eoin o’brien and eamon dolan emerging role for nocturnal bp · eoin o’brien and eamon dolan ......
TRANSCRIPT
Eoin O’Brien and Eamon Dolan
MUCH HAPPENS to the cardiovascularsystem during the night and during sleep,especially in relation to blood pressure.These nocturnal occurrences have beenlargely ignored in clinical practice becausethe methodology for assessing nocturnalprofiles of blood pressure – 24-hour ambu-latory blood pressure measurement(ABPM) – has been accepted only slowly inclinical practice, or used only sparingly forthe recording of blood pressure during thenight.
With the recent publication of the DublinOutcome Study there is now renewed inter-est in the importance of nocturnalhypertension in clinical practice. 1
Which measurement of blood pressure isbest?
The most commonly used technique ofblood pressure measurement in clinicalpractice is the auscultatory method with amercury sphygmomanometer and stetho-scope.
A meta-analysis of clinic blood pressuremeasurement (CBPM) in one million adultsparticipating in 61 prospective studies hasshown that a systolic CBPM 10mmHg ordiastolic CBPM 5mmHg above normal isassociated with about 40% higher risk ofstroke death and about 30% higher risk ofdeath from ischaemic heart disease andother vascular causes.
There are, however, numerous criticismsof CBPM, which include interobserver andintraobserver variability and terminal digitpreferences, all of which may bias the accu-racy of measurement. Moreover, CBPMcannot detect white-coat hypertension, alargely innocent condition, which obscuresthe true level of blood pressure and theprevalence of which can be as high as 30%.Which measure is best for predictingoutcome?
There is no doubt but that ABPM is supe-rior to CBPM in predicting target organinvolvement, such as left ventricular hyper-
trophy, microalbuminuria and cerebralischaemia, in patients with hypertension.
However, the ultimate prognostic end-point is cardiovascular death, and evidencethat ABPM is superior to other measure-ments in predicting cardiovascularmortality has been lacking.
A number of small studies have sug-gested that ABPM is a better predictor ofmortality than CBPM, and similarly, evi-dence has been accumulating to suggestthat night-time pressure might be superiorto daytime pressure in predicting cardio-vascular outcome.The Dublin outcome study cohort
The Blood Pressure Unit (formerly locatedat the Charitable Infirmary and based lat-terly Beaumont Hospital in Dublin) hasbeen in operation for 22 years. The demo-graphic details and cardiovascular riskfactors of more than 20,000 patients havebeen entered into a database since 1980,making it the largest single centre data-
blood pressure measurement
Spring 2006 cardiologyprofessional 23
Evidence is growing to support the use of ABPM in allpatients with high BP, not just in selected individuals
Emerging role fornocturnal BP
O'Brien article-NH 06/03/2006 15:21 Page 1
24 cardiologyprofessional Spring 2006
base of its kind in the world.From this cohort, 5,292 untreated
patients whose ABPM record included atleast 10 daytime and five night-time read-ings and who had had standardised CBPMconstituted the Dublin outcome study.
All data were transferred into a softwarepackage (dabl®Cardiovascular, dabl® Lim-ited, Dublin, Ireland), which allowscalculation of systolic and diastolic pres-sures for the daytime period (average ofreadings between 9am and 9pm, thenight-time period average of readingsbetween 1am and 6am) and the 24-hourperiod without applying any editing crite-ria.
A methodical search of the death registerfor these patients showed that there hadbeen 646 deaths, of which 389 were cardio-vascular during a median follow-up periodof 8.4 years.Results of the Dublin outcome study
The first point in need of emphasis isthat the Dublin Outcome Study is thelargest single-centre study to date usingcarefully collected computerised data froma large western population of hypertensivepatients, who were not on antihyperten-sive medication at the time of bloodpressure measurement.
Firstly, as might be expected, the preva-lence of known cardiovascular risk factorswas higher among patients who died ofcardiovascular causes.
