endothelin-1 focally constricts … focally constricts pulmonary veins in rats serum endothelin...
TRANSCRIPT

ENDOTHELIN-1 FOCALLY CONSTRICTS PULMONARY VEINS IN RATS
Serum endothelin levels increase during sepsis, ischemia, reperfusion, pulmo- nary operations, and systemic hypertension after surgery. Despite extensive study, the site and extent of action of endothelin on the pulmonary microcir- culation are not well established. To assess the e~ect of endothelin on the pulmonary vasculature, especially the veins, the circulation of the lung was cast with methyl methacrylate 10 minutes after endothelin-1 was given intrave- nously to rats. Endothelin-1, at concentrations of 0.1, 1.0, and 10.0/xg/kg of body weight, increased the mean systemic arterial blood pressure 8%, 7%, and 17% (p < 0.01) and mean pulmonary arterial blood pressure 15%, 28%, and 53%, respectively (p < 0.01). The proportional increases in the pulmonary pressures were greater than those of the systemic pressures (p < 0.01). Scanning electron microscopy of cast blood vessels showed more contraction of the veins than the arteries. For doses of 0, 0.1, 1.0, and 10.0 /xg/kg, the respective focal contraction of small veins was 6.7% (-+4.4), 15.4% (_9.1), 23.3% (-10.1), and 14.4% (---9.0) of the vessel diameter (p < 0.01). In addition, the diameters of capillaries increased (p < 0.01) and the capillary interspaces decreased (p < 0.01) after endothelin administration, but not in a linear dose-dependent manner. The dose of endothelin correlated with the change in the mean systemic (r = 0.82,p < 0.01) and the mean pulmonary (r = 0.80,p < 0.01) blood pressures. The mean pulmonary pressure change correlated with the focal venous contraction on the casts (r = 0.35, p < 0.01), capillary diameter (r = 0.64,p < 0.01), and capillary interspace distance (r = -0 .34,p < 0.01). The venous contraction was related to the capillary diameter (r = 0.26, p < 0.01). The most notable elect of endothelin-1 in rat pulmonary microcir- culation is focal constriction of small veins. Because this e~ect may lead to pulmonary edema, endothelin antagonists may be of benefit in a variety of clinical situations. (J TrIORAC CARDIOVASC SURG 1995;110:148-56)
S. Aharinejad, MD, PhD,* D. E. Schraufnagel, MD,** A. Miksovsky, MD,*** E. K. Larson, MS,**** and S. C. Marks, Jr., DDS, PhD,**** Worcester, Mass.
[~ndothel in-1 , a 21-residue pept ide first isolated 1 I . . f r o m endothelial cell cultures, has impor tant
effects on vascular smooth muscle. 2 Endothe l in con- trois regional perfusion of the lung 3 and its serum level increases during sepsis, 4 ischemia, 5 reperfu-
From the Department of Cell Biology, University of Massachu- setts Medical Center, Worcester, Mass.
Supported in part by a grant from the National Institutes of Health (No. DE-07444) (Sandy C. Marks, Jr.) and the James E. Liston Fund at the University of Illinois at Chicago.
Received for publication June 23, 1994. Accepted for publication Oct. 24, 1994. *From the Department of Thoracic and Cardiovascular Surgery,
University of Vienna. **From the Departments of Medicine and Pathology, the Uni-
versity of Illinois at Chicago. ***From St. Elisabeth Hospital, Vienna. ****From the University of Massachusetts Medical Center.
1 4 8
sion, 6 and pu lmonary operations. 7 Endothe l in plays a role in vascular restenosis in patients undergoing angioplasty s and contracts bronchi in experimental lung t ransplantat ion in dogs. 9 It has been associated with systemic hyper tens ion after liver transplanta- tion. 1~ Al though its effects are largely vasoconstric- tive, 11 an initial vasodilatory effect of endothelin-1 occurs in certain young animal species) 2' 13 Endo- thelin-1 causes a biphasic response in the systemic vasculature and increases myocardial contractility in adult rabbits, a l though the reason for the initial
Address for reprints: Dean E. Schraufnagel, MD, Section of Respiratory and Critical Care Medicine, Department of Med- icine M/C 787, University of Illinois at Chicago, 840 S. Wood St., Chicago, IL 60612-7323.
Copyright �9 1995 by Mosby-Year Book, Inc. 0022-5223/95 $3.00 + 0 12/1/61492

The Journal of Thoracic and Cardiovascular Surgery Volume 110, Number 1
Aharinejad et aL 1 4 9
dilation remains uncertain. 14 There is d isagreement about the location o f action and its magni tude in response to specific doses. 15 Fortes, de Nucci, and Garc ia -Leme 16 found it constricts both per ipheral arteries and veins, but Brain 17 found that endothe l in did not affect peripheral veins. Synthes ized by the pu lmonary vasculature, TM endothel in increases pul- monary vascular resistance, a9-22 Endothe l in is in- creased in the alveoli of animals that have b e e n experimentally injured z3 and in the serum of pa- tients who have pu lmonary hyper tension 24-27 and those who undergo hear t transplantation. 28
Most studies of the effect of endothel in on the pu lmonary vasculature have used physiologic mea- surements, such as the pressure genera ted by the shortening of smooth muscle or the resistance to pu lmonary blood flow. Al though these studies give impor tan t functional informat ion they do not show the site o f action, especially on the small pu lmona ry b lood vessels. We were interested in the effect o f endothelin-1 on the pu lmonary vascular bed espe- cially as concerns the veins, which we have studied earlier.29, 30 W e used vascular casts examined with scanning electron microscopy, which show changes in three dimensions in disease 3~ and after the appli- cat ion o f vasoactive drugs. 32 Unders tand ing these effects contributes to our unders tanding of pu lmo- nary vascu la r reactions in patients undergoing sur- gery.
