epilepsy post graduate medi
TRANSCRIPT
EpilepsyPost graduate medicine Jan 2002
What is epilepsy Occurance of two or more unprovoked seizures is
called epilepsy Epileptic seizures are behavioral changes resulting
from paroxysmal, excessive discharges from brain Single or occasional epileptic seizures or febrile fits
should not be classified as epilepsy Not all jerks , shakes and episodic behaviors are
seizures Tics, tremors, dystonias and sustained clonus in a
stroke pt may mimic epilepsy
Non epileptic paroxysmal dissorders that can mimic epilepsy Syncope
Reflex(vasovagal, carotid sinus, glossopharyngeal, cough)
cardiac output Decreased LV filling
(hypovolumia, orthostatic hypotensio, PE)
Cardiac arrhythmias Migraine (classic, basillar and
confusional) Cerebrovascular event (TIA) Periodic paralysis Sleep dissorders
GI disorders (Reflux, motility disorders)
Movement disorders Tics Tourette’s synd Non epileptic myoclonus Parox. Choreoathetosis
Psychiatric disorders Panic Somatization Dissociation
Conversion (non epileptic psychogenic fits)
Drug toxicity et subs abuse Breath holding spells
Non epileptic psychogenic seizure How to differentiate
Cannot reliably differrentiate Gradual onset Stopping & restarting Out of phase clonic movements of extremities Vocalization in the middle of the seizure Pelvic thrusting and lack of whole body rigidity
But frontal lobe cpx seizures may be misdiagnosed (rocking, kicking, bicycling, pelvic thrusting, genital manipulat ion and cursing)
Aetiology Unknown in 2/3rd
Head injury Stroke Brain tumor Cortical dysplasia Infection eg:neurocysticercosis Alcohol related
Diagnostic workup Firist diagnose seizure Then determine
Seizure type Syndromic classification Etiology Likelyhood of recurrence Is treatment needed
Diagnostic workup History taking Physical examination Neurological examination Diagnostic testing
Establishing the diagnosis Is a paroxysmal event with impairement of
awareness Diagnosis is clinical Eye witness is very essential There is no substitute for detailed Hx
Circumstance of the episode Patterns of occurance Preceding symptoms that may localise or suggest other
conditions Timing, pattern and tempo of evolution of symptoms Reported behaviour before, during and after the
event
History- before the event
Unusual stress (eg, severe emotional trauma)Sleep deprivationRecent illnessUnusual stimuli (eg, flickering lights)Use of medications and drugsActivity immediately before event (eg, change in posture, exercise)
History during the event Symptoms at onset (eg, aura)
Temporal mode of onset: gradual versus suddenDuration: brief (ictal phase <5 min) versus prolongedStereotypy: duration and features of episodes nearly identical versus frequently changingTime of day: related to sleep or occuring on awakening
History during the event Ability to talk and respond appropriately
Ability to comprehendAbility to recall events during the seizureAbnormal movements of the eyes, mouth, face, head, arms, and legsBowel or bladder incontinenceBodily injury
History after the event Confusion
LethargyAbnormal speechFocal weakness or sensory loss (ie, Todd's paralysis)Headache, muscle soreness, or physical injury
Episode is more likely to be syncopal if Is precipitated by anxiety or pain (eg, venipuncture) Occurs after the patient assumes an upright position Occurs only when the patient is standing or sitting Is associated with facial pallor and diaphoresis Is not associated with sustained tonic or clonic
movements, bladder incontinence, or biting of the tongue or cheek
Is not followed by postictal confusion, lethargy, muscle soreness, and headache
Is followed by a relatively rapid return to baseline
Past medical history Prolonged febrile fit Meningitis Encephalitis Head injury Cancer Stroke In diabetic pts hypo/hyperglycemia Hyponatremia, hypocalcemia, hypo
parathyroidism and hypothyroidism can cause fits
Drug history Theophyllin INAH Phenothiazine Clozapine Radiocontrast dye Alkylating agents Beta lactam antibiotics Others : lignocain, general anesthetics,
Tricyclics, SSRI, Acyclovir, beta blockers, decongestants, ectasy(MDMA)
Physical examination Examine the patient for injuries from the seizure or
fall. Check oxygen saturation and auscultate the chest for
possible aspiration. Measure heart rhythm and rate, blood pressure, and
orthostatic changes for assessment of syncope. Auscultate for carotid murmurs or carotid bruits and
sources of embolic stroke. Check for rapid pulses, which are often present after
seizure and may help in evaluation of psychogenic seizures.
