enabling stroke victims to interact with a microcomputer - a comparison of input devices
TRANSCRIPT

Inr. Disahil. Srudies. 10, 73-80, @ Eular Publishers
Enabling stroke victims to interact with a microcomputer - a comparison of input devices
BRIAN PETHERAM
Department of Computer Studies and Mathematics, Bristol Polytechnic, Coldharbour Lane, Frenchay, Bristol BS16 IQY, Great Britain
Revised paper accepted for publication: Correspondence to: Mr B. Petheram, Department of Computer Studies and Mathematics, Bristol Polytechnic,
August 1987
Coldharbour Lane, Frenchay, Bristol BS16 IQY, Great Britain
Key words
Summary Five commonly available input devices were evaluated with respect to the facility with which aphasic stroke victims could use them to interact with a microcomputer. The tests by which they were assessed were content-free abstractions from the underlying physical structures of language stimulation exercises. The devices tested were the mouse, joystick, tracker ball, concept keyboard, and touch screen. Success rates, times, and subjective preference were all recorded. The tracker ball was found to be best on success rate and subjective preference.
Input device - Microcomputer - Stroke
Introduction
CONTEXT This study was undertaken as part of a larger project, the aim of which is to investigate the potential contribution of microcomputers to enabling speech- and language- handicapped stroke victims to self-administer therapy in their own homes under the indirect supervision of a qualified speech therapist. This activity would typically take place in the periods between therapist contact as an integrated part of the therapy process. The development and progressive enhancement and evaluation of such a system is intended to establish whether such a process is effective, and the necessary characteristics of such a system.
One of the common effects of a stroke is that the victim loses some degree of physical control over one side of the body. This effect can range from a slight impairment to complete hemiplegia. The problem is worsened by the fact that speech and language handicap is associated with injuries to the left hemisphere of the brain and therefore the right side of the body, the dominant side for most people, is the one affected.
In order to enable such a person to benefit from using a microcomputer it is necessary that the patient is able to physically interact with the machine, usually via a VDU screen. The standard mechanism for interaction with a computer is usually a ‘QWERTY’ keyboard, similar to that of an electric typewriter. This is a skill which needs considerable practice to master, even for the able-bodied. Therefore it was decided that the first task of the project should be to establish the most suitable alternative input device, bearing in mind the characteristics of stroke victims, and the ways in which they would need to interact with the computer system in order to achieve an improvement in their condition.
AIMS OF THIS STUDY There are many alternative input devices now available for use with microcomputers, which have the potential to enable people of limited physical dexterity to interact with a microcomputer. The primary aim of this study is to assess which of these devices is the most suitable for stroke victims to use with those types of exercise which are typically encountered by the patient in the remedial
process. It is hoped that the work reported in this paper will be of assistance to those interested in other areas, since the problem addressed by this work is a physical one which is by no means confined to stroke victims.
There have been previous comparative studies done on such devices but it is believed that this work differs in two major ways: previous studies have all used able-bodied subjects: air traffic controllers; ’ schoolchildren;’ ~ndergraduates;~ and the range of devices actually used in the tests or preliminarily assessed is wider. Other work has been implicitly or explicitly ‘productivity-oriented’; by that it is meant that the interest in the devices has been based on their potential for improving the subjects’ performance. Whilst speed and error rate are the main parameters that can be measured, this study is concerned mainly with providing stroke victims with the most effective and comfortable interface to the therapy system.
The experiment has been designed as an attempt to scientifically assess the relative merits of a range of input devices for the purposes outlined above. Therefore the test software incorporates facilities for measuring the technical criteria of error rate and speed of response. However the nature of the main project calls for some evaluation of the subjective appeal of the various devices, since they will be used voluntarily and without supervi- sion. It is felt that this is a fundamentally different situation from commercial and formal educational en- vironments in which considerations based on ‘production rationality’ may be more pertinent. Therefore an attempt has been made to assess the relative subjective appeal of the devices. In this context speed of response is primarily an indicator of ease of use. It is, of course, vital that the error rate is minimized in order to avoid damaging the patients’ motivation, as well as for accurate recording of performance.
APPROACH
Method
EQUIPMENT Due to the nature of the main project there were some constraints on the choice of equipment. The anticipated mode of use of the system - one set of hardware per
73
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mcg
ill U
nive
rsity
on
10/3
0/14
For
pers
onal
use
onl
y.