Methods
This experiment was approved by the Animal Care Committee at the University of Massachusetts Medical Center at Worcester. The animals were handled humanely according to the Public Health Service guidelines.
Blood pressure measurements. We divided 24 male Wistar Kyoto rats (Charles River, Boston, Mass.) weigh- ing 160 to 320 gm into four groups and anesthetized them with diethyl ether (Metofane; Fisher Chemicals, Chicago, Ill.). We opened the abdomen, cannulated the aorta, and connected the cannula t o a transducer that recorded blood pressure on a Grass polygraph (Grass, Quincy, Mass.). We connected a 24-gange Teflon catheter with an outer diameter of 0.99 mm, an inner diameter of 0.66 mm, and a tip shaped into an "R crook" to a transducer and placed it into a metal cannula. 33 The cannula was inserted into the right jugular vein and advanced into the r ight ventricle until the typical right ventricular pressure wave-
33 form was obtained. After recording the pressure, we plied the catheter into the pulmonary artery and recorded the pressure again. Then, the caudal vena cava was cannulated at the level of the renal arteries with a 20-gauge catheter. The rats were given 0, 0.1, 1.0, or 10/xg of endotheliml per kilogram of body weight through the caudal vena cava and both systemic and pulmonary arte- rial pressures were again recorded. The different doses of
endothelin-1 were selected on the basis of previous re- ports2O, 22, 34 and correlated with pharmacologic dosesY In pilot studies in a group of animals - in which the lungs were not cast, the vasoconstrictor effect of endothelin-1 lasted 35 (---7) minutes before the blood pressure gradu- ally decreased to the baseline level. The body temperature was maintained with use of a heat lamp. Animals recov- ered from the surgical procedure for 30 minutes before baseline blood pressures were recorded and any drug administered.
Cast preparation. Ten minutes after the endothelin injection, the catheter in the jugular vein was clamped. The vasculature was flushed with 20% dextran 40 in 0.9% saline (Macrodex; Pharmacia, Piscataway, N.J.) with 5000 IU/L of heparin at 42~ through the caudal vena cava until the aortic etflux cleared. This required about 60 ml of solution. 3~ Then, 20 ml of methyl methacrylate (Mercox; Ladd Industries, Burlington, Vt.), mixed with 2 gm of catalyst, was injected over about 1 minute through the vena cava to cast the lungs. 36 Af te r hardening at room temperature for 2 hours, the lungs were dissected out and transferred to a 60 ~ C water bath overnight. The tissue was macerated in a 5% potassium hydroxide solution at 40 ~ C for 6 days. 3~ The specimens were rinsed with tap water for 30 minutes, with 5% formic acid for 10 minutes, and then with three rinses in distilled water for 2 minutes each. 31 The casts were frozen in distilled water, freeze-dried, cut with scissors into 1 to 2 mm thick slices, and mounted onto studs with silver paste and conductive bridges. 37 The casts were sputter coated with palladium-gold for 3 minutes and examined with a JEOL JSM-35C scanning electron micro- scope (JEOL, Tokyo, Japan) at an accelerating voltage of 10 kV.
Specimens were coded so that the microscopist was unaware of the group to which they belonged. From each lung we mounted four slices on aluminum studs. On each stud we studied four arteries, four veins, and four alveolar fields. The fields containing the arteries and veins were selected randomly at 200-fold magnification. Those con- taining alveoli were also selected randomly at 1000-fold magnification. We looked for changes in the surface and caliber of the arteries and veins. 31' 38 Casts of arteries are distinguishable from those of veins because the nuclei of arterial endothelial cells imprint oval impressions that run with the long axis of the vessel. The nuclei of venous endothelial cells imprint round impressions that have no direction. 39 Arteries track with the airways; veins lie apart. Veins have regular ring-shaped indentations; arteries do not. The depths of the contractions in the veins were measured by the method of Schraufnagel and Thakkar. 32 Briefly, the casts were fractured at the constricted sites of the blood vessels. The constricted sites were rotated perpendicular to the viewing plane of the scanning elec- tron microscope. The constricted diameter and outer vessel diameter were measured at the same site. One minus the inner constricted segment divided by the outer diameter of the cast was the percentage of contraction.
