endocrine glands
TRANSCRIPT
ENDOCRINE GLANDS
• CONTROL OF SECRETIONS
• FUNCTIONAL TESTS
David Adams
INTRODUCTION• the hypothalamus is part of the brain• thus receives neural signals directly from
the body’s nervous system
INTRODUCTION• the hypothalamus is part of the brain• thus receives neural signals directly from
the body’s nervous system• the hypothalamus links the neural and the
endocrine systems
INTRODUCTION• the hypothalamus is part of the brain• thus receives neural signals directly from
the body’s nervous system• the hypothalamus links the neural and the
endocrine systems• signals from the hypothalamus go to the
pituitary which controls the endocrinefunctions
HYPOTHALAMIC HORMONES
• and the posterior pituitary– there is a direct neural connection between the
hypothalamus and the posterior pituitary
HYPOTHALAMIC HORMONES
• and the posterior pituitary– there is a direct neural connection between the
hypothalamus and the posterior pituitary– three peptides are synthesised by the
hypothalamus and are stored by the posteriorpituitary
POSTERIOR PITUITARYHORMONES
• antidiuretic hormone (ADH)– controls water retention by the kidneys

POSTERIOR PITUITARYHORMONES
• antidiuretic hormone (ADH)– controls water retention by the kidneys
• oxytocin– controls ejection of milk from the lactating
breast and has a role in initiating uterinecontraction during labour
POSTERIOR PITUITARYHORMONES
• antidiuretic hormone (ADH)– controls water retention by the kidneys
• oxytocin– controls ejection of milk from the lactating
breast and has a role in initiating uterinecontraction during labour
• neurophysin– function unclear– may aid transport and storage of the former two
hormones

HYPOTHALAMIC HORMONES
• and the anterior pituitary– no direct neural connection
HYPOTHALAMIC HORMONES
• and the anterior pituitary– no direct neural connection– localised blood supply carries hypothalamic
controlling hormones directly to the anteriorpituitary
HYPOTHALAMIC HORMONES
• and the anterior pituitary– no direct neural connection– localised blood supply carries hypothalamic
controlling hormones directly to the anteriorpituitary
– these stimulate or inhibit secretions by theanterior pituitary
ANTERIOR PITUITARYHORMONES
• growth hormone– controls development and growth
ANTERIOR PITUITARYHORMONES
• growth hormone– controls development and growth
• excess leads to gigantism• deficiency leads to dwarfism
ANTERIOR PITUITARYHORMONES
• growth hormone– controls development and growth
• excess leads to gigantism• deficiency leads to dwarfism
• prolactin– stimulates lactation
ANTERIOR PITUITARYHORMONES
• growth hormone– controls development and growth
• excess leads to gigantism• deficiency leads to dwarfism
• prolactin– stimulates lactation
• excess leads to infertility• deficiency leads to lactation failure
ANTERIOR PITUITARYHORMONES cont.
• tropins - stimulate other endocrine organs
ANTERIOR PITUITARYHORMONES cont.
• tropins - stimulate other endocrine organs– thyrotropin (TSH)
• stimulates thyroid gland
ANTERIOR PITUITARYHORMONES cont.
• tropins - stimulate other endocrine organs– thyrotropin (TSH)
• stimulates thyroid gland
– gonadotropins - follicle stimulating hormoneand luteinising hormone
• necessary for normal gonadal development &function
ANTERIOR PITUITARYHORMONES cont.
– pro-opiocortin - this is a pro-hormone for bothadrenocorticotropin (ACTH) and β-lipotropin
ANTERIOR PITUITARYHORMONES cont.
– pro-opiocortin - this is a pro-hormone for bothadrenocorticotropin (ACTH) and β-lipotropin
• ACTH stimulates adrenals to to secrete a variety ofsteroids (other than aldosterone)
ANTERIOR PITUITARYHORMONES cont.
– pro-opiocortin - this is a pro-hormone for bothadrenocorticotropin (ACTH) and β-lipotropin
• ACTH stimulates adrenals to to secrete a variety ofsteroids (other than aldosterone)
• β-lipotropin is a precursor of endorphins (naturallyoccurring opiates)

SUMMARYBRAIN
HYPOTHALAMUS
POSTERIOR ANTERIORPITUITARY PITUITARY
anti-diuretic hormone&
oxytocin& tropins growth prolactin
neurophysin hormone
growth
thyrotropin gonadotropins pro-opiocortin
stimulates FSH & LHthyroid
stimulategonads
adrenocortico- β-lipotropintropin
(ACTH)endorphins
stimulatesadrenals
NOMENCLATURE
• liberins - stimulate anterior pituitary
NOMENCLATURE
• liberins - stimulate anterior pituitary– corticoliberin = corticotropin releasing factor
= CRF• stimulates release of adrenocorticotropin (ACTH)
and ß-lipotropin
NOMENCLATURE
• liberins - stimulate anterior pituitary– corticoliberin = corticotropin releasing factor
= CRF• stimulates release of adrenocorticotropin (ACTH)
and ß-lipotropin
– somatoliberin = growth hormone releasingfactor = GHRF
• stimulates release of growth hormone (somatotropin)
NOMENCLATURE• liberins (cont.)
– prolactoliberin = prolactin releasing factor = PRF
• stimulates release of prolactin
NOMENCLATURE• liberins (cont.)