Int. Disabil. Studies. 1988: vol. 10. no. 2
patient, each set being exclusively used by that patient for a considerable length of time - means that any treatment centre using the system will need to purchase a number of sets of hardware. .Therefore it is necessary that the total cost of the system hardware should be as low as possible consistent with acceptable performance.
Host computer and VDU Because of the nature of the application of the overall project it was important that the overall cost of the system should be less than f1000. Therefore the host computer should not cost more than f500 if adequate provision is allowed for peripherals. The machine chosen was the Acorn BBC model B. This machine has several advan- tages over other machines in its price range. Most relevant to this project it has comprehensive provision of input and output facilities enabling the connection of most types of device. Also the ‘BEEB’ is the dominant machine in the education and therapy fields, and so there are more input devices available for it than for any comparable machine. For the purposes of this study the results are applicable to virtually any other microcompu- ter, since only a small proportion of the processing power is used and most devices are marketed on the basis of being adaptable for a range of machines.
The video display terminal used was the 14 inch Microvitec medium-resolution VDU. This was selected for reasons of cost and availability.
Devices There are a great many input devices available for the BBC micro, many of which seem to have some potential for use with physically handicapped users. In order to select a sample for evaluation it was necessary to apply some criteria. Perhaps the most important was that the device should be reasonably robust and reliable. Also it was necessary that the equipment used should be widely and readily available. During the search for suitable input devices many were found that appeared to be suitable for consideration, but on further investigation it was found that they were produced on a very small scale (often literally in a garden shed) and were therefore only available in limited quantities.
There are also many input devices which have been developed to assist people more profoundly handicapped than most stroke victims, including simple switches, light- wand helmets, and eye-focus-dependent devices. These devices were not included because it is desirable that the patients should make full use of whatever physical abilities they have. Speech input technology was con- sidered but not tested, because it is felt that it is not sufficiently developed in terms of ease of use and reliability; and because some of the relevant exercises test spatial awareness; therefore physical devices are arguably more suitable.
The devices that were chosen for the experiment fulfilled all the above criteria and are considered to be a representative selection of the main generic types of input devices currently available for use with microcomputers. The devices chosen are illustrated in Figure 1.
The mouse This device is becoming increasingly com- mon as a secondary input device for business micros. It consists of a small box resting on a ball-bearing. As the box is held in one hand, and is moved over a flat surface, the ball-bearing rotates. This movement is reflected in the movement of a cursor on the VDU screen. There are up to three buttons on the front of the mouse, over which the fingers naturally rest. Indication of the cursor reaching a desired position is given by pressing one of these buttons. The example used in the tests was the AMX Mouse, and all three buttons were programmed to give a similar response.
74
Thejoystick The joystick is one of the most familiar and well-established input devices, partly because of its widespread use with video games. Like the mouse, movement of the stick controls the movement of a cursor on the screen. There is also a button to indicate when the cursor is at a desired position. In the preliminary trials of devices the positional relationship between the stick and the ‘fire’ button was found to be crucial. If they were widely separated it required considerable dexterity to hold the stick still whilst pressing the button. This problem occurs if the user only has the use of one hand. The example used in the tests was the Clares Beebstick by Micrex.
The touchpad The touchpad consists of a tablet, usually of A4 or A3 size. The surface of the tablet is pressure- sensitive and is divided into 128 or 256 distinct squares. The device is usually used with an overlay sheet which is a representation of the screen image. The user makes a choice from alternatives on the screen by pressing the overlay in the equivalent position. A major drawback of this device for the application of the overall project is that the overlays need to be changed every time the structure of the screen image is changed. It was decided to include this device in the tests because it is widely used in situations where the patient or pupil, etc., is under the supervision of a therapist or teacher. Thus its inclusion will hopefully make this experiment of wider interest and relevance. The device used in the tests was the Star Microterminals Concept Keyboard, A4 size.
The tracker ball The tracker ball, also known as the roller ball, is basically a mouse turned upside-down. The ball is set in a firm base and the ball is large enough for it to be conveniently rotated by the fingers or the palm of the hand, the base remaining in one position. There are up to three buttons close to the ball which can be programmed to indicate a choice being made. The device used in the tests was the Marconi RB2.
The touch screen A touch screen consists of a frame which is attached to the VDU screen and a means of determining the position of any object that touches the screen. This is normally implemented either by a touch- sensitive membrane or by infra-red beams. The touch screen used in the tests was the Microvitec Touchtec 501, which uses infra-red beams.