Cast alveolar capillaries cover most of the alveolus but leave a small opening between spokes in their hub-and- spoke configuration. In each alveolar capillary basket, the horizontal distances of 10 capillary interspaces (scanning from top to bottom) were measured. ~ In separate areas, we
15 0 Aharinejad et aL The Journal of Thoracic and
Cardiovascular Surgery July 1995
12(
r 10(
0 o
�9
8C
A
25
0.1 1 10
Dose of endothelin-1 (/~g/kg)
20
10 0
5
a 0.1 1 10
Dose of endothelin-1 (#g/kg)
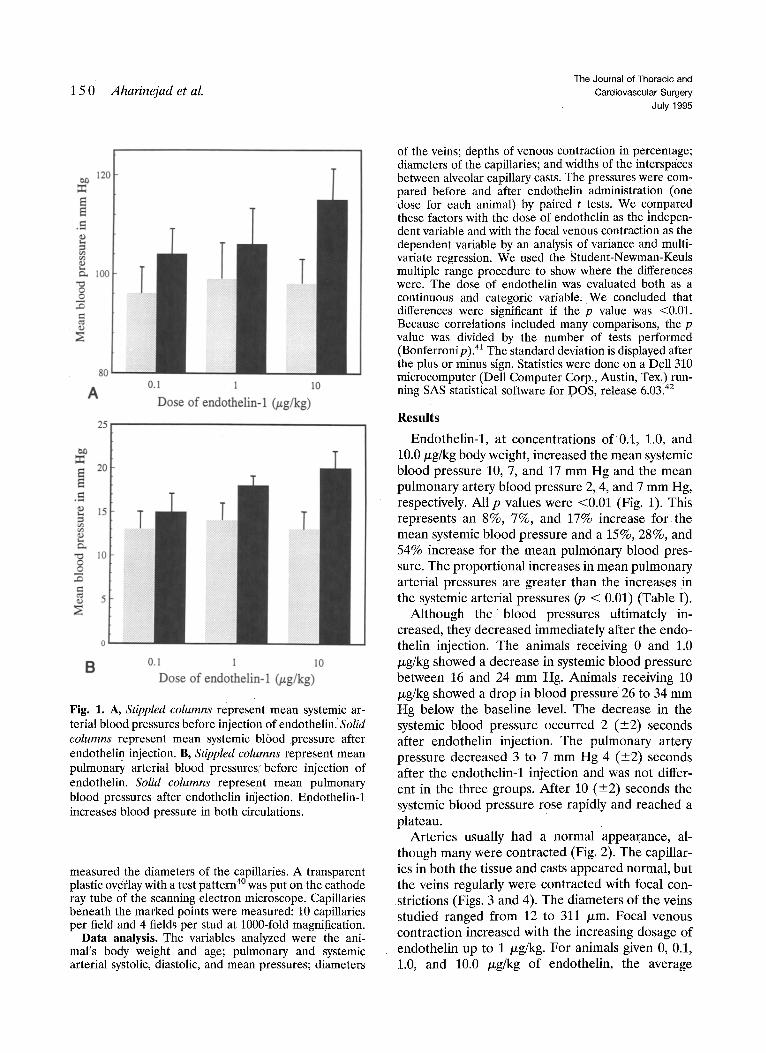
Fig. 1. A, Stippled columns represent mean systemic ar- terial blood pressures before injection of endothelinJ Solid columns represent mean systemic blood .pressure after endotheli n injection. B, Stippled columns represent mean pulmonary arterial blood pressures before injection of endothelin. Solid columns represent mean pulmonary blood pressures after endothelin injection. Endothelin-1 increases blood pressure in both circulations.
measured the diameters of the capillaries. A transparent plastic overlay with a test pattern 4~ was put onthe cathode ray tube of the scanning electron microscope, Capillaries beneath the marked points were measured: 10 capillaries per field and 4 fields per stud at 1000-fold magnification.
Data analysis. The variables analyzed were the ani- mal's body weight and age; pulmonary and systemic arterial systolic, diastolic, and mean pressures; diameters
of the veins; depths of venous contraction in percentage; diameters of the capillaries; and widths of the interspaces between alveolar capillary casts. The pressures were com- pared before and after endothelin administration (one dose for each animal) by paired t tests. We compared these factors with the dose of endothelin as the indepen- dent variable and with the focal venous contraction as the dependent variable by an analysis of variance and multi- variate regression. We used the Student-Newman-Keuls multiple range procedure to show where the differences were. The dose of endothelin was evaluated both as a continuous and categoric variable, We concluded that differences were significant if the p value was <0.01. Because correlations included many comparisons, the p value was divided by the number of tests performed (Bonferronip). 41 The standard deviation is displayed after the plus or minus sign. Statistics were done on a Dell 310 microcomputer (Dell Computer Corp., Austin, Tex.) run- ning SAS statistical software for DOS, release 6.03. 42
Results
Endothelin-1, at concentrations of 0.1, 1.0, and 10.0/xg/kg body weight, increased the mean systemic blood pressure 10, 7, and 17 m m Hg and the mean pulmonary artery blood pressure 2, 4, and 7 m m Hg, respectively. All p values were <0.01 (Fig. 1). This represents an 8%, 7%, and 17% increase for the mean systemic blood pressure and a 15%, 28%, and 54% increase for the mean pulmonary blood pres- sure. The proport ional increases in mean pulmonary arterial pressures are greater than the increases in the systemic arterial pressures (p < 0.01) (Table I).
Although the blood pressures ultimately in- creased, they decreased immediately after the endo- thelin injection. The animals receiving 0 and 1.0 /.~g/kg showed a decrease in systemic blood pressure between 16 and 24 m m Hg. Animals receiving 10 p,g/kg showed a drop in blood pressure 26 to 34 mm Hg below the baseline level. The decrease in the systemic blood pressure occurred 2 (_+2) seconds after endothelin injection. The pulmonary artery pressure decreased 3 to 7 mm Hg 4 (+2) seconds after the endothelin-1 injection and was not differ- ent in the three groups. After 10 (_+2) seconds the systemic blood pressure rose rapidly and reached a plateau.
