epidemiology of benzodiazepine prescribing and use gerry & marci’s story 4 nd annual...
Post on 22-Dec-2015
219 views
TRANSCRIPT

Epidemiology of Benzodiazepine Prescribing and UseGerry & Marci’s Story
4nd Annual Benzodiazepine Conference
Portland, Maine2006

J. Gerry Mugford, PhD, CMHAsst. Prof. of Medicine, Pharmacy, & Psychiatry
Memorial University of Newfoundland©JGM 2006
Marcella H. Sorg, RN, PhDMargaret Chase Smith Policy Center
University of Maine

Credit Where Credit is Credit Where Credit is DueDue
Stevan GressittStevan Gressitt Karen SimoneKaren Simone Todd MandellTodd Mandell Len KayeLen Kaye Bill FlaggBill Flagg Office of Substance Abuse, State of MaineOffice of Substance Abuse, State of Maine Dorothy Rhodes, IMS HealthDorothy Rhodes, IMS Health Maine Care, Anthem, Express ScriptsMaine Care, Anthem, Express Scripts Office of Chief Medical ExaminerOffice of Chief Medical Examiner

Credit Where Credit is Credit Where Credit is DueDue
All contributors to Maine All contributors to Maine Benzodiazepine Study Group Benzodiazepine Study Group data collectiondata collection
All you here today and tomorrowAll you here today and tomorrow All those who have made All those who have made
commitments to US/Canada BSG commitments to US/Canada BSG and couldn’t be hereand couldn’t be here

Focus on ResearchFocus on Research
Why more numbers?? Build effective feedback loops
between practice and policy to change behavior INFORMATION SYSTEMS
New DAWN New Prescription Monitoring Program
Monitor change: CONTEXT & PLAYERS CHANGING

HistoryHistory
Maine Benzodiazepine Study Group created in 2002 –collecting data 5th. year of data 4th. year of Annual Benzodiazepine
Conferences Published “white papers”
summarizing data from diverse links in the benzodiazepine “life cycle”
Journal articles under development

Epidemiology: Inform Epidemiology: Inform Public Health and Clinical Public Health and Clinical
PracticePractice Increased morbidity in particular Increased morbidity in particular
populations and populations and potential need to screen & potential need to screen & treat underlying problem treat underlying problem (e.g., anxiety in (e.g., anxiety in women)women)
Variation in clinical prescribing practices Variation in clinical prescribing practices and and potential need to set guidelines potential need to set guidelines (e.g., (e.g., issues of polypharmacy or long-term issues of polypharmacy or long-term treatment) treatment)
Increased individual and public health risks Increased individual and public health risks posed by high prescriptive & misuse posed by high prescriptive & misuse prevalence and the prevalence and the potential need to potential need to regulateregulate (e.g., driving with BZDs) (e.g., driving with BZDs)

What Patterns are What Patterns are Consistent? Consistent?
(a preview of what we will (a preview of what we will show)show)Prescriptions
Females > males Older > younger, generally, with peak in
50s
Associated risks Accidents: falls, motor vehicle Polypharmacy adverse events Suicides (multiple drug) Illicit drug use (associated with opiates,
alcohol) Drug dependency with long-term use

BZDUses
Anxiolytic
Hypnotic
Amnesic
Anticonvulsant
Myorelaxant

NNEPC: Maine BZD Citings, Human Poisoning Exposures by Gender
0
100
200
300
400
500
600
700
800
2002 2003 2004 2005 2006est
Female
Male
Unknown
Total

NNEPC: Maine BZD Citings, Information Calls by Gender
0500
1,0001,5002,0002,5003,0003,5004,0004,5005,000
2002 2003 2004 2005 2006est
Female
Male
UNK/INV
Total

Maine Medicaid Total BZD Users & BZD Scripts
0
50000
100000
150000
200000
250000
300000
350000
1998 1999 2000 2001 2002 2003 2004 2005
Total Enrollees
Total Users
Total Scripts

Maine Medicaid: Number of Scripts per BZD User
0123456789
10
1998 1999 2000 2001 2002 2003 2004 2005
Ratio
12.8% of enrollees
12.5%of enrollees

Vermont Medicaid: Enrollees with Paid BZD Claims
0
500
1,000
1,500
2,000
2,500
Males
Females
Total

BZD Prevalence Comparison by Age & GenderAnthem 2003 & Medicaid 2004
0
5
10
15
20
25
30
0-9 10-19
20-29
30-39
40-49
50-59
60-69
70-79
80+
Age Group
Perc
ent w
ith B
ZD
Scrip
t
FE Anthem 03
FE Medicaid 04
MA Anthem 03
MA Medicaid 04