Confirming the results of smaller studies,the Dublin Outcome Study demonstratedbeyond any doubt in this large cohort thatafter adjusting for gender, age, risk indicesand clinic blood pressure, higher meanvalues of ABPM were independent predic-tors for cardiovascular mortality.
Most interestingly, the Dublin Outcome
Study showed clearly that night-time bloodpressure was the best predictive measure-ment of cardiovascular outcome, and thehazard ratios for night-time ABPMremained significant after adjustment fordaytime ambulatory blood pressure.
The results of the Dublin Outcome Studyconfirm, therefore, the superiority of ABPMover CBPM in predicting cardiovascularmortality.The relevance of night-time bloodpressure
The dipper/non-dipper classification ofnocturnal blood pressure was first intro-duced in The Lancet by the Dublin BloodPressure Unit in 1988, when a retrospectiveanalysis suggested that non-dippinghypertensive patients had a higher risk ofstroke than the majority of patients with adipping pattern.2
Since then there have been many studiesevaluating morbidity and dipping status,and though there has been some disagree-ment in the literature, on balance, mostlarge-scale prospective studies support theconcept that a diminished nocturnal bloodpressure fall is associated with a worseprognosis.
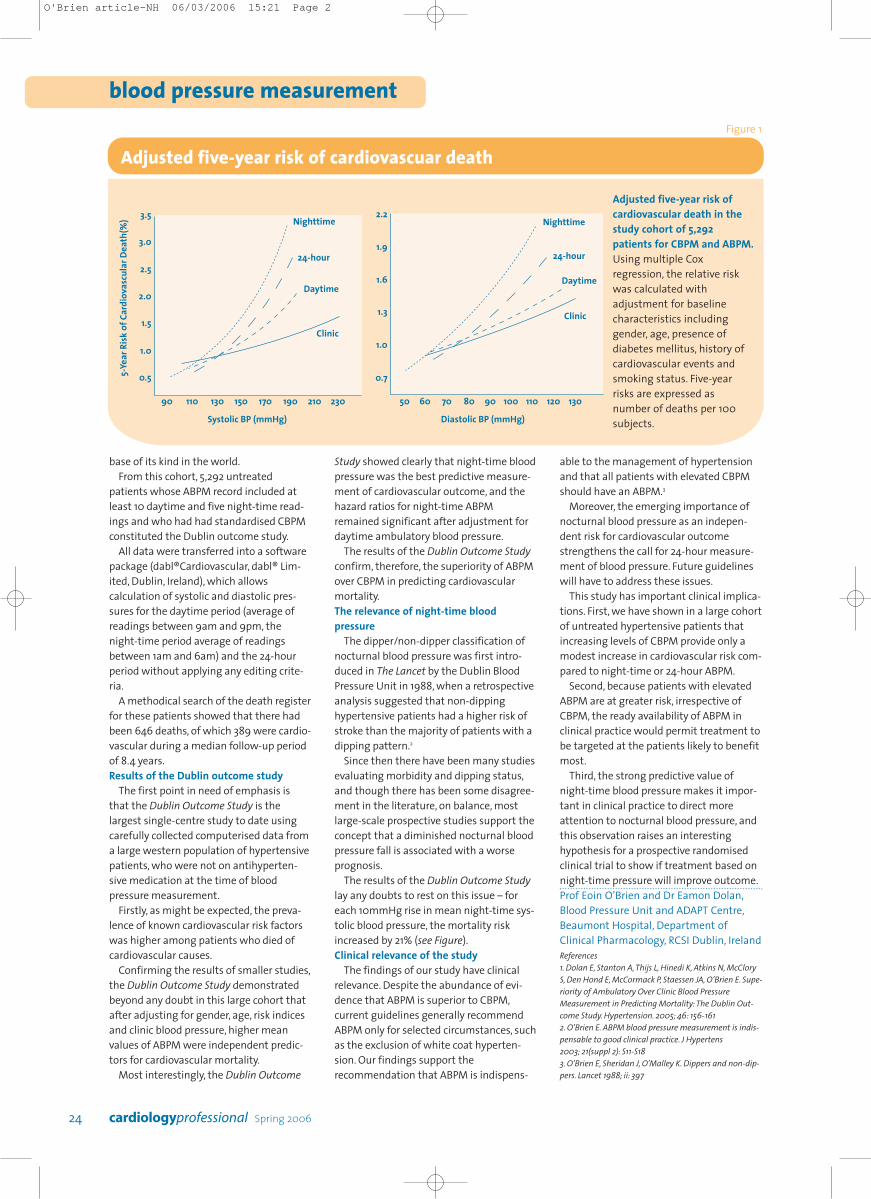
The results of the Dublin Outcome Studylay any doubts to rest on this issue – foreach 10mmHg rise in mean night-time sys-tolic blood pressure, the mortality riskincreased by 21% (see Figure).Clinical relevance of the study
The findings of our study have clinicalrelevance. Despite the abundance of evi-dence that ABPM is superior to CBPM,current guidelines generally recommendABPM only for selected circumstances, suchas the exclusion of white coat hyperten-sion. Our findings support therecommendation that ABPM is indispens-
able to the management of hypertensionand that all patients with elevated CBPMshould have an ABPM.3
Moreover, the emerging importance ofnocturnal blood pressure as an indepen-dent risk for cardiovascular outcomestrengthens the call for 24-hour measure-ment of blood pressure. Future guidelineswill have to address these issues.