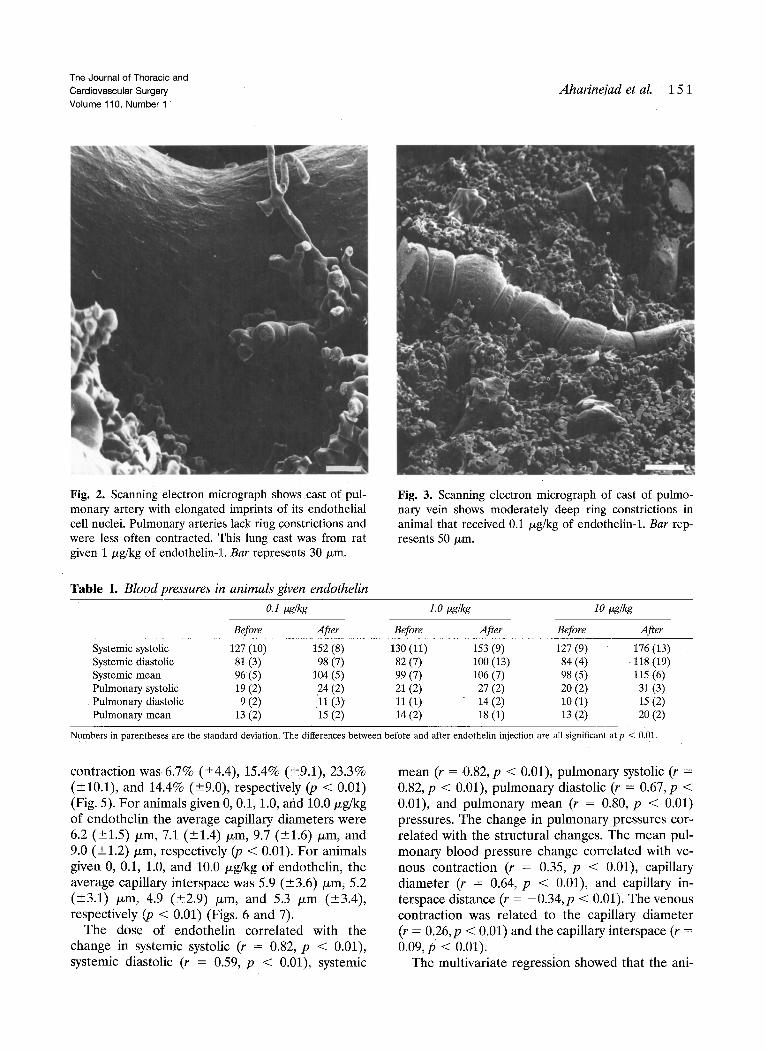
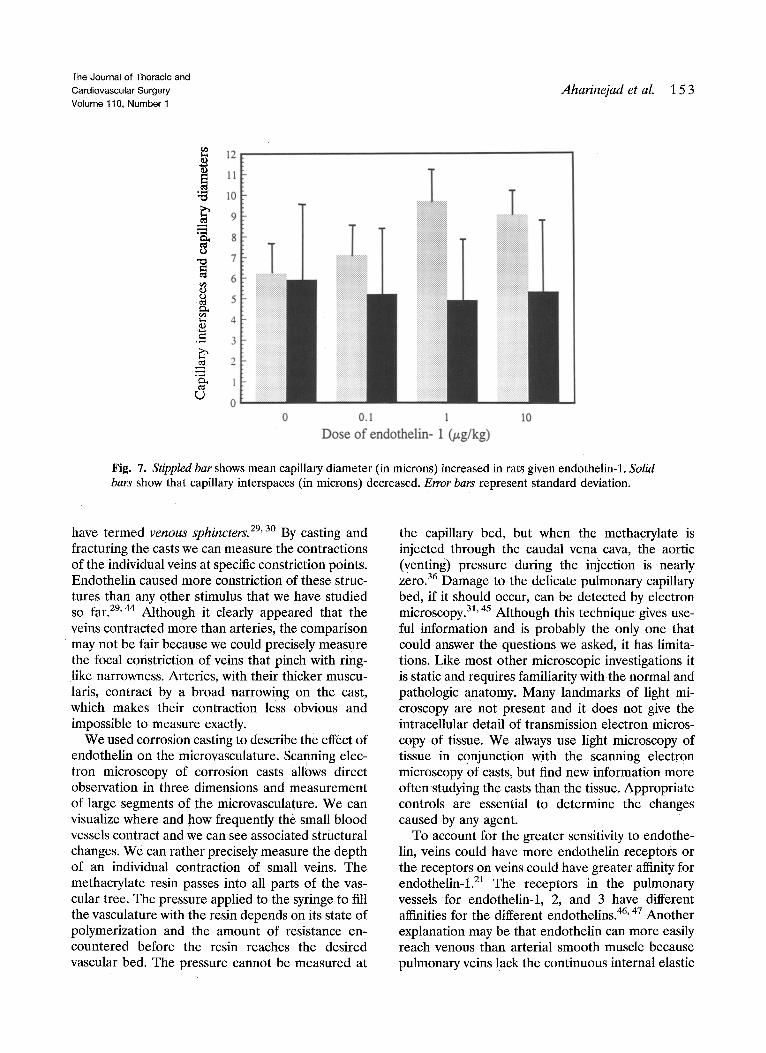
Arteries usually had a normal appearance, al- though many were contracted (Fig. 2). The capillar- ies in both the tissue and casts appeared normal, but the veins regularly were contracted with focal con- strictions (Figs. 3 and 4). The diameters of the veins studied ranged f rom 12 to 311 /~m. Focal venous contraction increased with the increasing dosage of endothelin up to 1 /~g/kg. For animals given 0, 0.1, 1.0, and 10.0 txg/kg of endothelin, the average
The Journal of Thoracic and Cardiovascular Surgery Volume 110, Number 1
Aharineiad et al. 15 1
Fig. 2. Scanning electron micrograph shows cast of pul- monary artery with elongated imprints of its endothelial cell nuclei. Pulmonary arteries lack ring constrictions and were less often contracted. This lung cast was from rat given 1 /xg/kg of endothelin-1. Bar represents 30/xm,
Table I. Blood pressures in animals given endothelin
Fig. 3. Scanning electron micrograph of cast of pulmo- nary vein shows moderately deep ring constrictions in animal that received 0.1 /xg/kg of endothelin-1. Bar rep- resents 50/xm.
0.1 tzg/kg 1.0 tlg/kg 10 tzg/kg
Before After Before After Before After
Systemic systolic 127 (10) 152 (8) 130 (11) 153 (9) 127 (9) 176 (13) Systemic diastolic 81 (3) 98 (7) 82 (7) 100 (13) 84 (4) 118 (19) Systemic mean 96(5) 104 (5) 99 (7) 106 (7) 98 (5) 115 (6) Pulmonary systolic 19 (2) 24 (2) 21 (2) 27 (2) 20 (2) 31 (3) Pulmonary diastolic 9 (2) '11 (3) 11 (1) 14 (2) 10 (1) 15 (2) Pulmonary mean 13 (2) 15 (2) 14 (2) 18 (1) 13 (2) 20 (2)
Numbers in parentheses are the standard deviation. The differences between before and after endothelin injection are all significant at p < 0.01.