TESTS The device should enable the user to interact with the computer over the whole range of exercises which a therapist is likely to require the patient to undertake. Thus the key factor in simulating such interaction was thought to be the basic pattern of the screen design. In order to ensure that the tests covered the range of likely interactions a study was made of a wide range of sources of material for aphasia therapy. From this survey nine underlying structures for the ‘physical’ design of linguis- tic tasks were identified. These were:
1. Choosing from up to three alternatives. 2. Sorting mixed-up sentences. 3. Picking letters from an alphabet and making a word. 4. Pointing to a picture or part of a picture. 5 . Picking a word from a sentence or paragraph. 6. Choosing from a large group of words. 7. Simple arithmetic. 8. Choosing from a matrix. 9. Choosing from a menu.
The next stage was to translate these underlying struc- tures into patterns that would correlate to the way the
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mcg
ill U
nive
rsity
on
10/3
0/14
For
pers
onal
use
onl
y.

PETHERAM: Stroke victims and the comDuter
Mouse
Touchpad
Touch Screen
Joystick
Tracker Ball
Figure 1 Input devices
75
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mcg
ill U
nive
rsity
on
10/3
0/14
For
pers
onal
use
onl
y.

Inr. Dbabil. Studies. 1988; vol. 10. no. 2
exercises would be presented on a VDU screen. During this process it was found that one screen pattern could represent more than one structure. This was so in three cases: 2 and 5 ; 7 and 9; 6 and 8. Thus the number of tests necessary to establish usability was reduced to six. The relationship between tests and structures is shown in Table 1.
Table I
Test Structure Test Structure
I 1 4 4 2 3 5 6.8 3 2.5 6 7 3
It was felt to be important that the tests should be as far as possible content-free, in the sense that the only effort necessary for the patient to make a correct choice should be the physical indication of the required element of the pattern on the screen. This was implemented by express- ing the pattern in the form of blocks, all of which were yellow except for the target block, which was red. Those colours were chosen because they are unlikely to be confused, even by people with visual defects. The tests are shown in Figure 2. They are straightforward apart from tests 2 and 3, in which the subject had to select a block from the top group and then from the bottom group; and test 6 in which the three patterns were presented individually in random order and in random positions on the screen.
SUBJECT'S The full diet of tests was undertaken by 12 subjects. Nine of these had suffered strokes, and three were volunteers of a similar age group (strokes usually affect people who are over 40 and a large proportion of sufferers are 60 +), who were included as a control. The controls were
Test 1
Test 3
Test 5
Figure 2 Test layouts
76
Test 2
Test 4
Test 6
included in case the results were such that the needs of stroke victims were special in any unanticipated way. The stroke victims were either inpatients or outpatients at Frenchay Hospital, and the controls were volunteer therapy assistants or nurses. One of the most relevant attributes of the stroke group was thought to be the degree of physical handicap suffered as a result of the stroke. In order to ensure that the group covered the range of disability a Barthel Test' was administered to each subject prior to testing. The Barthel Test identifies three levels of handicap: mild, moderate, and severe. Three stroke victims in each group were tested. The other attributes recorded were the subject's Functional Communication Profile (FCP),* a measure of communi- cative ability, and age. Some relevant characteristics of the subjects are set out in Table 2.
Table 2 Subjects
Subject ARe Sex Borthel FCP
I 2 3 4 5 6 7 8 9
ControLF 10 I I 12
77 80 91 46 76 a4 48 67 41
64 50 59
M M F F M F M M M
F F F
9 81 13 40 10 74 18 90 19 54 19 85 9 84
13 56 9 47
NA NA NA NA NA NA
N.B. None of the subjects had any known perceptual deficits.
CONDUCT OF TESTS All the tests were personally administered by the author, and took place between the hours of 10 a.m. and 4 p.m. A pilot study was conducted with one stroke victim to establish the level of guidance and practice that would be necessary. Undertaking the full range of tests took an average of 1.5-2 hours. In order to minimize the problem of fatigue it was emphasized to the subjects that they could stop at any time if they were tired, thus the tests were split into as many as three sessions. In order to balance the effect of familiarization the order of presen- tation of the devices was varied according to a heuristic algorithm. Each exercise was attempted 10 times by each subject with each device. Thus the total number of tries per subject was 300 and the total number of tries in the experiment was 3600 (720 per device).
Before the results were recorded the subject was encouraged to practise with each device. Test 1 was used for initial familiarization, and test 2 to ensure that the subject was ready for the more difficult tests. The way of using each device was explained to the patient, and it was demonstrated by the author. No results were taken until the subject and the author agreed that it was appropriate. The times and error rates were automatically recorded by the software.
