elevated cd14 cd16 monocytes predict...
TRANSCRIPT
Elevated CD14��CD16� Monocytes PredictCardiovascular Events
Katarina E. Berg, PhD; Irena Ljungcrantz, BSI; Linda Andersson, MSc; Carl Bryngelsson, RE;Bo Hedblad, MD, PhD; Gunilla N. Fredrikson, PhD; Jan Nilsson, MD, PhD; Harry Bjorkbacka, PhD
Background—Although monocytes in peripheral blood are no longer considered to be a homogeneous population,associations between distinct monocyte subsets and cardiovascular disease have not been highlighted in largeepidemiological studies.
Methods and Results—The study included 700 randomly selected subjects from the cardiovascular arm of the Malmo Diet andCancer study. Among these, 123 subjects experienced ischemic cardiovascular events during the follow-up until December2008. Mononuclear leukocytes frozen at the baseline investigation in 1991 to 1994 were thawed and analyzed with flowcytometry to enumerate monocyte subsets, based on CD14 and CD16 expression. The percentage and number of classicalCD14��CD16� monocytes were increased in the cardiovascular-event group compared with the event-free subjects (median,69% [interquartile range, 62% to 76%] versus 67% [59% to 72%], P�0.017; 344 [251 to 419] cells/�L versus 297 [212 to384] cells/�L, P�0.003). The hazard ratio was 1.66 for suffering a cardiovascular event in the highest tertile of the numberof CD14��CD16� monocytes compared with the lowest tertile, even after adjustment for common risk factors (HR, 1.66;95% CI: 1.02 to 2.72). CD14��CD16� monocytes did not, however, associate with the extent of atherosclerosis at baseline.In contrast, the percentage of monocytes expressing CD16 was negatively associated to the extent of carotid atherosclerosismeasured as intima-media thickness at baseline. The chemokine receptors CCR2, CX3CR1, and CCR5 were not differentiallyexpressed between cases and controls on any of the monocyte subsets, but CCR5 expression on CD14�CD16�� monocyteswas negatively associated to carotid intima-media thickness.
Conclusions—This study shows that classical CD14��CD16� monocytes can predict future cardiovascular riskindependently of other risk factors in a randomly selected population. (Circ Cardiovasc Genet. 2012;5:122-131.)
Key Words: monocytes � leukocytes � cardiovascular disease � myocardial infarction � ischemic stroke
Monocytes and macrophages are considered indisputableplayers in the etiology of atherosclerosis.1 Although
monocyte count is a predictor of subclinical carotid athero-sclerosis and plaque formation, associations between mono-cyte counts and cardiovascular disease (CVD) risk, have notbeen highlighted in large epidemiological studies.2,3 In con-trast, both white blood cell and neutrophil counts are inde-pendent risk factors for cardiovascular disease.4 The lack ofassociation between monocyte count and CVD may beexplained by the fact that human monocytes were, in thepast, considered to be a homogeneous population.5 At thepresent time, at least 3 human monocyte populations canbe defined by the expression of CD14, a part of thelipopolysaccharide receptor, and the Fc�III receptor CD16.The dominant classical monocyte species are the CD14��
CD16� monocytes that constitute 65% to 85% of allmonocytes. CD14��CD16� monocytes express CCR2,which is the receptor for monocyte chemo-attractant
protein-1 and are believed to actively be recruited to sitesof inflammation.6 Monocytes expressing CD16 are aheterogenous population that can be divided into intermediateCD14��CD16� and nonclassical CD14�CD16�� monocytes.7
The CD16-positive monocytes express higher levels of thefractalkine receptor CX3CR1 than the CD14��CD16� mono-cytes. The CD16-positive monocytes have been shown toproduce more TNF� and less IL-10 than the CD14��CD16�
monocytes and have accordingly been coined pro-inflammatorymonocytes.8 An increase in CD14�CD16�� monocytes havebeen reported for a number of inflammatory and infectiousdiseases in humans.9
Editorial see p 7Clinical Perspective on p 131
In mice, monocytes are divided into a Ly-6ChighCX3CR1low
CCR2� subset that is actively recruited into inflamed tissueand a Ly-6ClowCX3CR1highCCR2� subset that home into
Received March 16, 2011; accepted December 29, 2011.From the Department of Clinical Sciences, Skåne University Hospital Malmo, Lund University, Malmo, Sweden (K.E.B., I.L., L.A., C.B., B.H., G.N.F.,
J.N., H.B.); Faculty of Health and Society, Malmo University, Malmo, Sweden (G.N.F.).The online-only Data Supplement is available at http://circgenetics.ahajournals.org/lookup/suppl/doi:10.1161/CIRCGENETICS.111.960385/-/DC1.Correspondence to Harry Bjorkbacka, Experimental Cardiovascular Research, CRC 91:12, Lund University, Entrance 72, Skåne University Hospital
Malmo, SE-205 02 Malmo, Sweden. E-mail [email protected]© 2012 American Heart Association, Inc.
Circ Cardiovasc Genet is available at http://circgenetics.ahajournals.org DOI: 10.1161/CIRCGENETICS.111.960385
122
by guest on July 13, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

noninflamed tissues in a CX3CR1-dependent process.6 Nota-bly, the expression pattern of CX3CR1 and CCR2 on mousemonocyte subsets can also be used to identify human mono-cyte subsets, but, although considerable additional overlap inexpression profile exists, it remains to be confirmed if thesesubsets can be functionally translated across species.10 TheLy-6Chigh monocytes are increased in hypercholesterolemicapolipoprotein E-deficient mice consuming a high-fat diet,and Ly-6Chigh monocytes are recruited to atheroscleroticplaques.11,12 Ly-6Clow monocytes have been shown to enterplaques less frequently than Ly-6Chigh monocytes but aremore prone to develop into plaque-resident cells expressingCD11c.12 Recruitment of monocytes into plaques in mice hasbeen shown to depend on expression of chemokine receptorsCCR2, CCR5 (the receptor for RANTES, MIP-1� andMIP-1�), and CX3CR1, and these receptors have beenattributed nonredundant and independent roles in experimen-tal atherosclerosis.12–14 Interestingly, disruption of CCL2(monocyte chemo-attractant protein-1)/CCR2 or CX3CL1(fractalkine)/CX3CR1 interactions in mice reduces the num-bers of circulating monocytes, which may, at least in part,contribute to the reduced atherosclerosis observed in micelacking these chemokine/chemokine receptors.13,14
Although evidence for a role of monocyte subsets inatherosclerosis is accumulating from animal studies, there arefew clinical studies investigating the role of monocyte subsetsin CVD in humans. Still, studies in populations enriched inprevalent CVD patients and in populations with increasedCVD risk show that certain monocyte subsets can showstronger associations with CVD than others. A highCD14��CD16� monocyte count, but not total monocyte orCD16-negative monocyte count, has been shown to beassociated with higher rates of cardiovascular events in aprospective cohort of 94 patients on dialysis, followed forclose to 3 years, and in 119 patients not on dialysis, but withchronic kidney disease, followed up to 5 years.15,16 Mono-cytes expressing CD16 have also been shown to be associatedwith prevalence of coronary artery disease in a study popu-lation of 247 patients, with stable or unstable angina pectorisor acute coronary syndrome, and 61 healthy controls.17 Inpatients with stable coronary artery disease, the percentage ofCD14��CD16� monocytes was elevated in patients with 5 ormore risk factors compared with low- to medium-risk pa-tients.18 Here we show that monocyte subsets measured atbaseline can predict incident CVD, also, in a randomlyselected population cohort over a median follow-up of 15years. We also investigate if monocyte subsets are associatedwith extent of atherosclerosis at baseline by correlatingmonocyte subsets to intima media thickness in the carotidartery measured by ultrasound.