– prolactoliberin = prolactin releasing factor = PRF
• stimulates release of prolactin
– gonadoliberin = gonadotropin releasing factor = GnRF& luteinizing hormone releasing factor
= LHRF• stimulates release of follicle stimulating hormone
(FSH) and luteinizing hormone (LH)
NOMENCLATURE
• liberins (cont.)– thyroliberin = thyrotropin releasing hormone
= TRH• stimulates release of thyrotropin
= thyroid stimulating hormone (TSH)
NOMENCLATURE• statins - inhibit release of hormones by
anterior pituitary
NOMENCLATURE• statins - inhibit release of hormones by
anterior pituitary– somatostatin
• inhibits release of growth hormone
NOMENCLATURE• statins - inhibit release of hormones by
anterior pituitary– somatostatin
• inhibits release of growth hormone
– prolactostatin = prolactin inhibiting factor = PIF
• inhibits release of prolactin
NOMENCLATURE• statins - inhibit release of hormones by
anterior pituitary– somatostatin
• inhibits release of growth hormone
– prolactostatin = prolactin inhibiting factor = PIF
• inhibits release of prolactin
– other statins corresponding to the remainingliberins probably also occur
PITUITARY HORMONES - TROPINS
• pituitary secretions stimulate theirrespective endocrine organs
PITUITARY HORMONES - TROPINS
• pituitary secretions stimulate theirrespective endocrine organs– thyroid, adrenals and gonads
PITUITARY HORMONES - TROPINS
• pituitary secretions stimulate theirrespective endocrine organs– thyroid, adrenals and gonads– these in turn produce hormones which target
specific organs
PITUITARY HORMONES - TROPINS
• pituitary secretions stimulate theirrespective endocrine organs– thyroid, adrenals and gonads– these in turn produce hormones which target
specific organs– the target cells must possess specific receptors
for the hormones
PITUITARY HORMONES - TROPINS
• pituitary secretions stimulate theirrespective endocrine organs– thyroid, adrenals and gonads– these in turn produce hormones which target
specific organs– the target cells must possess specific receptors
for the hormones• a combination of the density of receptors on the
target cells and the concentration of hormone in thecirculation will determine the effect of the hormoneon the target tissues
HORMONE TYPES
• divided into two broad classes depending onthe events which follow binding to thetarget tissue
HORMONE TYPES
• divided into two broad classes depending onthe events which follow binding to thetarget tissue– those which primarily affect the properties of
the plasma membrane itself

HORMONE TYPES
• divided into two broad classes depending onthe events which follow binding to thetarget tissue– those which primarily affect the properties of
the plasma membrane itself– those which enter the target cells

HORMONES WHICH INTERACT WITHTHE CELL MEMBRANE
• they do not enter cell but cause an effect by settingoff a cascade of reactions after binding– one of two different mechanisms may occur
HORMONES WHICH INTERACT WITHTHE CELL MEMBRANE
– stimulate adenyl cyclase, thus increaseintracellular levels of cAMP causing activationof specific protein kinases e.g. adrenalinee andglucagon (and many others)
HORMONES WHICH INTERACT WITHTHE CELL MEMBRANE
– stimulate adenyl cyclase, thus increaseintracellular levels of cAMP causing activationof specific protein kinases e.g. adrenaline andglucagon (and many others)
• or– alter membrane permeability
• e.g. adrenaline changes Ca++ flow into cells• insulin increases the permeability of some cells to
amino acids and glucose
HORMONES WHICH ENTER TARGETCELLS
• second group are taken into cell andtransported to nucleus
HORMONES WHICH ENTER TARGETCELLS
• second group are taken into cell andtransported to nucleus– they affect mRNA transcription and
subsequently synthesis of certain proteins• thyroid hormones and all steroids act in this way
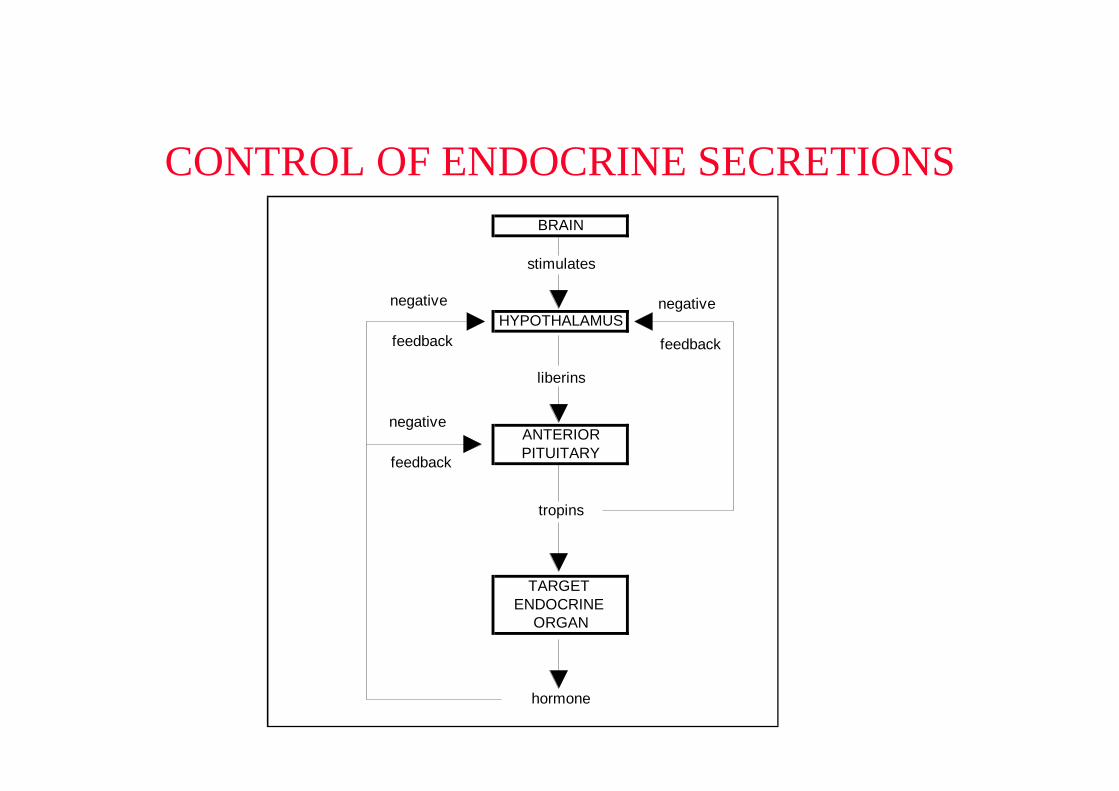
CONTROL OF ENDOCRINE SECRETIONSBRAIN
stimulates
HYPOTHALAMUS
liberins
ANTERIORPITUITARY
tropins
TARGET ENDOCRINE
ORGAN
hormone
negative
feedback
negative
feedback
negative
feedback
ENDOCRINE DISEASES
• either hypo-secretion or hyper-secretion canoccur
ENDOCRINE DISEASES
• either hypo-secretion or hyper-secretion canoccur– the abnormality can be of hypothalamic origin
• lack of liberins• or excess of liberins
ENDOCRINE DISEASES
• either hypo-secretion or hyper-secretion canoccur– the abnormality can be of hypothalamic origin
• lack of liberins• or excess of liberins
– or of pituitary origin• lack of tropins• or excess of tropins
ENDOCRINE DISEASES• hyposecretion
– is a result of lack of function of either thehypothalamus or the pituitary
ENDOCRINE DISEASES• hyposecretion
– is a result of lack of function of either thehypothalamus or the pituitary
– may be caused by• destruction of tissue by a tumor
ENDOCRINE DISEASES• hyposecretion
– is a result of lack of function of either thehypothalamus or the pituitary
– may be caused by• destruction of tissue by a tumor• infarction
ENDOCRINE DISEASES• hyposecretion
– is a result of lack of function of either thehypothalamus or the pituitary
– may be caused by• destruction of tissue by a tumor• infarction• surgery or irradiation

ENDOCRINE DISEASES• hyposecretion
– is a result of lack of function of either thehypothalamus or the pituitary
– may be caused by• destruction of tissue by a tumor• infarction• surgery or irradiation• genetic defect in synthesis or release of the hormone
ENDOCRINE DISEASES• hyposecretion
– is a result of lack of function of either thehypothalamus or the pituitary
– may be caused by• destruction of tissue by a tumor• infarction• surgery or irradiation• genetic defect in synthesis or release of the hormone• infection
ENDOCRINE DISEASES• hypersecretion
– may be a result of• loss of feedback control
ENDOCRINE DISEASES• hypersecretion
– may be a result of• loss of feedback control• a tumor of the hypothalamus or pituitary causing
overproduction of a hormone
ENDOCRINE DISEASES• hypersecretion
– may be a result of• loss of feedback control• a tumor of the hypothalamus or pituitary causing
overproduction of a hormone• ectopic production of a hormone
ENDOCRINE DISEASES• hypersecretion
– may be a result of• loss of feedback control• a tumor of the hypothalamus or pituitary causing
overproduction of a hormone• ectopic production of a hormone
• all of these diseases may affect secretion ofindividual hormones or may affect secretionof a number of hormones simultaneously
ENDOCRINE DISEASES
• laboratory investigations– assay hypothalamic secretions

ENDOCRINE DISEASES
• laboratory investigations– assay hypothalamic secretions
• this is specialist testing as the concentrations arevery low - tests are expensive
ENDOCRINE DISEASES
• laboratory investigations– assay hypothalamic secretions
• this is specialist testing as the concentrations arevery low - tests are expensive
– assay pituitary secretions• more commonly done
ASSAY OF PITUITARYSECRETIONS
• three questions arise
ASSAY OF PITUITARYSECRETIONS
• three questions arise– is the output by the anterior pituitary normal?