After the subject had completed all the tests he or she was asked to evaluate the comparative appeal of the five devices on the form shown in Figure 3. Because of the communication problems of some of the subjects a discussion of the meaning of the form was often necessary. The form itself was designed with these problems in mind; hence the use of pictograms. Whilst the problems in attitudinal surveys are well established, the prime purpose of the experiment was such that the patients' opinion of the comparative merits of the devices must be accorded due significance.
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mcg
ill U
nive
rsity
on
10/3
0/14
For
pers
onal
use
onl
y.
P E T H E R A M : Stroke victims and the computer
3
2
How would you feel i t this device was the one that you had to use with the computer?
~~ ~
Concept Keyboard
Tracker Ball 1
wouldn't unhappy wouldn't happy very use it mind happy
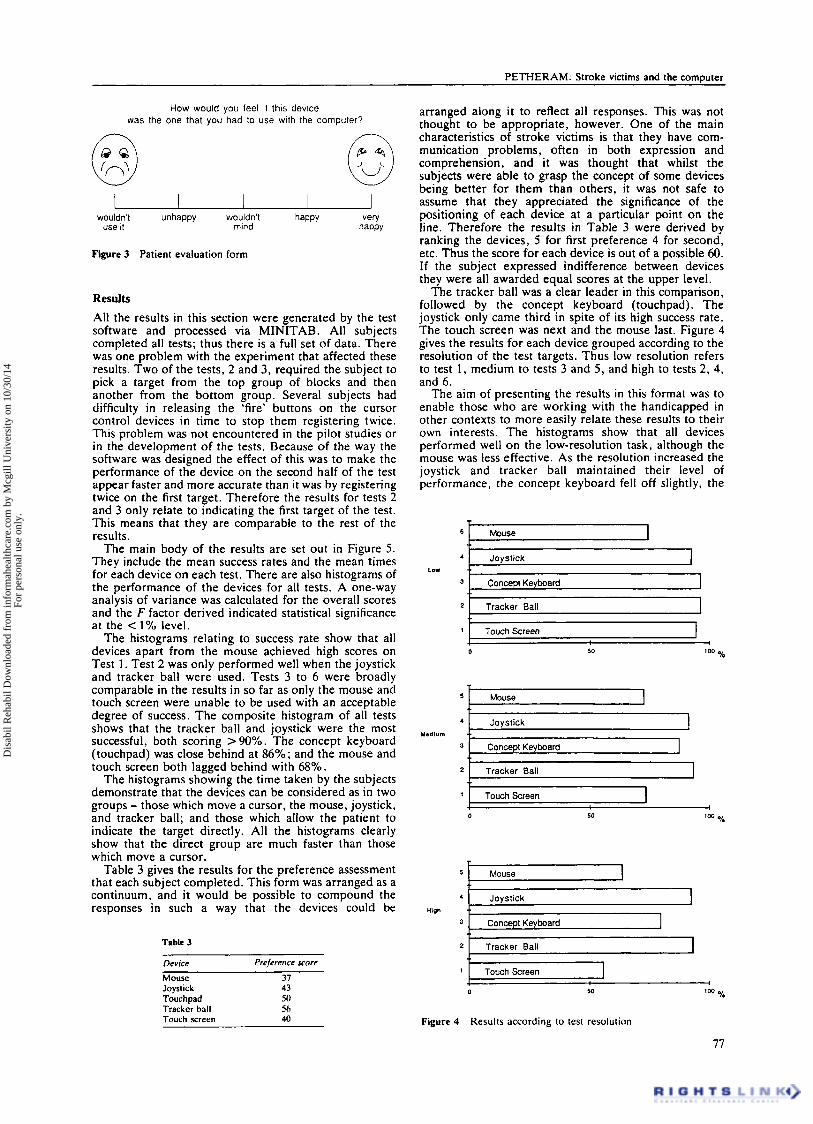
Figure 3 Patient evaluation form
Results All the results in this section were generated by the test software and processed via MINITAB. All subjects completed all tests; thus there is a full set of data. There was one problem with the experiment that affected these results. Two of the tests, 2 and 3, required the subject to pick a target from the top group of blocks and then another from the bottom group. Several subjects had difficulty in releasing the 'fire' buttons on the cursor control devices in time to stop them registering twice. This problem was not encountered in the pilot studies or in the development of the tests. Because of the way the software was designed the effect of this was to make the performance of the device on the second half of the test appear faster and more accurate than it was by registering twice on the first target. Therefore the results for tests 2 and 3 only relate to indicating the first target of the test. This means that they are comparable to the rest of the results.