MethodsStudy PopulationThe study population consists of a cohort from the cardiovasculararm of the Malmo Diet and Cancer study.19 In the Malmo Diet andCancer study, complete birth cohorts, born between 1921 and 1949,were invited from the population in the city of Malmo, Sweden. Ahealth examination of the participants included a physical examina-tion, a panel of laboratory tests, and a self-administered question-naire, with items relevant for the occurrence of CVC. Between
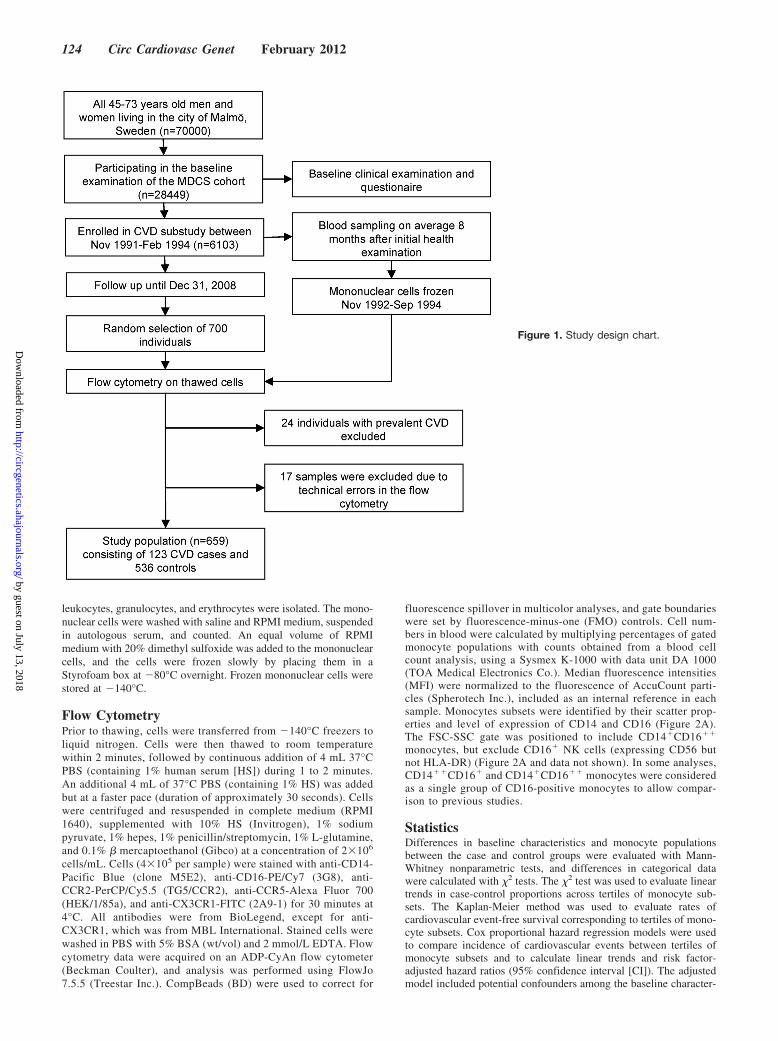
October 1991 and February 1994, every other participant was invitedto take part in a substudy of the epidemiology of carotid arterydisease.20 From these, a subcohort of 700 randomly selected indi-viduals was included in this study (Figure 1). Individuals withprevalent CVD (24) were excluded from further analysis. For 17samples, the cell number in the thawed samples was too low to beanalyzed, or the flow cytometry data were disqualified, because oftechnical errors. The health service authority of Malmo approved andfunded the screening program. All participants gave written in-formed consent. The study was approved by the Ethics Committee ofLund University and was conducted in accordance with the HelsinkiDeclaration.
Baseline CharacteristicsInformation on baseline characteristics was collected from theself-administered questionnaire and clinical examination. Body massindex was calculated as weight/height2 (kg/m2) and categorized intonormal weight (body mass index �25) and overweight/obese (bodymass index �25). Smoking habits were categorized into never orformer (smokers who had quit smoking at least 1 year before theexamination) and current smokers. Diabetes mellitus was defined asfasting whole blood glucose �6.1 mmol/L or self-reported diabetes,according to the questionnaire. By using a mercury sphygmomanom-eter, blood pressure (mm Hg) was measured twice in the right armafter a 10-minute rest. The average of the 2 measurements was used.Hypertension was defined as systolic blood pressure �140 mm Hgor diastolic blood pressure �90 mm Hg or the use of blood pressurelowering medication.
Laboratory Tests and Measurement of CarotidIntima-Media ThicknessBlood samples were drawn after overnight fasting. Fasting venousblood glucose, serum cholesterol, low-density lipoprotein (LDL)cholesterol, high-density lipoprotein (HDL) cholesterol, C-reactiveprotein, and triglycerides were analyzed with standard methods at thelaboratory of the Malmo University Hospital. Hypercholesterolemiawas defined as total cholesterol �6.2 mmol/L (�240 mg/dL). Theintima-media thickness (IMT) of the right common carotid arterywas measured according to a standardized protocol by trained,certified sonographers. The carotid IMT was determined off-line asthe mean wall thickness 1 cm proximal to the bifurcation, and eachimage was analyzed by a blinded observer. Methods of qualitycontrol have been published previously.21
Follow-Up PeriodAll subjects were followed from the baseline examination until firsthospitalization because of incident myocardial infarction, stroke,death, emigration, or December 31, 2008. Incident cases experienc-ing cardiovascular events or ischemic strokes were retrieved by datalinkage to the Swedish Hospital Discharge Register, the MalmoMyocardial Register, the Stroke register of Malmo (STROMA), andCause of Death Registry of Sweden. Ascertainment of cases andvalidity of the registries used have been proven to be high.22,23 Themedian follow-up period was 15.2 (interquartile range [IQR] 11.3 to16.2) years. Throughout the follow-up period, 123 incident cardio-vascular disease events were identified. A cardiovascular diseaseevent was defined as a fatal or nonfatal myocardial infarction(ICD-9: 410), ischemic stroke (ICD-9: 434), or death attributable tounderlying coronary heart disease (ICD-9: 410 to 414), using theSwedish Hospital Discharge Register, the Malmo Myocardial Reg-ister, the Stroke register of Malmo (STROMA), and Cause of DeathRegistry of Sweden. Individuals experiencing subarachnoid andintracerebral bleedings (ICD-9: 430 or 431) were excluded from theCVD case group and included in the control group, because theetiology differs from ischemic disease.
Isolation of Mononuclear CellsBlood samples for cell isolation were obtained in heparin tubes, puton top of a Ficoll-Paque cushion, and centrifuged at 1350 g for 12minutes at 20°C.24 Fractions of platelet-poor plasma, mononuclear
Berg et al CD14��CD16� Monocytes Predict CVD 123
by guest on July 13, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
leukocytes, granulocytes, and erythrocytes were isolated. The mono-nuclear cells were washed with saline and RPMI medium, suspendedin autologous serum, and counted. An equal volume of RPMImedium with 20% dimethyl sulfoxide was added to the mononuclearcells, and the cells were frozen slowly by placing them in aStyrofoam box at �80°C overnight. Frozen mononuclear cells werestored at �140°C.
Flow CytometryPrior to thawing, cells were transferred from �140°C freezers toliquid nitrogen. Cells were then thawed to room temperaturewithin 2 minutes, followed by continuous addition of 4 mL 37°CPBS (containing 1% human serum [HS]) during 1 to 2 minutes.An additional 4 mL of 37°C PBS (containing 1% HS) was addedbut at a faster pace (duration of approximately 30 seconds). Cellswere centrifuged and resuspended in complete medium (RPMI1640), supplemented with 10% HS (Invitrogen), 1% sodiumpyruvate, 1% hepes, 1% penicillin/streptomycin, 1% L-glutamine,and 0.1% � mercaptoethanol (Gibco) at a concentration of 2�106
cells/mL. Cells (4�105 per sample) were stained with anti-CD14-Pacific Blue (clone M5E2), anti-CD16-PE/Cy7 (3G8), anti-CCR2-PerCP/Cy5.5 (TG5/CCR2), anti-CCR5-Alexa Fluor 700(HEK/1/85a), and anti-CX3CR1-FITC (2A9-1) for 30 minutes at4°C. All antibodies were from BioLegend, except for anti-CX3CR1, which was from MBL International. Stained cells werewashed in PBS with 5% BSA (wt/vol) and 2 mmol/L EDTA. Flowcytometry data were acquired on an ADP-CyAn flow cytometer(Beckman Coulter), and analysis was performed using FlowJo7.5.5 (Treestar Inc.). CompBeads (BD) were used to correct for
fluorescence spillover in multicolor analyses, and gate boundarieswere set by fluorescence-minus-one (FMO) controls. Cell num-bers in blood were calculated by multiplying percentages of gatedmonocyte populations with counts obtained from a blood cellcount analysis, using a Sysmex K-1000 with data unit DA 1000(TOA Medical Electronics Co.). Median fluorescence intensities(MFI) were normalized to the fluorescence of AccuCount parti-cles (Spherotech Inc.), included as an internal reference in eachsample. Monocytes subsets were identified by their scatter prop-erties and level of expression of CD14 and CD16 (Figure 2A).The FSC-SSC gate was positioned to include CD14�CD16��
monocytes, but exclude CD16� NK cells (expressing CD56 butnot HLA-DR) (Figure 2A and data not shown). In some analyses,CD14��CD16� and CD14�CD16�� monocytes were consideredas a single group of CD16-positive monocytes to allow compar-ison to previous studies.