ASSAY OF PITUITARYSECRETIONS
• three questions arise– is the output by the anterior pituitary normal?– does the anterior pituitary have a normal
reserve capacity of hormone(s)?
ASSAY OF PITUITARYSECRETIONS
• three questions arise– is the output by the anterior pituitary normal?– does the anterior pituitary have a normal
reserve capacity of hormone(s)?– does hormone output respond to normal control
mechanisms?
ASSAY OF PITUITARYSECRETIONS
• normal output as measured by single plasmameasurements does not necessarily reflect acorrectly functioning anterior pituitary
ASSAY OF PITUITARYSECRETIONS
• normal output as measured by single plasmameasurements does not necessarily reflect acorrectly functioning anterior pituitary
• generally, the anterior pituitary function must beinvestigated by assessing its response to specificstimulation or suppression

ASSAY OF PITUITARYSECRETIONS
• normal output as measured by single plasmameasurements does not necessarily reflect acorrectly functioning anterior pituitary
• generally, the anterior pituitary function must beinvestigated by assessing its response to specificstimulation or suppression
• done by applying an appropriate dynamic functiontest
ASSAY OF PITUITARYSECRETIONS
• hormones are assayed by immunoassaymost commonly
ASSAY OF PITUITARYSECRETIONS
• hormones are assayed by immunoassaymost commonly– important to differentiate immunoreactivity
from biological activity
ASSAY OF PITUITARYSECRETIONS
• hormones are assayed by immunoassaymost commonly– important to differentiate immunoreactivity
from biological activity– problems encountered are
• cross-reactivity• non-specific interference
DYNAMIC FUNCTION TESTS
• 3 examples will be discussed
– ACTH and cortisol
– growth hormone
– triple function test
DYNAMIC TESTING OF ACTHSECRETION
• can be measured by immunoassay, butresults are unreliable, therefore cortisol ismeasured in preference
DYNAMIC TESTING OF ACTHSECRETION
• can be measured by immunoassay, butresults are unreliable, therefore cortisol ismeasured in preference– this is satisfactory because
• plasma cortisol levels directly reflect ACTH levels
DYNAMIC TESTING OF ACTHSECRETION
• can be measured by immunoassay, butresults are unreliable, therefore cortisol ismeasured in preference– this is satisfactory because
• plasma cortisol levels directly reflect ACTH levels• the hormone cascade effect means that small
quantities of ACTH are amplified to relatively largeamounts of cortisol
DYNAMIC TESTING OF ACTHSECRETION
• can be measured by immunoassay, butresults are unreliable, therefore cortisol ismeasured in preference– this is satisfactory because
• plasma cortisol levels directly reflect ACTH levels• the hormone cascade effect means that small
quantities of ACTH are amplified to relatively largeamounts of cortisol
• cortisol assay is quick and simple
REVISION - CORTISOL EFFECTS
• increases blood glucose• insulin antagonist
REVISION - CORTISOL EFFECTS
• increases blood glucose• insulin antagonist
– decreases glucose utilisation
REVISION - CORTISOL EFFECTS
• increases blood glucose• insulin antagonist
– decreases glucose utilisation– increases gluconeogenesis
REVISION - CORTISOL EFFECTS
• increases blood glucose• insulin antagonist
– decreases glucose utilisation– increases gluconeogenesis
• increases liver glycogen storage
REVISION - CORTISOL EFFECTS
• increases blood glucose• insulin antagonist
– decreases glucose utilisation– increases gluconeogenesis
• increases liver glycogen storage• increases fat mobilisation
DYNAMIC TESTING OF ACTHSECRETION cont.
• hyposecretion– if a lack of cortisol secretion is suspected, it
may be due to• adrenal insufficiency (where cortisol itself is not
synthesised even though ACTH secretion isadequate)
DYNAMIC TESTING OF ACTHSECRETION cont.
• hyposecretion– if a lack of cortisol secretion is suspected, it
may be due to• adrenal insufficiency (where cortisol itself is not
synthesised even though ACTH secretion isadequate)
• anterior pituitary insufficiency (lack of ACTH tostimulate the adrenals)
DYNAMIC TESTING OF ACTHSECRETION cont.
• adrenal insufficiency is checked usingsynacthen (synthetic form of thebiologically active portion of ACTH)
DYNAMIC TESTING OF ACTHSECRETION cont.
• adrenal insufficiency is checked usingsynacthen (synthetic form of thebiologically active portion of ACTH)– after injection cortisol levels should rise
significantly if the adrenals are functioningnormally
DYNAMIC TESTING OF ACTHSECRETION cont.
• to test whether there is adequate secretion ofACTH, a physiological stress is placed onthe patient
DYNAMIC TESTING OF ACTHSECRETION cont.
• to test whether there is adequate secretion ofACTH, a physiological stress is placed onthe patient– because stress ---> inc. CRF ---> inc. ACTH
---> inc. cortisol
DYNAMIC TESTING OF ACTHSECRETION cont.
• to test whether there is adequate secretion ofACTH, a physiological stress is placed onthe patient– because stress ---> inc. CRF ---> inc. ACTH
---> inc. cortisol• hypoglycaemia is produced by insulin injection
DYNAMIC TESTING OF ACTHSECRETION cont.