Express Scripts 2002 Express Scripts 2002 (2003)(2003)
N = 206,675; n= RS 4,993N = 206,675; n= RS 4,993
0
10
20
30
40
50
0-9 10-19
20-29
30-39
40-49
50-59
60-69
70-79
80+
Females
Males
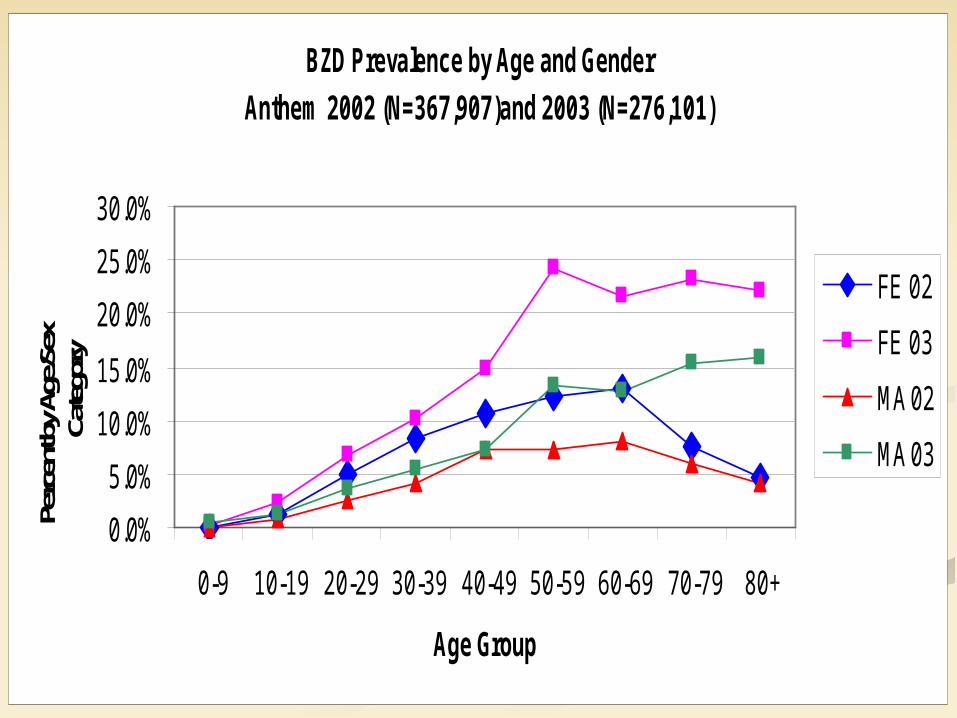
BZD Prevalence by Age and Gender
Anthem 2002 (N=367,907)and 2003 (N=276,101)
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
30.0%
0-9 10-19 20-29 30-39 40-49 50-59 60-69 70-79 80+
Age Group
Perc
ent b
y Age
/Sex
Ca
tego
ry
FE 02
FE 03
MA 02
MA 03

US Per Capita Retail Scripts: Age/Gender
0
10
20
30
40
50
US 8.1 13.8 20.8 28.9
Maine 8.4 14.2 17.1 20.4
TN 13.3 22.9 29.5 41.6
19-64 19-64 65+ 65+
Males Females Males Females

Anthem 2003 HighlightsAnthem 2003 Highlights
10% of 2003 subscribers with prescriptions had at least 1 prescription for a BZD (n=27,308 out of 276,101)
Of those with a BZD prescription 4% had a prescription for more than one
type 16% had a prescription for >180 days 67% of subscribers with a BZD scrip were
female (similar across age groups 15+)

Note about Express Note about Express ScriptsScripts
Express Scripts states 2003 rates are unlikely to be significantly different from 2002 From sample n=8267: 3.3% Population size is 206,675 (possibly
includes subscribers without any prescriptions)
Possibly does not cover all BZDs (Anthem 10%)

Comparison of BZD Prescription Prevalence
9.75
6.15
3.3
9.85
3.3
10.7410.76
10.08
0 2 4 6 8 10 12
ME-Medicaid
VT-Medicaid
Anthem
Express Scripts
2006
2005
2004
2003
2002

Percent Female Among BZD Prescription Recipients
0 10 20 30 40 50 60 70 80
ME-Medicaid % Female
VT-Medicaid % Female
NNEPC Poisonings % Female
Anthem % Female
Express Scripts % Female
2006
2005
2004
2003
2002

Maine Nursing Home Maine Nursing Home Sample “H” 2003-04Sample “H” 2003-04
DrugClass
HRange
H Ave.
MaineAve.
Anti anxiety 12-28% 21% 18–19%
Sedative/hypnotic
0-8% 3% 4%

Some Nursing Home Some Nursing Home EstimatesEstimates
Important –Patterns Do Important –Patterns Do Vary!Vary!Antianxiety Hypnotic
Canada 12.7% 12.2%
US 15.7% 5.0%
Low 6.0 % HI 1.9% CO/WI
High 24.0% TN 8.5% LA
Maine 19.4% ME 4.3% ME

CI: Why Do They Give It?CI: Why Do They Give It?
Indication Global %
Anxiety 48.6
Depression 14.4
Agitated Depression 9.9
Insomnia 16.0
Alcoholism 1.7
Organic disorder 9.4

Is there a problem?Is there a problem? Women more likely than men to have
prescription–why? (genders more equal for emergency room)
Higher prescribing rates for Medicare/Medicaid –why?
Older age has rates > 2X general population for prescriptions (younger ages for emergency room)
24% increase in hip fracture comparing seniors take BDZ vs. no BDZ

Is there a problem?Is there a problem?
Implication in suicide rates in persons >65 as high as 39% [BZD sole agent in 72% of cases]
Associated with illicit drug use Associated with substance abuse Associated with automobile
accidents [BDZ established main cause]
Associated with drug overdose [BDZ established cause]

Thank youThank youOn to MarciOn to Marci