StatisticsDifferences in baseline characteristics and monocyte populationsbetween the case and control groups were evaluated with Mann-Whitney nonparametric tests, and differences in categorical datawere calculated with �2 tests. The �2 test was used to evaluate lineartrends in case-control proportions across tertiles of monocyte sub-sets. The Kaplan-Meier method was used to evaluate rates ofcardiovascular event-free survival corresponding to tertiles of mono-cyte subsets. Cox proportional hazard regression models were usedto compare incidence of cardiovascular events between tertiles ofmonocyte subsets and to calculate linear trends and risk factor-adjusted hazard ratios (95% confidence interval [CI]). The adjustedmodel included potential confounders among the baseline character-
Figure 1. Study design chart.
124 Circ Cardiovasc Genet February 2012
by guest on July 13, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
istics that differed between monocyte tertiles (ANOVA or �2 test forlinear trend). Natural-logarithmic transformation was used on mono-cyte parameters, with distributions deviating from normality beforeanalyzing bivariate Pearson correlations to carotid IMT and labora-tory parameters. Laboratory parameters that also displayed signifi-
cant Pearson correlations to carotid IMT were included as covariatesin linear regression models evaluating multivariable adjusted corre-lations between monocytes and carotid IMT. P�0.05 was consideredsignificant. Statistical analyses were performed using PASW Statis-tics 18 (SPSS) and GraphPad 5 software.
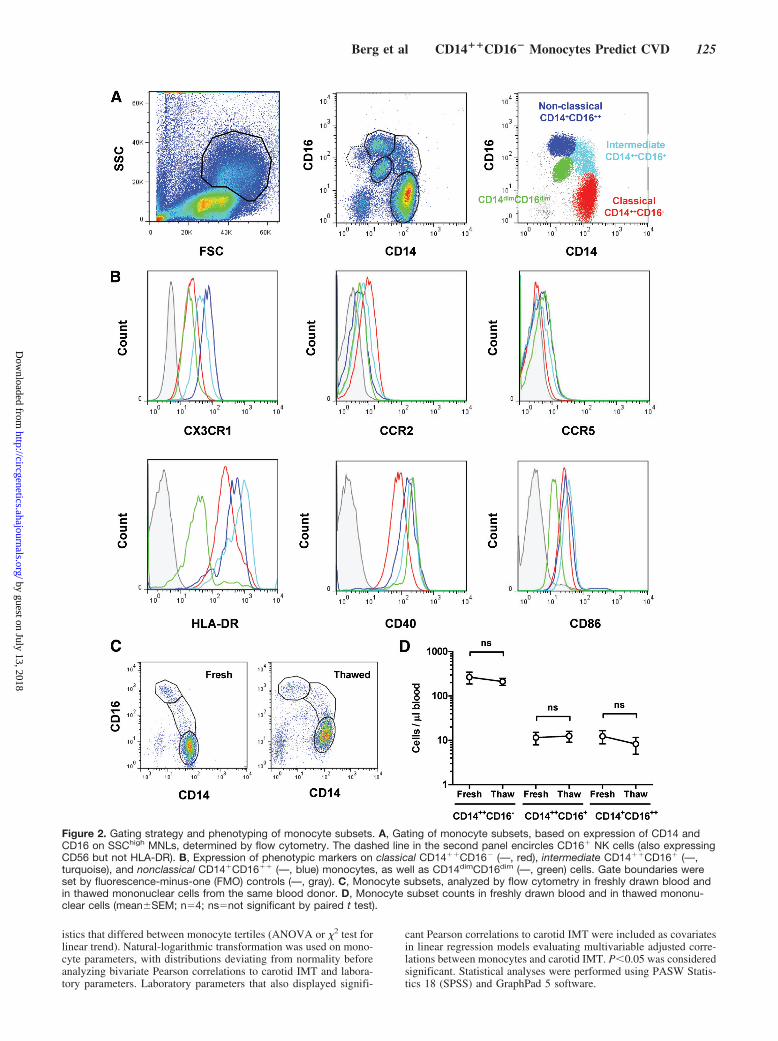
Figure 2. Gating strategy and phenotyping of monocyte subsets. A, Gating of monocyte subsets, based on expression of CD14 andCD16 on SSChigh MNLs, determined by flow cytometry. The dashed line in the second panel encircles CD16� NK cells (also expressingCD56 but not HLA-DR). B, Expression of phenotypic markers on classical CD14��CD16� (—, red), intermediate CD14��CD16� (—,turquoise), and nonclassical CD14�CD16�� (—, blue) monocytes, as well as CD14dimCD16dim (—, green) cells. Gate boundaries wereset by fluorescence-minus-one (FMO) controls (—, gray). C, Monocyte subsets, analyzed by flow cytometry in freshly drawn blood andin thawed mononuclear cells from the same blood donor. D, Monocyte subset counts in freshly drawn blood and in thawed mononu-clear cells (mean�SEM; n�4; ns�not significant by paired t test).
Berg et al CD14��CD16� Monocytes Predict CVD 125
by guest on July 13, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
ResultsDuring the follow-up period, 39 men and 36 women experi-enced coronary events, and 26 men and 22 women experi-enced ischemic strokes, making up a total of 123 in thecardiovascular disease cases group. The median time frombaseline to occurrence of an event in the case group was 9.0(IQR, 5.3 to 12.6) years. The case group contained more maleand diabetic individuals than the control group (Table 1). Thenumber of individuals on antidiabetic or blood pressure-lowering medication was also higher in the case group,compared with the controls. The number of individuals withhigh cholesterol (�6.2 mmol/L), however, was not signifi-cantly different between the case and control group. Labora-tory parameters were in agreement with the clinical makeupof the case and control groups.
Three monocyte populations were identified as CD14��
CD16� classical monocytes, CD14�CD16�� nonclassicalmonocytes, and CD14��CD16� intermediate monocytes, inaccordance with the proposed nomenclature (Figure 2A).7 Toconfirm that these were indeed discrete monocyte subsets, weanalyzed the expression of several markers, including CCR2,
CX3CR1, and CCR5 on these subsets (Figure 2B). CD14��
CD16� monocytes expressed CCR2, and CD14�CD16��
monocytes expressed �3-fold more CX3CR1 than CD14��
CD16� monocytes, as has been described previously,25,26
whereas only the CD16-positive monocyte subsets expressedCCR5. The CD16-positive monocytes also expressed moreCD40 and HLA-DR than CD14��CD16� monocytes,whereas CD86 expression was similar between the subsets.None of the subsets were CD3-, CD19-, or CD56-positive(data not shown). The identity of the CD14dimCD16dim
population is unclear, but it is not an artifact arising fromfreezing and thawing of cells, as we have observed thispopulation in fresh samples. The CD14dimCD16dim popula-tion was not associated with events or extent of atheroscle-rosis. To test if the monocyte subsets are sensitive to freezingand thawing, we compared monocyte counts in freshly drawnblood to counts in thawed mononuclear cells from the samedonor, frozen using the same protocol as during the baselineexamination (Figure 2C). No significant difference betweenmonocyte counts in fresh and frozen samples was observed(Figure 2D). Although cells with compromised plasma mem-brane integrity (7-AAD positive) were found among theisolated mononuclear cells (median, 6.6%; IQR, 5.2 to 9.9%),no significant difference in cell viability was found betweenfresh and frozen CD45� mononuclear cells (data not shown).Also, no differences in cell viability were observed betweenmonocyte subsets, indicating that the monocyte subsets wereequally sensitive to freeze-thawing (data not shown).