• to test whether there is adequate secretion ofACTH, a physiological stress is placed onthe patient– because stress ---> inc. CRF ---> inc. ACTH
---> inc. cortisol• hypoglycaemia is produced by insulin injection• the extent of the hypoglycaemia is assessed by
plasma glucose measurements and plasma cortisolmeasurements are performed at regular intervals
DYNAMIC TESTING OF ACTHSECRETION cont.
• to test whether there is adequate secretion ofACTH, a physiological stress is placed onthe patient– because stress ---> inc. CRF ---> inc. ACTH
---> inc. cortisol• hypoglycaemia is produced by insulin injection• the extent of the hypoglycaemia is assessed by
plasma glucose measurements and plasma cortisolmeasurements are performed at regular intervals
• the plasma cortisol should rise significantly within2 hours if the anterior pituitary is normal
DYNAMIC TESTING OF ACTHSECRETION cont.
• high circulating cortisol levels may be dueto– adrenal hyperplasia
DYNAMIC TESTING OF ACTHSECRETION cont.
• high circulating cortisol levels may be dueto– adrenal hyperplasia
• due to excess stimulation of adrenals by ACTH(control is set too high)
DYNAMIC TESTING OF ACTHSECRETION cont.
• high circulating cortisol levels may be dueto– adrenal hyperplasia
• due to excess stimulation of adrenals by ACTH(control is set too high)
• adrenal tumor - lack of feed back inhibition
DYNAMIC TESTING OF ACTHSECRETION cont.
• high circulating cortisol levels may be dueto– adrenal hyperplasia
• due to excess stimulation of adrenals by ACTH(control is set too high)
• adrenal tumor - lack of feed back inhibition
– excess ACTH secretion by the anterior pituitary
DYNAMIC TESTING OF ACTHSECRETION cont.
• high circulating cortisol levels may be dueto– adrenal hyperplasia
• due to excess stimulation of adrenals by ACTH(control is set too high)
• adrenal tumor - lack of feed back inhibition
– excess ACTH secretion by the anterior pituitary– ectopic ACTH production
INVESTIGATION OF HIGHCIRCULATING CORTISOL
• negative feedback control should suppressACTH secretion (and hence cortisol levels)when cortisol levels are high
INVESTIGATION OF HIGHCIRCULATING CORTISOL
• negative feedback control should suppressACTH secretion (and hence cortisol levels)when cortisol levels are high– this can be assessed by the dexamethasone
suppression test
INVESTIGATION OF HIGHCIRCULATING CORTISOL
• negative feedback control should suppressACTH secretion (and hence cortisol levels)when cortisol levels are high– this can be assessed by the dexamethasone
suppression test– dexamethasone is a synthetic steroid with about
25 times the potency of cortisol
DEXAMETHASONE SUPPRESSIONTEST
• interpretation– high circulating cortisol levels may be due to
simple obesity
DEXAMETHASONE SUPPRESSIONTEST
• interpretation– high circulating cortisol levels may be due to
simple obesity• a low dose of dexamethasone will suppress the
cortisol level in this case
DEXAMETHASONE SUPPRESSIONTEST
• interpretation– high circulating cortisol levels may be due to
simple obesity• a low dose of dexamethasone will suppress the
cortisol level in this case
– high circulating cortisol may be due to anteriorpituitary hyperplasia (i.e. causing excess ACTHproduction)
DEXAMETHASONE SUPPRESSIONTEST
• interpretation– high circulating cortisol levels may be due to
simple obesity• a low dose of dexamethasone will suppress the
cortisol level in this case
– high circulating cortisol may be due to anteriorpituitary hyperplasia (i.e. causing excess ACTHproduction)
• a low dexamethasone dose will not suppress thecortisol level, however a higher dose will
DEXAMETHASONE SUPPRESSIONTEST
• interpretation– high circulating cortisol levels may be due to
simple obesity• a low dose of dexamethasone will suppress the
cortisol level in this case
– high circulating cortisol may be due to anteriorpituitary hyperplasia (i.e. causing excess ACTHproduction)
• a low dexamethasone dose will not suppress thecortisol level, however a higher dose will
• this condition is Cushing’s syndrome
DEXAMETHASONE SUPPRESSIONTEST
• if there is no suppression even at the higherdose, the excess cortisol production is dueto– adrenal hyperplasia (excess cortisol production
even without the stimulation of ACTH)
DEXAMETHASONE SUPPRESSIONTEST
• if there is no suppression even at the higherdose, the excess cortisol production is dueto– adrenal hyperplasia (excess cortisol production
even without the stimulation of ACTH)– ectopic ACTH production

DEXAMETHASONE SUPPRESSIONTEST
• if there is no suppression even at the higherdose, the excess cortisol production is dueto– adrenal hyperplasia (excess cortisol production
even without the stimulation of ACTH)– ectopic ACTH production
• these two alternatives could be differentiated bydirect plasma ACTH measurement

DEXAMETHASONE SUPPRESSIONTEST
• if there is no suppression even at the higherdose, the excess cortisol production is dueto– adrenal hyperplasia (excess cortisol production
even without the stimulation of ACTH)– ectopic ACTH production
• these two alternatives could be differentiated bydirect plasma ACTH measurement
• in the former, ACTH will be low
DEXAMETHASONE SUPPRESSIONTEST
• if there is no suppression even at the higherdose, the excess cortisol production is dueto– adrenal hyperplasia (excess cortisol production
even without the stimulation of ACTH)– ectopic ACTH production
• these two alternatives could be differentiated bydirect plasma ACTH measurement
• in the former, ACTH will be low• in the latter, ACTH will be high

GROWTH HORMONE
• growth hormone levels are affectedmarkedly by– food, exercise, sleep & stress
GROWTH HORMONE
• growth hormone levels are affectedmarkedly by– food, exercise, sleep & stress– the concentration changes significantly with
these factors
GROWTH HORMONE
• growth hormone levels are affectedmarkedly by– food, exercise, sleep & stress– the concentration changes significantly with
these factors– it is not possible to distinguish normal from
deficient with spot tests
GROWTH HORMONE
• growth hormone levels are affectedmarkedly by– food, exercise, sleep & stress– the concentration changes significantly with
these factors– it is not possible to distinguish normal from
deficient with spot tests– dynamic testing is essential
DYNAMIC TESTING OF GROWTHHORMONE SECRETION
• stimulation of growth hormone secretion
DYNAMIC TESTING OF GROWTHHORMONE SECRETION
• stimulation of growth hormone secretion– these tests are designed to assess the pituitary
reserves of growth hormone (GH)
DYNAMIC TESTING OF GROWTHHORMONE SECRETION
• stimulation of growth hormone secretion– these tests are designed to assess the pituitary
reserves of growth hormone (GH)• they are generally performed when a deficiency of
GH is suspected
DYNAMIC TESTING OF GROWTHHORMONE SECRETION cont.
– sleep• deep sleep causes a reproducible marked elevation
in plasma GH levels, particularly in children andadolescents
DYNAMIC TESTING OF GROWTHHORMONE SECRETION cont.
