epithelialization of the corneal endothelium in posterior...
TRANSCRIPT

832 ReportsInvest. Ophthalmol. Vis. Set.
July 1980
tested. This is consistent with results reported byKaye et al.,6 who found no changes in rabbit en-dothelium exposed to pressures of 60 to 80 mm Hg.
This study demonstrates that rabbit corneal en-dothelium functions normally in the presence ofshort-term hydrostatic pressure increases between15 to 50 mm Hg. Regenerated rabbit endotheliumfunctions similarly to normal endothelium in thepresence of elevated hydrostatic pressure.
From the Departments of Ophthalmology and Physi-ology, The Medical College of Wisconsin, and WoodVeterans Administration Medical Center, Milwaukee,Wise. This investigation was supported in part by NEIresearch grant EY-01436, research center grant EY-01931, medical research funds from the Veterans Admin-istration, and an unrestricted grant from Research toPrevent Blindness. Submitted for publication Dec. 17,1979. Reprint requests: D. L. Van Horn, Ph.D., Re-search Service/151, Veterans Administration MedicalCenter, Wood (Milwaukee), Wise. 53193.
Key words: cornea, corneal endothelium, intraocularpressure, rabbit
REFERENCES1. Edelhauser HF, Van Horn DL, Hyndiuk RA, and
Schultz RO: Intraocular irrigating solutions: their ef-fect on the corneal endothelium. Arch Ophthalmol94:648, 1975.
2. Coles WH: Pilocarpine toxicity. Effects on the rabbitcorneal endothelium. Arch Ophthalmol 93:36, 1975.
3. Bowman KA and Green K: Hydrostatic pressure ef-fects on deswelling of de-epithelialized and de-endothelialized corneas. INVEST OPHTHALMOL 15:546,
1976.4. Hodson S: The regulation of corneal hydration by a
salt pump requiring the presence of sodium and bi-carbonate ions. J Physiol 221:29, 1974.
5. Svedbergh G: Effects of artificial intraocular pressureelevation on the corneal endothelium in the vervetmonkey (Cercopithecus ethiops). Acta Ophthalmol53:839, 1975.
6. Kaye GI, Sibley RC, and Hoefle FB: Recent studieson the nature and function of the corneal endothelialbarrier. Exp Eye Res 15:585, 1973.
7. Van Horn DL, Sendele DD, Seideman S, and BucoPJ: Regenerative capacity of the corneal endotheliumin rabbit and cat. INVEST OPHTHALMOL Vis Sci 16:597,
1977.
Epithelialization of the corneal endotheliumin posterior polymorphous dystrophy.MERLYN M. RODRIGUES, TUNG-TIEN SUN, JAY
KRACHMER, AND DAVID NEWSOME.
The unusual cell type present on the posterior cornealsurface of posterior polymorphous dystrophy patients
has been characterized. In addition to microvilli anddesmosomes, these cells contain abundant 10 nm fila-ments which by immunofluorescent staining were shownto consist of keratin proteins, a marker for epithelialcells.
