effects of topical unoprostone and latanoprost on acute and recurrent herpetic keratitis in the...
TRANSCRIPT
Effects of Topical Unoprostone andLatanoprost on Acute and Recurrent Herpetic
Keratitis in the Rabbit
HERBERT E. KAUFMAN, MD, EMILY D. VARNELL, BS, HIROSHI TOSHIDA, MD,ATSUSHI KANAI, MD, HILARY W. THOMPSON, PHD, AND
NICOLAS G. BAZAN, MD, PHD
● PURPOSE: To determine the effect of the topical ocularhypotensive drug, isopropyl unoprostone, a docosanoidmolecule with very weak prostaglandin activity, on her-pes keratitis in the rabbit eye.● METHODS: For acute disease, rabbit corneas inoculatedwith the corticosteroid-sensitive F(MP)E strain of herpessimplex virus type 1 were treated with various combina-tions of 0.12% isopropyl unoprostone, latanoprost, tri-fluridine, benzalkonium chloride 0.02%, dexamethasonesodium phosphate, ketorolac tromethamine, or salinesolution beginning 1 day after infection. Severity ofkeratitis was evaluated in a masked manner. For recur-rent disease, rabbit corneas infected with McKrae strainherpes simplex virus type 1 were treated with unopros-tone or saline solution on postinfection days 25 to 42,and the presence or absence of lesions was recorded.● RESULTS: Eyes treated with unoprostone showedsignificantly less severe disease than saline-treated orlatanoprost-treated eyes during acute infection. Uno-prostone-treated and saline-treated eyes showed no sig-nificant difference in the frequency of recurrent lesions.Eyes treated with latanoprost and/or dexamethasone,separately or in combination, showed increased severityof acute herpes simplex virus keratitis, whereas benzal-konium chloride 0.02%–treated eyes showed no signif-
icant difference, compared with saline treatment.Trifluridine resulted in rapid healing.● CONCLUSIONS: Unoprostone did not increase the se-verity or recurrence rate of herpes simplex virus kerati-tis. Unoprostone requires twice-a-day administration,compared with once-a-day for latanoprost, and unopros-tone lowers intraocular pressure less than latanoprost.Nevertheless, unoprostone’s superior safety profile maymake its use advantageous. Benzalkonium chloride alonedid not make the keratitis worse. (Am J Ophthalmol2001;131:643–646. © 2001 by Elsevier Science Inc.All rights reserved.)
P ROSTAGLANDINS, WHICH ARE ACTIVELY GENERATED
in experimental herpetic keratitis,1 play an importantrole in epithelial repair and act as mediators of the
injury/inflammatory response.2 Latanoprost is a prostaglan-din F2a analog that binds to prostaglandin receptors. Inaddition to lowering intraocular pressure, however, it hasbeen associated with uveitis, cystoid macular edema, hy-pertrichosis, and iris pigmentation,3 as well as dendritiformepitheliopathy4 and exacerbation of ocular herpetic diseaseand recurrences,5 in clinical reports. Latanoprost has alsobeen associated with more severe disease and increasedrecurrences in an animal model.6
Isopropyl unoprostone, a 22-carbon docosanoid struc-ture, is an ocular hypotensive agent that has been usedclinically in Japan for the past 6 years and has recentlybeen approved by the FDA for clinical use in the UnitedStates. Its mechanism of action is uncertain, and it doesnot appear to bind to prostaglandin receptors. To ourknowledge, no studies of the effect of unoprostone onocular herpetic infection have been reported.
This study was designed to determine whether unopros-tone worsens ocular herpes as latanoprost has been shownto do, and whether the exacerbation of ocular herpescaused by latanoprost is related to the presence of thepreservative benzalkonium chloride in the commercialformulation.
Accepted for publication Nov 20, 2000.From the Louisiana State University Eye Center (Drs Kaufman,
Toshida, Thompson, and Bazan, and Ms Varnell) and the NeuroscienceCenter of Excellence (Drs Kaufman, Thompson, and Bazan), LouisianaState University Health Sciences Center, New Orleans, Louisiana, andDepartment of Ophthalmology, Juntendo University (Dr Kanai), Tokyo,Japan.