– sleep• deep sleep causes a reproducible marked elevation
in plasma GH levels, particularly in children andadolescents
• blood samples are obtained by in-dwelling catheterwhilst sleeping subject is monitored by EEG
DYNAMIC TESTING OF GROWTHHORMONE SECRETION cont.
– sleep• deep sleep causes a reproducible marked elevation
in plasma GH levels, particularly in children andadolescents
• blood samples are obtained by in-dwelling catheterwhilst sleeping subject is monitored by EEG
• samples collected every 30 min. for 3 - 4 hours afteronset of sleep
DYNAMIC TESTING OF GROWTHHORMONE SECRETION cont.
– sleep• deep sleep causes a reproducible marked elevation
in plasma GH levels, particularly in children andadolescents
• blood samples are obtained by in-dwelling catheterwhilst sleeping subject is monitored by EEG
• samples collected every 30 min. for 3 - 4 hours afteronset of sleep
• the spurt of GH generally occurs within 30 - 90 min.of sleep onset and lasts for 1 - 2 hours
DYNAMIC TESTING OF GROWTHHORMONE SECRETION cont.
– sleep• deep sleep causes a reproducible marked elevation
in plasma GH levels, particularly in children andadolescents
• blood samples are obtained by in-dwelling catheterwhilst sleeping subject is monitored by EEG
• samples collected every 30 min. for 3 - 4 hours afteronset of sleep
• the spurt of GH generally occurs within 30 - 90 min.of sleep onset and lasts for 1 - 2 hours
• the sleep peak is absent in both deficiency andacromegaly (due to hypersecretion)
DYNAMIC TESTING OF GROWTHHORMONE SECRETION cont.
• exercise– hard physical exercise stimulates a marked
increase in GH in normal individuals
DYNAMIC TESTING OF GROWTHHORMONE SECRETION cont.
• exercise– hard physical exercise stimulates a marked
increase in GH in normal individuals– basal GH levels are determined and patients are
given a standardised workload using a bicycleergometer
DYNAMIC TESTING OF GROWTHHORMONE SECRETION cont.
• exercise– hard physical exercise stimulates a marked
increase in GH in normal individuals– basal GH levels are determined and patients are
given a standardised workload using a bicycleergometer
– the normal response is a rise in GH levels toabout 10 times basal levels
DYNAMIC TESTING OF GROWTHHORMONE SECRETION cont.
• arginine load– certain amino acids, including arginine,
stimulate GH release
DYNAMIC TESTING OF GROWTHHORMONE SECRETION cont.
• arginine load– certain amino acids, including arginine,
stimulate GH release• basal levels are determined, arginine infusion is
begun and samples are taken at specified times.
DYNAMIC TESTING OF GROWTHHORMONE SECRETION cont.
• arginine load– certain amino acids, including arginine,
stimulate GH release• basal levels are determined, arginine infusion is
begun and samples are taken at specified times.• normal individuals show a rise in GH levels to about
10 times the basal level
DYNAMIC TESTING OF GROWTHHORMONE SECRETION cont.
• insulin hypoglycaemia– one effect of GH is to increase the blood
glucose level (as a response to hypoglycaemia)
DYNAMIC TESTING OF GROWTHHORMONE SECRETION cont.
• insulin hypoglycaemia– one effect of GH is to increase the blood
glucose level (as a response to hypoglycaemia)– therefore induced hypoglycaemia causes a
release of GH in the normal individual (to about10 times basal level)
DYNAMIC TESTING OF GROWTHHORMONE SECRETION cont.
• insulin hypoglycaemia– one effect of GH is to increase the blood
glucose level (as a response to hypoglycaemia)– therefore induced hypoglycaemia causes a
release of GH in the normal individual (to about10 times basal level)
– little or no rise is seen in the deficientindividual
DYNAMIC TESTING OF GROWTHHORMONE SECRETION cont.
• suppression
DYNAMIC TESTING OF GROWTHHORMONE SECRETION cont.
• suppression– the suppression tests are designed to
differentiate those patients with high circulatinglevels of GH due to a pathological cause fromthose with high levels due to stress or othernon-pathological causes
DYNAMIC TESTING OF GROWTHHORMONE SECRETION cont.
• glucose suppression test– hyperglycaemia will suppress GH levels in the
normal individual
DYNAMIC TESTING OF GROWTHHORMONE SECRETION cont.
• glucose suppression test– hyperglycaemia will suppress GH levels in the
normal individual– suppression to within reference range or to
undetectable levels indicates a normal response
DYNAMIC TESTING OF GROWTHHORMONE SECRETION cont.
• glucose suppression test– hyperglycaemia will suppress GH levels in the
normal individual– suppression to within reference range or to
undetectable levels indicates a normal response– in acromegaly and gigantism there is a failure
to suppress significantly
TRIPLE FUNCTION TEST
• A deficiency of a single pituitary hormoneis rare
TRIPLE FUNCTION TEST
• A deficiency of a single pituitary hormoneis rare– clinical suggestion of pituitary dysfunction
generally requires that the pituitary reserve ofall hormones be evaluated
TRIPLE FUNCTION TEST
• A deficiency of a single pituitary hormoneis rare– clinical suggestion of pituitary dysfunction
generally requires that the pituitary reserve ofall hormones be evaluated
– this can be accomplished by combining severalof the stimulatory dynamic function tests in amodified form
TRIPLE FUNCTION TEST
• procedure– blood samples are taken by in-dwelling catheter

TRIPLE FUNCTION TEST
• procedure– blood samples are taken by in-dwelling catheter– basal levels of glucose, cortisol, GH, TSH, LH,
FSH and PRL are measured
TRIPLE FUNCTION TEST
• procedure– blood samples are taken by in-dwelling catheter– basal levels of glucose, cortisol, GH, TSH, LH,
FSH and PRL are measured– insulin, TRH (thyroliberin) and GnRH
(gonadoliberin) are injected IV simultaneously
TRIPLE FUNCTION TEST
• procedure– blood samples are taken by in-dwelling catheter– basal levels of glucose, cortisol, GH, TSH, LH,
FSH and PRL are measured– insulin, TRH (thyroliberin) and GnRH
(gonadoliberin) are injected IV simultaneously– the above hormones (and glucose) are measured
at 30 min. intervals for 2 hours
TRIPLE FUNCTION TEST cont.
• procedure cont.– glucose is measured to ensure an adequate
hypoglycaemia has been induced to permitinterpretation of cortisol levels in response tohypoglycaemia
TRIPLE FUNCTION TEST cont.
• procedure cont.– glucose is measured to ensure an adequate
hypoglycaemia has been induced to permitinterpretation of cortisol levels in response tohypoglycaemia
– synacthen may be injected and cortisol levelsmeasured at 30 and 60 min
TRIPLE FUNCTION TEST cont.