Posterior polymorphous dystrophy (PPMD) ofthe cornea is a disorder of the corneal endotheliumusually associated with autosomal dominant in-heritance.1 Clinically this entity is characterizedby bilateral involvement of the posterior cornea.Lesions can range from tiny vesicular areas,thickening, and bands to advanced posterior cor-neal changes with secondary stromal and epithel-ial edema, necessitating corneal transplantation.Congenital posterior corneal vesicles have beenobserved in offspring of families with this condi-tion.1 Histologically PPMD is associated with ir-regular multilaminar Descemet's membrane whichdisplays normal anterior banding as well as ab-normal cells present in the endothelial layer.2"5
Recently it has been shown that keratin proteinsare present in the form of tonofilaments not only inepidermal cells but also in corneal epithelial and awide variety of other epithelial cells.6"8 Of particu-lar interest is the fact that when frozen sections ofcornea were stained with antikeratin antiserum byindirect immunofluorescent staining, it was foundthat corneal epithelium was the only cell type thatstained; no staining could be detected in thestroma or endothelium." We now report that theunusual epithelial-like cells in the corneal endo-thelial layer in PPMD can be stained specificallywith antikeratin antiserum and thus that they con-tain keratin filaments, a marker for epithelialcells.6"8
Materials and methods. Antibodies preparedagainst a group of keratins purified from humanstratum corneum8' 9 were used to identify epithe-lial cells containing keratins by immunofluores-cence.10 The antiserum against the keratin fractionwas characterized by immunoelectrophoresis withsodium dodecyl sulfate slab gel and contained an-tibodies against all the major electrophoreticbands of keratins.10 For immunofluorescent stain-ing,6 frozen sections (6 pm thick) were prepared.The air-dried tissue sections were hydrated inphosphate-buffered saline (PBS) and covered with20 fx\ of antikeratin antiserum previously diluted1:48 with PBS. The sections were incubated in ahumidified chamber at 37° C for 30 min. Theywere then washed in three changes of PBS for atotal of 30 min, overlaid with fluorescein-conjugated goat anti-rabbit IgG (1:16 diluted;Miles Laboratories, Inc.) and incubated at 37° C for30 min. After they were rinsed again, these speci-
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933324/ on 06/20/2018
Volume 19Number 7 Reports 833
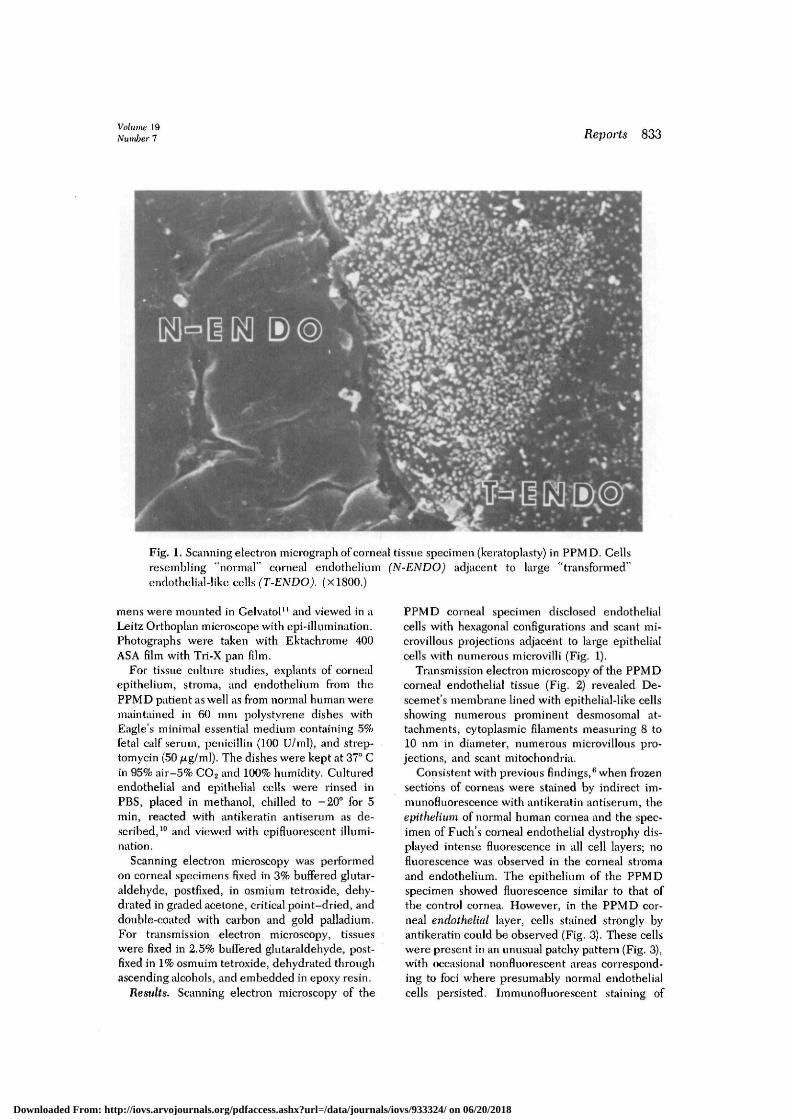
Fig. 1. Scanning electron micrograph ofcorneal tissue specimen (keratoplasty) in PPMD. Cellsresembling "normal" corneal endothelium (N-ENDO) adjacent to large "transformed"endothelial-Iike cells (T-ENDO). (X1800.)
metis were mounted in Gelvatol11 and viewed in aLeitz Orthoplan microscope with epi-illumination.Photographs were taken with Ektachrome 400ASA film with Tii-X pan film.