This study was supported in part by US Public Health Service GrantsEY02672 (Dr Kaufman) and EY02377 (Dr Kaufman) from the NationalEye Institute, National Institutes of Health, Bethesda, Maryland, and anunrestricted departmental grant from Research to Prevent Blindness,New York, New York.
This work was presented in part at the Association for Research inVision and Ophthalmology, April 30, 2000, Fort Lauderdale, Florida.
Reprint requests to Emily D. Varnell, BS, Louisiana State UniversityEye Center, 2020 Gravier St, Suite B, New Orleans, LA 70112; fax: (504)412-1315; e-mail: [email protected]
© 2001 BY ELSEVIER SCIENCE INC. ALL RIGHTS RESERVED.0002-9394/01/$20.00 643PII S0002-9394(00)00910-7

MATERIAL AND METHODS
NEW ZEALAND WHITE RABBITS OF BOTH SEXES WERE USED
and handled in accordance with the National Institutes ofHealth guidelines on the care and use of animals inresearch; the Association for Research in Vision andOphthalmology Statement for the Use of Animals inOphthalmic and Vision Research; and the Louisiana StateUniversity Health Sciences Center in New Orleans Insti-tutional Animal Care and Use Committee guidelines andapprovals.
The compounds used in this study were the commercialformulation of latanoprost (0.005% with benzalkoniumchloride 0.02%, Xalatan; Pharmacia, Inc, Kalamazoo,Michigan), the commercial formulation of isopropyl uno-prostone as used in Japan (0.12% with benzalkoniumchloride 0.01% and polysorbate 80 1%, Rescula; UenoPharmaceutical, Hyogo, Japan), dexamethasone sodiumphosphate 0.1% (Schein Pharmaceutical, Florham Park,New Jersey), ketorolac tromethamine 0.5% (Acular PF;Allergan, Irvine, California), trifluridine 1% (Schein Phar-maceutical, Florham Park, New Jersey), benzalkoniumchloride 0.02% (Sigma Chemical Company, St. Louis,Missouri) in balanced saline solution (Alcon Pharmaceu-ticals, Fort Worth, Texas), and balanced saline solution.
Herpes virus strains were propagated in primary rabbitkidney cells. The corticosteroid-sensitive F(MP)E strain ofherpes simplex virus type 1 was supplied by BernardRoizman, PhD, of the University of Chicago.7,8 TheMcKrae strain of herpes simplex virus type 1, which causesspontaneous recurrent disease, was isolated in our labora-tory more than 35 years ago.9
For virus inoculation, both corneas of each rabbit wereanesthetized with proparacaine hydrochloride, the superfi-cial corneal epithelium was lightly scarified with a 27-gauge needle (to synchronize the initial appearance andseverity of keratitis), and 2 3 105 plaque-forming units(PFU) of F(MP)E or 7.5 3 105 PFU of McKrae strain viruswas dropped onto the cornea. The eyelids were gentlyrubbed over the cornea for 15 seconds.
Three studies of acute infection were done. In one acuteinfection study, 50 rabbits were infected with the F(MP)Estrain. On day 1 after infection, the animals were random-ized to twice-a-day treatment with latanoprost, unopros-tone, dexamethasone, ketorolac, or balanced salinesolution. Dexamethasone treatment was administered for 3days, and the other compounds were administered for 9days. The severity of disease was graded on a masked basisdaily through day 9 after infection.10
In another acute infection study, 50 rabbits were in-fected with the F(MP)E strain of herpes simplex virus type1. On day 1 after infection, the animals were randomizedto twice-a-day treatment with latanoprost, dexametha-sone, latanoprost plus dexamethasone, latanoprost plustrifluridine, or balanced saline solution. Both eyes of agiven animal received the same treatment. Dexametha-
sone was administered for 3 days, and latanoprost, trifluri-dine, and balanced saline solution were administered for10 days. The severity of disease was graded daily on amasked basis from day 1 through day 10 after infection.
In a third acute infection study, 30 rabbits were infectedwith the F(MP)E strain. On day 1 after infection, theanimals were randomized to twice-a-day treatment withlatanoprost, benzalkonium chloride 0.02%, or balancedsaline solution. The severity of keratitis was graded dailyon days 1 through 7 after infection.