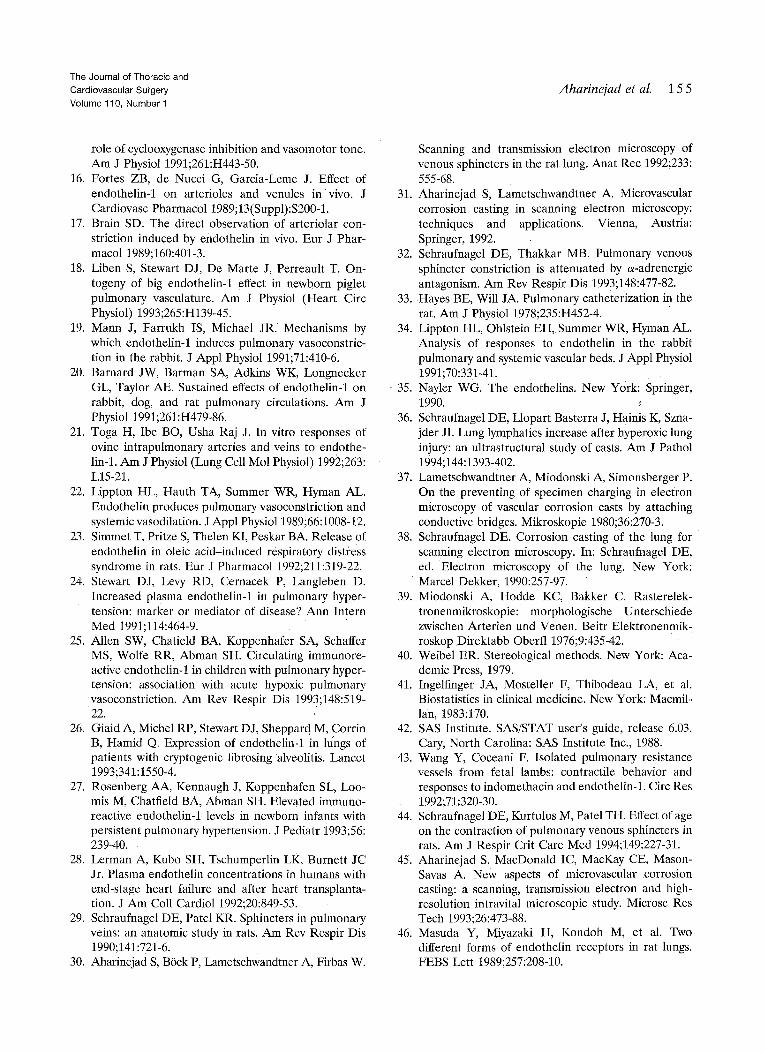
contraction was 6.7% (_+4.4), 15.4% (+9.1), 23.3% (+10.1), and 14.4% (_+9.0), respectively (p < 0,01) (Fig. 5). For animals given 0, 0.1, 1.0, and 10.0/xg/kg of endothelin the average capillary diameters were 6.2 (_+1.5) kern, 7.1 (+1.4)/xm, 9.7 (___1.6) Ixm, and 9.0 (_+1.2) Izm, respectively (p < 0.01). For animals given 0, 0.1, 1.0, and 10.0 Izg/kg of endothelin, the average capillary interspace was 5.9 (_+3.6) txm, 5.2 (_+3.1) tzm, 4.9 (+2.9) /xm, and 5.3 /xm (-+3.4), respectively (p < 0.01) (Figs. 6 and 7).
The dose of endothelin correlated with the change in systemic systolic (r = 0.82, p < 0.01), systemic diastolic (r = 0.59, p < 0.01), systemic
mean (r = 0.82, p < 0.01), pulmonary systolic (r = 0.82, p < 0.01), pulmonary diastolic (r = 0.67, p < 0.01), and pulmonary mean (r = 0.80, p < 0.01) pressures. The change in pulmonary pressures cor- related with the structural changes. The mean pul- monary blood pressure change correlated with ve- nous contraction (r = 0.35, p < 0.01), capillary diameter (r = 0.64, p < 0.01), and capillary in- terspace distance (r = -0 .34 ,p < 0.01). The venous contraction was related to the capillary diameter (r = 0.26,p < 0.01) and the capillary interspace (r = 0.09, p < 0.01).
The multivariate regression showed that the ani-

1 5 2 Aharinejad et al. The Journal of Thoracic and
Cardiovascular Surgery July 1995
35
,~- 30
c~
25
0
10 rm
e~
5 >
0
0 0.1 1 10
Dose of endothelin-1 (/zg/kg)
Fig. 5. Graph shows that mean venous contraction (_+ stan- dard deviation) at sphincters, expressed in percentage of diam- eter, was highest in animals receiving 1/~g/kg endothelin-1.
Fig. 4. This cast pulmonary vein with its round reliefs of endothelial cell nuclei has contraction of about 40% of its diameter at its constricted site. This lung cast was from rat that received 0.1 /zg/kg of endothelin-1. Bar represents 20/am.
mal's body weight and age had an effect on venous contraction in addition to the blood pressure change caused by endothelin. When each variable was en- tered first into the regression, the change in blood pressure (F = 26.3, p < 0.01) had a greater effect than weight (F = 0.2, p was not significant) and age (F = 7.8, p < 0.01), but when the other variables were in the equation, the change in blood pressure (F = l l . 6 , p < 0.01) had a lesser effect than weight (F = 36.2, p < 0.01) and age (F = 41,9, p < 0.01). Not surprisingly, these variables were interactive so that the effect of the change in pulmonary blood pressure on venous contraction was greater in the older animals (F = 22.2, p < 0.01), although the interactive term of weight and change in blood pressure was not significant (F = 0.01). Older and heavier animals also had greater contraction (F = 14.8, p < 0.01 for the interactive term age times weight with the dependent variable contraction).
