enfoque de la hipercalcemia
TRANSCRIPT

Enfoque del paciente con Hipercalcemia

Conceptos básicos• Ion divalente
• Rol esencial en función celular como segundo mensajero
• Contractilidad muscular y miocárdica
• Coagulación
• Secreción hormonal
• 98% en esqueleto – 50% ionizado – 50% unido albumina
Harrison`s Principles of Internal Medicine, 18th edition 2011, Chapter 46, Hipercalcemia

Fisiología
American Family Physician Volume 67, Number 9 / MAY 1, 2003

Fisiología
Rev Chil Pediatr 2012; 83 (2): 117-127

Clasificación
American Family Physician Volume 67, Number 9 / MAY 1, 2003
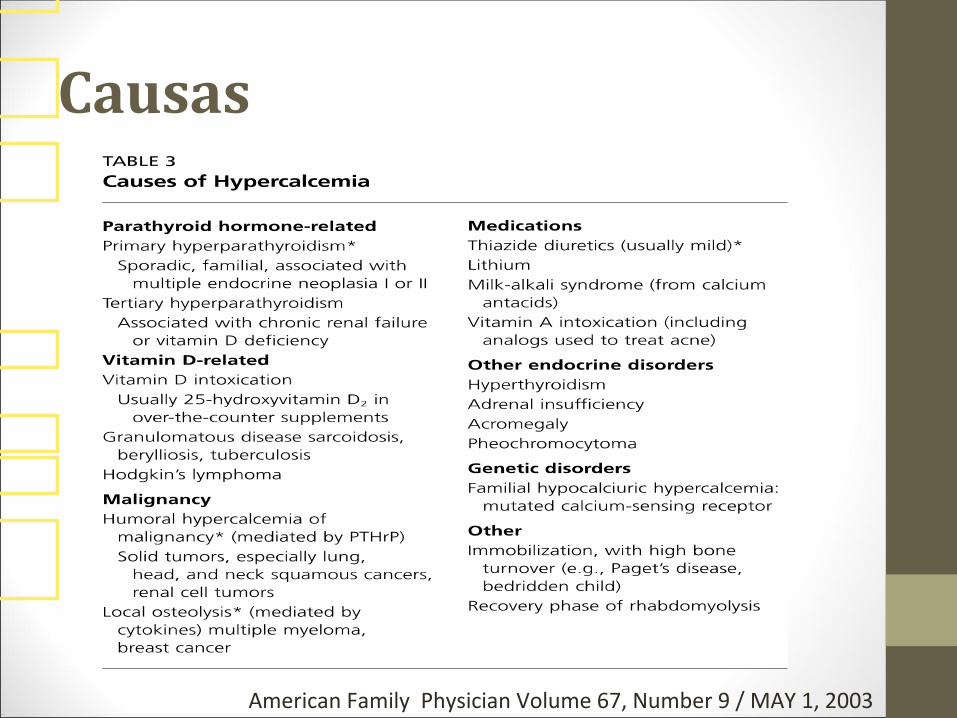
Causas
American Family Physician Volume 67, Number 9 / MAY 1, 2003

Manifestaciones clínicas
American Family Physician Volume 67, Number 9 / MAY 1, 2003

Enfoque diagnostico

Importancia corrección de acuerdo a albumina
Harrison`s Principles of Internal Medicine, 18th edition 2011, Chapter 46, Hipercalcemia

Enfoque
American Family Physician Volume 67, Number 9 / MAY 1, 2003

Siguiente paso: PTH

PTH suprimida

PTH normal o elevada

Tratamiento• De acuerdo:
1.Severidad y síntomas
2.Causa especifica
Harrison`s Principles of Internal Medicine, 18th edition 2011, Chapter 46, Hipercalcemia

Leve (10 – 12 mg/dl) asintomatica• Proceso diagnostico de causa subyacente
• Tratar enfermedad productora
• No existe beneficio de medidas especificas
Harrison`s Principles of Internal Medicine, 18th edition 2011, Chapter 46, Hipercalcemia