In all of these studies, treatments were coded. Corneaswere stained with fluorescein and examined with theslit-lamp biomicroscope, and the severity of keratitis wasgraded in a masked manner, based on a scale of 0 to 4 inwhich 0 5 normal cornea; 1 5 epithelial ulcerationinvolving a quarter of the epithelial area; 2 5 epithelialulceration involving half of the epithelial area; 3 5epithelial ulceration involving three quarters of the epi-thelial area; and 4 5 total epithelial involvement.
To examine the effect of unoprostone on recurrentkeratitis, 28 rabbits infected with McKrae strain herpessimplex virus type 1 were randomized to treatment withunoprostone or balanced saline solution on a twice-a-dayschedule for 17 days, beginning on day 25 after infection.The corneas were evaluated daily for the presence ofvisible lesions in a masked manner by slit-lamp biomicros-copy on postinfection days 15 through 42.
For statistical analysis, the outcome variable in the acuteinfection studies was the severity of keratitis score. Drugtreatments were the dependent variable. Variability result-ing from differences between rabbits within treatments wascontrolled for by application of a repeated measures anal-ysis of variance with subsequent comparisons of treatmentmeans conducted using protected t tests on least squaremeans from the analysis of variance.11 The recurrencestudy data were expressed as three time classes (25 to 30days, 31 to 36 days, and 37 to 42 days), to reduce thenumber of comparisons required in the analysis. Timeclasses were treated as dependent variables along with drugtreatments in a two-way analysis of variance. Comparisonsof drug by time class interactions were conducted usingprotected t tests on least square means. All P values forprotected t tests were adjusted to account for the numberof multiple comparisons in both analyses (severity scoresand recurrence).
RESULTS
IN THE STUDY OF ACUTE DISEASE, TREATMENT WITH UNO-
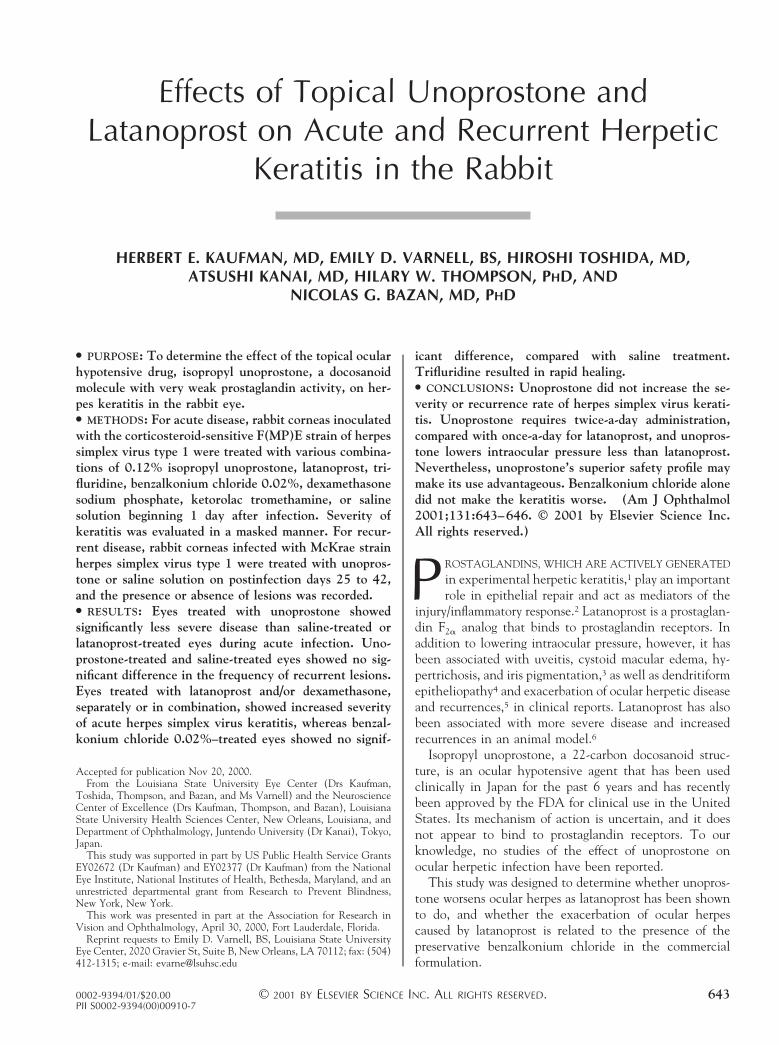
prostone twice a day produced a keratitis that was signifi-cantly less severe on postinfection day 5 (P 5 .0128) andday 6 (P 5 .0045) than treatment with balanced salinesolution and significantly less severe on postinfection day 5(P 5 .0001), days 6 and 7 (P 5 .001), and day 8 (P 5.0189) than treatment with latanoprost (Figure 1). In the
AMERICAN JOURNAL OF OPHTHALMOLOGY644 MAY 2001
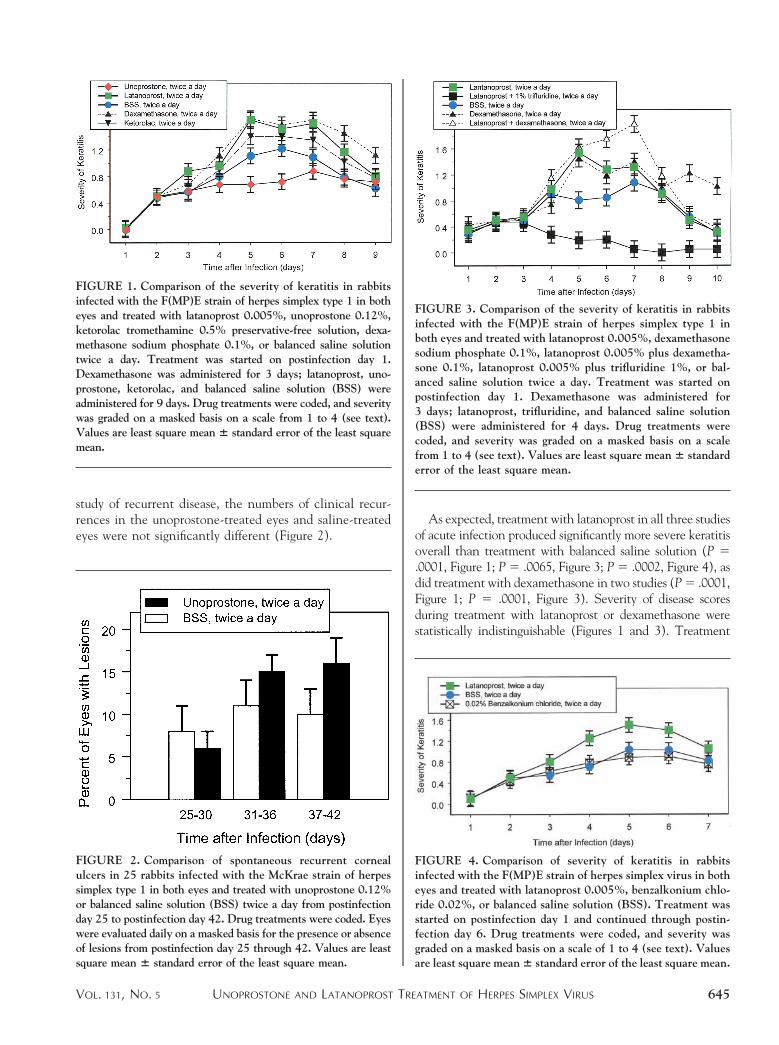
study of recurrent disease, the numbers of clinical recur-rences in the unoprostone-treated eyes and saline-treatedeyes were not significantly different (Figure 2).