This study has important clinical implica-tions. First, we have shown in a large cohortof untreated hypertensive patients thatincreasing levels of CBPM provide only amodest increase in cardiovascular risk com-pared to night-time or 24-hour ABPM.
Second, because patients with elevatedABPM are at greater risk, irrespective ofCBPM, the ready availability of ABPM inclinical practice would permit treatment tobe targeted at the patients likely to benefitmost.
Third, the strong predictive value ofnight-time blood pressure makes it impor-tant in clinical practice to direct moreattention to nocturnal blood pressure, andthis observation raises an interestinghypothesis for a prospective randomisedclinical trial to show if treatment based onnight-time pressure will improve outcome.Prof Eoin O’Brien and Dr Eamon Dolan,Blood Pressure Unit and ADAPT Centre,Beaumont Hospital, Department ofClinical Pharmacology, RCSI Dublin, Ireland References1. Dolan E, Stanton A, Thijs L, Hinedi K, Atkins N, McCloryS, Den Hond E, McCormack P, Staessen JA, O’Brien E. Supe-riority of Ambulatory Over Clinic Blood PressureMeasurement in Predicting Mortality:The Dublin Out-come Study. Hypertension. 2005; 46: 156-1612. O’Brien E. ABPM blood pressure measurement is indis-pensable to good clinical practice. J Hypertens2003; 21(suppl 2): S11-S18 3. O’Brien E, Sheridan J, O’Malley K. Dippers and non-dip-pers. Lancet 1988; ii: 397
Adjusted five-year risk ofcardiovascular death in thestudy cohort of 5,292patients for CBPM and ABPM.Using multiple Coxregression, the relative riskwas calculated withadjustment for baselinecharacteristics includinggender, age, presence ofdiabetes mellitus, history ofcardiovascular events andsmoking status. Five-yearrisks are expressed asnumber of deaths per 100subjects.
blood pressure measurementFigure 1
Adjusted five-year risk of cardiovascuar death
5-Ye
ar R
isk o
f Car
diov
ascu
lar D
eath
(%)
Systolic BP (mmHg) Diastolic BP (mmHg)
90
0.5
1.0
1.5
2.0
2.5
3.0
3.5
110 130 150 170 190 210 230 50
0.7
1.0
1.3
1.6
Nighttime Nighttime
24-hour 24-hour
DaytimeDaytime
Clinic
Clinic
1.9
2.2
60 70 80 90 100 110 120 130
O'Brien article-NH 06/03/2006 15:21 Page 2