Neurological examination Purpose is to identify focal or diffuse cerebral
dysfunction Certain features will suggest focus of fit
Aphasia – frontal lobe, temporal or parietal Right or left hemiparesis – contralateral motor cortex Sensory deficit – parietal lobe dysfunction
Should be observed for Fluency of language Facial asymetry Gaze preference Pupilary asymetry (Herniation of brain)
Extensor plantar for some time - normal
Diagnostic testing All pts should have
FBC Ca, SE Glucose LFT ECG – important to detect prolonged QT
(Morning generalised tonic clonic seizure)
Diagnostic testing Toxicity screening and alcohol level in
appropriate pts Lumbar puncture infection or fever
present, HIV or malignancy
Diagnostic testing -EEG Role misunderstood Detection of abnormality does not
equate epilepsy Absence of inter ictal abnormality does
not exclude epilepsy Only 1/3rd of epileptics show
abnormalities Ictal EEG could also be normal
Diagnostic testing -EEG EEG is diagnostic in certain conditions
Generalised 3Hz spike and wave activity-- 1ry generalised epilepsy
Ictal recordings are not routinely done except in incidental situations
EEG telemetry Ambualtory or video telemetry if
diagnosis remains in doubt Presurgical
Intracranial amytal testing to test memory and language function
Intracranial EEG to localise the focus
Imaging studies Immediately after fit CT scan– bleeding or
structural lesions MRI is the Ix of choice – sensitive & specific
for evaluation of structural lesions and brain parenchyma Mesial temporal sclerosis – hippocampus Dysplasia – cortical architectural abnormalities Better if could be done for all partial seizures Reveals abnormality in
30% with generalised epilepsy 70% with focal epilepsy
Detailed investigations Few pts will need
Hypoglycemia – early morning fits ECHO Ambulatory ECG Urinary catecholamines Porphyrins
Implications of diagnosis May loose job Life restricted Mental trauma Driving licence Marriage
So all differential diagnosis should be carefully considered
Classification Generalised
Arise from both sides of the brain simultaneously
Partial or focal Occurs within one or more restricted
regions of the brain and effect of a localised physiologic or structural abnormality of brain (Eg: tumor, dysplasia, stroke, trauma)
Classification Generalised
seizures Absence Atonic Myoclonic Clonic Tonic Tonic clonic (Grand
mal)
Partial Simple partial
consciousness not affected
Complex partialconsciousness
impaired Partial with 2ry
generalizationcan be tonic clonic,
tonic or clonic
When to treat Once diagnosed decide wether to treat or not Recurrece
After a single tonic clonic fit 15-60% After 2 fits – 85%
Probability of recurrence increases if Family history + Spike and wave pattern in EEG Hx of prior neurological insult Todd’s paralysis Status epilepticus Acute symp fit (occuring after brain insult)
First fit - to treat or not What is the risk of treating and non
treating What is the risk of recurrence Occupation- heavy vehicle drivers – yes In children – initial fit during sleep – no
need to treat Patients preference
Management - aim Prevent fits without causing adverse
effects Optimise patients quality of life Fits could be life threatening Pts with epilepsy are at risk of sudden
unexpected death (1/200/yr in refractory epilepsy)
Management - Principles Rx is usually not given after a single
unprovoked seizure, unless recurrence risk high
Avoid precipitating factors Identify underlying conditions and Rx Treatment strategies should be
explained to the pt
Management – Principles (Drugs) Choice – pts individual circumstance, syndrome and
side effect profile Low dose – slowly increase over weeks, minimising
side effects and promoting compliance If 1st line drug fails, add another 1st line drug while
gradually withdrawing the 1st drug If unsuccessful add 2nd line drug Vigabatrin and barbiturates should not be combined Refer refractory cases for evaluation for surgery
Monotherapy vs polytherapy 47% fit free with one drug 14% fit free with addition 2nd or 3rd drug If 2nd drug fails refer for evaluation of
surgery If not willing for surgery – consider
polytherapy
.