For tissue culture studies, explants of cornealepithelium, stroma, and endothelium from thePPMD patient as well as from normal human weremaintained in 60 mm polystyrene dishes withEagle's minimal essential medium containing 5%fetal calf serum, penicillin (100 U/ml), and strep-tomycin (50 /Ltg/ml). The dishes were kept at 37° Cin 95% air-5% CO2 and 100% humidity. Culturedendothelial and epithelial cells were rinsed inPBS, placed in methanol, chilled to -20° for 5min, reacted with antikeratin antiserum as de-scribed,10 and viewed with epifluorescent illumi-nation.
Scanning electron microscopy was performedon corneal specimens fixed in 3% buffered glutar-aldehyde, postfixed, in osmium tetroxide, dehy-drated in graded acetone, critical point-dried, anddouble-coated with carbon and gold palladium.For transmission electron microscopy, tissueswere fixed in 2.5% buffered glutaraldehyde, post-fixed in 1% osmuim tetroxide, dehydrated throughascending alcohols, and embedded in epoxy resin.
Results. Scanning election microscopy of the
PPMD corneal specimen disclosed endothelialcells with hexagonal configurations and scant mi-crovillous projections adjacent to large epithelialcells with numerous microvilli (Fig. 1).
Transmission electron microscopy of the PPMDcorneal endothelial tissue (Fig. 2) revealed De-scemet's membrane lined with epithelial-like cellsshowing numerous prominent desmosomal at-tachments, cytoplasmic filaments measuring 8 to10 nm in diameter, numerous microvillous pro-jections, and scant mitochondria.
Consistent with previous findings,6 when frozensections of corneas were stained by indirect im-munofluorescence with antikeratin antiserum, theepithelium of normal human cornea and the spec-imen of Fuch's corneal endothelial dystrophy dis-played intense fluorescence in all cell layers; nofluorescence was observed in the corneal stromaand endothelium. The epithelium of the PPMDspecimen showed fluorescence similar to that ofthe control cornea. However, in the PPMD cor-neal endothelial layer, cells stained strongly byantikeratin could be observed (Fig. 3). These cellswere present in an unusual patchy pattern (Fig. 3),with occasional nonfluorescent areas correspond-ing to foci where presumably normal endothelialcells persisted. Immunofluorescent staining of
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933324/ on 06/20/2018
834 Reports Invest. Ophthalmol. Vis. Sci.July 1980
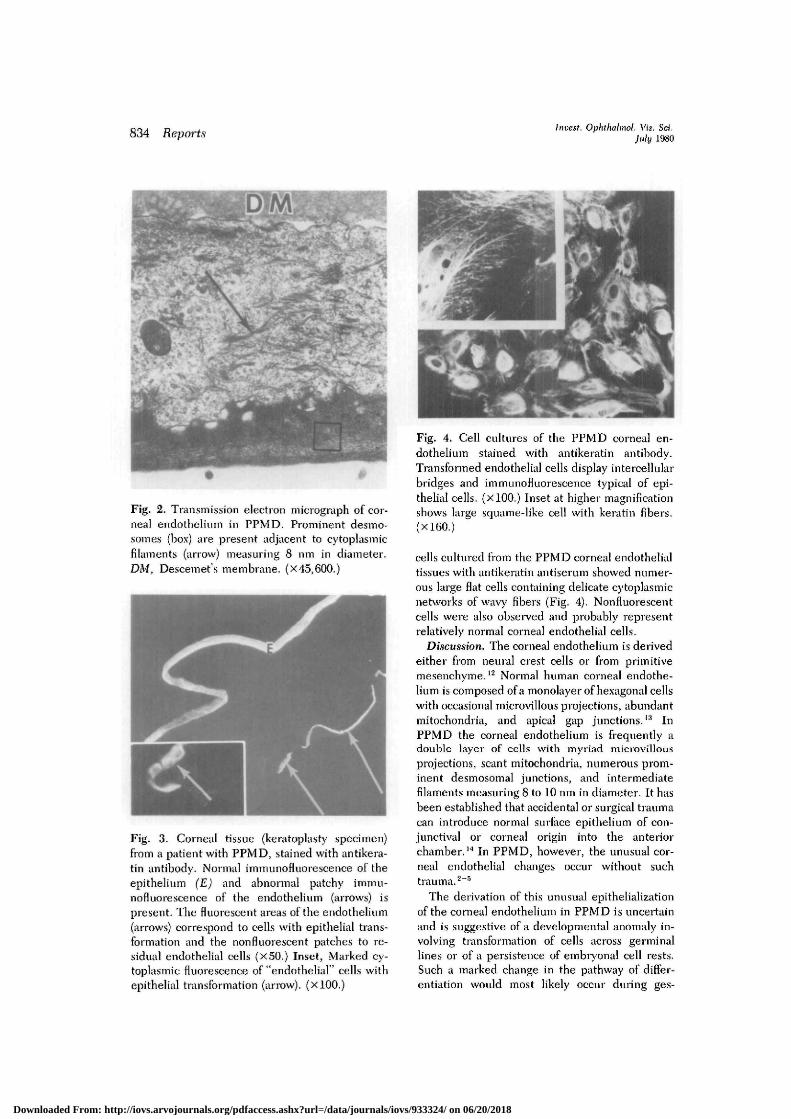
Fig, 2. Transmission election micrograph of cor-neal endothelium in PPMD. Prominent desmo-somes (box) are present adjacent to cytoplasmicfilaments (arrow) measuring 8 nm in diameter.DM, Descemet's membrane, (x 45,600.)