Discussion
Endothelin-1 had proportionally a greater effect on the pulmonary blood pressure than on the sys- temic blood pressure and pulmonary veins appeared
Fig. a. Cast shows capillaries of alveolus and spaces between them. This lung cast was from rat that received 10 /zg/kg endothelin-1. Bar represents 10/zm.
more constricted than pulmonary arteries in rats. Others have reported that pulmonary veins are more sensitive to endothelin-1 than arteries in sheep 21'43 and rabbits. 34 Small pulmonary veins contract with narrow ringlike constrictions that we
,., 12
,~ 10
9
8 O
�9 ~ 7
6
O
o
c ~
Aharinejad et al. 1 5 3 The Journal of Thoracic and Cardiovascular Surgery Volume 110, Number 1
0 0.1 1 10 Dose o f endothelin- 1 (/~g/kg)
Fig. 7. Stippled bar shows mean capillary diameter (in microns) increased in rats given endothelin-1. Solid bars show that capillary interspaces (in microns) decreased. Error bars represent standard deviation.
have t e rmed venous sphincters. 29' 3o By casting and fracturing the casts we can measure the contractions of the individual veins at specific constriction points. Endothelin caused more constriction of these struc- tures than any other stimulus that we have studied so far. 29' 44 Although it clearly appeared that the veins contracted more than arteries, the comparison may not be fair because we could precisely measure the focal constriction of veins that pinch with ring- like narrowness. Arteries, with their thicker muscu- laris, contract by a broad narrowing on the cast, which makes their contraction less obvious and impossible to measure exactly.
We used corrosion casting to describe the effect of endothelin on the microvasculature. Scanning elec- tron microscopy of corrosion casts allows direct observation in three dimensions and measurement of large segments of the microvasculature. We can visualize where and how frequently the small blood vessels contract and we can see associated structural changes. We can rather precisely measure the depth of an individual contraction of small veins. The methacrylate resin passes into all parts of the vas- cular tree. The pressure applied to the syringe to fill the vasculature with the resin depends on its state of polymerization and the amount of resistance en- countered before the resin reaches the desired vascular bed. The pressure cannot be measured at
the capillary bed, but when the methacrylate is injected through the caudal vena cava, the aortic (venting) pressure during the injection is nearly zero. 36 Damage to the delicate pulmonary capillary bed, if it should occur, can be detected by electron microscopy.31, 45 Although this technique gives use- ful information and is probably the only one that could answer the questions we asked, it has limita- tions. Like most other microscopic investigations it is static and requires familiarity with the normal and pathologic anatomy. Many landmarks of light mi- croscopy are not present and it does not give the intracellular detail of transmission electron micros- copy o f tissue. We always use light microscopy of tissue in conjunction with the scanning electron microscopy of casts, but find new information more often studying the casts than the tissue. Appropriate controls are essential to determine the changes caused by any agent.
To account for the greater sensitivity to endothe- lin, veins could have more endothelin receptors or the receptors on veins could have greater affinity for endothelin-1. 21 The receptors in the pulmonary vessels f o r endothelin-1, 2, and 3 have different affinities for the different endothelins. 46' 47 Another explanation may be that endothelin can more easily reach venous than arterial smooth muscle because pulmonary veins lack the continuous internal elastic

1 5 4 Aharinejad et aL The Journal of Thoracic ant
Cardiovascular Surgel3 July 1995
lamina that pulmonary arteries have. 48 Endothelin may also act on adrenergic neural transmission in addition to its direct effect on smooth muscle cells, 49 although our studies indicate that nerve endings are rare in the wall of rat pulmonary veins. 3~ 31
The average capillary diameter may have in- creased because the capillaries were fuller as a result of venous contraction. The size of the capillary interspace may be decreased because of passive distension of the capillaries. The struc- tural differences shown here were greater when the dose of endothel in was considered as a class variable in the multivariate analysis, which means that the structural changes in the capillaries do not respond in a linear, dose-dependent manner in the doses we used. This may be because the 10 /xg/kg dose of endothel in was not more potent than the 1.0 /xg/kg dose of endothelin, but more likely indicates that the expansion of capillaries is limited to about 9/xm and the intercapillary space will decrease only so far in response to an acute stimulus, which was reached with the 1 /xg/kg dose.
We have associated contract ion of pulmonary venous sphincters with pulmonary edema, z9-31 and o ther workers have found that endothelin-1 causes pulmonary edema in rats and dogs. 2~ En- dothelin levels increase in the plasma of patients who receive cyclosporine after sol id organ trans- plantat ion 5~ and in the pulmonary circulation of patients with mitral stenosis, sl Other studies have shown that endothel in contracts liver sinusoids 52 and is involved in the pathogenesis of ischemia and reperfusion liver injury af ter transplanta- tion. s3 Although the postoperat ive pulmonary edema may have many causes, this study adds to the evidence that sharp focal venous contractions are caused by endothel in and could be associated with pulmonary edema. Applicat ion of endothel in antagonists may be a potential adjunctive therapy after operat ion, especially in lung transplantation; but needs fur ther study. Recent reports have shown that endothel in receptor antagonists can lower blood pressure and block cardiac hypertro- phy in experimental rat models of hyper tension and circulatory overload. TM 55 Addit ional studies on injured and transplanted lung should fur ther define these effects and are planned.
We thank Mrs. Deborah Ellstrtim for excellent techni- cal assistance during blood pressure recording.
R E F E R E N C E S 1. Yanagisawa M, Kurihara H, Kimura N~,etal. A novel
potent vasoconstrictor peptide produced by vascular erid0th61ial cells. Nature 1988;323:411-5.