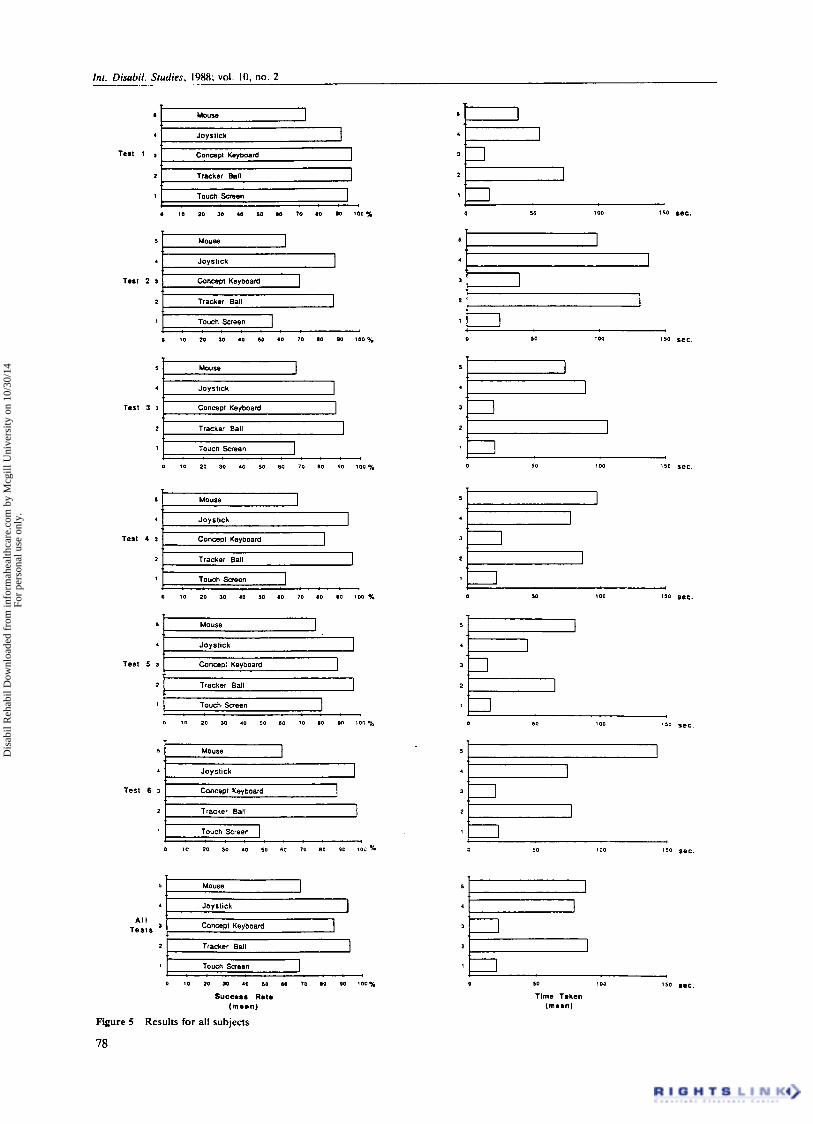
The main body of the results are set out in Figure 5. They include the mean success rates and the mean times for each device on each test. There are also histograms of the performance of the devices for all tests. A one-way analysis of variance was calculated for the overall scores and the F factor derived indicated statistical significance at the < 1% level.
The histograms relating to success rate show that all devices apart from the mouse achieved high scores on Test 1. Test 2 was only performed well when the joystick and tracker ball were used. Tests 3 to 6 were broadly comparable in the results in so far as only the mouse and touch screen were unable to be used with an acceptable degree of success. The composite histogram of all tests shows that the tracker ball and joystick were the most successful, both scoring > 90%. The concept keyboard (touchpad) was close behind at 86%; and the mouse and touch screen both lagged behind with 68%.
The histograms showing the time taken by the subjects demonstrate that the devices can be considered as in two groups - those which move a cursor, the mouse, joystick, and tracker ball; and those which allow the patient to indicate the target directly. All the histograms clearly show that the direct group are much faster than those which move a cursor.