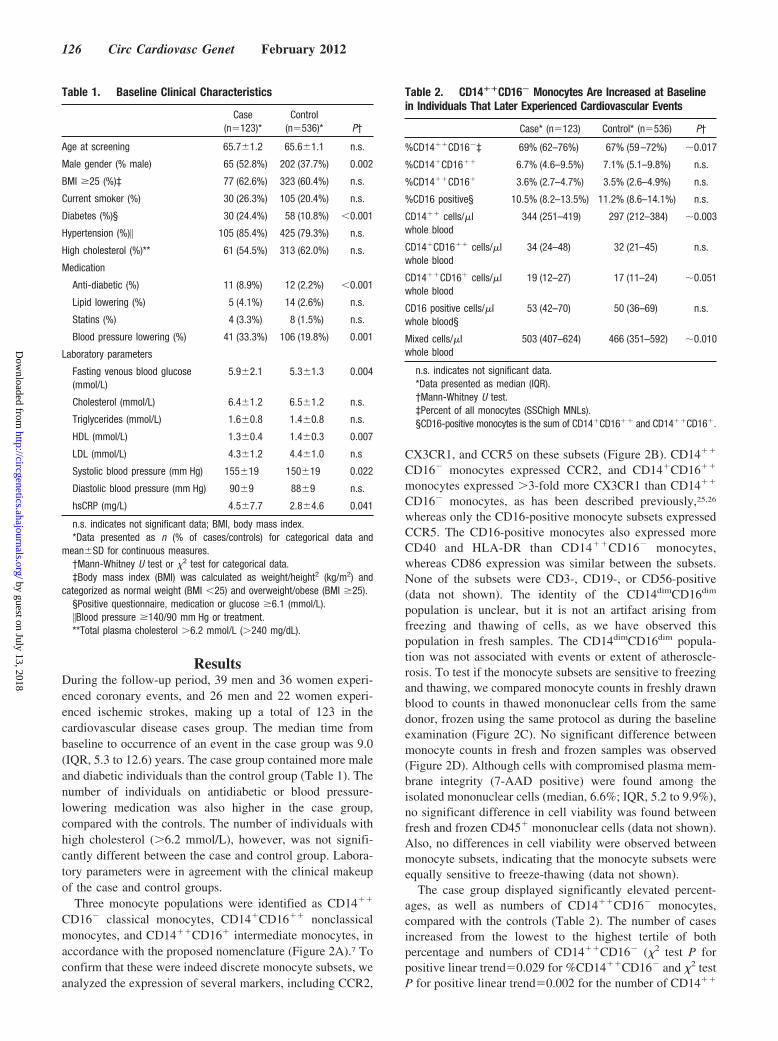
The case group displayed significantly elevated percent-ages, as well as numbers of CD14��CD16� monocytes,compared with the controls (Table 2). The number of casesincreased from the lowest to the highest tertile of bothpercentage and numbers of CD14��CD16� (�2 test P forpositive linear trend�0.029 for %CD14��CD16� and �2 testP for positive linear trend�0.002 for the number of CD14��
Table 1. Baseline Clinical Characteristics
Case(n�123)*
Control(n�536)* P†
Age at screening 65.7�1.2 65.6�1.1 n.s.
Male gender (% male) 65 (52.8%) 202 (37.7%) 0.002
BMI �25 (%)‡ 77 (62.6%) 323 (60.4%) n.s.
Current smoker (%) 30 (26.3%) 105 (20.4%) n.s.
Diabetes (%)§ 30 (24.4%) 58 (10.8%) �0.001
Hypertension (%)� 105 (85.4%) 425 (79.3%) n.s.
High cholesterol (%)** 61 (54.5%) 313 (62.0%) n.s.
Medication
Anti-diabetic (%) 11 (8.9%) 12 (2.2%) �0.001
Lipid lowering (%) 5 (4.1%) 14 (2.6%) n.s.
Statins (%) 4 (3.3%) 8 (1.5%) n.s.
Blood pressure lowering (%) 41 (33.3%) 106 (19.8%) 0.001
Laboratory parameters
Fasting venous blood glucose(mmol/L)
5.9�2.1 5.3�1.3 0.004
Cholesterol (mmol/L) 6.4�1.2 6.5�1.2 n.s.
Triglycerides (mmol/L) 1.6�0.8 1.4�0.8 n.s.
HDL (mmol/L) 1.3�0.4 1.4�0.3 0.007
LDL (mmol/L) 4.3�1.2 4.4�1.0 n.s
Systolic blood pressure (mm Hg) 155�19 150�19 0.022
Diastolic blood pressure (mm Hg) 90�9 88�9 n.s.
hsCRP (mg/L) 4.5�7.7 2.8�4.6 0.041
n.s. indicates not significant data; BMI, body mass index.*Data presented as n (% of cases/controls) for categorical data and
mean�SD for continuous measures.†Mann-Whitney U test or �2 test for categorical data.‡Body mass index (BMI) was calculated as weight/height2 (kg/m2) and
categorized as normal weight (BMI �25) and overweight/obese (BMI �25).§Positive questionnaire, medication or glucose �6.1 (mmol/L).�Blood pressure �140/90 mm Hg or treatment.**Total plasma cholesterol �6.2 mmol/L (�240 mg/dL).
Table 2. CD14��CD16� Monocytes Are Increased at Baselinein Individuals That Later Experienced Cardiovascular Events
Case* (n�123) Control* (n�536) P†
%CD14��CD16�‡ 69% (62–76%) 67% (59–72%) �0.017
%CD14�CD16�� 6.7% (4.6–9.5%) 7.1% (5.1–9.8%) n.s.
%CD14��CD16� 3.6% (2.7–4.7%) 3.5% (2.6–4.9%) n.s.
%CD16 positive§ 10.5% (8.2–13.5%) 11.2% (8.6–14.1%) n.s.
CD14�� cells/�lwhole blood
344 (251–419) 297 (212–384) �0.003
CD14�CD16�� cells/�lwhole blood
34 (24–48) 32 (21–45) n.s.
CD14��CD16� cells/�lwhole blood
19 (12–27) 17 (11–24) �0.051
CD16 positive cells/�lwhole blood§
53 (42–70) 50 (36–69) n.s.
Mixed cells/�lwhole blood
503 (407–624) 466 (351–592) �0.010
n.s. indicates not significant data.*Data presented as median (IQR).†Mann-Whitney U test.‡Percent of all monocytes (SSChigh MNLs).§CD16-positive monocytes is the sum of CD14�CD16�� and CD14��CD16�.
126 Circ Cardiovasc Genet February 2012
by guest on July 13, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
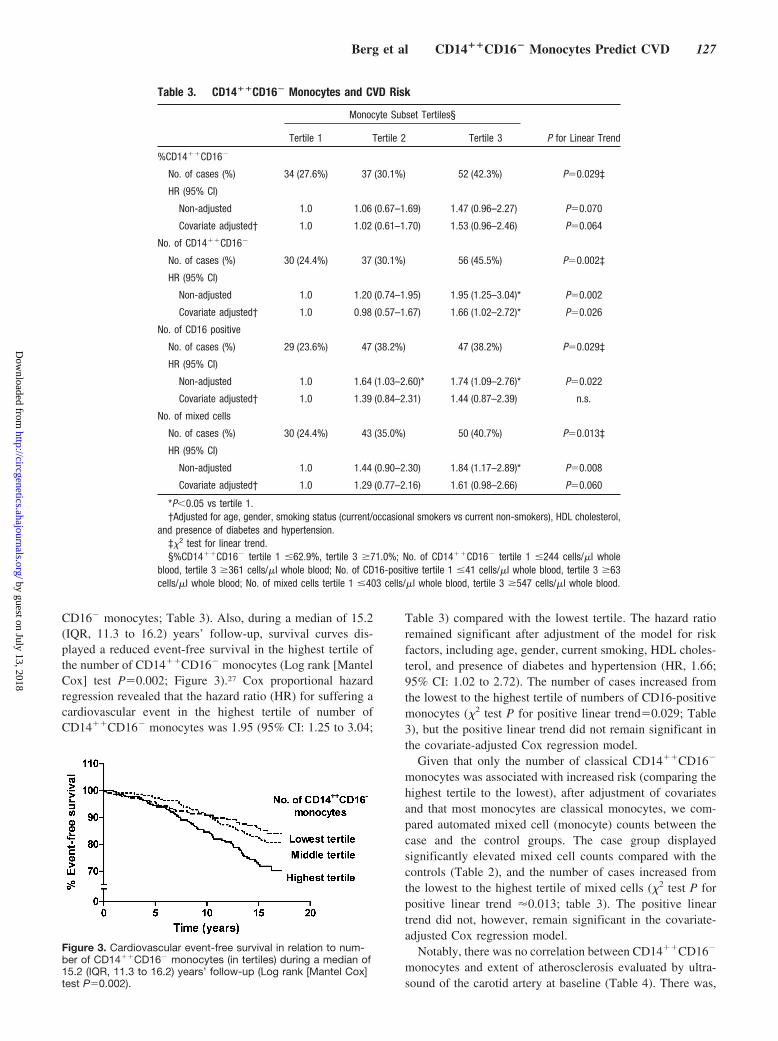
CD16� monocytes; Table 3). Also, during a median of 15.2(IQR, 11.3 to 16.2) years’ follow-up, survival curves dis-played a reduced event-free survival in the highest tertile ofthe number of CD14��CD16� monocytes (Log rank [MantelCox] test P�0.002; Figure 3).27 Cox proportional hazardregression revealed that the hazard ratio (HR) for suffering acardiovascular event in the highest tertile of number ofCD14��CD16� monocytes was 1.95 (95% CI: 1.25 to 3.04;
Table 3) compared with the lowest tertile. The hazard ratioremained significant after adjustment of the model for riskfactors, including age, gender, current smoking, HDL choles-terol, and presence of diabetes and hypertension (HR, 1.66;95% CI: 1.02 to 2.72). The number of cases increased fromthe lowest to the highest tertile of numbers of CD16-positivemonocytes (�2 test P for positive linear trend�0.029; Table3), but the positive linear trend did not remain significant inthe covariate-adjusted Cox regression model.