Fig. 3. Corneal tissue (keratoplasty specimen)from a patient with PPMD, stained with antikera-tin antibody. Normal immunofluorescence of theepithelium (E) and abnormal patchy immu-nofluorescence of the endothelium (arrows) ispresent. The fluorescent areas of the endothelium(arrows) correspond to cells with epithelial trans-formation and the nonfluorescent patches to re-sidual endothelial cells (X50.) Inset, Marked cy-toplasmic fluorescence of "endothelial" cells withepithelial transformation (arrow). (xlOO.)
Fig. 4. Cell cultures of the PPMD corneal en-dothelium stained with antikeratin antibody.Transformed endothelial cells display intercellularbridges and immunofluorescence typical of epi-thelial cells. (XlOO.) Inset at higher magnificationshows large squume-like cell with keratin fibers.(X160.)
cells cultured from the PPMD corneal endothelialtissues with antikeratin antiserum showed numer-ous large flat cells containing delicate cytoplasmicnetworks of wavy fibers (Fig. 4). Nonfluorescentcells were also observed and probably repiesentrelatively normal corneal endothelial cells.
Discussion. The corneal endothelium is derivedeither from neural crest cells or from primitivemesenchyme.12 Normal human corneal endothe-lium is composed of a monolayer of hexagonal cellswith occasional microvillous projections, abundantmitochondria, and apical gap junctions.13 InPPMD the corneal endothelium is frequently adouble layer of cells with myriad microvillousprojections, scant mitochondria, numerous prom-inent desmosomal junctions, and intermediatefilaments measuring 8 to 10 nm in diameter. It hasbeen established that accidental or surgical traumacan introduce normal surface epithelium of con-junctival or corneal origin into the anteriorchamber.14 In PPMD, however, the unusual cor-neal endothelial changes occur without suchtrauma.2"5
The derivation of this unusual epithelializationof the corneal endothelium in PPMD is uncertainand is suggestive of a developmental anomaly in-volving transformation of cells across germinallines or of a persistence of embryonal cell rests.Such a marked change in the pathway of differ-entiation would most likely occur during ges-
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933324/ on 06/20/2018

Volume 19Number 7 Reports 835
tation2 and has been observed at birth.1 In
PPMD, Descemet's membrane displays anterior
banding, usually occurring during the fifth month
of gestation,2 but lack of a uniform posterior granu-
lar layer suggests intrauterine damage to the cor-
neal endothelium. If the abnormal corneal endo-
thelial cells were displaced ectodermal cells, they
would most likely have expressed their dysfunc-
tion at the same time as other derivatives of sur-
face ectoderm, which are unaffected in this dis-
ease. All these factors are consistent with a most
unusual transformation of corneal endothelial cells
into keratin-containing epithelial cells. We have
demonstrated that this change of cell type, an im-
portant feature of PPMD, distinguishes it from
normal human corneal endothelium and from
other disease of the corneal endothelium such as
Fuchs' dystrophy,
We thank Alfred J. Coulombre for his comments andPatricia Donohoo and Joseph Hackett for technical as-sistance.
From the Clinical Branch National Eye Institute (Dr.Rodrigues and Dr. Newsome), the Departments ofDermatology and of Cell Biology and Anatomy, JohnsHopkins University Medical School, Baltimore, Md (Dr.Sun), and the Corneal Service, Department of Ophthal-mology, University of Iowa Iowa City, Iowa (Dr. Krach-mer). Supported in part by NIH research grantsEY02472, AM25140, and AM21358 as well as ResearchCareer Development Aware EY00125 to Dr. Sun.Submitted for publication Nov. 26, 1979. Reprint re-quests: Merlyn M. Rodrigues, M.D., National Eye Insti-tute, National Institutes of Health, Bethesda, Md.20205.