Table 3 gives the results for the preference assessment that each subject completed. This form was arranged as a continuum, and it would be possible to compound the responses in such a way that the devices could be
Table 3
Device Preference score
Mouse Joystick Touchpad Tracker ball Touch screen
37 43 50 5h 40
arranged along it to reflect all responses. This was not thought to be appropriate, however. One of the main characteristics of stroke victims is that they have com- munication problems, often in both expression and comprehension, and it was thought that whilst the subjects were able to grasp the concept of some devices being better for them than others, it was not safe to assume that they appreciated the significance of the positioning of each device at a particular point on the line. Therefore the results in Table 3 were derived by ranking the devices, 5 for first preference 4 for second, etc. Thus the score for each device is out of a possible 60. If the subject expressed indifference between devices they were all awarded equal scores at the upper level.
The tracker ball was a clear leader in this comparison, followed by the concept keyboard (touchpad). The joystick only came third in spite of its high success rate. The touch screen was next and the mouse last. Figure 4 gives the results for each device grouped according to the resolution of the test targets. Thus low resolution refers to test 1 , medium to tests 3 and 5 , and high to tests 2 , 4, and 6 .
The aim of presenting the results in this format was to enable those who are working with the handicapped in other contexts to more easily relate these results to their own interests. The histograms show that all devices performed well on the low-resolution task, although the mouse was less effective. As the resolution increased the joystick and tracker ball maintained their level of performance, t h e concept keyboard fell off slightly, the
Mouse 1 ~
Joystick I J Concept Keyboard
2 Tracker Ball I TouchScreen
0 % 50
I Mouse I
Jovstick 1
TouchScreen I I
5 I m u s e I
Joystick
Tracker Ball
'O0 % 50
Figure 4 Results according to test resolution
77
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mcg
ill U
nive
rsity
on
10/3
0/14
For
pers
onal
use
onl
y.
Inl. Disahil. Studies, 19x8; vol. 10. no. 2
I
4
Test I , 2
1
:k I M U S e
Joystick
Concept Keyboard
Tracker Ball
Touch Screen
1 1
; .
5
4
3
2
1
1
5 1 Mouss I
2
4 1 Jovstick I
Tracker Ball
Test 2 3
0 10 20 10 40 50 60 70 80 00 100%
5 1 Mouse I
4 Joystick 1 Test 3 3
1 Touch Screen
0 10 20 30 40 SO 60 70 80 PO 100%
5 Mouse I . Joystick I Test 4 1 Coneeot Kevboard I
0 I 0 20 30 40 50 60 10 60 00 100 %
5 Mouse 1 . Joystick
Test 5 3 Canceo: Kevboard 1 2 Tracker Ball
1 Touch Screen
I
0 10 1 0 30 .o so 80 70 80 00 100% 0 50 100
Test 6 3
1 Touch Screen
0 10 20 30 40 50 60 70 60 PO 100 % 0 50 100 150 sec.
A l l T e s t s
2 1 I I Tracker Ball L I
1 . : : . : . I : Touch Screen
0 10 20 10 10 50 80 10 10 $0 100%
Succmss Rmtm (memn)
Figure 5 Results for all subjects
0 so 101)
T h e Tmken (mean)
78
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mcg
ill U
nive
rsity
on
10/3
0/14
For
pers
onal
use
onl
y.

PETHERAM: Stroke victims and the cornmter
’
touch screen quite dramatically, and the mouse deterior- ated further.
Another area of interest was whether any attribute of a subject could be identified which could be used as an indication as to the subject’s likely performance. Since the main parameter was thought to be the level of physical handicap the patients were grouped according to Barthel classification. Figure 6 shows the overall results on this basis. As can be readily seen, apart from the control group, any relationship between performance and Barthel group is the opposite of what would be expected.
~ ~~
Control Group
8arth.l G,O”P.
I
* Severe
Control Group
- - 0 50 % 1w
Figure 6 Results according to the Barthel group
There was, however, some indication of a positive correlation between a subject’s FCP and performance. Since FCP is a compound measure further investigation is needed to determine whether any element can be useful as a performance predictor.
F.C.P.
0 50 ’ %
Figure 7 Results according to FCP
Note: Complete results for each subject and fuller statistical analyses are available from the author on request.
