competent to handle intensive care patients in the requisite nurse to patient ratio proved to be the greatest problem, and in- vestigators revealed frequent need for breaking the cohort system to achieve optimum medical care of pa- tients.
On October 17, 1979, nurse to patient ratios were modified to allow increased census on both wings, but cohorting was enforced more rigidly and continued for another 12 weeks until all infants with colonization were discharged. No further new colonizations appeared after December 17,1979, and on December 28,1979, the epidemic was declared at an end.
COMMENTS
Our experience describes the effect of a control program on a serious nosocomial infection problem. It is impor- tant to emphasize the special nature of a tertiary-care neonatal intensive care unit in two respects. First, pa-
m Patient Wmitted Within Previous Week m
f Patient Colonired With M-eR 5 aureus m i 1 s 01 10
WithIn First Week of tbspitaiization .S 5 0
.E
5
15
3 5
‘G d 5
9
4 11 18 25 1 2 9 16 23 30 1 4 15 20 27 1 3 10 it 24 June 1 July 1 August 1 September
Figure 2. Number of infants admitted per week and number with colonization (colonized) within first week of hospitali- zation.
tients generally remain hospitalized for a much longer time than in a normal newborn unit. Secondly, it is virtually impossible to close such a unit to admissions because of the shortage of neonatal intensi.ve care beds in a region such as ours. Thus, it was imperative that the control measures be instituted without the luxury of a “clean break,” and with the recognition that some in- fants with colonization would serve as a reservoir of the organism for a prolonged period of time. Both of these factors are responsible for the fact that 20 weeks of the epidemic control period were required to eradicate the infection from our nursery. Nevertheless, our experi- ence confirms that standard infection control measures can be applied to a neonatal intensive care unit and can result in the elimination of epidemics of multiple anti- biotic-resistant Staph. aureus.
The concept of control of antibiotic usage is important in this setting because the maintenance and transfer of antibiotic resistance plasmids among organisms seems to require the continued presence of antibiotics. So long
Dbcharged Pdtients 888
bocomial infections m with M-G-R 5 aureus -
June July August Se@ Ott Nov OK
-l_ll
Figure 3. Number of patient discharges and methicillin- gentamicin-resistant Staph. aureus infections by month, both wings.
February 1981 The American Journal of Medicine Volume 70 457

METHICILLIN-GENTAMICIN-RESISTANT STAPH. AUREUS IN NURSERY-DUNKLE ET AL.
as infections continued to occur and a small number of patients required long-term treatment with gentamicin, the prevalence of this drug in the environment was unchanged. Furthermore, as gentamicin continued to be used in either wing, reversion to gentamicin-sensi- tivity did not occur. However, with the elimination of the reservoir of the organism by discharge of the colo- nized patients, even with the continued presence of gentamicin in the wing housing the uncolonized pa- tients, gentamicin resistance did not reappear.
We conclude that the susceptibility pattern of an ep- idemic Staph. aureus is unlikely to change during an epidemic control period but that the control of antibiotic
use may be useful in preventing re-emergence of re- sistant strains after the epidemic is eradicated.
ACKNOWLEDGMENT
We wish to thank Dr. Dennis M. O’Connor and Mr. Lua Blankenship for the administrative support without which this program could not have been carried out, and the staff of the Pharmacy of Cardinal Glennon Memo- rial Hospital for Children for their assistance with the program. We also wish to acknowledge the assistance of Cynthia A. Slaten, R.N. in the completion of the epi- demic control period and Mrs. Ellen George in prepa- ration of the manuscript.
REFERENCES
Bint AJ, George RH, Healing DE, Wise R, Davies M: An out-
yIococcus aureus. J Chn Pathor1977; 30: 185-187. break of infection caused by a gentamicin resistant Staph-
Lewis SA, Altemier WA: Emergence of clinical isolates of Staphylococcus aureus resistant to gentamicin and corre- lation of resistance with bacteriophage type. J Infect Dis 1978: 137: 314-317.
5.
infections with emergence of gentamicin-methicillin re- sistant strains. Infection Control 1980: 1: 81-89.
Jaffe HW, Sweeney HM. Nathan C, et ai.: Identify and inter- specific transfer of gentamicin-resistant plasmids in Staphylococcus aureus and Staphylococcus epidermidis. J Infect Dis 1980; 141: 738-747.
6. Franc0 IA. Eitzman DV. Baer H: Antibiotic usaee and micro- Crossley K. Loesch D, Landesman B, Mead K, Chern M, Strate
R: An outbreak of infections caused by strains of Staphylo- coccus aureus resistant to methicillin and aminoglycosides. J Infect Dis 1979; 139: 273-287.
bial resistance in an intensive care nursery.im J Dis Child 1973; 126: 318-321.
Saroglou G, Cromer M, Bisno AL: Methicillin-resistant Staphylococcus aureus: interstate spread of nosocomial
7. Committee on Fetus and Newborn: Control of infection in standards and recommendations for hospital care of new- born infants. Evanston, III.: American Academy of Pediatrics 1977; 109-129.
458 February 1981 The American Journal of Medicine Volume 70