Key words: posterior polymorphous corneal dystrophy,keratin, immunofluorescence, epithelialization
REFERENCES1. Cibis GW, Krachmer JH, Phelps CB, and Weingeist
TA: The clinical spectrum of posterior polymorph-ous dystrophy. Arch Ophthalmol 95:152, 1977.
2. Rodrigues MM, Waring GO, Laibson PR, andWeinreb S: Endothelial alterations in congenitalcorneal dystrophies. Am J Ophthalmol 80:687, 1975.
3. Grayson M: The nature of hereditary deep dys-trophy of the cornea: its association with iris and
anterior chamber dysgenesis. Trans Am OphthalmolSoc 72:516, 1974.
4. Tripathi RC, Casey TA, and Wise G: Hereditaryposterior polymorphous dystrophy: an ultrastruc-tural and clinical report. Trans Ophthalmol Soc UK94:211, 1974.
5. Boruchoflf A and Kuwabara T: Electron microscopyof posterior polymorphous degeneration. Am JOphthalmol 72:897, 1971.
6. Sun T-T, Shih C, and Green H: Keratin cytoskele-tons in epithelial cells of internal organs. Proc NatlAcad Sci USA 76:2813, 1979.
7. Franke WW, Schmid E, Osborn M, and Weber K:Different intermediate sized filaments distinguishedby immunofluorescence microscopy. Proc Natl AcadSci USA 75:5034, 1978.
8. Sun T-T and Green H: Cultured epithelial cells ofcornea, conjunctiva and skin: absence of marked in-trinsic divergence of their differentiated states. Na-ture 269:489, 1977.
9. Sun T-T and Green H.: The keratin filaments ofcultured human epidermal cells: formation of inter-molecular disulfide bonds during terminal differ-entiation. J Biol Chem 253:2053, 1978.
10. Sun T-T and Green H: Immunofluorescent stainingof keratin fibers in cultured cells. Cell 14:469, 1978.
11. Rodriguez, J and Dienhardt F: Preparation of asemipermanent mounting medium for fluorescentantibody studies. Virology 12:316, 1960.
12. Johnston M, Noden D, Hazelton R, Coulombre J,and Coulombre A: Origins of avion ocular andperiocular tissues. Exp Eye Res 29:27, 1979.
13. Hogan M, Alvarado J, and Weddell J: Histology ofthe Human Eye. An Atlas and Textbook. Philadel-phia, 1971, W. B. Saunders Co., pp. 102-108.
14. Yanoff M and Fine B: Ocular Pathology. A Text andAtlas. Hagerstown, Md., 1975, Harper & Row,Publishers, p. 132.
Concentration-dependent morphologic ef-fects of cytochalasin B in the aqueous out-flow system. MURRAY JOHNSTONE, DAWN
TANNER, BRUCE CHAU, AND KENNETH
KOPECKY.
Cytochalasin B at concentrations of 1, 5, 10, 15, 20, or40 fJLg/ml was continuously exchange-perfused into theeyes of nine living Macaca mulatta monkeys while in-traocular pressure (IOP) was maintained at 25 mm Hgfor 30 min. Pressures were then slowly reduced to 4 mmHg to permit blood to reflux into Schlemms canal as atracer, and the eyes were fixed while maintained at 4 mmHg IOP. Tissues were examined in all eyes by light andtransmission electron microscopy. At concentrations ofl,5, and 10 /xg/ml cytochalasin B, the integrity of the endo-thelial lining of the trabecular wall of Schlemms canalwas maintained. At 15 fig/ml cytochalasin B, 6% of thelength of the endothelial lining was disrupted; at 20fig/ml, 54%; and at 40 fxghnl, 83%. There was a washoutof extracellular material at the site of breaks and also areflux of blood from Schlemms canal into the trabecular7neshwork in the same regions.
Intracameral infusion of cytochalasin B (CB)
causes a large increase in gross outflow facility in
the cynomolgus monkey.1 Since ruptures in the
endothelial lining of the inner wall of Schlemms
0146-0404/80/070835+07$00.70/0 © 1980 Assoc. for Res. in Vis. and Ophthal., Inc.
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933324/ on 06/20/2018