As expected, treatment with latanoprost in all three studiesof acute infection produced significantly more severe keratitisoverall than treatment with balanced saline solution (P 5.0001, Figure 1; P 5 .0065, Figure 3; P 5 .0002, Figure 4), asdid treatment with dexamethasone in two studies (P 5 .0001,Figure 1; P 5 .0001, Figure 3). Severity of disease scoresduring treatment with latanoprost or dexamethasone werestatistically indistinguishable (Figures 1 and 3). Treatment
FIGURE 1. Comparison of the severity of keratitis in rabbitsinfected with the F(MP)E strain of herpes simplex type 1 in botheyes and treated with latanoprost 0.005%, unoprostone 0.12%,ketorolac tromethamine 0.5% preservative-free solution, dexa-methasone sodium phosphate 0.1%, or balanced saline solutiontwice a day. Treatment was started on postinfection day 1.Dexamethasone was administered for 3 days; latanoprost, uno-prostone, ketorolac, and balanced saline solution (BSS) wereadministered for 9 days. Drug treatments were coded, and severitywas graded on a masked basis on a scale from 1 to 4 (see text).Values are least square mean 6 standard error of the least squaremean.
FIGURE 2. Comparison of spontaneous recurrent cornealulcers in 25 rabbits infected with the McKrae strain of herpessimplex type 1 in both eyes and treated with unoprostone 0.12%or balanced saline solution (BSS) twice a day from postinfectionday 25 to postinfection day 42. Drug treatments were coded. Eyeswere evaluated daily on a masked basis for the presence or absenceof lesions from postinfection day 25 through 42. Values are leastsquare mean 6 standard error of the least square mean.
FIGURE 3. Comparison of the severity of keratitis in rabbitsinfected with the F(MP)E strain of herpes simplex type 1 inboth eyes and treated with latanoprost 0.005%, dexamethasonesodium phosphate 0.1%, latanoprost 0.005% plus dexametha-sone 0.1%, latanoprost 0.005% plus trifluridine 1%, or bal-anced saline solution twice a day. Treatment was started onpostinfection day 1. Dexamethasone was administered for3 days; latanoprost, trifluridine, and balanced saline solution(BSS) were administered for 4 days. Drug treatments werecoded, and severity was graded on a masked basis on a scalefrom 1 to 4 (see text). Values are least square mean 6 standarderror of the least square mean.
FIGURE 4. Comparison of severity of keratitis in rabbitsinfected with the F(MP)E strain of herpes simplex virus in botheyes and treated with latanoprost 0.005%, benzalkonium chlo-ride 0.02%, or balanced saline solution (BSS). Treatment wasstarted on postinfection day 1 and continued through postin-fection day 6. Drug treatments were coded, and severity wasgraded on a masked basis on a scale of 1 to 4 (see text). Valuesare least square mean 6 standard error of the least square mean.
UNOPROSTONE AND LATANOPROST TREATMENT OF HERPES SIMPLEX VIRUSVOL. 131, NO. 5 645

with latanoprost plus dexamethasone produced significantlymore severe keratitis than treatment with balanced salinesolution (P 5 .0001, Figure 3) or treatment with latanoprostalone (P 5 .0015; Figure 3).
Treatment with latanoprost plus trifluridine producedsignificantly less severe keratitis than any of the othertreatments (P 5 .0001; Figure 3). The mean severity scorein the group treated with latanoprost plus trifluridine wassignificantly less than the score in the saline-treated groupon postinfection day 4 (P 5 .0006), and the scorescontinued to be significantly less through postinfection day9 (P , .006, days 5 to 9; Figure 3). Treatment with thepreservative-free nonsteroidal anti-inflammatory drug ke-torolac produced a keratitis that was not distinguishablefrom that seen in the saline-treated eyes (Figure 1).
Treatment with benzalkonium chloride solution 0.02%alone yielded severity scores that were significantly lessthan those obtained with latanoprost (P 5 .0001, Figure 4)and not statistically distinguishable from those of thesaline-treated eyes (Figure 4).
DISCUSSION
LATANOPROST IS A PROSTAGLANDIN ANALOG THAT BINDS
to prostaglandin receptors. Isopropyl unoprostone is asynthetic 22-carbon docosanoid molecule.12,13 Doco-sanoids are metabolites of docosahexaenoic acid, a memberof a family of essential fatty acids that do not bind toprostaglandin receptors. The mechanism of action of thesetwo compounds on aqueous humor outflow is different. Insome species, unoprostone has a greater effect on thetrabecular outflow than on the uveoscleral outflow andmay stimulate the synthesis of prostaglandin E in theeye.14,15 Unoprostone may also increase retinal blood flowand be neuroprotective at the level of the retinal ganglioncell. Based on the results of our studies, unoprostone doesnot increase the severity of acute herpes keratitis, nor doesit increase the risk of recurrent herpes. As a continuationof this project, we are currently studying the effects ofdifferent doses of unoprostone and latanoprost on herpetickeratitis and recurrences.