DISCUSSION OF DEVICES
Mouse This device showed up very poorly in this experiment, having the equal lowest success rate and the equal highest overall time. These results contrast strongly with those achieved by Wilton and McLean,’ and Card et al.,’ in which the mouse was found to be the most effective input device tested. From this experiment it may be inferred that whilst the mouse is suitable for able-bodied people it is not appropriate for use by stroke victims or those with similar problems. It should also be noted that the mouse was least liked by the subjects. It was noticed during the tests that some subjects tended to pivot on their elbow when moving the mouse, thus progressing in an arc rather than a straight line. Also the clenching movement necessary to press the buttons sometimes moved the mouse off target.
Joystick Although the joystick had a success rate that was very close to the best it scored poorly in the subjective evaluation. It is hard to account for this discrepancy since the times overall were less than the other two cursor control devices. It may be that the example used, although having a well-positioned button, did seem rather flimsy. Also the fact that it tended to slip around if not held firmly may have counted against it.
Concept keyboard The design of this experiment tended to work against this device in that the overlays necessarily consisted of the block patterns with no identifying characteristics. Thus in the tests with complex block patterns the content-free nature of the tests meant that it was quite difficult to relate the red block on the screen to the corresponding block on the overlay. In spite of this handicap the concept keyboard performed very well, achieving a success rate of 85% and the lowest overall time. It was also the second most popular device in the attitude survey.
Tracker ball The tracker ball came out best in both success rate and popularity, but it was one of the slowest devices. Observing the subjects using the device, i t seemed that they were more relaxed and in control than with any other input. There are two attributes which may account for this: the Marconi tracker ball is robust and has a ‘solid’ feel; also the user can position the cursor using the ball and then move the hand to press the button without disturbing the cursor position. It may be that breaking the process of positioning and indicating into two discrete operations reduces the perceived complexity of the task.
Touch screen This device had the lowest overall success rate at 68%. Although it was fast it was only fourth in the subjective evaluation. The success rate on test 1, the low resolution test, was high at 95% but apart from 80% on test 5 the other scores were very poor. The reason for this seems to be that in order for the position of the finger or pointer to be registered accurately it must be withdrawn at an angle of 90 degrees to the screen. Any variation from this introduces parallax error. This is unfortunate because the device is easy and pleasant to use - but it has a limit to the level of resolution it can work at.
GENERAL DISCUSSION OF RESULTS On examining the success rates, the results show that all devices except for the mouse are acceptable on low- resolution tasks (test l), but only the joystick, concept keyboard, and tracker ball are acceptable on all tasks. When times are examined the devices fall into two groups: the fast devices which allow direct indication of the target, and the slow devices which work by control- ling a cursor. When the experiment was being designed it was thought that the times of the devices would be a guide to ease of use, and might be reflected in the subjective preferences. In fact the slowest device, the tracker ball, proved to be the most popular, and the fastest device proved to be the second least popular.
Conclusion For the purposes of the project of which this experiment was a part, the tracker ball is a clear choice. It came out best as far as success rate and subjective preference. The o n l y close contenders were the joystick and the concept keyboard. The joystick was virtually as accurate as the tracker ball but was not so well liked. Joysticks are available in a wide range of configurations, and careful
79
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mcg
ill U
nive
rsity
on
10/3
0/14
For
pers
onal
use
onl
y.

Int. Dbabil. Studies. 1988: vol. 10. no. 2
attention should be paid to selecting the most appropri- ate. The concept keyboard was handicapped by the nature of this experiment, which divorced the overlay from the screen image to a greater extent than would normally be the case. The main problem with the concept keyboard is that the overlay needs to reflect the screen design. Thus every time the screen design alters the overlay needs to be changed. This involves extra work in producing overlays which must register accurately with the touch-sensitive squares, and also the need for synchronizing the changes of overlays with the changes of screen design. Thus if the situation in which it is to be used can accommodate the development, use, and management of overlays the concept keyboard can be very effective.
A side issue of this study was to see if any characteris- tics of the subjects could be used to predict their performance on the tests. This would be helpful in identifymg any section of the population which would be most likely to benefit from using a microcomputer. Due to the limited size of the sample the study was inconclu- sive in this respect. From the results in Figures 6 and 7 it would seem that FCP may be a better guide to potential performance than Barthel class. The results as they stand are not statistically significant, but they may be of interest as an indication of some directions further research could investigate.
It is felt that the availability of usable input devices is an important development in so far as it enables stroke victims to interact with microcomputers in a less re- stricted way than specialized apparatus which generally only gives access to specialized software. Given this potential, and the necessarily limited range and number
of subjects that participated in this study, there remains much scope,for further research using other subjects and any other input devices which may be developed. It is hoped that this study may lead to further efforts in this direction.