Given that only the number of classical CD14��CD16�
monocytes was associated with increased risk (comparing thehighest tertile to the lowest), after adjustment of covariatesand that most monocytes are classical monocytes, we com-pared automated mixed cell (monocyte) counts between thecase and the control groups. The case group displayedsignificantly elevated mixed cell counts compared with thecontrols (Table 2), and the number of cases increased fromthe lowest to the highest tertile of mixed cells (�2 test P forpositive linear trend 0.013; table 3). The positive lineartrend did not, however, remain significant in the covariate-adjusted Cox regression model.
Notably, there was no correlation between CD14��CD16�
monocytes and extent of atherosclerosis evaluated by ultra-sound of the carotid artery at baseline (Table 4). There was,
Table 3. CD14��CD16� Monocytes and CVD Risk
Monocyte Subset Tertiles§
Tertile 1 Tertile 2 Tertile 3 P for Linear Trend
%CD14��CD16�
No. of cases (%) 34 (27.6%) 37 (30.1%) 52 (42.3%) P�0.029‡
HR (95% CI)
Non-adjusted 1.0 1.06 (0.67–1.69) 1.47 (0.96–2.27) P�0.070
Covariate adjusted† 1.0 1.02 (0.61–1.70) 1.53 (0.96–2.46) P�0.064
No. of CD14��CD16�
No. of cases (%) 30 (24.4%) 37 (30.1%) 56 (45.5%) P�0.002‡
HR (95% CI)
Non-adjusted 1.0 1.20 (0.74–1.95) 1.95 (1.25–3.04)* P�0.002
Covariate adjusted† 1.0 0.98 (0.57–1.67) 1.66 (1.02–2.72)* P�0.026
No. of CD16 positive
No. of cases (%) 29 (23.6%) 47 (38.2%) 47 (38.2%) P�0.029‡
HR (95% CI)
Non-adjusted 1.0 1.64 (1.03–2.60)* 1.74 (1.09–2.76)* P�0.022
Covariate adjusted† 1.0 1.39 (0.84–2.31) 1.44 (0.87–2.39) n.s.
No. of mixed cells
No. of cases (%) 30 (24.4%) 43 (35.0%) 50 (40.7%) P�0.013‡
HR (95% CI)
Non-adjusted 1.0 1.44 (0.90–2.30) 1.84 (1.17–2.89)* P�0.008
Covariate adjusted† 1.0 1.29 (0.77–2.16) 1.61 (0.98–2.66) P�0.060
*P�0.05 vs tertile 1.†Adjusted for age, gender, smoking status (current/occasional smokers vs current non-smokers), HDL cholesterol,
and presence of diabetes and hypertension.‡�2 test for linear trend.§%CD14��CD16� tertile 1 �62.9%, tertile 3 �71.0%; No. of CD14��CD16� tertile 1 �244 cells/�l whole
blood, tertile 3 �361 cells/�l whole blood; No. of CD16-positive tertile 1 �41 cells/�l whole blood, tertile 3 �63cells/�l whole blood; No. of mixed cells tertile 1 �403 cells/�l whole blood, tertile 3 �547 cells/�l whole blood.
Figure 3. Cardiovascular event-free survival in relation to num-ber of CD14��CD16� monocytes (in tertiles) during a median of15.2 (IQR, 11.3 to 16.2) years’ follow-up (Log rank [Mantel Cox]test P�0.002).
Berg et al CD14��CD16� Monocytes Predict CVD 127
by guest on July 13, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
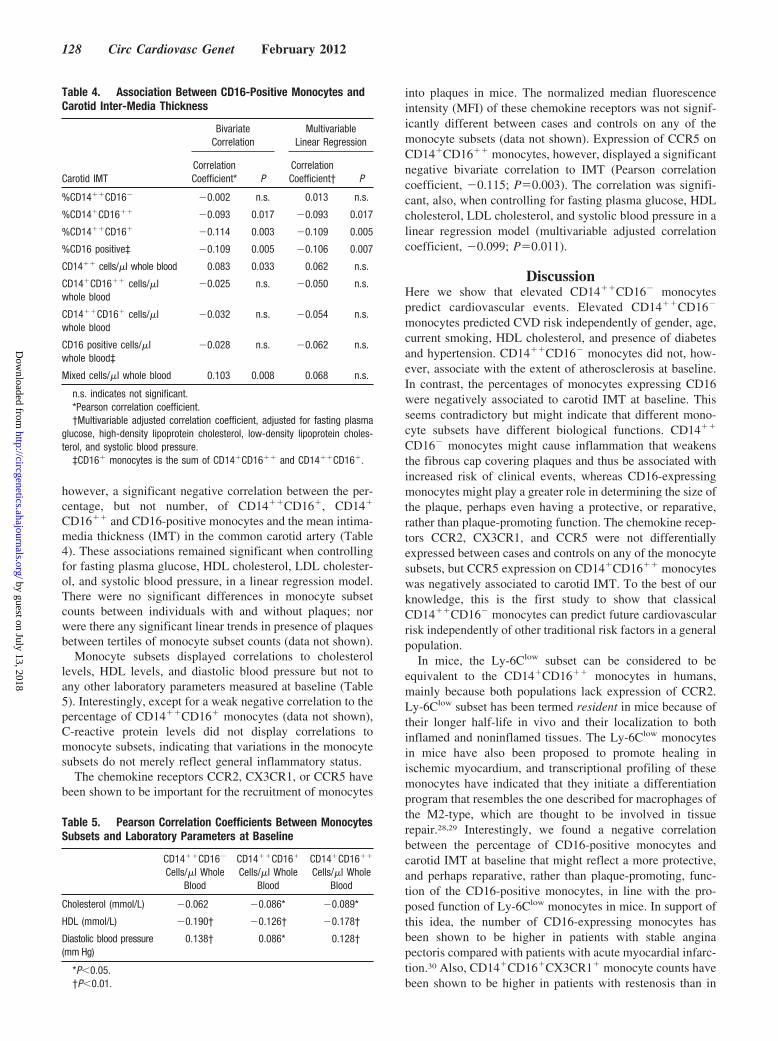
however, a significant negative correlation between the per-centage, but not number, of CD14��CD16�, CD14�
CD16�� and CD16-positive monocytes and the mean intima-media thickness (IMT) in the common carotid artery (Table4). These associations remained significant when controllingfor fasting plasma glucose, HDL cholesterol, LDL cholester-ol, and systolic blood pressure, in a linear regression model.There were no significant differences in monocyte subsetcounts between individuals with and without plaques; norwere there any significant linear trends in presence of plaquesbetween tertiles of monocyte subset counts (data not shown).
Monocyte subsets displayed correlations to cholesterollevels, HDL levels, and diastolic blood pressure but not toany other laboratory parameters measured at baseline (Table5). Interestingly, except for a weak negative correlation to thepercentage of CD14��CD16� monocytes (data not shown),C-reactive protein levels did not display correlations tomonocyte subsets, indicating that variations in the monocytesubsets do not merely reflect general inflammatory status.
The chemokine receptors CCR2, CX3CR1, or CCR5 havebeen shown to be important for the recruitment of monocytes
into plaques in mice. The normalized median fluorescenceintensity (MFI) of these chemokine receptors was not signif-icantly different between cases and controls on any of themonocyte subsets (data not shown). Expression of CCR5 onCD14�CD16�� monocytes, however, displayed a significantnegative bivariate correlation to IMT (Pearson correlationcoefficient, �0.115; P�0.003). The correlation was signifi-cant, also, when controlling for fasting plasma glucose, HDLcholesterol, LDL cholesterol, and systolic blood pressure in alinear regression model (multivariable adjusted correlationcoefficient, �0.099; P�0.011).