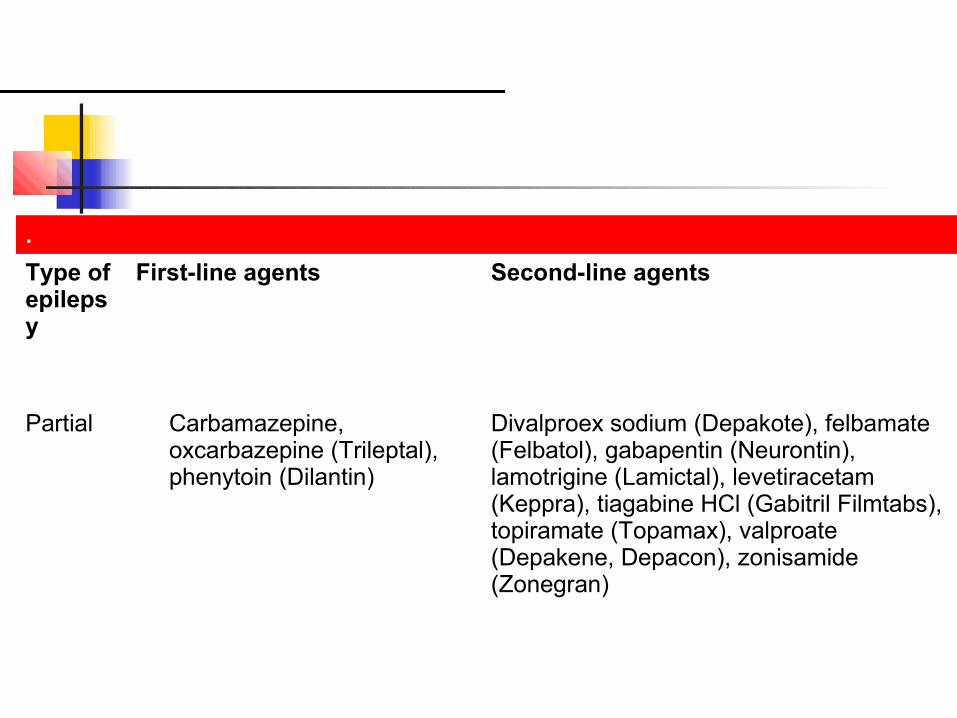
Type of epilepsy
First-line agents Second-line agents
Partial Carbamazepine, oxcarbazepine (Trileptal), phenytoin (Dilantin)
Divalproex sodium (Depakote), felbamate (Felbatol), gabapentin (Neurontin), lamotrigine (Lamictal), levetiracetam (Keppra), tiagabine HCl (Gabitril Filmtabs), topiramate (Topamax), valproate (Depakene, Depacon), zonisamide (Zonegran)
Init ial treatment for partial and general ized epilepsies
Init ial treatment for part ial and generalized epilepsies
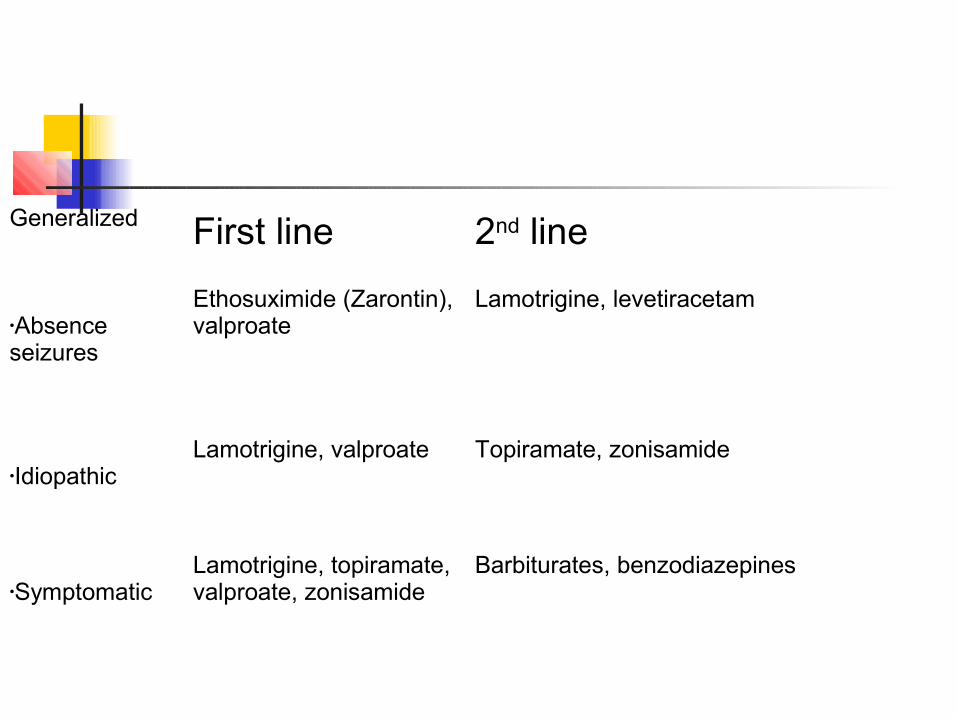
Generalized First line 2nd line
•Absence seizures
Ethosuximide (Zarontin), valproate
Lamotrigine, levetiracetam
•Idiopathic Lamotrigine, valproate Topiramate, zonisamide
•Symptomatic Lamotrigine, topiramate, valproate, zonisamide
Barbiturates, benzodiazepines
Seccond line drugs All of the newer AEDs, including
felbamate, gabapentin, lamotrigine, levetiracetam, oxcarbazepine, topiramate, tiagabine, and zonisamide, have demonstrated efficacy when used as adjunctive therapy in patients with poorly controlled seizures of partial onset
Seccond line drugs
Lamotrigine Could be used as 1st line
Gabapentin Safe, tolerable Monotherapy in liver disease, cutaneous
allergies, porphyria, immune deficiencies, elderly
Drug interactions
No interactionGabapentin (Neurontin)Levetiracetam (Keppra)
InducersCarbamazepinePhenobarbital (Bellatal, Luminal Sodium, Solfoton)Phenytoin (Dilantin)Primidone (Mysoline)
Drug interactions Inhibitors
Felbamate (Felbatol)Valproate (Depakene, Depacon)
Affected by enzyme-inducing drugsCarbamazepineFelbamateLamotrigine (Lamictal)Oxcarbazepine (Trileptal)PhenobarbitalPhenytoinPrimidoneTiagabine HCl (Gabitril Filmtabs)Topiramate (Topamax)ValproateZonisamide (Zonegran)
Healthcare issues for patients with epilepsy
Coping with the diagnosisObserving and recording seizuresIdentifying potential triggers and high-risk timesMaintaining personal safetyHandling seizure emergenciesManaging adverse drug effectsUnderstanding the nonmedical options for seizure management