Medidas generales: moderada (>12) + síntomas y severa (>14)
American Family Physician Volume 67, Number 9 / MAY 1, 2003

Medidas especificas

¿Cirugia?
only if they meet criteria recommended by theNational Institutes of Health ConsensusDevelopment Conference (Table 4).1 0 [Evi-dence level C, consensus opinion] The diseasewill progress in approximately one fourth ofpatients who do not undergo surgery.1 1 Pre-operative nuclear imaging of the parathyroidswith a sestamibi scan (Figure 4) allows the sur-geon to perform unilateral neck dissection,which results in reduced operative time andless morbidity.1 2 Risks of parathyroid surgeryinclude permanent hypoparathyroidism anddamage to the recurrent laryngeal nerve.
Chronic renal failure generally causeshypocalcemia. If untreated, prolonged highphosphate and low vitamin D levels can leadto increased PTH secretion and subsequenthypercalcemia. This is termed tertiary hyper-parathyroidism.
VITAMIN D-MEDIATED CAUSES
The most commonly available vitamin Dsupplements consist of 25-hydroxyvitaminD2 . In suspected overdose of over-the-countervitamin D, the level of 25-hydroxyvitamin D3
(not 1,25-dihydroxyvitamin D3 ) should bemeasured. Macrophages can cause granu-loma-forming (i.e., sarcoidosis, tuberculosis,Hodgkin’s lymphoma) increased extra-renalconversion of 25-hydroxyvitamin D3 to cal-citriol. PTH levels are suppressed, and levels of1,25-dihydroxyvitamin D3 are elevated.Hypercalcemia mediated by excessive vitaminD responds to a short course of glucocorti-coids if the underlying disease is treated.
HYPERCALCEMIA OF MALIGNANCY
Hypercalcemia of malignancy occurs in sev-eral settings.1 3 It is mediated most commonlyby systemic PTHrP in patients with solidtumors. This is known as the humoral hyper-calcemia of malignancy. PTHrP mimics thebone and renal effects of PTH. In contrast toprimary hyperparathyroidism, the humoralhypercalcemia of malignancy is associatedwith suppressed PTH levels and normal cal-citriol levels. Extensive bone lysis also cancause malignancy-associated hypercalcemia.
MAY 1, 2003 / VOLUME 67, NUMBER 9 www.aafp.org/afp AMERICAN FAMILY PHYSICIAN 1963
FIGURE 3. Representative serum calcium and PTH levels in pat ients withcalcium disorders. The four dif ferent ly shaped panels depict where theserum calcium level will plot in relat ion to the PTH level in various con-dit ions. In primary hyperparathyroidism, a high PTH level correlateswith a high calcium level. In malignancy-associated hypercalcemia, PTHis suppressed. (PTH = parathyroid hormone)
Representative Normogram for Interpreting Serum Intact PTH Levels
Total serum calcium level, mg/dL (mmol/L)
6 (1.5) 8 (2) 10 (2.5) 12 (3) 14 (3.5) 16 (4)
Inta
ct P
TH
(p
g/m
L)
500
200
150
100
50
Hypopara-thyroidism
Normal
Malignancy
Primary hyperparathyroidism
TABLE 4
Criteria for Surgery in Primary Hyperparathyroidism*
Serum total calcium level > 12 mg per dL (3 mmol per L) at any time
Hyperparathyroid crisis (discrete episode of life-threatening hypercalcemia)
Marked hypercalciuria (urinary calcium excretion more than 400 mg per day)
Nephrolithiasis
Impaired renal function
Osteitis fibrosa cystica
Reduced cortical bone density (measure with dual x-ray absorptiometry or similar technique)
Bone mass more than two standard deviations below age-matched controls (Z score less than 2)
Classic neuromuscular symptoms
Proximal muscle weakness and atrophy, hyperreflexia, and gait disturbance
Age younger than 50
* —Guidelines from the National Institutes of Health Consensus DevelopmentConference.
Information from NIH conference: diagnosis and management of asymptomaticprimary hyperparathyroidism: consensus development conference statement.Ann Intern Med 1991;114:593-7.

Gracias!