DiscussionHere we show that elevated CD14��CD16� monocytespredict cardiovascular events. Elevated CD14��CD16�
monocytes predicted CVD risk independently of gender, age,current smoking, HDL cholesterol, and presence of diabetesand hypertension. CD14��CD16� monocytes did not, how-ever, associate with the extent of atherosclerosis at baseline.In contrast, the percentages of monocytes expressing CD16were negatively associated to carotid IMT at baseline. Thisseems contradictory but might indicate that different mono-cyte subsets have different biological functions. CD14��
CD16� monocytes might cause inflammation that weakensthe fibrous cap covering plaques and thus be associated withincreased risk of clinical events, whereas CD16-expressingmonocytes might play a greater role in determining the size ofthe plaque, perhaps even having a protective, or reparative,rather than plaque-promoting function. The chemokine recep-tors CCR2, CX3CR1, and CCR5 were not differentiallyexpressed between cases and controls on any of the monocytesubsets, but CCR5 expression on CD14�CD16�� monocyteswas negatively associated to carotid IMT. To the best of ourknowledge, this is the first study to show that classicalCD14��CD16� monocytes can predict future cardiovascularrisk independently of other traditional risk factors in a generalpopulation.
In mice, the Ly-6Clow subset can be considered to beequivalent to the CD14�CD16�� monocytes in humans,mainly because both populations lack expression of CCR2.Ly-6Clow subset has been termed resident in mice because oftheir longer half-life in vivo and their localization to bothinflamed and noninflamed tissues. The Ly-6Clow monocytesin mice have also been proposed to promote healing inischemic myocardium, and transcriptional profiling of thesemonocytes have indicated that they initiate a differentiationprogram that resembles the one described for macrophages ofthe M2-type, which are thought to be involved in tissuerepair.28,29 Interestingly, we found a negative correlationbetween the percentage of CD16-positive monocytes andcarotid IMT at baseline that might reflect a more protective,and perhaps reparative, rather than plaque-promoting, func-tion of the CD16-positive monocytes, in line with the pro-posed function of Ly-6Clow monocytes in mice. In support ofthis idea, the number of CD16-expressing monocytes hasbeen shown to be higher in patients with stable anginapectoris compared with patients with acute myocardial infarc-tion.30 Also, CD14�CD16�CX3CR1� monocyte counts havebeen shown to be higher in patients with restenosis than in
Table 4. Association Between CD16-Positive Monocytes andCarotid Inter-Media Thickness
BivariateCorrelation
MultivariableLinear Regression
Carotid IMTCorrelationCoefficient* P
CorrelationCoefficient† P
%CD14��CD16� �0.002 n.s. 0.013 n.s.
%CD14�CD16�� �0.093 0.017 �0.093 0.017
%CD14��CD16� �0.114 0.003 �0.109 0.005
%CD16 positive‡ �0.109 0.005 �0.106 0.007
CD14�� cells/�l whole blood 0.083 0.033 0.062 n.s.
CD14�CD16�� cells/�lwhole blood
�0.025 n.s. �0.050 n.s.
CD14��CD16� cells/�lwhole blood
�0.032 n.s. �0.054 n.s.
CD16 positive cells/�lwhole blood‡
�0.028 n.s. �0.062 n.s.
Mixed cells/�l whole blood 0.103 0.008 0.068 n.s.
n.s. indicates not significant.*Pearson correlation coefficient.†Multivariable adjusted correlation coefficient, adjusted for fasting plasma
glucose, high-density lipoprotein cholesterol, low-density lipoprotein choles-terol, and systolic blood pressure.
‡CD16� monocytes is the sum of CD14�CD16�� and CD14��CD16�.
Table 5. Pearson Correlation Coefficients Between MonocytesSubsets and Laboratory Parameters at Baseline
CD14��CD16�
Cells/�l WholeBlood
CD14��CD16�
Cells/�l WholeBlood
CD14�CD16��
Cells/�l WholeBlood
Cholesterol (mmol/L) �0.062 �0.086* �0.089*
HDL (mmol/L) �0.190† �0.126† �0.178†
Diastolic blood pressure(mm Hg)
0.138† 0.086* 0.128†
*P�0.05.†P�0.01.
128 Circ Cardiovasc Genet February 2012
by guest on July 13, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

patients without restenosis 9 months after bare-metal stentimplantation following acute myocardial infarction.31 Instroke patients, CD16-positive monocytes have been found tohave beneficial effect on clinical outcome, whereas CD14��
CD16� monocytes have been associated with poor outcomeand higher mortality.32 In 1 study, however, the number ofCD16-positive monocytes has been shown to correlate posi-tively to carotid IMT in 622 healthy volunteers, but theassociation was not significant when adjusting for age,gender, and body mass index or Framingham risk score.33 Incontrast, in our study population, which was, on average,more than 20 years older, the negative association betweenCD16-positive monocytes and carotid IMT remained signif-icant, even after adjustment for traditional risk factors.
It should be noted, however, that we only found a negativeassociation between the percentage of CD16-positive mono-cytes and carotid IMT, whereas we did not find any associ-ation between the number of CD16-positive monocytes andcarotid IMT. Instead, an increased number of CD16-positivemonocytes were associated with increased risk, even if thesignificant association was lost when adjusting for traditionalrisk factors. A high CD14��CD16� monocyte count hasbeen associated with higher rates of cardiovascular events ina prospective cohort of 94 patients on dialysis, followed forclose to 3 years.15 CD14��CD16� monocytes have also beenindependently associated with cardiovascular events in 119nondialysis patients, with chronic kidney disease followed upto 5 years.16 Both dialysis patients and patients with chronickidney disease have an elevated risk of cardiovascular dis-ease, and traditional risk factors only account for a fraction ofthe excess risk of CVD in these patients, whereas nontradi-tional risk factors, such as the immune system, have adominant role.34 Furthermore, CD14�CD16�CX3CR1�
monocyte counts have been shown to be higher in patientswith stable angina pectoris, with vulnerable coronary plaques,identified by multidetector computer tomography, than inpatients without vulnerable plaques.35 The number ofCD14�CD16�CX3CR1� monocytes have also been shownto be elevated in patients with unstable angina pectoris, withruptured plaques, identified by optical coherence tomogra-phy, in comparison with patients with unstable angina pec-toris, with nonruptured plaques and patients with stableangina pectoris.36 Our findings that the percentage of CD16-positive monocytes are negatively associated with carotidIMT, whereas CD16-positive monocyte counts might beassociated with increased risk of cardiovascular events, re-flect the disease-promoting and protective roles proposed inthe various studies above. Clearly, more clinical studies andstudies of the biological function of the CD16-positivemonocytes are needed to fully understand their role in CVD.
The Ly-6Clow subset in mice, thought to correspond tohuman CD14�CD16�� monocytes, has been shown to ex-press CCR5 and, interestingly, anti-CCR5 antibody treatmenthas been shown to inhibit Ly-6Clow monocyte entry intoplaques in Apoe
�/�
mice.12,25 In this study, CCR5 expressionon CD14�CD16�� monocytes was negatively associatedwith carotid IMT at baseline. It is tempting to speculate thatCD14�CD16�� monocyte recruitment to plaques is depen-dent on CCR5 expression and that recruitment of CD14�
CD16�� monocytes, ascribed protective/reparative func-tions, reduces the extent of atherosclerosis; however, CCR5expression is not restricted to monocytes, and there isoverwhelming evidence from animal studies for an athero-sclerosis-promoting role for CCR5.37 Also, in human popu-lations, a naturally occurring deletion mutation of the CCR5gene, which results in a truncated nonfunctional CCR5, hasbeen associated with lower carotid IMT in the Bruneck studycohort.38 Consequently, it has been speculated that CCR5antagonists approved for HIV therapy could also limit plaquedevelopment.39 Still, the plaque-promoting contribution ofvarious immune cells expressing CCR5, such as T cells andmonocytes, remains to be fully defined. In addition, it shouldbe noted that we did not observe the selective expression ofCCR5 on intermediate CD14��CD16� monocytes, whichhas been reported by others (Figure 2B).16,26
In the present study, several monocyte subtypes displayeda positive correlation to diastolic blood pressure and negativecorrelations to HDL and cholesterol. Previous studies havereported similar correlations to blood pressure and HDL,whereas the correlation to cholesterol is unclear.2,33 Onepossible explanation to the blood pressure and HDL correla-tions is that they could reflect the general inflammatoryactivation associated with diabetes; however, the lack ofassociation between monocyte subsets and C-reactive protein,as well as a lack of difference in monocyte subsets betweensubjects with or without diabetes (data not shown), argueagainst this possibility.