Issues in social relationships and community living for patients with epilepsy
Personal adjustment to epilepsySexuality issuesEducation and employmentRecreational opportunitiesDisclosure of epilepsy to employersStigma and discriminationIndependent livingTransportationRespite care
Healthcare issues for patients with epilepsy
Managing concomitant illnessUnderstanding the relationship between seizures and hormonal statesPracticing family planningManaging pregnancy and menopauseMaintaining bone health
Withdrawl of treatment
>70% on Rx enter prolonged long term remission
Even untreated 50% undergo remission Why withdrawl
Side effects Social restrictions cost
Assess the patient Do a follow up EEG Counsel pt and family
Withdrawl of treatment Pts fit free for >2yrs to be considered 2/3rd are fit free Recurrences occur
50% within 6/12 Majority within 1 year
Surgical treatment Is not a recent development If refractory refer to specialist epilepsy
clinic for evaluation Prolonged video telemetry is the gold
standard for assesment of seizure before surgery
Fit free >60%
Presurgical evaluation for epilepsy Routine electroencephalography (EEG)
Video-EEG monitoringMagnetic resonance imagingPositron emission tomography*Single-photon emission computed tomography*Neuropsychological evaluationIntracarotid amobarbital test (ie, Wada's test)
Epilepsy in women Cong malformation with drugs 4-6% (2x
normal population) >90% with epilepsy have normal
pregnancy and deliver normal children Most will need drug Rx, because
benefits outweighs risks Number of drugs proportional to risk of
teratogenecity
Epilepsy in women All females in childbearing age should
be on folic acid Congenital abnormalities (with all)
Minor dysmorphic anomalies Hyperptelorism Epicanthal folds Distal digital hypoplasia
Valproate: 2% risk of spina bifida So avoid in females unless clearly indicated
Epilepsy in women Contraceptive failure
Barbiturates carbamezipine Phenytoin Topiramate
No effects on contraception Gabapentin Lamotrigine Valproate