• procedure cont.– glucose is measured to ensure an adequate
hypoglycaemia has been induced to permitinterpretation of cortisol levels in response tohypoglycaemia
– synacthen may be injected and cortisol levelsmeasured at 30 and 60 min
– this approach allows all the secretions of thepituitary to be assessed at one time on the patientwithout subjecting them to multiple testing
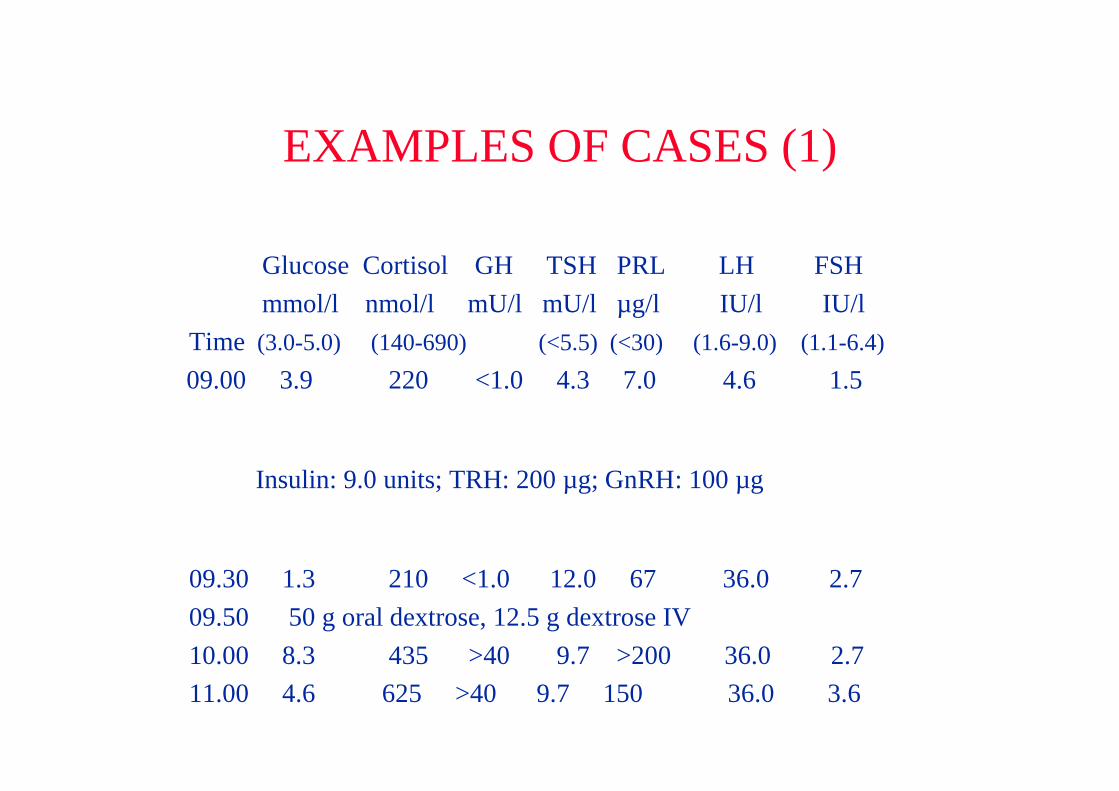
EXAMPLES OF CASES (1)
Glucose Cortisol GH TSH PRL LH FSH mmol/l nmol/l mU/l mU/l µg/l IU/l IU/l
Time (3.0-5.0) (140-690) (<5.5) (<30) (1.6-9.0) (1.1-6.4)
09.00 3.9 220 <1.0 4.3 7.0 4.6 1.5
Insulin: 9.0 units; TRH: 200 µg; GnRH: 100 µg
09.30 1.3 210 <1.0 12.0 67 36.0 2.7 09.50 50 g oral dextrose, 12.5 g dextrose IV 10.00 8.3 435 >40 9.7 >200 36.0 2.7 11.00 4.6 625 >40 9.7 150 36.0 3.6