This study was performed on thawed cells that were storedfrozen at �140°C for up to 15 years. Unfortunately, we havenot been able to control how the cells have changed fromfresh cells over this time period. For instance, we do not knowthe long-term effects of dimethyl sulfoxide, a known immu-nomodulator, used in the cryopreservation.40 Our own (datanot shown), and studies by others, on how cells and markerson cells withstand freezing and thawing show that cryopre-served cells generally compare well to fresh cells, demon-strating that cryopreserved cells could be used in studiesaimed at identifying risk markers.41,42 Still, direct incubationof freshly drawn blood, with antibodies followed by red celllysis, is preferred as ficoll centrifugation, and, perhaps also,freeze-thawing could alter monocyte activation status.43 Ourdata suggest, however, that the number of monocytes is notgreatly affected by freeze thawing (Figure 2C–D).
Although we show that CD14��CD16� monocytes areassociated with a considerable increase in cardiovascular risk,more studies are needed before monocyte analysis will beused in predicting cardiovascular risk in the clinic. Even ifconsidering monocytes as a useful risk marker is premature,clinical studies in larger and more specialized cohorts, withmore phenotypic markers, might help to elucidate the biolog-ical role of monocyte subsets in the various stages of thehuman disease. Animal models also show great potential toelucidate the function of monocyte subsets in experimentalatherosclerosis, even though care must be taken in extrapo-lating these results to humans because of the differences thatexists in atherosclerotic disease and monocyte subsets. Forthese reasons, and in the light of our data presented here,more studies of monocytes in humans are crucial for future
Berg et al CD14��CD16� Monocytes Predict CVD 129
by guest on July 13, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

risk stratification, the development of novel targeted thera-pies, and disease-monitoring, based on knowledge of humanmonocyte biology.
Sources of FundingThe Swedish Research Council, Swedish Heart Lung Foundation,CardioVax, Vinnova, the Foundation for Strategic Research, theSoderberg Foundation, European Community’s Sixth FrameworkProgramme contract (‘IMMUNATH’) LSHM-CT-2006-037400, theAlbert Påhlsson Foundation, the Crafoord Foundation, the MagnusBergvall Foundation, the Swedish Society of Medicine (Social-styrelsen), the Lars Hierta Memorial Foundation, the Thelma ZoegaFoundation, the Knut and Alice Wallenberg Foundation, and theMalmo University Hospital Foundation.
DisclosuresNone.
References1. Woollard KJ, Geissmann F. Monocytes in atherosclerosis: subsets and
functions. Nat Rev Cardiol. 2010;7:77–86.2. Chapman CM, Beilby JP, McQuillan BM, Thompson PL, Hung J.
Monocyte count, but not C-reactive protein or interleukin-6, is an inde-pendent risk marker for subclinical carotid atherosclerosis. Stroke. 2004;35:1619–1624.
3. Johnsen SH, Fosse E, Joakimsen O, Mathiesen EB, Stensland-Bugge E,Njølstad I, Arnesen E. Monocyte count is a predictor of novel plaqueformation: a 7-year follow-up study of 2610 persons without carotidplaque at baseline the Tromsø study. Stroke. 2005;36:715–719.
4. Madjid M, Awan I, Willerson JT, Casscells SW. Leukocyte count andcoronary heart disease: Implications for risk assessment. J Am CollCardiol. 2004;44:1945–1956.
5. Passlick B, Flieger D, Ziegler-Heitbrock HW. Identification and charac-terization of a novel monocyte subpopulation in human peripheral blood.Blood. 1989;74:2527–2534.
6. Geissmann F, Jung S, Littman DR. Blood monocytes consist of twoprincipal subsets with distinct migratory properties. Immunity. 2003;19:71–82.
7. Ziegler-Heitbrock L, Ancuta P, Crowe S, Dalod M, Grau V, Hart DN,Leenen PJ, Liu YJ, MacPherson G, Randolph GJ, Scherberich J, SchmitzJ, Shortman K, Sozzani S, Strobl H, Zembala M, Austyn JM, Lutz MB.Nomenclature of monocytes and dendritic cells in blood. Blood. 2010;116:e74–e80.
8. Belge KU, Dayyani F, Horelt A, Siedlar M, Frankenberger M, Franken-berger B, Espevik T, Ziegler-Heitbrock L. The proinflammatoryCD14�CD16�DR�� monocytes are a major source of TNF. J Immunol.2002;168:3536–3542.
9. Ziegler-Heitbrock L. The CD14�CD16� blood monocytes: their role ininfection and inflammation. J Leukoc Biol. 2007;81:584–592.
10. Ingersoll MA, Spanbroek R, Lottaz C, Gautier EL, Frankenberger M,Hoffmann R, Lang R, Haniffa M, Collin M, Tacke F, Habenicht AJ,Ziegler-Heitbrock L, Randolph GJ. Comparison of gene expressionprofiles between human and mouse monocyte subsets. Blood. 2010;115:e10–e19.
11. Swirski FK, Libby P, Aikawa E, Alcaide P, Luscinskas FW, WeisslederR, Pittet MJ. Ly-6chi monocytes dominate hypercholesterolemia-associated monocytosis and give rise to macrophages in atheromata.J Clin Invest. 2007;117:195–205.
12. Tacke F, Alvarez D, Kaplan TJ, Jakubzick C, Spanbroek R, Llodra J,Garin A, Liu J, Mack M, van Rooijen N, Lira SA, Habenicht AJ,Randolph GJ. Monocyte subsets differentially employ CCR2, CCR5, andCX3CR1 to accumulate within atherosclerotic plaques. J Clin Invest.2007;117:185–194.
13. Combadiere C, Potteaux S, Rodero M, Simon T, Pezard A, Esposito B,Merval R, Proudfoot A, Tedgui A, Mallat Z. Combined inhibition ofCCl2, CX3CR1, and CCR5 abrogates LY6C(hi) and LY6C(lo) mono-cytosis and almost abolishes atherosclerosis in hypercholesterolemicmice. Circulation. 2008;117:1649–1657.
14. Saederup N, Chan L, Lira SA, Charo IF. Fractalkine deficiency markedlyreduces macrophage accumulation and atherosclerotic lesion formation inCCR2�/� mice: Evidence for independent chemokine functions in athero-genesis. Circulation. 2008;117:1642–1648.
15. Heine GH, Ulrich C, Seibert E, Seiler S, Marell J, Reichart B, Krause M,Schlitt A, Kohler H, Girndt M. CD14(��)CD16� monocytes but nottotal monocyte numbers predict cardiovascular events in dialysis patients.Kidney Int. 2008;73:622–629.
16. Rogacev KS, Seiler S, Zawada AM, Reichart B, Herath E, Roth D, UlrichC, Fliser D, Heine GH. CD14��CD16� monocytes and cardiovascularoutcome in patients with chronic kidney disease. Eur Heart J. 2011;32:84–92.
17. Schlitt A, Heine GH, Blankenberg S, Espinola-Klein C, Dopheide JF,Bickel C, Lackner KJ, Iz M, Meyer J, Darius H, Rupprecht HJ.CD14�CD16� monocytes in coronary artery disease and their rela-tionship to serum TNF-alpha levels. Thromb Haemost. 2004;92:419–424.
18. Hristov M, Leyendecker T, Schuhmann C, von Hundelshausen P,Heussen N, Kehmeier E, Krotz F, Sohn HY, Klauss V, Weber C. Circu-lating monocyte subsets and cardiovascular risk factors in coronary arterydisease. Thromb Haemost. 2010;104:412–414.
19. Berglund G, Elmstahl S, Janzon L, Larsson SA. The Malmo Diet andCancer Study. Design and feasibility. J Intern Med. 1993;233:45–51.
20. Rosvall M, Janzon L, Berglund G, Engstrom G, Hedblad B. Incidence ofstroke is related to carotid imt even in the absence of plaque. Atherosclerosis.2005;179:325–331.
21. Hedblad B, Nilsson P, Janzon L, Berglund G. Relation between insulinresistance and carotid intima-media thickness and stenosis in non-diabeticsubjects. Results from a cross-sectional study in Malmo, Sweden. DiabetMed. 2000;17:299–307.
22. Welfare. TNBoHa. Evaluation of quality of diagnosis of acute myocardialinfarction, inpatient register 1997 and 1995. Stockholm, Sweden: Social-styrelsen; 2000.
23. Engstrom G, Jerntorp I, Pessah-Rasmussen H, Hedblad B, Berglund G,Janzon L. Geographic distribution of stroke incidence within an urbanpopulation: relations to socioeconomic circumstances and prevalence ofcardiovascular risk factors. Stroke. 2001;32:1098–1103.
24. Pero RW, Olsson A, Berglund G, Janzon L, Larsson SA, Elmstahl S. TheMalmo biological bank. J Intern Med. 1993;233:63–67.