Latanoprost is not only associated with cystoid macularedema, uveitis, and eyelash and iris hyperpigmentation,3but also with increased severity and recurrences of ocularherpes in patients5 and in an animal model.6 We do notuse latanoprost in postoperative patients who have under-gone penetrating keratoplasty. We believe that unopros-tone may have a superior safety profile, even if it must beadministered twice a day and lowers the intraocular pres-sure slightly less than latanoprost.
REFERENCES
1. Birkle DL, Sanitato JJ, Kaufman HE, Bazan NG. Arachi-donic acid metabolism to eicosanoids in herpes virus-infectedrabbit cornea. Invest Ophthalmol Vis Sci 1986;27:1443–1446.
2. Bazan NG, Allan G. Signal transduction and gene expressionin the eye: a contemporary review of the pro-inflammatory,anti-inflammatory and modulatory roles of prostaglandinsand other bioactive lipids. Surv Ophthalmol 1997;41(suppl2):S23–S34.
3. Warwar RE, Bullock JD, Ballal D. Cystoid macular edemaand anterior uveitis associated with latanoprost use. Experi-ence and incidence in a retrospective review of 94 patients.Ophthalmology 1999;105:263–268.
4. Sudesh S, Cohen EJ, Rapuano CJ, Wilson RP. Cornealtoxicity associated with latanoprost. Arch Ophthalmol 1999;117:539–540.
5. Wand M, Gilbert CM, Liesegang TJ. Latanoprost and herpessimplex keratitis. Am J Ophthalmol 1999;127:602–604.
6. Kaufman HE, Varnell ED, Thompson HW. Latanoprostincreases the severity and recurrences of herpetic keratitis inthe rabbit. Am J Ophthalmol 1999;127:531–536.
7. Centifanto-Fitzgerald YM, Yamaguchi T, Kaufman HE, Tog-non M, Roizman B. Ocular disease pattern induced by herpessimplex virus is genetically determined by a specific region ofviral DNA. J Exp Med 1982;155:475–489.
8. Kaufman HE, Varnell ED, Centifanto YM, Kissling GE.Effect of the herpes simplex virus genome on the response ofinfection to corticosteroids. Am J Ophthalmol 1985;100:114–118.
9. Kaufman HE, Maloney ED, Nesburn AB. Comparison ofspecific antiviral agents in herpes simplex keratitis. InvestOphthalmol 1962;1:686–692.
10. Meyer RF, Varnell ED, Kaufman HE. Phosphonoacetic acidin the treatment of experimental ocular herpes simplexinfections. Antimicrob Agents Chemother 1976;9:308–311.
11. Milliken GA, Johnson DE. Analysis of messy data. Designedexperiments. Volume 1. New York: Van Nostrand ReinholdCompany, 1984:473.
12. Bazan NG, Birkle DL, Reddy TS. Docosahexanoic acid(22:6, n-3) is metabolized to lipoxygenase reaction productsin the retina. Biochem Biophys Res Commun 1984;125:741–747.
13. Bazan NG. The metabolism of omega-3 polyunsaturated fattyacids in the eye: the possible role of docosahexaenoic acidand docosanoids in retinal physiology and ocular pathology.In: Bito LZ, Stjernschantz J, editors. The ocular effects ofprostaglandins and other eicosanoids. New York: Alan R.Liss, 1989:95–112.
14. Serle JB, Podos SM, Kitazawa Y, Wang RF. A comparativestudy of latanoprost (Xalatan) and isopropyl unoprostone(Rescula) in normal and glaucomatous monkey eyes. Jpn JOphthalmol 1998;42:95–100.
15. Eisenberg DL, Camras CB. A preliminary risk–benefit assess-ment of latanoprost and unoprostone in open-angle glau-coma and ocular hypertension. Drug Safety 1999;20:505–514.
AMERICAN JOURNAL OF OPHTHALMOLOGY646 MAY 2001