2. Ouchi Y, Kim S, Souza AC, et al. Central effect ol endothelin on blood pressure in conscious rats. Am J Physiol 1989;256:H1747-51.
3. Onizuka M, Miyauchi T, Mitsui K, et al. Endothelin-1 mediates regional blood flow during and after pulmo- nary operations. J THORAC CARDIOVASC SURG 1992; 104:1696-701.
4. Pittet JF, Morel DR, Hemsen A, et al. Elevated plasma endothelin-1 concentrations are associated with the severity of illness in patients with sepsis. Ann Surg 1991;2!3:261-4.
5. Tsuji S, Sawamura A, Watanabe H, Takihara K, Park SE, Azuma J. Plasma endothelin levels during myo- cardial ischemia and reperfusion. Life Sci 1991;48: 1745-9.
6. Pearson P J, Lin P J, Schaff HV. Production of endo- thelium-derived contracting factor is enhanced after coronary reperfusion. Ann Thorac Surg 1991;51:788- 93.
7. Onizuka M, Miyauchi T, Morita R, et al. Increased plasma concentrations of endothelin-1 during and after pulmonary surgery. J Cardiovasc Pharmacol 1991;17(Suppl);S402-3.
8. Douglas SA, Ohlstein EH. Endothelin-1 promotes neointima formation after balloon angioplasty in the rat. J Cardiovasc Pharmacol 1993;22(Suppl):S371-3.
9. McLarty AJ, Miller VM, Tazelaar HD, McGregor CG. Bronchial contractions in transplanted lungs: influence of denervation, acute rejection, and the bronchial epithelium. J THORAC CARDIOVASC SURG 1993; 106:797-804.
10. Lerman A, Click RL, Narr B J, et al. Elevation of plasma endothelin associated with systemic hyperten- sion in humans following orthotopic liver transplan- tation. Transplantation 1991;51:646-50.
11. Clarke JG, Larkin SW, Benjamin N, et al. Endothe- lin-1 is a potent long-lasting vasoconstrictor in dog peripheral vasculature in vivo. J Cardiovasc Pharma- col 1989;13(Suppl):S211-2.
12. Hasunuma K, Rodman DM, O'Brien RF, McMurtry IF. Endothelin 1 causes pulmonary vasodilation in rats. Am J Physiol 1990;259:H48-54.
13. Perreault T, De Marte J. Endothelin-1 has a dilator effect on neonatal pig pulmonary vasculature. J Car- diovasc Pharmacol 1991;18:43-50.
14. Roberts-Thomson P, McRitchie RJ, Chalmers JP. Endothelin-1 causes a biphasic response in systemic vasculature and increases myocardial contractility in conscious rabbits. J Cardiovasc Pharmacol 1994;24: 100-7.
15. Toga H, Usha Raj J, Hillyard R, Ku B, Anderson J. Endothelin effects in isolated, perfused lamb lungs:
The Journal of Thoracic and
Cardiovascular Sui'gery
Volume 110, Number 1
Aharinejad et al. 15 5
role of cyclooxygenase inhibition and vasomotor tone. Am J Physiol 1991;261:H443-50.
16. Fortes ZB, de Nucci G, Garcia-Leme J. Effect of endothelin-1 on arterioles and venules in vivo. J Cardiovasc Pharmac01 1989;13(Suppl):S200-1.
17. Brain SD. The direct observation of arteriolar con- striction induced by endothelin in vivo. Eur J Phar- macol 1989;160:401-3.
18. Liben S, Stewart DJ, De Matte J, Perreault T. On- togeny of big endothelin-1 effect in newborn piglet pulmonary vasculature. Am J Physiol (Heart Circ Physiol) 1993;265:H139-45.
19. Mann J, Farrukh IS, Michael JR. Mechanisms by which endothelin-1 induces pulmonary vasoconstric- tion in the .rabbit. J Appl Physiol 1991;71:410-6.
20. Barnard JW, Barman SA, Adkins WK, Longnecker GL, Taylor AE. Sustained effects of endothelin-1 on rabbit, dog, and rat pulmonary circulations. Am J Physiol 1991;261 :H479-86.
21. Toga H, Ibe BO, Usha Raj J. In vitro responses of ovine intrapulmonary arteries and veins to endothe- lin-1. Am J Physiol (Lung Cell Mol Physiol) 1992;263: L15-21.
22. Lippton HL, Hauth TA, Summer WR, Hyman AL. Endothelin produces pulmonary vasoconstriction and systemic vasodilation. J Appl Physiol 1989;66:1008-12.
23. Simmet T, Pritze S, Thelen KI, Peskar BA. Release of endothelin in oleic acid-induced respiratory distress syndrome in rats. Eur J Pharmacol 1992;211:319-22.
24. Stewart D J, Levy RD, Cernacek P, Langleben D. Increased plasma endothelin-1 in pulmonary hyper- tension: marker or mediator of disease? Ann Intern Med 1991;114:464-9.
25. Allen SW, Chatield BA, Koppenhafer SA, Schaffer MS, Wolfe RR, Abman SH. Circulating immunore- active endothelin-1 in children with pulmonary hyper- tension: association with acute hypoxic pulmonary vasoconstriction. Am Rev Respir Dis 1993;148:519-
22. 26. Giaid A, Michel RP, Stewart D J, Sheppar d M, Corrin
t
B, Hamid Q. Expression of endothelin-1 in lungs of patients with cryptogenic fibrosing alveolitis. Lancet 1993;341:1550-4.
27. Rosenberg AA, Kennaugh J, Koppenhafen SL, Loo- mis M, Chatfield BA, Abman SH. Elevated immuno- reactive endothelin-1 levels in newborn infants with persistent pulmonary hypertension. J Pediatr 1993;56: 239-40.