25. Weber C, Belge KU, von Hundelshausen P, Draude G, Steppich B, MackM, Frankenberger M, Weber KS, Ziegler-Heitbrock HW. Differentialchemokine receptor expression and function in human monocyte sub-populations. J Leukoc Biol. 2000;67:699–704.
26. Ancuta P, Rao R, Moses A, Mehle A, Shaw SK, Luscinskas FW,Gabuzda D. Fractalkine preferentially mediates arrest and migration ofCD16� monocytes. J Exp Med. 2003;197:1701–1707.
27. Kirkwood BR, Sterne JAC. Essential medical statistics. Malden, Mass.:Blackwell Science; 2003.
28. Auffray C, Fogg D, Garfa M, Elain G, Join-Lambert O, Kayal S, SarnackiS, Cumano A, Lauvau G, Geissmann F. Monitoring of blood vessels andtissues by a population of monocytes with patrolling behavior. Science.2007;317:666–670.
29. Nahrendorf M, Swirski FK, Aikawa E, Stangenberg L, Wurdinger T,Figueiredo JL, Libby P, Weissleder R, Pittet MJ. The healing myocardi-um sequentially mobilizes two monocyte subsets with divergent andcomplementary functions. J Exp Med. 2007;204:3037–3047.
30. Tsujioka H, Imanishi T, Ikejima H, Kuroi A, Takarada S, Tanimoto T,Kitabata H, Okochi K, Arita Y, Ishibashi K, Komukai K, Kataiwa H,Nakamura N, Hirata K, Tanaka A, Akasaka T. Impact of heterogeneity ofhuman peripheral blood monocyte subsets on myocardial salvage inpatients with primary acute myocardial infarction. J Am Coll Cardiol.2009;54:130–138.
31. Liu Y, Imanishi T, Ikejima H, Tsujioka H, Ozaki Y, Kuroi A, Okochi K,Ishibashi K, Tanimoto T, Ino Y, Kitabata H, Akasaka T. Associationbetween circulating monocyte subsets and in-stent restenosis aftercoronary stent implantation in patients with ST-elevation myocardialinfarction. Circ J. 2010;74:2585–2591.
32. Urra X, Villamor N, Amaro S, Gomez-Choco M, Obach V, Oleaga L,Planas AM, Chamorro A. Monocyte subtypes predict clinical course andprognosis in human stroke. J Cereb Blood Flow Metab. 2009;29:994–1002.
33. Rogacev KS, Ulrich C, Blomer L, Hornof F, Oster K, Ziegelin M,Cremers B, Grenner Y, Geisel J, Schlitt A, Kohler H, Fliser D, Girndt M,Heine GH. Monocyte heterogeneity in obesity and subclinical atheroscle-rosis. Eur Heart J. 2010;31:369–376.
34. Stenvinkel P, Pecoits-Filho R, Lindholm B. Coronary artery disease inend-stage renal disease: no longer a simple plumbing problem. J Am SocNephrol. 2003;14:1927–1939.
130 Circ Cardiovasc Genet February 2012
by guest on July 13, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from

35. Kashiwagi M, Imanishi T, Tsujioka H, Ikejima H, Kuroi A, Ozaki Y, IshibashiK, Komukai K, Tanimoto T, Ino Y, Kitabata H, Hirata K, Akasaka T. Asso-ciation of monocyte subsets with vulnerability characteristics of coronary plaquesas assessed by 64-slice multidetector computed tomography in patients withstable angina pectoris. Atherosclerosis. 2010;212:171–176.
36. Ikejima H, Imanishi T, Tsujioka H, Kashiwagi M, Kuroi A, Tanimoto T,Kitabata H, Ishibashi K, Komukai K, Takeshita T, Akasaka T. Upregu-lation of fractalkine and its receptor, CX3CR1, is associated withcoronary plaque rupture in patients with unstable angina pectoris. Circ J.2010;74:337–345.
37. Zernecke A, Shagdarsuren E, Weber C. Chemokines in atherosclerosis:An update. Arterioscler Thromb Vasc Biol. 2008;28:1897–1908.
38. Afzal AR, Kiechl S, Daryani YP, Weerasinghe A, Zhang Y, Reindl M, MayrA, Weger S, Xu Q, Willeit J. Common CCR5-DEL32 frameshift mutationassociated with serum levels of inflammatory markers and cardiovasculardisease risk in the Bruneck population. Stroke. 2008;39:1972–1978.
39. Weber C. Obstacles and options in the quest for drug candidates againstvascular disease. Thromb Haemost. 2010;104:1–3.
40. Camici GG, Steffel J, Akhmedov A, Schafer N, Baldinger J, Schulz U,Shojaati K, Matter CM, Yang Z, Luscher TF, Tanner FC. Dimethylsulfoxide inhibits tissue factor expression, thrombus formation, andvascular smooth muscle cell activation: A potential treatment strategy fordrug-eluting stents. Circulation. 2006;114:1512–1521.
41. Maecker HT, Moon J, Bhatia S, Ghanekar SA, Maino VC, Payne JK,Kuus-Reichel K, Chang JC, Summers A, Clay TM, Morse MA, LyerlyHK, DeLaRosa C, Ankerst DP, Disis ML. Impact of cryopreservation ontetramer, cytokine flow cytometry, and ELISPOT. BMC Immunol.2005;6:17.
42. Van Hemelen D, Oude Elberink JN, Heimweg J, van Oosterhout AJ,Nawijn MC. Cryopreservation does not alter the frequency of regulatoryt cells in peripheral blood mononuclear cells. J Immunol Methods. 2010;353:138–140.
43. Lundahl J, Hallden G, Hallgren M, Skold CM, Hed J. Altered expressionof CD11b/CD18 and CD62l on human monocytes after cell preparationprocedures. J Immunol Methods. 1995;180:93–100.
CLINICAL PERSPECTIVEMacrophage foam cells are the archetypical cells of the atherosclerotic lesion, and recruitment of monocytes is thought tobe a prerequisite for lesion formation. Although monocyte count is a predictor of subclinical carotid atherosclerosis andplaque formation, associations between monocyte counts and cardiovascular disease risk have not been highlighted in largeepidemiological studies. In the present study, mononuclear leukocytes, frozen at the baseline investigation in 1991 to 1994,from 700 randomly selected individuals, were thawed, and monocyte subsets were enumerated with flow cytometry basedon their expression of CD14 and CD16. Classical CD14��CD16� monocytes were increased in the group of individualsexperiencing cardiovascular events compared with the event-free group during follow up, until 2008. Elevated classicalmonocytes predicted cardiovascular disease risk, independently of common risk factors. Classical monocytes did not,however, associate with the extent of carotid atherosclerosis measured as intima-media thickness at baseline. In contrast,the percentage of monocytes expressing CD16 was negatively associated to the extent of atherosclerosis. These findingsmight indicate that different monocyte subsets have different biological functions and thus contribute to lesion size andclinical events in different ways. Clinical studies in larger and more specialized cohorts with more phenotypic markersmight help to elucidate the biological role of monocyte subsets in the various stages of human atherosclerosis andcardiovascular disease. The relation between circulating monocyte subsets and macrophage phenotypes found within theatherosclerotic lesion and the mechanisms of monocyte recruitment also needs to be clarified before we fully understandthe role of monocytes in cardiovascular disease.
Berg et al CD14��CD16� Monocytes Predict CVD 131
by guest on July 13, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from
N. Fredrikson, Jan Nilsson and Harry BjörkbackaKatarina E. Berg, Irena Ljungcrantz, Linda Andersson, Carl Bryngelsson, Bo Hedblad, Gunilla
Monocytes Predict Cardiovascular Events−CD16++Elevated CD14
Print ISSN: 1942-325X. Online ISSN: 1942-3268 Copyright © 2012 American Heart Association, Inc. All rights reserved.
Dallas, TX 75231is published by the American Heart Association, 7272 Greenville Avenue,Circulation: Cardiovascular Genetics
doi: 10.1161/CIRCGENETICS.111.9603852012;5:122-131; originally published online January 11, 2012;Circ Cardiovasc Genet.
http://circgenetics.ahajournals.org/content/5/1/122World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circgenetics.ahajournals.org//subscriptions/
is online at: Circulation: Cardiovascular Genetics Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
requested is located, click Request Permissions in the middle column of the Web page under Services. FurtherCenter, not the Editorial Office. Once the online version of the published article for which permission is being
can be obtained via RightsLink, a service of the Copyright ClearanceCirculation: Cardiovascular Geneticsin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on July 13, 2018http://circgenetics.ahajournals.org/
Dow
nloaded from