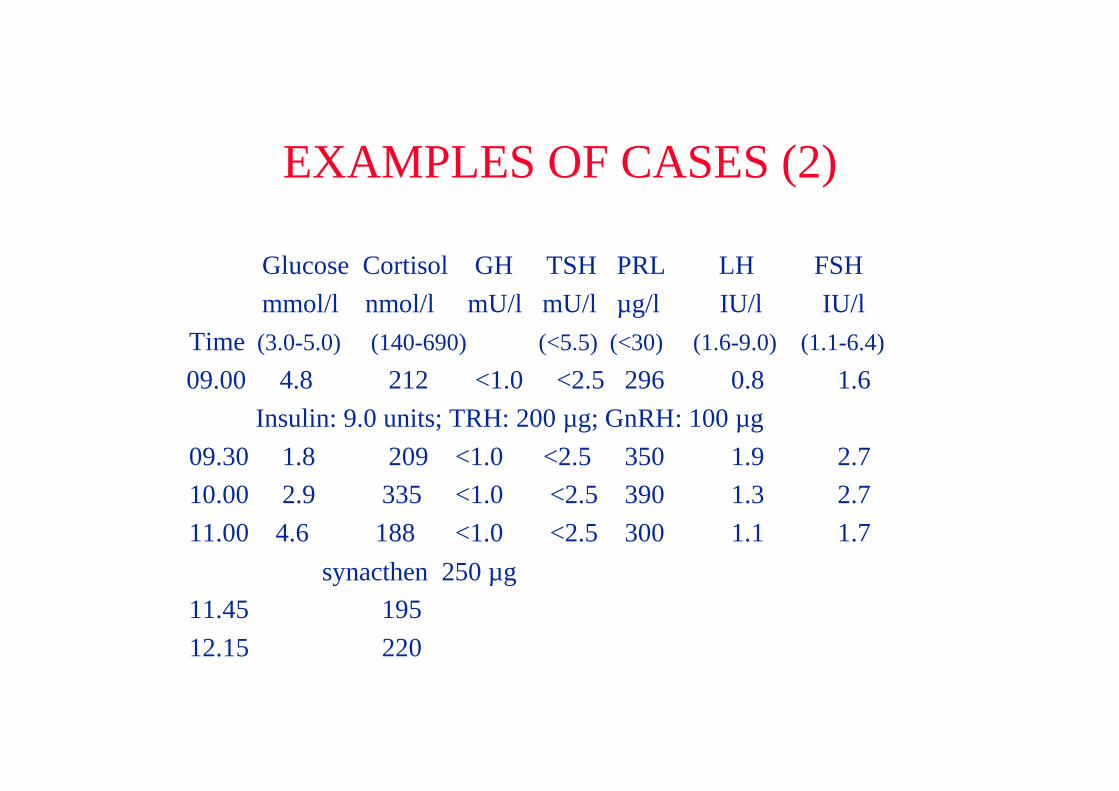
EXAMPLES OF CASES (2)
Glucose Cortisol GH TSH PRL LH FSH mmol/l nmol/l mU/l mU/l µg/l IU/l IU/l
Time (3.0-5.0) (140-690) (<5.5) (<30) (1.6-9.0) (1.1-6.4)
09.00 4.8 212 <1.0 <2.5 296 0.8 1.6 Insulin: 9.0 units; TRH: 200 µg; GnRH: 100 µg
09.30 1.8 209 <1.0 <2.5 350 1.9 2.7 10.00 2.9 335 <1.0 <2.5 390 1.3 2.7 11.00 4.6 188 <1.0 <2.5 300 1.1 1.7
synacthen 250 µg 11.45 195 12.15 220
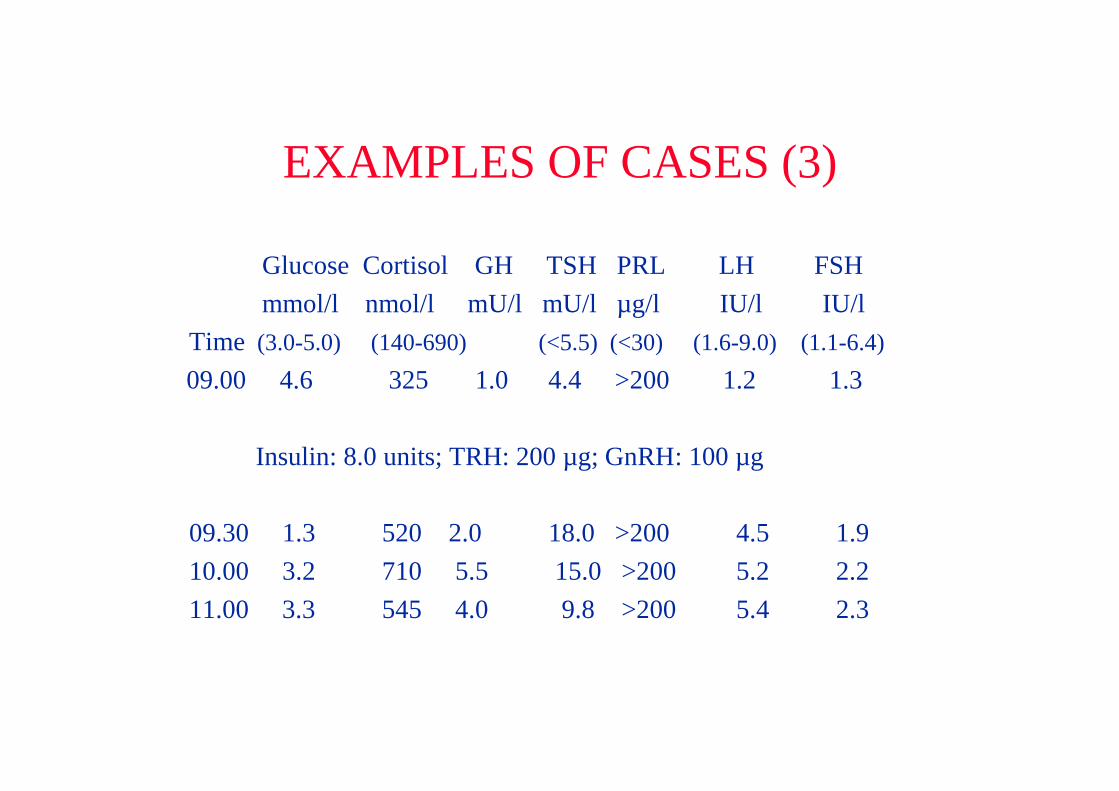
EXAMPLES OF CASES (3)
Glucose Cortisol GH TSH PRL LH FSH mmol/l nmol/l mU/l mU/l µg/l IU/l IU/l
Time (3.0-5.0) (140-690) (<5.5) (<30) (1.6-9.0) (1.1-6.4)
09.00 4.6 325 1.0 4.4 >200 1.2 1.3
Insulin: 8.0 units; TRH: 200 µg; GnRH: 100 µg
09.30 1.3 520 2.0 18.0 >200 4.5 1.9 10.00 3.2 710 5.5 15.0 >200 5.2 2.2 11.00 3.3 545 4.0 9.8 >200 5.4 2.3