28. Lerman A, Kubo SH, Tschumperlin LK, Burnett JC Jr. Plasma endothelin concentrations in humans with end-stage heart failure and after heart transplanta- tion. J Am Coll Cardiol 1992;20:849-53.
29. Schraufnagel DE, Patel KR. Sphincters in pulmonary veins: an anatomic study in rats. Am Rev Respir Dis 1990;141:721-6.
30. Aharinejad S, B6ck P, Lametschwandtner A, Firbas W.
Scanning and transmission electron microscopy of venous sphincters in the rat lung. Anat Rec 1992;233: 555-68.
31. Aharinejad S, Lametschwandtner A. Microvascular corrosion casting in scanning electron microscopy: techniques and applications. Vienna, Austria: Springer, 1992.
32. Schraufnagel DE, Thakkar MB. Pulmonary venous sphincter constriction is attenuated by ~-adrenergic antagonism. Am Rev Respir Dis 1993;148:477-82.
33. Hayes BE, Will JA. Pulmonary catheterization in the rat. Am J Physiol 1978;235:H452-4.
34. Lippton HL, Ohlstein EH, Summer WR, Hyman AL. Analysis of responses to endothelin in the rabbit pulmonary and systemic vascular beds. J Appl Physiol 1991;70:331-41.
�9 35. Nayler WG. The endothelins. New York: Springer, 1990.
36. Schraufnagel DE, Llopart Basterra J, Hainis K, Szna- jder JI. Lung lymphatics increase after hyperoxic lung injury: an ultrastructural study of casts. Am J Pathol 1994; 144:1393-402.
37. Lametschwandtner A, Miodonski A, Simonsberger P. On the preventing of specimen charging in electron microscopy of vascular corrosion casts by attaching conductive bridges. Mikroskopie 1980;36:270-3.
38. Schraufnagel DE. Corrosion casting of the lung for scanning electron microscopy. In: Schraufnagel DE, ed. 'Electron microscopy of the lung. New York: Marcel Dekker, 1990:257-97.
39. Miodonski A, Hodde KC, Bakker C. Rasterelek- tronenmikroskopie: morphologische Unterschiede zwischen Arterien und Venen. Beitr Elektronenmik- roskop Direktabb Oberfl 1976;9:435-42.
40. Weibel ER. Stereological methods. New York: Aca- demic Press, 1979.
41. Ingelfinger JA, Mosteller F, Thibodeau LA, et al. Biostatistics in clinical medicine. New York: Macmil- lan, 1983:170.
42. SAS Institute. SAS/STAT user's guide, release 6.03. Cary, North Carolina: SAS Institute Inc., 1988.
43. Wang Y, Coceani F. Isolated pulmonary resistance vessels from fetal lambs: contractile behavior and responses to indomethacin and endothelin-1. Circ Res 1992;71:320-30.
44. Schraufnagel DE, Kurtulus M, Patel TH. Effect of age on the contraction of pulmonary venous sphincters in rats. Am J Respir Crit Care Med 1994;149:227-31.
45. Aharinejad S, MacDonald IC, MacKay CE, Mason- Savas A. New aspects of microvascular corrosion casting: a scanning, transmission electron and high- resolution intravital microscopic study. Microsc Res Tech 1993;26:473-88.
46. Masuda Y, Miyazaki H, Kondoh M, et al. Two different forms of endothelin receptors in rat lungs. FEBS Lett 1989;257:208-10.

15 6 Aharinejad et al. The Journal of Thoracic and
Cardiovascular Surgery July 1995
47. Kondoh M, Miyazaki H, Uchiyama Y, Yanagisawa M, Masaki T, Murakami K. Solubilization of two types of endothelin receptors, ETA, and ETB from lung with retention of binding activity. Biomed Res 1991;12: 417-23.
48. Wagenvoort CA, Dingemans KP. Pulmonary vascular smooth muscle and its interaction with endothelium: morphologic considerations. Chest 1985;88:200S-2S.
49. Wiklund NP, Ohlen A, Cederqvist B. Adrenergic neuromodulation by endothelin in guinea pig pulmo- nary artery. Neurosci Lett 1989;101:269-73.
50. Grieff M, Loertscher R, Shohaib SA, Stewart DJ. Cyclosporine-induced elevation in circulating endo- thelin-1 in patients with solid-organ transplants. Transplantation 1993;56:880-4.
51. Yamamoto K, Ikeda U, Mito H, Fujikawa H, Sekigu- chi H, Shimada K. Endothelin production in pulmo-
nary circulation of patients with mitral stenosis. Cir- culation 1994;89:2093-8.
52. Okumura S, Takei Y, Kawano S, et al. Vasoactive effect of endothelin~l on rat liver in vivo. Hepatology 1994;19:155-61.
53. Goto M, Takei Y, Kawano S, et al. Endothelin-1 is involved in the pathogenesis of ischemia/reperfusion liver injury by hepatic microcirculatory disturbances. Hepatology 1994;19:675-81.
54. Douglas SA, Gellai M, Ezekiel M, Ohlstein EH. BQ-123, a selective endothelin subtype A-receptor antagonist, lowers blood pressure in different rat models of hypertension. J Hypertens 1994;12:56/1-7.
55. Ito H, Hiroe M, Hirata Y, et al. Endothelin ETA receptor antagonist blocks cardiac hypertrophy pro- voked by hemodynamic overload. Circulation 1994; 89:2198-203.
1-800-55-MOSBY
This number links you to the full text of articles published in over 25,000 journals, including all Mosby journals. MOSBYDocument Express | a rapid response information retrieval service, provides quick turnaround, 24-hour availability, and speedy delivery methods. For inquiries and pricing information, call our toll-free, 24-hour order line: 1-800-55-MOSBY; outside the United States: 415-259-5046; fax: 415-259-5019; E-mail: [email protected].
MOSBY Document Express | is offered in cooperation with Dynamic Information Corp.