Acknowledgements
The author gratefully acknowledges help from the following sources: Dr Pam Enderby and John Betts - project supervisors; staff and patients of the Stroke Unit and the Speech Therapy Department, Frenchay Hospital, Bristol; Andy Vince - advice on statistics; Marconi (Power Division), Microvitec Ltd, and Bristol SEMERC - loan or donation of test equipment; Bristol Polytechnic and Frenchay Hospital - funding and facilities.
References 1 Whitfield D, Ball RG, Bird JM. Some comparisons of on-display
and off-display touch input devices for interaction with computer generated displays. Ergonomics 1983; M(11): 1033-1053
2 Wilton J, McLean RS. Evaluation of a mouse as an educational pointing device. Comput Educ 1984; S(4): 455-461
3 Card SK, English WK, Burr BJ. Evaluation of mouse, rate- controlled isometric joystick, step keys, and text keys for text selection on a CRT. Ergonomics 1978; 21(8): 601-613
4 Keith RL. Speech and language rehabilitation: a workbook for the neurologically impaired. Interstate 1972
5 Stryker S. Speech after stroke: a rnanuul for the speech pathologisr and family member. C. C. Thomas, 1975
6 Lazzari AM, Peters PM. Handbook of exercises for languge processing. Linguisysterns, Moline, IL, USA 1980
7 Wade DT, Langton Hewer R. Functional abilities after stroke: measurement, natural history, and prognosis. J.N.N.P., 1986
8 Sarno MT. Functional communication profile. New York Univer- sity Medical Center, 1963
Book review
Function, fitness and fun
International Perspectives on Adapted Physical Activiry. Edited by M.E. Bemdge and G.R. Ward. Human Kinetics, Illinois, 1987.297 pp., 49 illus. $US 27. ISBN 0-87322-079-X.
The fifth international symposium on adapted physical activity was held in Toronto in 1985, and this book is a selection of 36 of the 170 papers presented. The themes of the meeting were function, fitness, and fun, but the book has been split into nine sections ranging from motor development of disabled children, through physical activity in psychiatric illness, special problems of impaired athletes, finishing with two sections on elderly people. The contributors are as diverse as the topics, although most are working in departments of physical education in North America. The preface makes it clear that working with impaired people is a new departure for physical educators, and for those of us who have spent most of our time in medicine it is very enlightening to see what other professions are up to. I do wonder, rhough, how often a true synthesis of views and approaches is achieved at meetings like this. Many of the papers are ‘not science’, making extravagant claims for the value of hippother- apy (horse riding!), or dance-movement therapy, whereas others are painstakingly controlled experiments with null hypotheses and very sexy statistics. I can almost hear the scientists complaining about lack of evidence of effectiveness of new therapies and the innovative educators dismayed by the inaccessibility and impracticability of much of the science. It should be stimulating but I fear it tends to switch people off.
A paper on limitations to exercise in coronary artery disease patients illustrates this difference in approach. Exercise in the supine position leads to an increase in myocardial oxygen demand
80
compared with the upright position. Presumably this information is relevant to giving patients advice about sexual activity but there is no evidence of this synthesis in the author’s discussion. Maybe his contribution was in the ‘fitness’ rather than the ‘fun’ section. Another paper on the skills of wheelchair basketball players uses an abundance of statistics, only to conclude that ‘the degree of handicap plays an important part in testing wheelchair athletes’ and ‘the judgement of the coach was reliable’. A few papers contained evidence of the worst of all worlds - bad science made to look like good science. One example was a study of a home exercise programme for children with cystic fibrosis, which used a control group composed of those children who were too fit to need any extra exercise. At the end of the exercise programme the fitness scores of the experimental group remained lower than the control group scores. Surprised? A study of the factors influencing exercise claimed to randomly select subjects, reported that those aged 65+ were more likely than subjects aged 45-64 years to engage in strenuous activity, and then came clean in the discussion, admitting that the sample were all volunteers and that care should be taken in generalizing to other groups of old people.
In general the ‘how to do it’ papers are more thought-provoking and more likely to achieve the objective of seeding innovations than the ‘does it work’ contributions. The book is very late in appearing, for a set of conference papers, and investigators at the cutting edge of adapted physical activity will be better served by the quarterly journal. For the rest of us it is worth spending an evening with someone else’s copy of the book.
SHAH EBRAHIM
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Mcg
ill U
nive
rsity
on
10/3
0/14
For
pers
onal
use
onl
y.