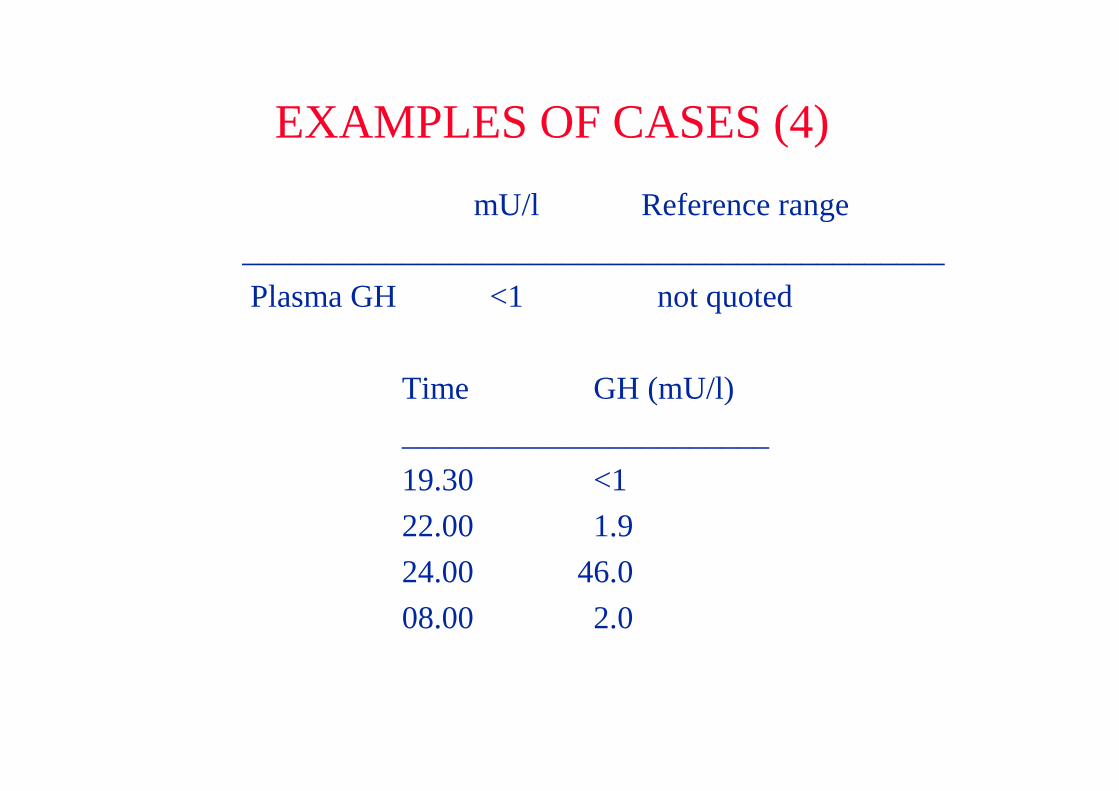
EXAMPLES OF CASES (4)
mU/l Reference range____________________________________________ Plasma GH <1 not quoted
Time GH (mU/l)_______________________19.30 <122.00 1.924.00 46.008.00 2.0
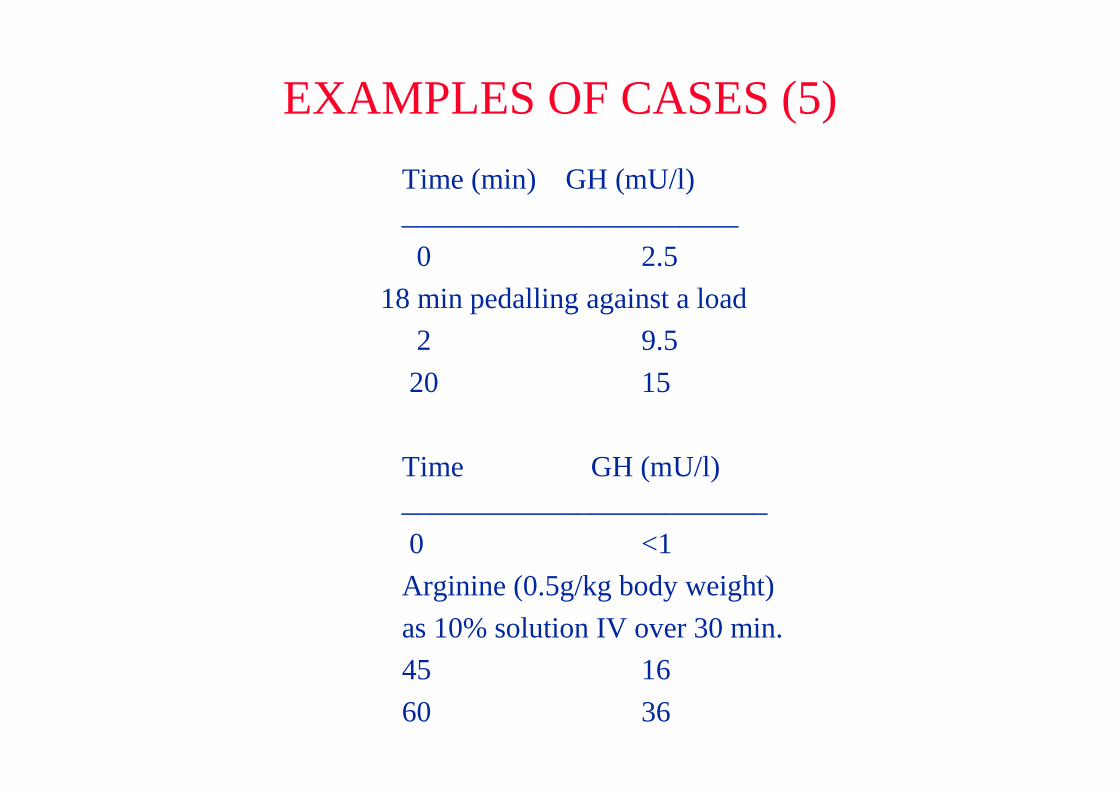
EXAMPLES OF CASES (5)Time (min) GH (mU/l)_______________________ 0 2.5
18 min pedalling against a load 2 9.5 20 15
Time GH (mU/l)_________________________ 0 <1Arginine (0.5g/kg body weight)as 10% solution IV over 30 min.45 1660 36
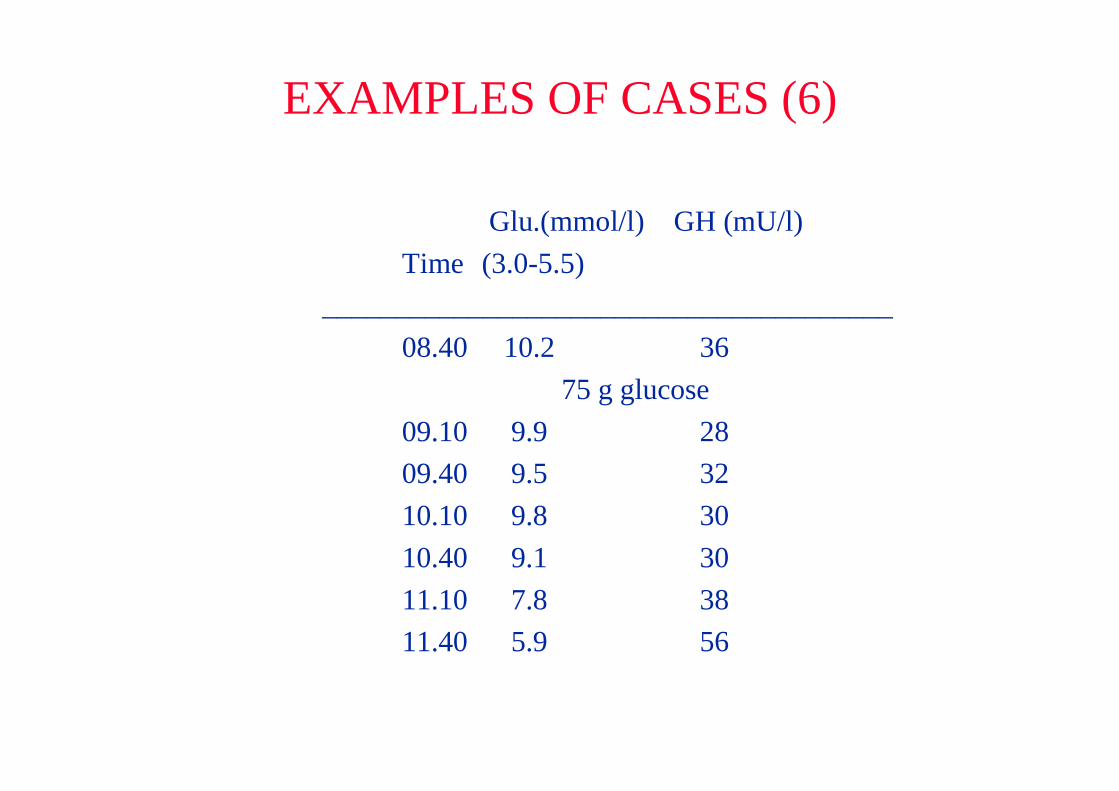
EXAMPLES OF CASES (6)
Glu.(mmol/l) GH (mU/l)Time (3.0-5.5)
_______________________________________08.40 10.2 36
75 g glucose09.10 9.9 2809.40 9.5 3210.10 9.8 3010.40 9.1 3011.10 7.8 3811.40 5.9 56